
Abstract
This study controls for officer characteristics (i.e., age, race, children living in the home, relationship status, time in policing, military experience, community size, and country) while examining the effects of critical incidents, social stressors, and coping on alcohol use and posttraumatic stress disorder among men (N = 1,144) and women (N = 309) using self-report surveys from an international sample of police. Gender differences were found in the Alcohol Use Disorders Identification Test but not in posttraumatic stress disorder models. The critical incidents by coping by social stressors three-way interaction was significantly associated with men’s, but not women’s, drinking, and the effects of critical incidents were positive for men but negative for women.
Introduction
Law enforcement is recognized as one of the most stressful occupations (Swanson, Territo, & Taylor, 2012). Police officers are continuously exposed to critical incidents, they are criticized and stigmatized, and they do not always receive support from their superiors or the public. Further, they work irregular hours, which may make social support to deal with these problems less available and can be a stressor itself (e.g., family resentment due to missed holidays and special occasions). Research suggests critical incidents and other work-related stressors can lead officers to use maladaptive coping strategies, such as avoidance (Pasillas, Follette, & Perumean-Chaney, 2006), and to suffer negative outcomes, such as alcohol problems (Swatt, Gibson, & Piquero, 2007) and posttraumatic stress disorder (PTSD; Marmar et al., 2006; Weiss et al., 2010).
Although a number of studies have examined the links between critical incidents and the development of alcohol problems and traumatic symptoms, much of the work was completed with men and so less is known about these relationships among policewomen. Given research finds male and female officers experience different stressors and respond to such stressors with different coping strategies (He, Zhao, & Archbold, 2002), it is possible that gender differences in the relationships between stressors and their outcomes exist. To that end, the current study examines gender differences in the effects of stressors (experiential and social) and negative coping on alcohol problems and PTSD symptoms among an international (primarily United States, Canada, United Kingdom, Australia, and New Zealand) sample of police officers.
Women in Policing
Policewomen are a fairly new phenomenon for agencies in the United States and abroad. Four decades ago, there were very few female officers (Martin & Jurik, 2007). This situation changed with the introduction of civil rights laws. In 1969 in the United States, President Richard Nixon issued an executive order declaring the federal government could not use gender as a qualification for hiring, resulting in federal law enforcement agencies hiring women. In 1972, the Equal Employment Opportunity Act was passed by Congress, which extended the provisions of the Civil Rights Act to local police departments (Price & Sokoloff, 2004). Similar antidiscrimination laws were passed in Britain in 1975 (Sullivan, 1979), and in Australia (Foreman, 1978) and Canada in 1977 (LeBeuf, 1996), removing barriers to women in policing. Women represent 20% of sworn officers in the United States (Bureau of Justice Statistics, 2010) with comparable rates found in other countries (e.g., 20% of officers in Canada, Burczycka, 2012; 26.8% in the United Kingdom, Home Office, 2012; 16.7% in New Zealand, Mossman, Mayhew, Rowe, & Jordan, 2008; and 32.5% in Australia, Productivity Commission, 2013). Despite the growth in their numbers, women are still minorities within the profession, a status that likely contributes to the stress of the job. The recency and uniqueness of this status and their smaller numbers mean less is known about how women cope; thus, research is warranted.
Stress in Policing
Both male and female police officers face stress from organizational characteristics (Morash, Kwak, & Haar, 2006), from exposure to critical incidents (Weiss et al., 2010), and from social stressors (Arter, 2008; Arter & Ménard, 2012). While the literature indicates organizational stressors are reported at higher levels than are experiential stressors (Buker & Wiecko, 2007; Morash et al., 2006), critical incidents and other stressors are more frequently associated with negative outcomes, such as alcohol use and PTSD (Ballenger et al., 2010; Weiss et al., 2010). However, the relationship of gender to these outcomes is not clear, as will be discussed later.
Police officers face exposure to critical incidents capable of creating both stress and aversive reactions to stress. Critical incidents include those situations outside the usual range of experiences of a police officer and that have the potential to overwhelm the officer’s psychological defense and coping mechanisms. Some of the most profound and stressful law enforcement critical events include the violent death of a partner, taking a life or shooting someone in the line of duty, and duty-related violent injury (Weiss et al., 2010).
The social stressors of policing can also negatively impact officers’ well-being (Marmar et al., 2006; Ménard & Arter, 2013). Social stressors include rejection by friends, isolation and consequent resentment from family (due to shift work), and stigmatization and abuse from the public or superiors (e.g., Anshel, 2000; Arter, 2005). Both male and female officers experience these types of stressors, but not necessarily at the same rate, and they may respond differently to them. Research finds policewomen report higher levels of stress and different stressors than do their male counterparts (He, Zhao, & Ren, 2005; Morash et al., 2006).
Some of the unique stressors policewomen face include sexism, negative attitudes and disapproving responses, lack of role models and mentoring, demands to prove themselves, and lack of acceptance by the policing subculture and even by their own friends and families (McCarty, Zhao, & Garland, 2007). Kurtz (2008) found women officers are more likely to report they were treated differently by administration due to their gender. Compared with males, females also experience significantly more problems with underestimated physical ability, perceived lack of influence on how policing gets done, bias, language harassment, and sexual harassment (Morash et al., 2006).
