
Abstract
Law enforcement officers’ health and wellness is important at the individual and community levels in terms of maintaining a fit workforce to uphold the mission of public safety. The current study was designed to assess officer wellness across the U.S. From a nationally representative random sample of 1,135 local and state agencies, a random, probability-based sample of officers was selected, oversampling for female officers. Latent class analyses were conducted to assess wellness profiles based on a set of eleven physical, psychological, and behavioral health indicators for 2,232 officers. Personal and professional characteristics were included as auxiliary variables in models of the resulting classes. Results from this sample indicated that over two-thirds of officers fit a healthy profile, whereas one in four officers presents with moderate health concerns and nearly 6% are classified in a profile of broad health concerns. In this sample, sexual assault in childhood, greater exposure to critical incidents, working a current rotation schedule, and being female were characteristics associated with broad health concerns. Emotional and/or physical assault in childhood, greater exposure to critical incidents, and being female were characteristics associated with moderate health concerns, whereas older age and being Hispanic were protective factors. In sum, full-time sworn law enforcement officers across the U.S. are reasonably healthy but their exposures to stressful situations put them at increased risk particularly in terms of post-traumatic stress, risky drinking, and suicidality. These results are important for agency administrators and policymakers to consider in terms of wellness programs, prevention efforts and budget allocations.
Law enforcement as a profession is characterized by operational risk and organizational stressors to officers’ safety and health, relevant to individual performance (Abdollahi, 2002) as well as to the recruitment, hiring, training, and retention of officers (U.S. Department of Justice, 2020). The daily risks during routine operations, plus risks associated with major natural or man-made disasters, are recognized to have an impact on officer mental health and behavioral outcomes in the short and long-term (Regehr et al., 2019; Velazquez & Hernandez, 2019). A recent systematic review suggests that police officers’ exposure to occupational health hazards often arise from accidents, chemicals, needle sticks, unacceptable noise levels, air pollutants, and the muscular challenges of extended periods of driving and/or lifting heavy objects, as well as critical incidents such as exposure to an abused child or being trapped in a life threatening situation (Mona et al., 2019). Compounding direct exposures to occupational risks, officers also face secondary trauma risks through their provision of support to community members and peers (Greinacher et al., 2019). Moreover, officers face these occupational hazards in the context of unique organizational stressors, such as rotating shifts, chain of command management environment, and cultural stigmas regarding mental health supports (Purba & Demou, 2019). Parallel to documentation of the hazards of working in law enforcement, there is a growing body of research examining officer wellness outcomes.
Wellness Indicators
While law enforcement officers have been shown to have poor outcomes relative to the general population on a number of psychological and behavioral health outcomes (Hartley et al., 2011; Mumford et al., 2015), studies of physical health indicators suggest that active duty officers are in better shape compared to their fellow citizens. Prior research found that only 14% of officers reported physical health problems in the highest tertile of a validated scale of somatic symptomology, compared to nearly a third of patients in a primary care sample (Kroenke et al., 2002). Moreover, a recent systematic review indicated that officers’ physical fitness indicators are in line with or somewhat better than that of general population samples (Marins et al., 2019).
While some health indicators are promising, there are a range of indicators for greater concern about officers’ well-being. As a starting place, regularly getting a good night’s sleep is one of the challenges officers face. Whereas 26–40% of participants in general population samples report poor sleep quality (Carroll et al., 2015; Doi et al., 2001; Hinz et al., 2017), a meta-analysis of data across 13 studies of police officers estimated that of 51% of officers suffer from poor sleep (Garbarino et al., 2019). Poor sleep quality has implications for sufficient activation after sleep (Fekedulegn et al., 2018) and officer performance (Rajaratnam et al., 2011), as well as health outcomes (Altman et al., 2012; Chopko et al., 2018). Sleep problems also have long-term associations with resilience (Segovia et al., 2013), a quality essential to managing the stressors specific to law enforcement.
