
Abstract
Teaching parents to serve as interventionists for their children is a common approach to enhance child learning. Research demonstrates that parents are able to implement evidence-based interventions with high integrity; however, there is limited research indicating the extent to which parents are able to maintain skills. We taught parents of two children, age 10 and 11, to implement three positive behavior support skills: praise, choice making, and setting expectations. Using a multiple baseline across skills design, parents demonstrated criterion level use of all three skills; however, only one skill for one parent maintained. We then taught parents to self-monitor the use of skills that did not maintain. Following self-monitoring, parents demonstrated immediate increases in strategy implementation. In addition, both children demonstrated significant increases in engagement and decreases in problem behavior. Social validity results indicated high acceptability by both parents.
Teaching parents to implement evidence-based interventions is a common practice for many reasons. First, parents have the most frequent and continual presence in their child’s life (Marcus et al., 2001; Maughan et al., 2005) and thus have the ability to provide interventions within the natural environment for extended amounts of time (Maughan et al., 2005). In addition, this approach may also address long wait times to receive services (Lane et al., 2016), possible specialist shortages due to increasing demand (Maughan et al., 2005), and families who are isolated geographically (Subramaniam et al., 2017). Furthermore, parent education and training has been validated by positive outcomes that have demonstrated parents are able to learn and implement intervention strategies leading to positive child gains (Lundahl et al., 2006).
Parent Education Scope
Parents have served as interventionists in a broad range of areas, including communication skills (Barton & Fettig, 2013; Hemmeter & Kaiser, 1994), functional living skills (Sharp et al., 2014), and positive behavior supports (Durand et al., 2013). In addition, a broad range of child populations have been represented in the parent education literature. This includes children with autism spectrum disorder (ASD; Matson et al., 2009), developmental disabilities (DDs; Marcus et al., 2001; McIntyre, 2008), emotional and behavioral disorders (EBDs; Danforth, 1998), and attention-deficit/hyperactivity disorder (ADHD; Lee et al., 2012). In spite of research to support parent skill implementation with high integrity, there has been limited research assessing whether parents maintain those skills over time (Moore & Symons, 2011).
Maintenance
Maintenance refers to parent adherence to the intervention after clinician support is faded. Research indicates that even after initial mastery, parents do not always maintain the skills learned. For example, Moore and Symons (2011) taught parents six skills (establish reinforcer, offer choices, deliver instructions, honor requests, redirect, and respond to behavior) to implement with their children. At follow up, parents maintained only one (honor requests) at a sufficient level (above 80%).
A related issue pertains to the time period in which maintenance is assessed. For example, in a review of interventions implemented by parents of young children, Barton and Fettig (2013) found that only nine of 24 studies measured maintenance, and the length of time when the maintenance was assessed ranged from 1 week to 7 years. This makes it difficult to assess when parent implementation of skills begins to decline. A meta-analysis of behavioral training for parents of children with ADHD conducted by Lee et al. (2012) indicated that effects dissipated rapidly when clinician services were fully faded prior to the maintenance phase. However, given the heritability of ADHD, it is unclear whether these findings might generalize to parents of children with other disorders. Thus, issues related to dissipation of parent maintenance of skills warrant additional research (Moore & Symons, 2011).
In addition, the procedures employed during the maintenance period also vary and appear to influence maintenance results. Studies in which parents have been provided ongoing clinical support (therapist supervision, phone calls, and check-in visits) following parent instruction have produced better maintenance. For example, Subramaniam et al. (2017) conducted maintenance probes while parents still had access to video-conferencing feedback and reported that parents were able to maintain skills taught. In contrast, training effects do not appear to maintain when clinician services were fully faded following interventions (Lee et al., 2012).
Finally, when parent skills do not maintain, it is common to retrain using strategies such as a booster session (Van Camp, Montgomery, et al., 2008). Instruction during booster sessions is often consistent with the initial training (Eyberg et al., 1998), assuming a skill deficit. However, it may be inaccurate to assume that parents do not recall the skill taught. Another explanation for lack of maintenance is that parents can perform the skill, but do not remember to implement it when needed. In this case, self-monitoring interventions may be more effective for skill maintenance.
Self-Monitoring
Self-monitoring has been demonstrated to be an effective method to increase fidelity of behavioral interventions (Pinkelman & Horner, 2017). Research has demonstrated that becoming aware of and recording one’s own behavior can result in behavioral change (Reid & Harris, 1993). To date, however, research has almost exclusively assessed educator use of self-monitoring to improve fidelity. For example, Pinkelman and Horner (2017) found that self-monitoring increased educational assistants’ implementation of behavior intervention strategies. In addition, the assistants reported ease of use on the social validity measure.
This finding is consistent with a recent systematic review of teachers’ use of self-monitoring behavior strategies conducted by Rispoli et al. (2017). The review included 17 studies, seven meeting all Council for Exceptional Children Quality Indicators (Cook et al., 2015). Among the reviewed studies, praise was the most common practice targeted for self-monitoring. The self-monitoring varied to include frequency count, rate, steps implemented correctly, and quality ratings. Although only eight studies assessed social validity, most teachers indicated self-monitoring was effective and helpful and were favorable about future use.
Given the likelihood that similar barriers (e.g., competing demands) impede ongoing implementation fidelity by both teachers and parents, these studies suggest a possible strategy for use by parents. This is particularly important because research has found that parents’ continued adherence to training predicts child improvement (Rooney et al., 2018). In spite of potential benefits, studies aimed at teaching parents to self-monitor their own behaviors are limited. As early as the 1980s, a review by Sanders and James (1982) noted that behavioral parent training already had much evidence of effectiveness, but maintenance of parent skills had been neglected. The authors noted that the very premise of parent education was founded on the expectation that parents will engage in self-controlling behaviors (i.e., outside of the direct influence of a clinician), yet parents were not being taught to accomplish this distinct skill.