Female officers also report stress resulting from problematic family relationships at higher levels than do males and indicate that stress from law enforcement duties is related to family and partner relationship problems (Piquero, 2005; Thompson, Kirk, & Brown, 2005). These social stressors or lack of social support may exacerbate trauma symptom severity. Research shows officers with poor social support report more severe symptoms of PTSD (Marmar et al., 2006; Stephens, Long, & Miller, 1997). Thus, women may experience greater stressors from both an unsupportive workplace and resentful social network substantially challenging their ability to cope, which may differentially affect their outcomes, including alcohol problems and PTSD symptoms.
Coping
In addition to critical incidents and social stressors, coping strategies are important in how police officers react to, and deal with, stress. Lazarus and Folkman (1984) define coping as “constantly changing cognitive and behavioral efforts to manage specific external and/or internal demands that are appraised as taxing or exceeding the resources of the person” (p. 141). Research finds male and female officers not only view stressful stimuli differently, they adopt different coping strategies when under stress (He et al., 2002, 2005; McCarty et al., 2007). A meta-analysis with general population samples finds women are more likely than men to engage in coping strategies (Tamres, Janicki, & Helgeson, 2002). Yet, research with police officers “showed that dynamic factors such as measures of work environment and coping mechanism contributed more in explaining police stress than static factors such as race and gender” (He et al., 2005, p. 535). This result suggests that for police, coping strategies may be more important than gender when responding to stress.
Although some officers use adaptive coping strategies (e.g., exercise) to deal with stressors, others use maladaptive ones (e.g., dissociation, suppressing, and avoidant behaviors) that may lead to problems (Ballenger et al., 2010; Pasillas et al., 2006; Violanti et al., 2011). Avoidant coping is considered the least effective coping strategy (Ben-Zur, 2009; Carver, Scheier, & Weintraub, 1989), yet it is the method most consistent with police subculture that shuns showing weakness (Blau, 1994) and encourages another form of maladaptive coping—alcohol use (Violanti et al., 2011).
Alcohol Use
Alcohol was cited as one of the primary coping strategies of police officers in dealing with work-related stressors (Violanti et al., 2011). The police subculture encourages the use of alcohol; in many instances, drinking is expected by colleagues (Lindsay & Shelley, 2009), and there is significant social pressure to conform (Swanson et al., 2012). Indeed, Lindsay and Shelley (2009) found that fitting in was one of the most prevalent reasons cited by officers for drinking. Although population samples (Kessler et al., 2005) and some police samples (Davey, Obst, & Sheehan, 2000; Violanti et al., 2011) find women have lower rates of alcohol use and abuse, results are inconsistent. For instance, Ballenger et al. (2010) using self-report data from 746 officers found significant gender differences in the current at-risk category (16% women vs. 11% men) but not in the lifetime use or binge drinking categories. Further, in the multivariate model predicting current alcohol use, there were no significant gender effects for critical incidents, but female officers were less likely to drink than males under greater conditions of workplace stress. Thus, although both men and women drink consistent with the policing subculture, their reasons for doing so may differ.
Posttraumatic Stress Disorder
PTSD has been identified as one of the most significant outcomes related to stress in policing. Studies on this phenomenon indicate between 7 and 19% of officers surveyed met the criteria for PTSD (Carlier, Lamberts, & Gersons, 1997; Marmar et al., 2006). Although consistently high rates of PTSD among police have been found, the effects of gender are more complex.
Research with police samples produce inconsistent results with some studies reporting no gender differences in rates of PTSD (Ballenger et al., 2010; Pole et al., 2001) and other studies reporting higher rates among women (Bowler et al., 2012). General population samples also find higher rates of PTSD among women than men (Tolin & Foa, 2006). A review by Tolin and Foa (2006) indicates that even though women experienced fewer potentially traumatic events than did men, their odds of meeting criteria for PTSD were twice as high as those of men. This difference may be due to women’s higher rates of sexual abuse when compared with men’s (Koenen & Widom, 2009). Alternatively and referring specifically to policewomen, it may be due to the different ways in which they respond to stress. One study comparing female officers to female civilians found that group differences in PTSD (civilians had higher rates) were explained by higher levels of peritraumatic emotional distress among civilians (Lilly, Pole, Best, Metzler, & Marmar, 2009). Thus, policewomen may respond more like their male colleagues, suppressing emotional response to traumatic events in keeping with subcultural values to do so.
In sum, both male and female officers are exposed to critical incidents and social stressors, although the number and responses to these stressors may differ. Further, in spite of the fact that consistent gender differences exist for alcohol and traumatic problems among the general population (women having lower rates of alcohol problems and higher rates of PTSD), these differences are inconsistent among police officers. Failure to find these patterns may be due to differences in coping strategies as encouraged by the policing subculture. Based on the previously mentioned literature review, we anticipate that negative coping will exacerbate the effects of critical incidents and social stressors on male officers’ drinking and trauma, but there is too little consensus in the research to predict their effects on females.