Exposure to critical incidents in policing as well as organizational stressors gives rise, for some officers, to stress, anxiety and depression (Acquadro Maran et al., 2015; Bishopp et al., 2018; Husain, 2020; Kleim & Westphal, 2011; Velazquez & Hernandez, 2019). For example, stress and anxiety may arise as a consequence of workplace injuries (West et al., 2017) or in association with shiftwork and sleep patterns (Gerber et al., 2010). A growing concern in this sector is suicidality, with one study showing that suicidal ideation in the prior two weeks exceeded past year suicidal ideation in the general population (Chae & Boyle, 2013; Stanley et al., 2016). Completed suicide risk within law enforcement exceeds the average risk across a range of industries (Violanti et al., 2013), and research suggests that the rate has remained steady over the period 2008-2012 (O’Hara et al., 2013). Across the nation, protective services (which includes law enforcement) is the industry with the highest rate of female suicide (McIntosh et al., 2016). However, as a result of conflicting findings in the literature, Violanti et al. highlighted in a recent review of police suicidality studies the need for representative research (Violanti et al., 2019).
Exposure to traumatic stress also raises concerns about impact on cognitive functioning. Officers diagnosed with post-traumatic stress exhibit differential inhibitory response compared to civilians without trauma (Covey et al., 2013) and perform less well on memory recall tests (Lindauer et al., 2006). Even short-term exposures to stressful scenarios may impact officers’ cognitive functions and ability to process information (Gutshall et al., 2017), with implications for job performance over time. The reality of cumulative trauma for these professionals may result in an array of deleterious physical outcomes as well, including metabolic syndrome, cardiovascular disease precursors and outcomes, and neurological disorders (Juster et al., 2010; Violanti et al., 2017).
Job stressors, as well as physical and mental health problems, may lead to poor behavioral health choices. A central behavioral health indicator of officer wellness is alcohol misuse (K. D. Bradley, 2020). Although, for some officers, drinking may be associated with social norms (Lindsay & Shelley, 2009), problem drinking is also associated with poor coping strategies in response to feelings of stress (Ballenger et al., 2011; Ménard & Arter, 2013). Past estimates of problem drinking (varying definitions including binge drinking) among officers range from 17% to over half of both male and female officers (Ballenger et al., 2011; Chopko et al., 2013; Ménard & Arter, 2013; Mumford et al., 2015; Zavala & Curry, 2018), exceeding general population risks (K. A. Bradley et al., 2007). The extent to which problem drinking serves as an indicator of and self-medication to manage stress and traumatic exposures ( Ballenger et al., 2011; Chopko et al., 2013; Lindsay & Shelley, 2009; Ménard & Arter, 2013; Violanti et al., 2011) is relevant to agency resource allocations for mental and behavioral health programming.
Taken together, there is a growing body of research regarding a range of physical, psychological and behavioral health outcomes for law enforcement officers. However, past empirical research on officer wellness has tended to focus on selected individual physical or mental health outcomes, thus offering limited understanding of overall profiles of officer health and/or comorbidities and creating a methodological division between physical and psychological health symptomology. Moreover, the literature to date describing officer wellness outcomes relies on local and/or convenience samples, with limitations in terms of describing the population of officers across the United States.
Current Study
The current study addresses these gaps through estimation of wellness profiles across a range of officer outcomes in a national representative sample of officers. The key research questions are what proportion of officers fall into a profile of diminished wellness, whether profile analyses can reveal correlations in officer conditions that point to appropriate agency supports, and whether other officer characteristics can help identify officers at risk in advance of worse health outcomes. Whereas most officers are expected to fit a profile of good health given the rigorous requirements of the job, past research would suggest that a small proportion of police officers likely fit a profile of deleterious mental, physical, and behavioral health outcomes. Results of this study are expected to be informative to law enforcement leadership in consideration of agency recruitment, policies, and programming, as well as to officers attending to self-care, behavioral health, and coping strategies for managing the stressors of police work.