In one of the few studies examining self-management with parents, Sanders and Glynn (1981) examined maintenance of skills taught during parent education using a variety of self-management procedures, including goal selection, program design, self-monitoring, and planning skills. Results indicated that parents generalized and maintained skills following self-management instruction. However, the authors noted their inability to determine a causal relationship due to study design (generalization and maintenance may have resulted from initial instruction alone) and to isolate which of the self-management strategies was effective. The authors recommended that maintenance should be systematically planned and called for future research in this area. In spite of extensive research on parent education, there continues to be an overall lack of knowledge surrounding the variables associated with skill maintenance (Eyberg et al., 1998; Lee et al., 2012; Van Camp, Montgomery, et al., 2008) and many questions remain unanswered.
Purpose
This study sought to fill the gap in the area of maintenance of parent skills by examining the effectiveness of behavioral parent training followed by self-management for declining skills. The research questions and hypothesis were:
Will behavioral parent training result in criterion-level mastery of three skills by parents? Based on previous findings, it was hypothesized that by following training strategies culled from the literature parents would master all skills with high integrity.
Will parents maintain implementation of three mastered skills over time? As suggested by previous research, it was hypothesized that parents would not maintain implementation of all three skills.
For skills that show below criterion-level maintenance, will self-monitoring increase parent implementation of the skill? Previous research suggests that self-monitoring tool will result in return to criterion levels of parent skill implementation.
Method
Participants and Setting
Recruitment
Participants were referred by an agency that provides services to individuals with disabilities. Providers referred parent/child dyads in which one parent was willing to serve as the primary participant. The investigator subsequently met with each family to obtain consent via forms approved by the University Institutional Review Board. After consent was provided, the researcher (first author) conducted screening to determine whether potential participants met inclusionary/exclusion criteria.
Parents
Parents served as primary participants. The participating parent was the primary caregiver, defined by seeing the child at least 5 out of 7 days for a minimum of 5 hrs per day. To be included, the caregiver had to (a) be willing to implement three positive behavior support strategies and (b) have a child who would benefit from positive behavior support strategies implemented in the home setting. The parent for dyad 1, Jane, was a white single mother of one child. Jane reported her highest educational level achieved was a master’s degree. At the time of the study, she was currently working full time while residing with her son in a suburban neighborhood. The parent for dyad 2, Mary, was also a white single mother of two children. She reported her highest education level achieved as a master’s degree. She worked full time and resided in a suburban neighborhood with her children.
Children
Although child behavior was not the primary variable of interest, child data were collected to evaluate whether parent implementation of intervention strategies was associated with child behavior improvements. Child inclusionary criteria were (a) age between 3 and 12 years old, (b) moderate behavioral concerns as reported by parent, and (c) Individuals with Disabilities Education Act (IDEA; 2004) or Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013) diagnosis of EBD, learning disability, or ADHD. Children with severe behavioral needs (self-injury and aggression) were excluded from the study as a functional behavioral assessment, and behavior intervention plan was not a component of the study.
The child for dyad 1, Jerome, was a biracial, 11-year-old boy, diagnosed with a specific learning disability and anxiety disorder. During the study, he attended a private school. His mother reported primary behavior concerns were resistance and refusal to complete household tasks and lack of independence with common routines, such as getting ready for school. Jane reported it was common for Jerome to refuse to complete tasks, resulting in her completing them for him. Jane reported no home routines or tasks that Jerome would independently complete, and reported approximately six tasks she believed he would attempt with her assistance.
The child for dyad 2, Mason, was a white, 10-year-old boy, diagnosed with a specific learning disability and ADHD. During the study, he attended a public school. His mother reported primary behavior concerns were long delays to begin tasks (requiring extensive prompting) and inability to remain engaged in tasks. This commonly led to incomplete or unsatisfactory completion (i.e., completing a chore incorrectly or missing required steps in nighttime routine). Tasks required parental supervision and assistance beyond what would be expected when compared to a peer of his chronological age.
All sessions were conducted in the participants’ homes. Sessions for Jane and Jerome were conducted in the home (kitchen, living room, and play room). Jerome’s father and grandmother were present in the home, but not in the same room as the mother and child. Sessions for Mary and Mason also were conducted in the home (kitchen, living room, bedroom, and bathroom). Mason’s sister was present for most sessions.
Materials
Training Materials
A systematic protocol for instructing parents was used that outlined the training procedures and sequence. The protocol was based on the common teaching practices outlined in Barton and Fettig (2013) using teaching procedures with demonstrated evidence of effectiveness in training behavioral skills to parents (Lane et al., 2016). The researcher used a form for direct instruction, outlining the purpose and rationale, definition, and how to implement the skill along with examples and nonexamples of each of the three behavior support strategies to be taught.
Self-Monitoring Tool
Self-monitoring was completed using an individualized form developed through a Google host. The form consisted of the skill(s) that the parent was to monitor. The parent set a timer at the beginning of the first task to alert her to the end of each interval, then indicated on the form if she engaged in the listed skill (yes or no) for praise and choice, and if yes, how many times (scale = 0–10) at the end of each 4- or 5-min interval. For setting expectations, a checkmark indicating that expectations were reviewed was placed next to the task completed.
Measures and Measurement Procedures
Parent Strategy Implementation
The primary dependent variable was parent implementation of three evidence-based general positive behavior support strategies. The first strategy was providing specific verbal praise, defined as verbally stating a positive evaluation of the behavior the child is demonstrating (e.g., Danforth, 1998). Examples included, “I love how you are chewing with your mouth closed” and “Thank you for sitting on the chair.”