Method
Procedures
Officers were recruited and invited to complete the survey online. Well-known police organizations (e.g., International Association of Chiefs of Police and Fraternal Order of Police) were identified using a Google search of terms such as “police officer association.” Specific searches for police associations were completed for each of the six most populous states in the United States (i.e., California, Texas, New York, Florida, Illinois, and Pennsylvania). Because of their common language, heritage, and evolution as it relates to women in policing (Dempsey & Forst, 2010; Segrave, 2014), these same searches were completed for four additional countries (i.e., Canada, United Kingdom, Australia, and New Zealand). Finally, for all states and countries, searches of underrepresented groups (e.g., women, African American, Hispanic, and Asian) were also completed (e.g., Asian police officer association in Canada). One hundred twenty-five organizations were identified (65 within and 60 outside the United States), sent information regarding the survey (i.e., a brochure via e-mail or regular post), and asked to disseminate the information to their members as well as other officers. Additional subjects were also recruited by sending the same information and request to 35 police officers and agencies in Canada and the United States known to the authors. 1 Officers were informed the survey was online, confidential, anonymous (only identifier was country), and approved by the investigators’ university institutional review board. Officers had to indicate their understanding of their rights as research participants by agreeing to an electronic consent form to gain access to the survey.
Participants
The original sample comprised 1,582 officers from 13 different countries. Missing data on respondents’ sex reduced the sample to 1,453, and the use of listwise deletion further reduced the sample in the multivariate models. Because it cannot be known how many officers were provided with the information to the survey, it is impossible to compute a response rate. However, we can track that 82.3% of those who accessed the survey completed it. Almost 79% of participating officers were male, and slightly more than 93% were White, with 2.5% Black, 0.8% Asian, 2.9% Latino/a, and 1.1% of other or mixed racial or ethnic background. The average age of respondents was 42.04 years (range 20.00–77.00, SD = 9.62), and they averaged 18.29 years in policing (range 0.00–50.00; SD = 9.67). Our sample is not random and underrepresents younger, women, and minority police officers. Given we recruited officers via police associations, it may be that these officers are not as active in associations as their older, male, Caucasian counterparts.
Measures
Ten items from Weiss and colleagues’ (Weiss et al., 2010) Critical Incidents Questionnaire, including “being shot at,” “being threatened with a gun, knife, or other weapon,” “a colleague being injured” or “killed,” and “seeing someone die,” were used to represent this construct. Each item was rated from 0, indicating officers never experienced the incident described, to 6, indicating they experienced it 50 or more times in their life. These items were summed to indicate officers’ experience with critical incidents (α = .79 for men and .71 for women). Police officers were also asked if they experienced any of six social stressors (e.g., lost previously enjoyed social contacts, enjoy social contacts with civilians other than family—reverse coded, difficulty establishing relationships, lack of understanding from civilians, negative stigma associated with law enforcement, and lost friendships since becoming an officer). Although an open-ended format was used on the survey, because the majority of officers replied with “yes” or “no” answers, these variables were recoded (dichotomized) to indicate whether the officer experienced these social stressors. The sum of these items was used to represent the total number of social stressors officers experienced (α = .60 for men and .57 for women). Because we were primarily interested in officers’ negative coping strategies (e.g., escape-avoidance), we used 16 items from the 66-item Ways of Coping Questionnaire—Revised (Folkman & Lazarus, 1985), including “criticized or lectured myself,” “refused to believe that it had happened,” “tried to make myself feel better by eating, drinking, smoking, using drugs or medication, etc.,” and “took it out on other people.” 2 Each coping strategy was rated on a 4-point scale from 0 “never used” to 3 “used a great deal.” The items were summed to represent officers’ negative coping strategies (α = .87 for both men and women).
Two dependent variables were used in the analyses. First, officers’ alcohol use was measured using the Alcohol Use Disorders Identification Test (AUDIT; Babor, Higgins-Biddle, Saunders, & Monteiro, 2001). The AUDIT is a validated and reliable instrument designed to screen for harmful patterns of alcohol consumption. This scale includes items such as “How often during the last year have you needed a first drink in the morning to get yourself going after a heavy drinking session?” and “How often during the last year have you been unable to remember what happened the night before because you were drinking?” Each of the 10 items has a score range of 0 (no or never) to 4 (daily or almost daily). Because we were interested in alcohol use in a statistical model, rather than as a clinical diagnostic screener, we summed the items to create a dimensional measure, with higher scores representing more problematic drinking (α = .79 for men and .81 for women). Second, officers’ PTSD symptoms were measured using the PTSD Checklist – Civilian (PCL–C; Weathers, Huska, & Keane, 1991). The PCL–C is a valid and reliable 17-item self-report measure that asks about symptoms in relation to “stressful experiences” the respondent ever experienced. Sample items include “How much have you been bothered by avoiding activities or situations because they reminded you of a stressful experience from the past?” “How much have you been bothered by repeated, disturbing dreams of a stressful experience from the past?” and “How much have you been bothered by feeling jumpy or easily startled?” The PCL–C can be scored using diagnostic cutoff criteria or as a total symptom severity score, and the latter was used in this study (α = .92 for both men and women).