Method
Participants
Data for this study were collected over the period August 2017 to February 2019 from a nationally representative sample of law enforcement officers through the Officer Safety and Wellness (OSAW) Initiative, funded by the National Institute of Justice (NIJ). Using a two-stage sampling process (study methods approved by the authors’ institutional IRB), we (1) selected a representative sample of law enforcement agencies (LEAs) across the US and requested rosters of all their officers, and (2) applied a systematic randomization procedure to sample officers from each agency roster. The randomization procedure was designed to select the appropriate number of officers from each roster according to agency size (i.e., the number of sworn officers), while also oversampling females at a rate of 2:1; see Mumford et al. (2020) for details. Field methods for inviting officers to the online survey and prompting participation over time consisted of reminder notes to officers’ work email addresses (a reminder letter mailed to officers from small agencies did not appear to be cost-effective in terms of responses), continued through the full field period to allow officers to join the study at their own convenience. No incentives were offered with for study participation. Agency leadership were not informed of which officers completed surveys and which did not, from the sample of officers selected in each agency. Out of the 8,060 invited eligible officers, a total of 2,867 officers (35.6% 1 ) completed the OSAW questionnaire. Two-thirds (66.3%) of this officer sample worked in municipal law enforcement, nearly one in four (23.3%) worked for county law enforcement, 10% worked for state police or highway patrols, and fewer than 1% worked for the Bureau of Indian Affairs. The response rate to this panel study exceeds that of other established panels (Fontes et al., 2015). Most of these officers completed all the survey questions, with minimal item-level missing values. Inclusion in the current analytic sample (n = 2,232 officers, ∼80% of the total sample), which was weighted to address officer non-participation in the study, was based on the following criteria: (1) the officer responded to at least one of the six items regarding the type of wellness programs offered (218 officers were excluded because of missing values on all six outcome variables); and (2) the officer responded to all exogenous items detailing other officer characteristics included in the analytic model (417 officers were excluded due to a missing value on at least one characteristic).
Measures
Officer Wellness Indicators
Physical Health
Officers responded on a 3-point scale to 15 items from the Patient Health Questionnaire regarding how much they were bothered by physical pains (i.e., stomach, back and chest) and pain during sexual intercourse, as well as dizziness, rapid heart rate, shortness of breath, constipation, nausea, low energy and insomnia (Kroenke et al., 2010). A categorization of the total score indicated whether officers were experiencing minimal (scored 1–4), mild (scored 5–9), moderate (scored 10–14), or severe (scored 15+) physical health issues. As only 3% of the sample reported severe physical health issues, the variable was further dichotomized into minimal/mild (coded 0) versus moderate/severe (coded 1) physical health issues.
Psychological Health
Higher scores on the Perceived Stress Scale (PSS; Chronbach’s alpha = 0.84; range 0–4), originally designed for community samples and widely applied (Cohen et al., 1983), represent more officer stress in the past month. The Mental Health Inventory (MHI-5), a 5-item validated scale assessing anxiety and depression (Berwick et al., 1991), was a continuous measure (Chronbach’s alpha = 0.83; range 0 to 100) assessed for the past month, with higher scores representing greater emotional distress. (Typically, MHI-5 is coded with higher scores representing better emotional well-being, and so for comparison the inverse of the OSAW sample MHI-5 score is provided in the results below). The Primary Care-PTSD scale is a four-item screener used in general population and military research for post-traumatic stress disorder (PTSD) (Prins et al., 2004); an indicator variable of officers’ lifetime experience of PTSD was coded 1 for scores of 3 or higher on the 4-point scale (Chronbach’s alpha = 0.78). Responding to the Suicidal Behaviors Questionnaire (SBQ), respondents were also asked if they had ever thought about or attempted suicide, whether they had conveyed these thoughts to someone else, and the likelihood of an eventual attempt. The four items were scored and a summary score ranging from 3 to 18 was created (Chronbach’s alpha = 0.74). An indicator of an officer being at risk of suicide was coded 1 for scores of 7 or above (Osman et al., 2001).
We also assessed officers’ neurocognitive functioning on a 5-point Likert frequency scale in response to 27 items drawn from the Deployment Risk and Resilience Inventory (DRRI). A factor analysis confirmed the three subscales — executive functioning (Chronbach’s alpha = 0.90), attention and concentration (alpha = 0.94), and memory (alpha = 0.92) — found in prior research (King et al., 2006). Higher values (5-point Likert frequency response scale for each item) represent greater deficits in each construct.