The second strategy was offering dichotomous choice, defined as providing an opportunity for the child to select from among two choice options. This could be a choice of the task to complete, the sequence of tasks, materials to use, where to complete tasks, or with whom to complete tasks (Bambara & Kern, 2005). Examples include, “Do you want to sit here or there?” “Do you want to get dressed or brush your teeth first?” “Do you want to draw or color?”
The third strategy was setting expectations, defined as the parent describing to the child the exact behavior she would like the child to perform in a clear, brief, specific manner (e.g., Van Camp, Vollmer, et al., 2008) using declarative language such as, “It’s time to eat, sit down.” Non-examples included “Don’t do that,” “You need to finish,” or “Are you hungry?”
All training, parent implementation, and maintenance sessions were video recorded for measurement purposes. Each of the three skills was coded as occurrence or non-occurrence during each 30-s interval.
Child Behaviors
Secondary dependent variables included child engagement and challenging behavior. Engagement was defined as remaining in the designated area, following parent instructions, and interacting appropriately with activity materials provided (e.g., Blair et al., 2011). Challenging behavior was defined as any behavior that interferes with or is at risk of interfering with optimal learning or engagement in pro-social interactions with peers and adults (e.g., Smith & Fox, 2003). Examples include disruption (e.g., throwing materials), inappropriate vocalizations, screaming, tantrums, aggression, and statements of refusal to parent request. Child behavior was coded as occurrence or nonoccurrence during each 30-s interval.
Observer Training
Two graduate students, masked to the study purpose and procedures, coded parent and child behavior data from videotaped sessions. The researcher trained observers using direct instruction by reviewing the operational definition of primary and secondary dependent variables along with examples and nonexamples. Observers practiced collecting data using videotaped examples until they met a minimum agreement of 80% on each adult and child behavior for three consecutive 3- to 6-min sessions.
Fidelity
Three different graduate students assessed implementation fidelity of training (skill and self-monitoring) using a researcher-made checklist. Fidelity was assessed during 100% of sessions via videotapes, with the exception of one session for dyad 2 due to a technology error resulting in loss of the video. The checklist evaluated training on each skill, indicating whether the researcher included direct instruction, model, and guided practice. In addition, procedural fidelity data were collected on the researcher during parent implemented sessions using a researcher made checklist. The checklist assessed the following procedural components: researcher provided parents with three tasks, researcher provided no instructions, and sessions concluded at the end of three tasks or when 30 min had elapsed. Graduate students were trained on use of each fidelity checklist using direct instruction accompanied by examples and nonexamples. Observers practiced using taped examples until they met a minimum agreement of 80% on three consecutive trials. Fidelity was 100% for all training and implementation sessions.
Social Validity
Immediately after meeting mastery criteria in the maintenance phase, parents completed the Treatment Acceptability Rating Form—Revised (TARF-R; Reimers et al., 1992), with “treatment” substituted with “training” or “strategies.” The TARF assesses acceptability and feasibility of the intervention with 20-items, each scored on a 7-point Likert-type scale. This assessment has adequate validity and reliability (Reimers et al., 1992; Harrison et al., 2016).
Interobserver Agreement
Interobserver agreement (IOA) for fidelity of training was assessed during 33.33% of training sessions. IOA was calculated on an item-by-item basis during each training by calculating the frequency of training steps coded as implemented by one observer divided by frequency coded by a second observer and multiplying by 100. Mean IOA across training sessions was then calculated. IOA for training fidelity was 100% for dyads 1 and 2.
IOA for parent and child behavior was assessed during a minimum of 33% of parent implementation sessions within each phase (i.e., baseline, training, maintenance, and self-management). If reliability fell below 80% on parent or child behavior, coders were provided an additional training session. One additional training was required for the two primary coders during the training phase for family dyad 2. IOA for parent and child behavior was assessed for each session on an interval-by-interval basis by dividing intervals with occurrence and nonoccurrence agreement by the total number of intervals and multiplying by 100. Mean IOA across sessions was then calculated by summing percentage of IOA for sessions and diving by number of sessions. Mean IOA for parent behavior for dyad 1 was 98% (range = 91%–100%) and for dyad 2 was 96% (range = 85%–100%). Mean IOA for child behavior for dyad 1 was 98% (range = 95%–100%) and for dyad 2 was 94% (range = 64%–100%).
Experimental Design
A multiple baseline across skills design was used for each parent, followed by sequential implementation of self-monitoring, if needed. Baseline continued for a minimum of five sessions and until a stable or decreasing trend was observed in the first tier. The first skill was moved to the intervention phase while continuing baseline in tiers 2 and 3. Once the skill in tier 1 was stable within the intervention phase, intervention was implemented in tier 2. These procedures continued until intervention was applied to all three skills.
Procedures
General
Throughout all phases, each parent/child dyad engaged in three activities during each session. Activities were predetermined by the parent and researcher that ensured adequate opportunities to exhibit each skill and allowed opportunities to adapt the strategy for use in various situations. Activities selected based on need reported by the parent included setting up for homework, packing lunch for school, packing backpack for school, cleaning up toys, taking vitamins, completing a household chore (i.e., putting laundry away and setting kitchen table), and nighttime routine (brush/floss teeth). All sessions were conducted 1 to 3 days each week and lasted until the activity was completed or 30 min elapsed.
Baseline
During baseline, parents engaged in the three predetermined activities. Parents were provided with a general prompt to complete the activity (e.g., “Have your child complete the three tasks), without any additional instruction or directives.