We also controlled for a number of variables. Because research finds alcohol problems and PTSD development vary by individual characteristics such as sex and race/ethnicity in the United States (Dawson, Grant, Chou, & Pickering, 1995; Kessler et al., 2005; Roberts, Gilman, Breslau, Breslau, & Koenen, 2011; Tolin & Foa, 2006), we controlled for officers’ sex (dummy coded), age (in years), and race or ethnicity (White or non-White). Also, because childrearing and marital status can affect well-being (Vanassche, Swicegood, & Matthijs, 2013), we controlled for whether officers had dependent children living with them full or part time versus those who did not have children or whose children were no longer living with them and for officers’ relationship status (single, divorced, or widowed vs. married or cohabitating). We also controlled for officers’ different time at risk and for potential prior trauma by including measures of officers’ time in policing (years) and military experience (yes or no). Because Federal Bureau of Investigation (2013) data suggest crime rates vary by population size (Table 16), we also controlled for the size of the community (using the nine Federal Information Processing Standards [FIPS] codes with 1 representing completely rural or less than 2,500 urban population, not adjacent to a metro area, and 9 representing counties in metro areas of 1 million population or more) in which officers work. Finally, because we had too few officers from countries outside the United States, we combined them (N = 615) and we controlled for country where officers work, with the United States serving as the reference group (U.S. N = 838).
Plan of Analyses
We first compared male and female officers’ scores or percentages on the dependent and the independent variables using t and chi-square tests. Then, Fisher’s r to z transformations were calculated on the bivariate correlations to conduct z tests to determine whether significant gender differences existed at the bivariate level. Next, because we were interested in gender differences, we ran separate Ordinary Least Squares (OLS) regressions with men and women officers’ alcohol use and PTSD symptoms treated as outcomes. 3 Because we anticipated that negative coping and social stressors may moderate the effects of critical incidents, we computed interactive terms (both two-way and a three-way) to examine their influence on these same outcomes. These interaction terms were added individually to the basic model, which comprised the demographic variables, critical incidents, negative coping, social stressors, and PTSD or AUDIT scores (Aiken & West, 1991). Finally, z tests (Paternoster, Brame, Mazerolle, & Piquero, 1998) were completed to determine whether the regression coefficients for men and women differed significantly from one another across the two outcome variables.
Results
Bivariate Analysis
Comparison of Men and Women’s Mean Scores and Percentages.
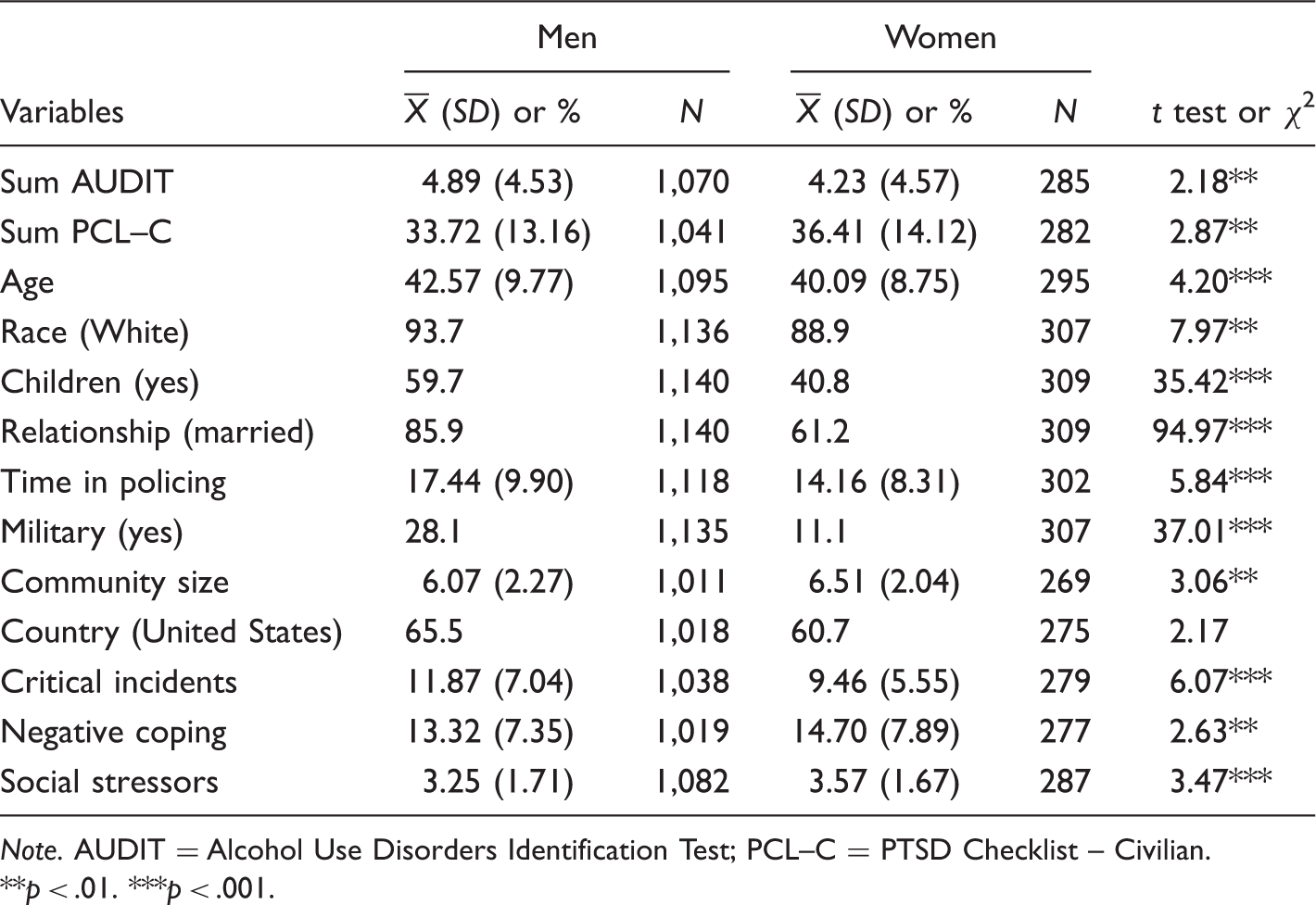
Note. AUDIT = Alcohol Use Disorders Identification Test; PCL–C = PTSD Checklist – Civilian.