Behavioral Health
An indicator for risky drinking measured by the 3-item AUDIT-C screener was coded 1 for total scores of 4 or greater for males and 3 or greater for females (K. A. Bradley et al., 2007). Prescription drug use misuse within the past 12 months was assessed by a single-item 4-point scale from never to weekly or more (Harris, 2009), coded as an indicator of any use in the past year. Officers’ conventional cigarette smoking status, following measurement in the Tobacco Use Supplement to the Current Population Survey (Fagan et al., 2007), was coded as current smoking (1) or never/former smokers (0).
Covariates
Critical Incident History
Created to document exposures that might lead to officer stress or trauma, respondents viewed 29 items drawing on the Critical Incident History Questionnaire (Weiss et al., 2010) with modifications made in discussion with a panel of experts. Respondents were asked about their lifetime exposure to each of 29 incidents such as “You were in a life-threatening high speed chase or vehicle collision” and “You were threatened with a knife/gun/other weapon.” Items added to the index assessed stressful policing exposures not on the original questionnaire, such as “You were attacked on social media for an action related to your police work.” Respondents reported exposure to each potential experience on a 3-point frequency scale, never, once or twice, or more than twice, recoded into 0 (never occurring) and 1 (ever occurring). A count variable was created to represent the number of unique types of stressful exposures experienced.
Adverse Childhood Experiences
Eleven items were included to determine prevalence of adverse childhood experiences (ACEs) or early-life stressors among participants. A confirmatory factor analysis was conducted, yielding the same subscale structure found in prior research (Ford et al., 2014; Mumford et al., 2019). The three ACE factors were coded 1, respectively, indicating the presence of family instability, physical/emotional abuse, and sexual abuse, with each of the three factors representing an affirmative response to at least one of the items loading on that factor.
Demographics and Employment History