Intervention
Intervention training occurred in one-to-one sessions with the researcher and parent participant. The child was present for the guided practice component. Throughout the training phase, sessions followed a systematic procedure consisting of direct instruction, model of the skill, and guided practice and occurred within a 1-hr time frame. During direct instruction, the researcher provided the parent with a written description of each skill that included “What” (definition and description of the skill with an example and nonexample), “Why” (rationale for use, description of how the practice benefits the child) and “How” (instructions of how to implement the skill, in what context, providing an example and nonexample) and described information on the handout to the parent using a predeveloped script. The researcher then modeled how to implement the skill (e.g., “I will show you how to positively praise Jerome like we just learned. I love how you put the toys away when you were done playing.”). Finally, during guided practice, the researcher provided an opportunity for the parent to practice the skill with their child. If the parent did not demonstrate accurate implementation of the strategy, feedback was provided.
Parent implementation sessions occurred immediately following each training session. The researcher activated the camcorder to record the session. No instruction or interaction was provided other than an initial cue (i.e., “Please have your child complete [activity/activities]”). Training continued prior to each session until the parent met a pre-established criterion for each specific skill. Criterion for verbal praise was 0.8 per min across the session. Criterion level for dichotomous choice was 0.5 per minute across the session, while setting expectations was two correct out of three opportunities. After the parent met criterion for a skill for a minimum of three consecutive sessions, the maintenance phase was introduced.
Maintenance
Maintenance was assessed after intervention ended for each specific skill. During this phase, no training occurred for the skill, and only the directive to complete the activity/activities with their child was provided. The maintenance phase remained in place for a minimum of five sessions, unless a skill decreased to below the training criterion level, in which case maintenance enhancement was introduced.
Self-Monitoring
Self-monitoring procedures were introduced in a staggered manner, maintaining the multiple baseline design. Parents were taught to self-monitor implementation of skills during sessions with their child. Training occurred using the same procedures as intervention for the first session in each phase. Specifically, parents were provided direct instruction on the self-monitoring tool (description, purpose, and rationale), the researcher modeled use of the self-monitoring tool, and the parent participated in guided practice. Upon completion of the training parents continued sessions independently, without the researcher present. This phase concluded after each targeted skill returned to pre-established mastery levels for a minimum of three sessions and five data points.
Data Analysis Procedures