p < .01. ***p < .001.
Correlation Matrix by Gender (Females on the Upper Diagonal).
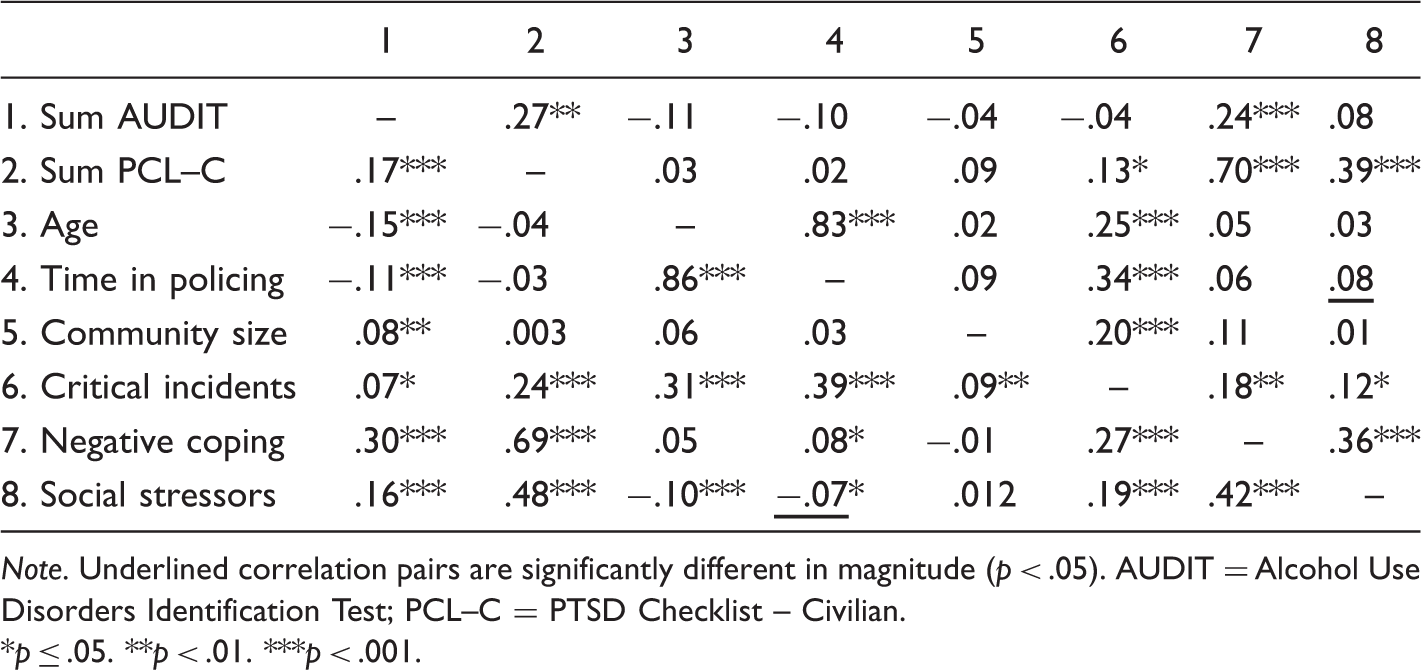
Note. Underlined correlation pairs are significantly different in magnitude (p < .05). AUDIT = Alcohol Use Disorders Identification Test; PCL–C = PTSD Checklist – Civilian.
p ≤ .05. **p < .01. ***p < .001.
Multivariate Analysis
OLS Regressions of Officers’ AUDIT and PCL–C (PTSD) Scores.