Officers responded to items regarding demographics (age, biological sex, and race/ethnicity), education level (college or higher degree, less than college degree), any military experience (no experience, less than five years in the military, five or more years in the military), years of sworn experience in law enforcement (measured as a 5-level variable, 0–5 years, 6–10 years, 11–15 years, 16–20 years, 21+ years, and treated as a continuous measure), current rank (line officer, supervisor, or commander), and current assignment to a rotating shift (coded 1 vs. fixed shift coded 0). An indicator of whether the officer was working overtime and/or working a second job (coded 1) was also included.
Analytical Model
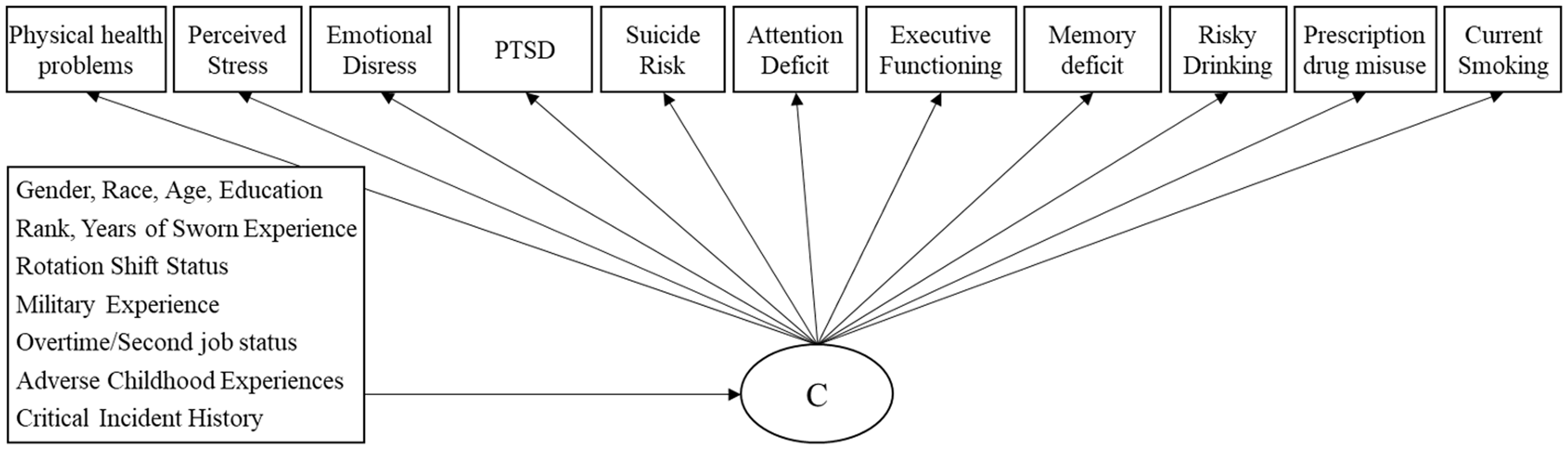
We empirically identified profiles of officer physical, mental, and behavioral health using latent class analysis (LCA) (Muthén, 2001). LCA divides the population with similar response patterns into an unknown number of mutually exclusive and exhaustive subpopulations (or latent classes, “C” in Figure 1). LCA models with different numbers of profiles were estimated and compared with respect to their model fit based on a substantive evaluation of the classes as well as fit statistics for non-nested models, such as the Bayesian Information Criterion (BIC) (Nylund et al., 2007), where a lower BIC indicates better fit and the Lo-Mendell-Rubin likelihood ratio test (Lo et al., 2001), where a K-1 class model can be rejected in favor of a K-class model at the conventional significance level. In addition, entropy values (ranges from 0 to 1 and indicates a better classification of individuals as values approach 1) were examined (Ramaswamy et al., 1993). The LCA approach yields information on how many officer physical, mental and behavioral health profiles are present in the sample. In addition to estimating the prevalence of officers classified in these profiles, we also examined how officer characteristics are related to these profiles by regressing “C” on covariates via multinomial logistic regression (Long, 1997). All analyses were conducted using Mplus software version 7.3 (Muthén & Muthén, 1998–2012).
Analytical Model.
Overall, most of the officers who responded to the survey skipped very few questions (among the 2,232 officers in this analytic sample, 98% of the responding officers answered all 11 health indicators). Continuous indicators were rescaled to a consistent range of 0 to 100. Partial missing data on the outcome variables (latent class indicators) were accounted for by using the widely accepted full information maximum likelihood (FIML) estimation method (Arbuckle, 1996; Schafer & Graham, 2002) and results are weighted to ensure national representativeness (DiSogra, 2009); weights were calculated with the probability of selection and adjusted for survey non-response.