To answer Research Question 1 regarding skill acquisition, data for parent skill implementation were examined to determine whether parents reached criterion level for each skill. To answer Research Question 2, parent maintenance of skills, data were evaluated to determine whether skills remained at the mastery criterion level. To answer Research Question 3, effects of self-monitoring, data were evaluated to determine whether skills returned to previously attained mastery levels for a minimum of three sessions. Changes in the two secondary dependent measures (child engagement and problem behavior) were evaluated, examining trends, level, variability, immediacy of effect, overlap, and overall consistency. In addition, effect size was calculated using Tau-U. Effect size was interpreted as small (<0.65), medium to high (0.66–0.92), or strong (0.93–1), as recommended by Parker and Vannest (2012).
Results
Jane
Data for Jane are presented in Figure 1. During baseline, Jane demonstrated no occurrences of specific praise or setting expectations and one occurrence of dichotomous choice. Following four parent training intervention sessions, Jane’s use of behavior-specific praise met criterion each session, increasing from zero in baseline to a mean of 2.03 per min (range = 1.4–3) in training. For setting expectations, five training sessions were conducted, during which Jane consistently met criterion, increasing from zero in baseline to three in training. Similar changes were observed for dichotomous choice, which also met criterion after each of the four training sessions, increasing from a mean rate per min of .008 to 1.47 (range = 1.25–2).
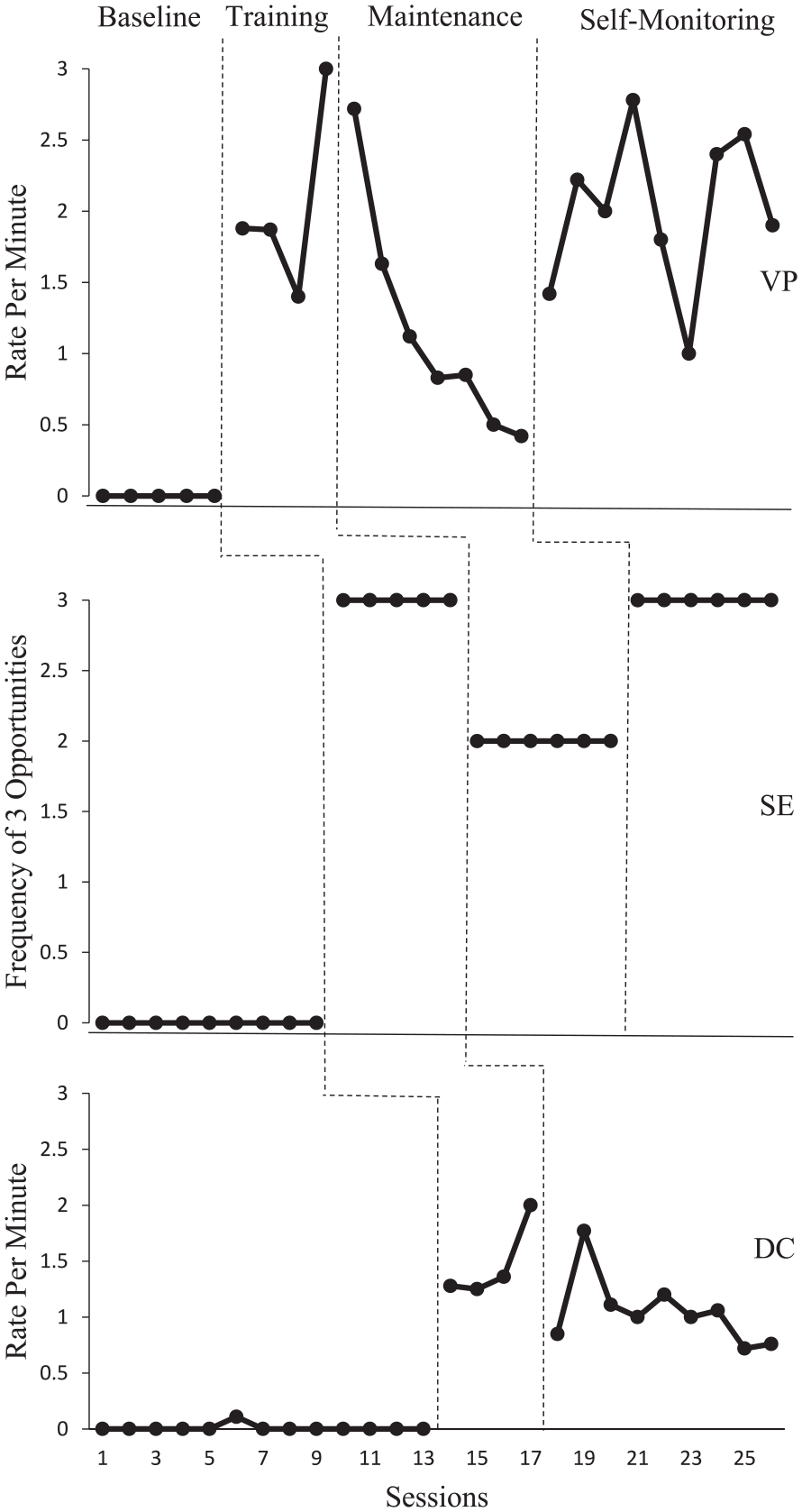
Jane’s Implementation of Three Skills
Jane’s use of two skills decreased immediately during maintenance, when training was discontinued. For behavior-specific praise, rate per min decreased from a mean of 2.03 in training to a mean of 1.15 in maintenance (range = 0.42–2.72), showing a downward trend. Setting expectations decreased from three occurrences in training to a mean of two in maintenance. Although this met criterion, the self-monitoring tool was provided with the goal of improving setting expectations from 2 to all 3 tasks as demonstrated in training. The mean rate per min of choice was 1.47 in training and remained relatively stable at a rate of 1.05 during maintenance (range = 0.72–1.77).
During the self-monitoring phase, although some variability was observed, the rate per min of behavior-specific praise consistently met criterion, increasing to a mean of 2 (range = 1–2.78), with a reverse in the decreasing trend observed during maintenance. Setting expectations increased from a mean of two occurrences in maintenance to three, restoring the skill to training-level performance. Overall, following self-monitoring, all three skills met criterion.
Tau-U was calculated using the web-based calculator for single-case analysis (Version 2.0; Vannest et al., 2016). Tau-U for behavior-specific praise comparing baseline to training indicated a strong effect (Tau = 1). For setting expectations, Tau-U calculations indicated a strong effect from baseline to training (Tau = 1). Last, choice baseline to training showed in a strong effect (Tau = 1).