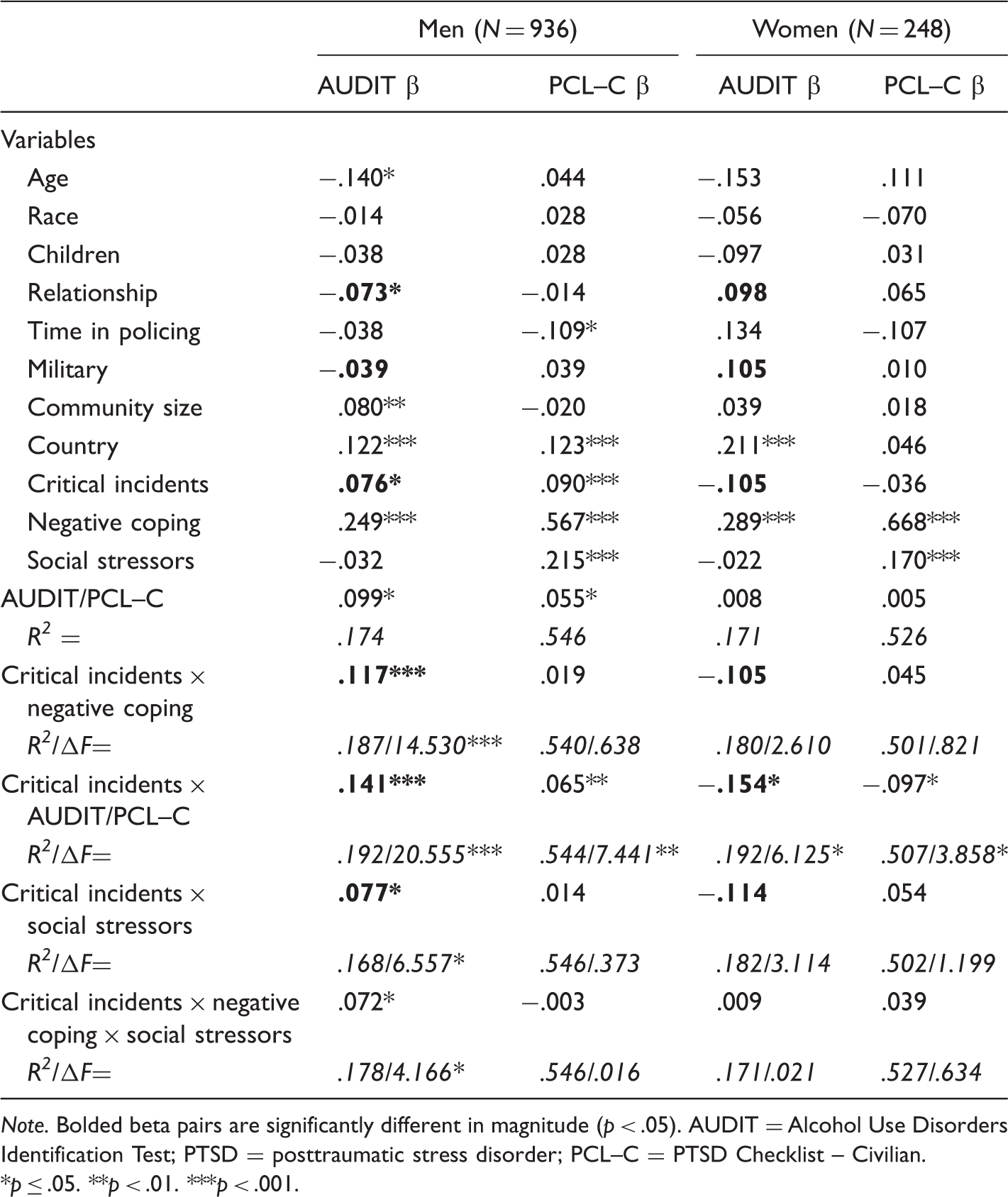
Note. Bolded beta pairs are significantly different in magnitude (p < .05). AUDIT = Alcohol Use Disorders Identification Test; PTSD = posttraumatic stress disorder; PCL–C = PTSD Checklist – Civilian.
p ≤ .05. **p < .01. ***p < .001.
Men
A number of factors were associated with male officers’ problematic drinking. Age, relationship status, and military experience were significantly and negatively associated, while critical incidents were positively associated with AUDIT scores accounting for 17% of the variance in this behavior. Further, among men, the three-way interaction of critical incidents by negative coping by social stressors was also significant, increasing the variance the model explained to 18%. This result suggests that those male officers with high scores on all three constructs may be especially likely to develop drinking problems. Fewer variables were significantly associated with PTSD symptoms, but the base model explained a substantial 55% of the variance in this behavior. Although time in policing was significantly and negatively associated with PSTD symptoms, being a non-U.S. officer with higher scores on critical incidents, negative coping, social stressors, and the AUDIT was significantly and positively associated with greater PTSD symptomology. The critical incidents by AUDIT interaction was significantly and positively related to PTSD, but none of the remaining interaction terms were significant.
Women
Although fewer variables were significantly associated with women’s AUDIT scores, the basic model explained 17% of the variance, the same percentage as for men. Coming from a country other than the United States and using negative coping was associated with higher AUDIT scores. Further, the critical incident by PCL–C interaction was significantly and negatively associated with drinking problems. The direction of the relationship is opposite to that found among men, and z test (z = 3.92, p < .001) indicates the difference in the regression coefficients is significant. Significantly different directional effects were also found for relationship (z = 2.58, p < .01), which was positive and not significantly associated with AUDIT scores among women (compared with negative and not significant among men), and military experience (z = 2.03, p < .05), which was positive and not significantly associated with AUDIT scores among women (compared with negative and not significant among men). Significant directional effects were also found for critical incidents (z = 2.31, p < .05) and its interaction with negative coping (z = 2.90, p < .01); both were negatively associated with AUDIT scores among women but were positively associated among men. With regard to PTSD, fewer variables were significantly associated with this construct, and the percentage of variance explained, 53%, was similar to that found among men. Higher scores on negative coping and social stressors were significantly related to PTSD. Although main effects for critical incidents on PTSD were not significant, the critical incidents by AUDIT interaction was significantly and negatively associated with PTSD. The direction of the effect was different for men and women, but z tests indicate these differences were not significant (z = 1.90).