As parents used the form consistently for each session, to assess the accuracy of self-monitoring, the data collectors’ coding sheets were compared to the electronically saved parent-completed self-monitoring sheets. Accuracy was assessed for praise by calculating total frequency agreement with the coder. Jane’s self-monitoring accuracy averaged 89.2% (range = 73%–100%). Setting expectations accuracy was coded if both Jane and the coder recorded accurately setting an expectation at the beginning of each new task. Jane’s accuracy for setting expectations was 100% for all self-monitoring sessions.
Mary
Data for Mary’s parent skills are presented in Figure 2. During baseline, Mary did not demonstrate any occurrences of specific praise. Her rate increased to a mean of 1 per min during training (range = .94–1.04), meeting criterion after three sessions. Similarly, dichotomous choice did not occur in baseline, but increased to a mean rate per min of .87 (range = 0.25–1.71) during training, meeting criterion after four training sessions. The mean number of accurate expectations increased from a mean of 0.16 in baseline to a mean of 2.5 during training, meeting criterion after all five training sessions.
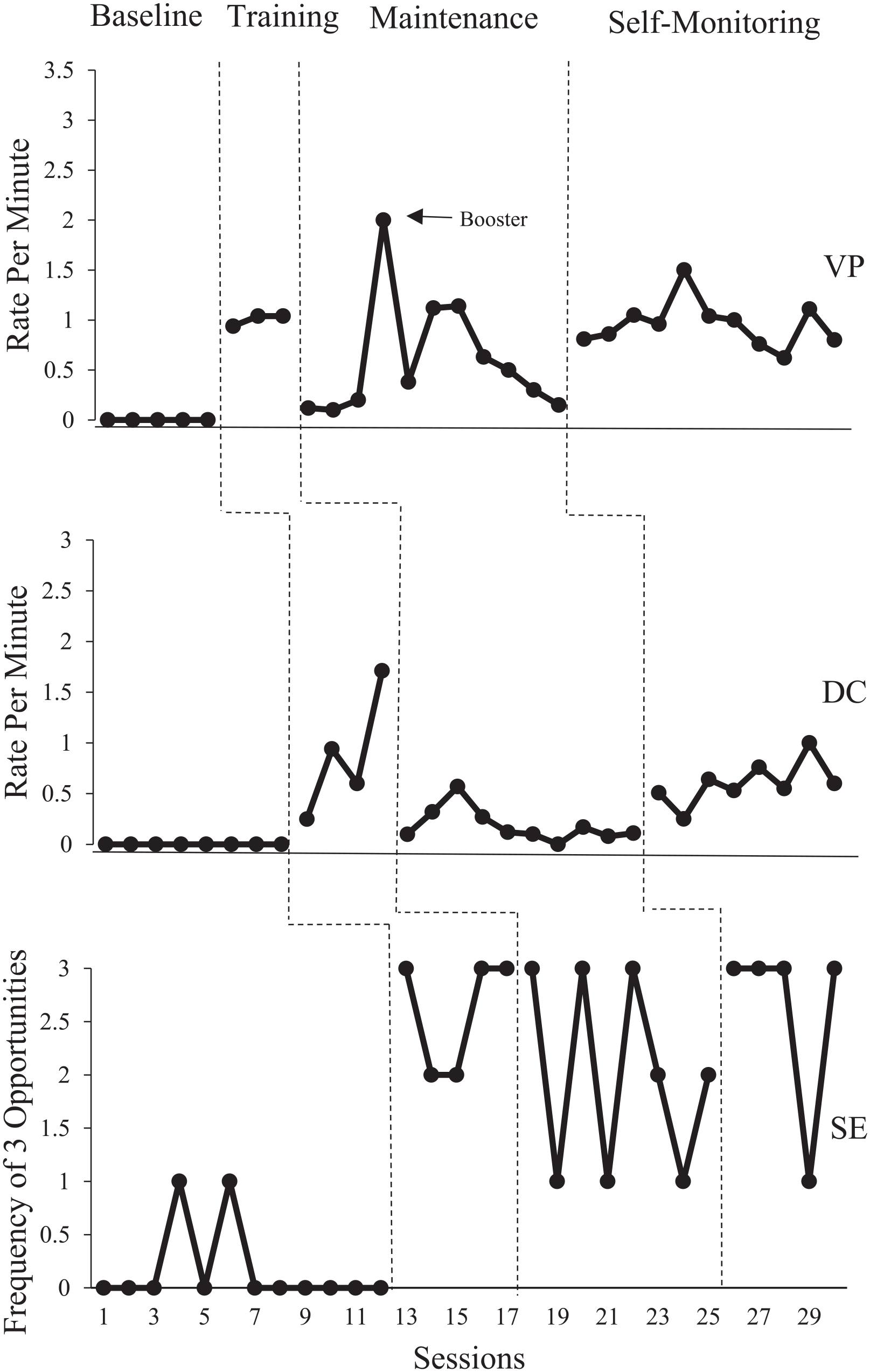
Mary’s Implementation of Three Skills
Mary’s use of two strategies (verbal praise and dichotomous choice) decreased immediately in the maintenance phase. For behavior-specific praise, rate per min decreased from 1 in training to a mean of 0.42 in maintenance (range = 0.1–2). Due to this immediate-level change, a booster session was implemented in order to determine whether additional training would result in an increase in praise. The booster (conducted session 4) increased praise to rates similar to training; however, data from the subsequent sessions indicated behavior change did not maintain. For dichotomous choice, the mean rate per min of .87 in training decreased to a rate of 0.18 (range = 0.1–.57) in maintenance. Setting expectations resulted in a stable mean of 2.5 in both training and maintenance (range = 1–3).
As skills did not meet criterion, self-monitoring was introduced. In the self-monitoring phase, for behavior-specific praise, criterion was met during nine sessions, with rate per min increasing from a mean of 0.42 to a mean of .95 (range = 0.62–1.11). Dichotomous choice showed an increasing trend, with criterion met during seven sessions. Choice increased from a mean of .18 in maintenance to .60 in self-monitoring (range = 0.25–0.76). Setting expectations increased from a mean of 2 in maintenance to a mean of 2.6, meeting criterion in all but one session.
Mary’s self-monitoring accuracy averaged 70% (range = 33%–100%) for verbal praise, and 77 (range = 43%–100%) for choice. Mary’s mean accuracy for setting expectations was 85% (range = 50%–100%).
Tau-U for behavior-specific praise baseline to training resulted in a strong effect (Tau = 1). For choice from baseline to training a strong effect was demonstrated (Tau = 1). Tau-U for setting expectations resulted in strong effect from baseline to training resulted (Tau = 1).
Jerome
Jerome’s data are presented in Figure 3. Jerome’s mean engagement during baseline was 18.2% (range = 9%–30%), which increased to 83.11% (range = 63%–100%) during intervention. Jerome’s mean problem behavior during baseline was 32.8% (range = 18%–50%) and decreasing to 2.36% (range = 0%–13%) during intervention. Tau-U indicated a strong effect for both engagement (Tau = 0.95) and problem behavior (Tau = 1).
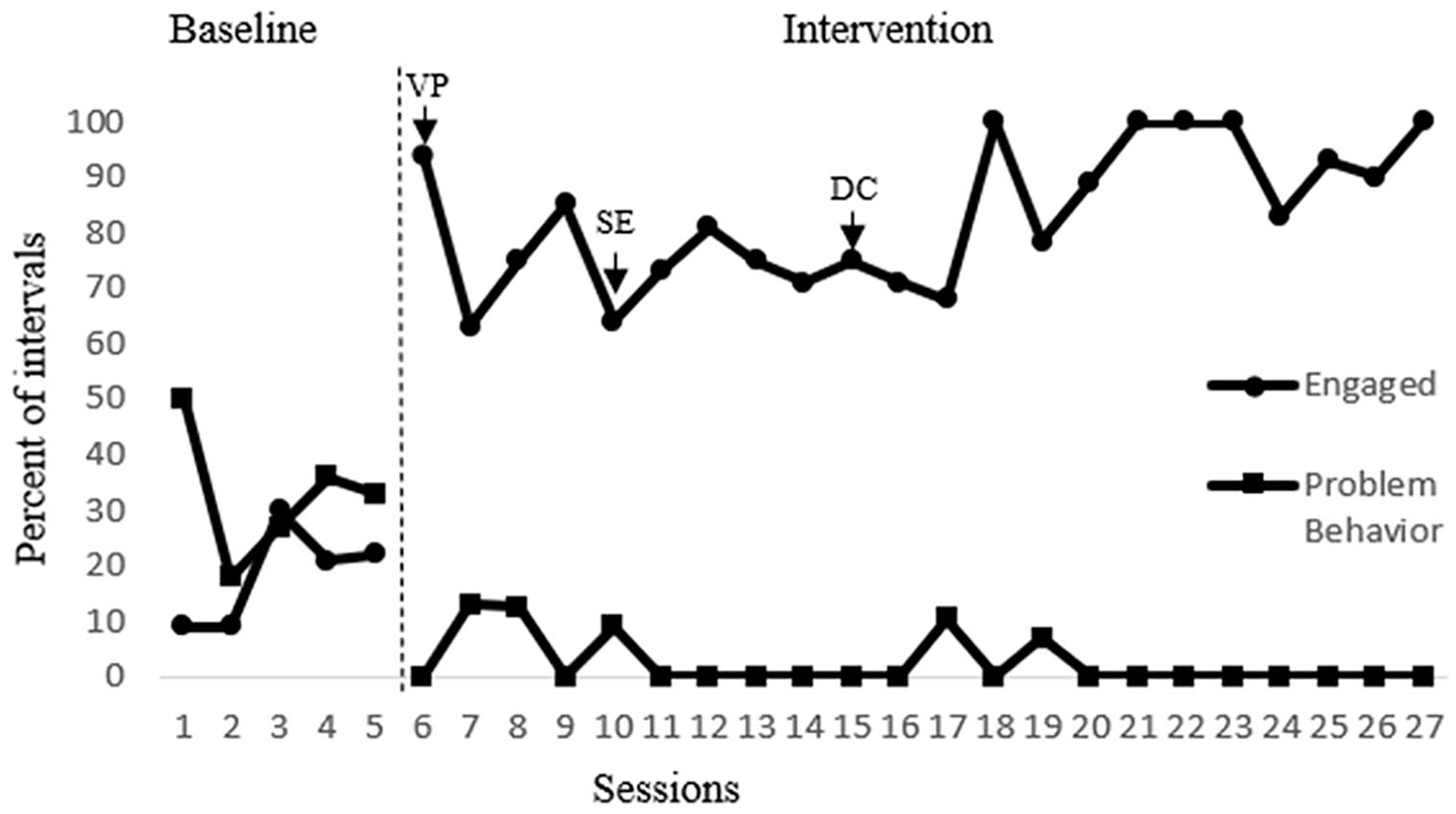
Jerome’s Behavior
Mason
Data for Mason are presented in Figure 4. Mason’s mean engagement behavior during baseline was 39.65% (range = 25%–70.58%), increasing to 84.60% (range = 50%–100%) during intervention. Mason’s mean problem behavior during baseline was 27% (range = 11.76%–37.5%) and decreasing to 2.02% (range = 0%–14%) during intervention. Tau-U calculations indicated a strong effect for both engagement (Tau = 0.93) and problem behavior (Tau = 0.98).
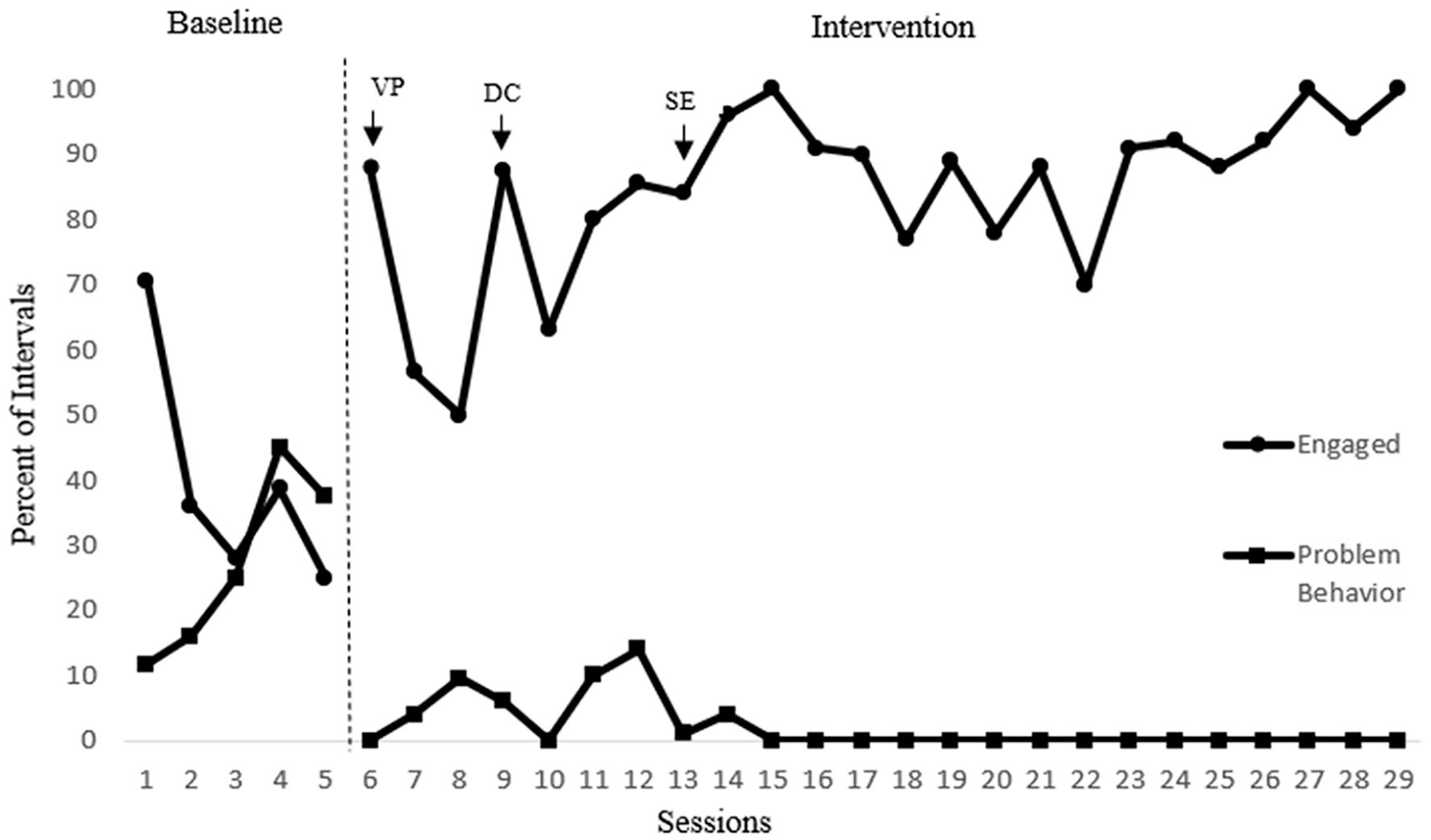
Mason’s Behavior
Social Validity
Total scores on the TARF-R for Jane and Mary were 91 and 88, respectively, indicating high acceptability according to the following range categories: high acceptability = 85–119, average acceptability = 52–84, and low acceptability = 17–51 (Mandal et al., 2000).