In sum, results suggest somewhat different models predict men’s and women’s AUDIT, but not PTSD, scores. Critical incidents and its interaction with negative coping, PTSD, and social stressors are positively associated with men’s drinking problems but are negatively associated with this behavior among women. With regard to trauma, negative coping and social stressors are positively associated with PTSD for both genders, and, although critical incidents seem to have a different effect on men and women officers’ PTSD symptoms, these differences were not statistically significant.
Discussion
This study examined gender differences in police officers’ alcohol use and PTSD symptomology focusing on the effects of critical incidents, social stressors, and negative coping. Although there were some similarities in the relationship of these variables to drinking and PTSD across gender, there were also differences. Specifically, the effects of negative coping and social stressors were the same for both outcomes and genders, but the effects of critical incidents were not universal. Our results, as well as their implications and limitations, are discussed next.
We found 13.6% of male and 11.6% of female officers demonstrate problematic drinking, when using the AUDIT cutoff score of 8. These rates are consistent with some police studies that find females have lower rates than men (Davey et al., 2000; Violanti et al., 2011), but not with others (Ballenger et al., 2010). Given our sample is not representative (i.e., overrepresents older, White, male officers), these prevalence rates are not generalizable, but the data are better suited to the examination of predictive models that control for these differences. Consistent with prior research and police subculture (Anshel, 2000; Lindsay & Shelley, 2009; Swanson et al., 2012), negative coping was positively associated with officers’ AUDIT scores. Also, for both men and women, being from a country other than the United States was associated with higher AUDIT scores. Although few (if any) studies have examined differences in police officer alcohol consumption across countries, national data suggest the United States consumes less alcohol per capita (8.3 L) than many of the other nations included in this sample (i.e., Australia = 9.8, Canada = 7.8, U.K. = 11.2, and New Zealand = 8.9 L, respectively; NationMaster.com, 2013). The fact that country is significantly associated with drinking suggests the need for cross-country research to determine what elements of the nation contribute to this problem.
In spite of these similarities and that the amount of variance explained by our model was the same for men and women, z tests of the regression coefficients across gender find the relationships of several variables differed as well. The role of critical incidents and its interaction with PTSD symptoms on drinking is different for men and women. This effect is driven by critical incidents, which were associated with lower AUDIT scores among women and higher scores among men. This result suggests male and female officers respond differently to the stressors of policing, at least exposure to critical incidents. Whereas men may cope with critical incidents by using and abusing alcohol, critical incidents appear to reduce women’s problematic alcohol use. Our results appear to run counter to those of Ballenger et al. (2010), wherein gender by critical incident was positively associated with alcohol use but only approached standard levels of significance (p = .06). However, in their study, work stress was associated with lower current alcohol use by women when compared with men. As our only measure of work-related stress is “critical incidents,” our failure to include other measures of this stress may have confounded the effect. Research suggests that men and women police officers may experience different types of work stress (Piquero, 2005; Thompson et al., 2005). For instance, Piquero (2005) found females reported more stress from female-specific stressors (e.g., discrimination), whereas males reported more stress from typical elements of police work. Clearly, more research is needed to disentangle the effect different stressors of policing (e.g., organizational, critical incidents, emotional toll of the job—for instance, being a rape survivor and having to work the sex crimes unit) have on male and female officers’ drinking behavior.
With regard to PTSD, 18.9% of the male and 22.7% of female officers’ scores met criteria for PTSD, reporting sufficient symptoms from categories A, B, C, and D of the PCL–C (Weathers et al., 1991). 4 Although our sample overrepresents older, White, male officers, these rates are consistent with population samples, and some police studies that find women have higher rates of PTSD than do men (Bowler et al., 2012; Tolin & Foa, 2006). Fewer variables were associated with PTSD among women, and no significant gender differences in regression coefficients were found. However, there was a trend (z = 1.90) similar to that described earlier for AUDIT, for critical incidents to be negatively related to PTSD among women but positively related to PTSD among men. It may be that factors other than critical incidents influence women’s development of PTSD. In their review of 25 years of research, Tolin and Foa (2006) found that women had higher rates of PTSD, even though they experienced fewer potentially traumatic events than did men. One prospective study suggests this sex difference may be due to situational vulnerabilities, including women’s greater exposure to trauma (e.g., rape; Koenen & Widom, 2009). It may be that policewomen’s PTSD stems from their experiences before entering law enforcement. Alternatively, it may be that typical measures of police stress (e.g., critical incidents) may not adequately reflect women’s experience or their development of PTSD. Research on policewomen found a three-factor model of stress including operational, management/organizational, and interpersonal, with the latter accounting for the most variance (Thompson et al., 2005). Thus, in addition to measuring prior stressors (e.g., sex assault victimization), we echo the call of Hickman and colleagues (Hickman, Fricas, Strom, & Pope, 2011) to measure officers’ stress more directly (e.g., via heart rate monitor) rather than relying solely on self-report measures that may not capture all types of stress experienced.