Discussion
The purpose of this study was to evaluate parent mastery and maintenance of three behavior support strategies implemented during typical household activities. A further purpose was to assess the effectiveness of self-monitoring to increase skills that did not maintain. This was used as an alternative to traditional boosters that target skill deficits rather than performance deficits.
Findings from the first research question, regarding parent’s ability to master the skills using general teaching strategies, are consistent with Barton and Fettig’s (2013) and provide additional support for the continuation of behavioral skill training. Furthermore, the brevity of training (3–5 sessions, 1 hr each maximum) is consistent with the brief training required by Lane et al. (2016) (i.e., 3–7 1-hr sessions for each of the 3 skills). This study extends Lane et al. by teaching different skills to parents, using naturalistic approaches in the home setting, and targeting a different population of children. In addition, Lane et al. (2016) called for investigation into parents’ ability to demonstrate skills outside of clinician presence to better understand the lasting effectiveness of brief training packages; something this study incorporated.
The second research question, continuous and on-going assessment of maintenance, was intended to address a critical gap in the parent-training literature (Barton & Fettig, 2013; Roberts & Kaiser, 2011; Moore & Symons, 2011). Although results differed across skills, all but one skill for one parent declined below criterion, with many reaching near baseline levels. This is consistent with findings from Moore and Symons (2011), who reported a decrease in all but one skill, two of which were the same used in this study. Trends in skill maintenance also differed across parents and skills. For example, Jane demonstrated a gradual decrease in praise while Mary tended to demonstrate more immediate decreases as well as more variability. This finding supports the need to move toward more methodical measurement of maintenance, rather than conducting periodic probes. For instance, parents who demonstrate rapid skill dissipation might need self-monitoring immediately after training while intermittent self-monitoring might be sufficient when skills gradually decline over time. Future research might examine alternative strategies to ensure maintenance in a manner that requires the least effort from parents and clinicians. Individualizing follow-up strategies could also be a cost-efficient approach for maintaining parent skills (Van Camp, Montgomery, et al., 2008).
Regarding the third research question, self-monitoring was effective for increasing parent implementation of all targeted skills. This is consistent with findings of positive effects of self-monitoring on implementation fidelity for teachers (Pinkelman & Horner, 2017; Rispoli et al., 2017) and may assist in answering an early question posed by Sanders and Glynn (1981), which was to determine whether self-monitoring was a critical feature of the self-management package used with parents. Furthermore, the failure of a booster session implemented with one parent supports targeting diminishing parent skills as performance deficits instead of skill deficits, for which self-monitoring is well aligned.
Providing a feasible parent training package that is both successful in teaching skills and also supports maintenance is valuable only if it has a positive impact on child behavior. As such, child engagement and problem behavior, evaluated as secondary variables, and showed substantial improvements. In addition, Jane anecdotally reported substantial improvements in Jerome’s responsiveness to directives and independence with task completion. To confirm this parent report, changes in the mean amount of time it took to complete the three activities was assessed. Duration of task completion decreased from a mean of 11 min in baseline to a mean of 7.5 min in intervention. Analysis of videos suggests this was due to elimination of refusal behavior, decreased latency to begin tasks, and increased independence with tasks. Similarly, Mary reported substantial improvements in Mason’s responsiveness to directives and parent–child positive relationship, which she attributed to her use of positive praise and attention.
In spite of the favorable findings, several limitations should be considered. First, parent training was conducted by the researcher and should be replicated by a community-based interventionist who typically delivers home-based behavioral support. Second, parents were taught to implement procedures across three tasks. Thus, generalization to novel tasks was not assessed. Future research might determine the minimal number of skills that need to be taught to occasion generalization. In addition, results indicated effectiveness for single mothers of children, ages 10 and 11, diagnosed with high-incidence disabilities. As such, results cannot be generalized to low-incidence populations or alternative family structures. Finally, mothers in the study reported higher than average educational levels; therefore, future research with parents of diverse demographics is recommended.
The findings have immediate implications for practice. First, practitioners should adequately train so that failed maintenance is not a result of skill deficits. Simultaneously, practitioners are encouraged to incorporate self-monitoring strategies into behavioral skills training to increase skill maintenance. This may be particularly easy and cost-efficient for skills that are relatively simple to teach, such as those used in this study.
In summary, this study strengthens the parent training literature by demonstrating the effectiveness self-management for improving maintenance of parent implemented support strategies following behavioral skills training. Importantly, parents rated the intervention as feasible and acceptable. Additional research is needed to further assess maintenance over an extended period. In addition, extensions of this study are important to identify permutations of self-management to best promote long-term adherence and sustainment of parent skills.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.