For both men and women, negative coping was significantly associated with PTSD symptoms. Social stressors were also associated with greater PTSD scores for both. These results are consistent with prior research that finds negative coping and social stressors (or lack of social support) can exacerbate mental health problems such as PTSD (Marmar et al., 2006; Stephens et al., 1997). For men, PTSD was also significantly associated critical incidents, the AUDIT score, and their interaction, with higher scores reflecting greater symptomology. This result demonstrates the important interplay between critical incidents and the methods used by officers to cope with them (i.e., drinking). In addition, time in policing was negatively associated with PTSD, while living outside the United States was positively associated with PTSD among males. Although the negative association between time in policing and PTSD may seem counter-intuitive, it may be due to greater attrition among officers with problems. Alternatively, it may be that there are higher levels of both negative coping skills and PTSD among newer officers who experience critical events. Finally, that country of origin is significantly associated with PTSD symptoms suggests the need for research on country variation in policing.
In sum, it is clear that as currently measured, critical incidents have a different influence on male and female police officers’ drinking. Critical incidents are associated with an increase in men’s AUDIT scores but a decrease in women’s. A similar trend was found for PTSD symptoms, but the regression coefficients did not significantly differ by gender. These results suggest research is needed to determine what factors contribute to the development of alcohol problems and PTSD among policewomen to better inform policy.
Implications
Given the prevalence of alcohol and trauma problems, the fact that negative coping was positively associated with both these outcomes across gender has important policy implications. As a preventative measure, police departments need to promote adaptive coping behaviors to counter the negative, “drinking” subculture that still permeates some agencies (Lindsay & Shelley, 2009). Researchers have begun to develop and explore officer resiliency programs designed to teach officers better coping skills (Arnetz, Arbel, Backman, Lynch, & Lublin, 2013; Arnetz, Nevedal, Lumley, Backman, & Lublin, 2009; Berking, Meier, & Wupperman, 2010; Shochet et al., 2011). Although samples are small, existing research finds that officers who receive training to improve their coping skills (Arnetz et al., 2009, 2013), including emotion-regulation skills (Berking et al., 2010), had better outcomes than their untrained counterparts. Thus, empirical development and use of these promising programs should be expanded. Departments should also provide officers with ongoing health education information (e.g., newsletters) and free or reduced cost services (e.g., gym memberships, counseling, coping skills training) to help them learn and use adaptive coping strategies to deal with stress. In addition to these programs, the positive relationship between social stressors and PTSD symptoms for both male and female officers suggests agencies need to try to ameliorate this type of stressor. Policies designed to reduce social stressors may help to reduce officer trauma. Further, the significant three-way interaction between social stressors, critical incidents, and negative coping among men suggests policies should include a multipronged approach to improve officers’ mental health. Departments may need to deal with social stressors on a more proactive, continual basis, rather than just providing services after officers experience critical events.
Because critical incidents had a different effect on male and female police officers’ drinking, a trend that was similar but not significant for PTSD, more research is needed to determine what work-related stressors most contribute to these problems among women. If most organizational responses to the development of mental health problems (e.g., alcohol and PTSD) focused on critical incidents and these incidents are not the source of these problems among policewomen, then an effort must be made to determine the primary cause. Most departments have developed responses to critical incidents (e.g., Critical Incident Stress Debriefing), but they do not have programs to deal with other sources of job stress. Research is needed to identify and find effective responses to all stressors of policing experienced by both men and women. Departments may need to develop gendered organizational responses to help officers deal with critical incidents. However, a more productive approach may be to make greater use of preventive programs (e.g., officer resiliency) designed to help officers cope with all forms of stress and alleviate negative mental health outcomes before they start.
In short, although there were similarities across gender (e.g., negative coping and social stressors) that provide clear direction as to the best prevention, education, and treatment policies, there were also gender differences (e.g., critical incidents) that require further study to better inform policy.
Limitations
This study used a large sample, reliable measures, and controlled for a number of officer characteristics on alcohol use and PTSD, but it also had limitations. First, the sample was not random, so the results are not generalizable. The female subsample was not as large as the male group, and the smaller size reduced the statistical power of those models. Future research should endeavor to include more young, women, minority officers from several nations to gain a better understanding of their ways of coping with stress. Second, this research was correlational, so causal inferences cannot be made. However, the study was based on prior research and results suggest replication is warranted. Third, although we included the measures of critical incidents and social stressors, we did not include other types of work-related stressors officers may encounter. This omission may be especially relevant for policewomen. Thus, future research should measure a broad spectrum of workplace and prior stressors (e.g., victimization) experienced. Fourth, we controlled for country of origin, but we did not include other country-level measures that may help in determining why country matters. Future research should include information from the country (e.g., crime rate, spending on emergency services) and include multilevel analyses to help clarify the role of country on officers’ well-being. Finally, self-reports can be problematic when measuring subconscious behavior. Future research should use a multimethod approach (i.e., combining self-report with biological or other objective measures) when examining stress and coping behavior.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.