Results
Descriptive Analysis
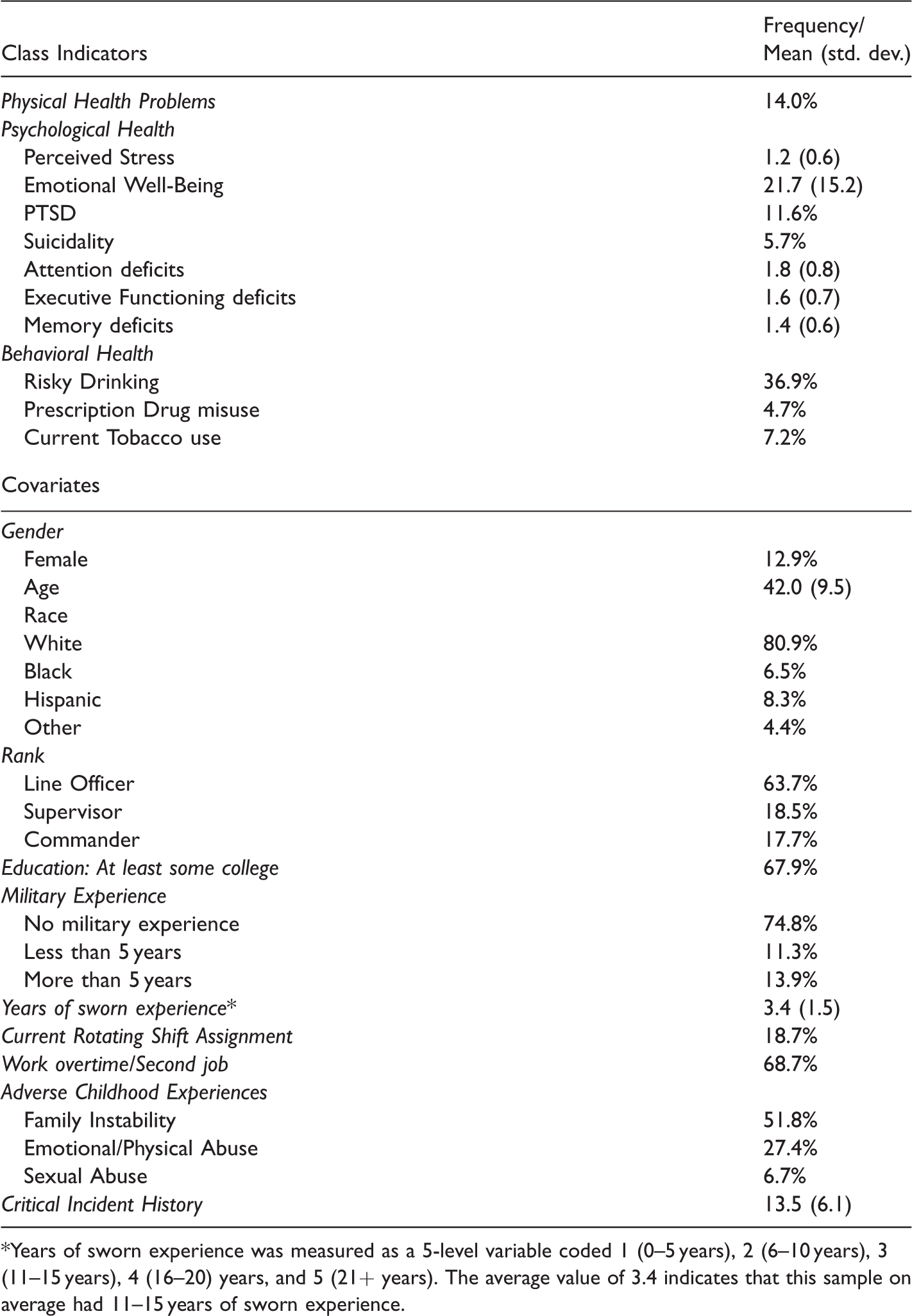
Table 1 presents the weighted distribution of all study variables. The majority of the respondents (87%) were male, 81% were White, 64% were line officers, 19% were supervisors, and 18% were commanders. The average age of the officers who responded to the survey was 42, and on average they had 11–15 years of experience as a sworn police officer. In this officer sample, 68% had a college degree or higher, 19% were currently working a rotating shift, 69% worked more than full time or had a second job, and the majority (75%) did not have any military experience. Before age 18, over half (52%) of the sampled officers had experienced family instability, 27% experienced physical or emotional abuse, and close to 7% experienced sexual abuse. On average, officers in the sample had ever experienced 14 types of critical incidents in their law enforcement careers.
Weighted Distribution of Physical, Psychological, and Behavioral Health, OSAW Initiative (N = 2,232).
*Years of sworn experience was measured as a 5-level variable coded 1 (0–5 years), 2 (6–10 years), 3 (11–15 years), 4 (16–20) years, and 5 (21+ years). The average value of 3.4 indicates that this sample on average had 11–15 years of sworn experience.
About one in seven (14%) of the responding officers reported moderate or severe physical health problems. Officers’ average emotional distress score was 21.7 (the inverse score, for comparison with other studies, was 78.3), and the average perceived stress level was 1.2 (on a 0–4 scale). In this sample, officers’ average levels of attention deficit, executive functioning deficit, and memory deficit were 1.8, 1.6, and 1.4 respectively (on a 1-5 scale). Nearly 12% officers screened positive for PTSD, and 5.7% were at risk for suicide. About two out of five officers (37%) reported risky drinking during the past year (35.4% of male officers and 47.3% of female officers – not presented in Table), 5% reported misusing prescription drugs, and 7% were current smokers.
Latent Profiles of Officer Health Profiles
We identified three distinct officer profiles based on physical, psychological and behavioral health outcomes (see Table 2 for model fit statistics). Figure 2 presents the three profiles, with the scale on the left side representing the continuous health measures (rescaled 0-100) and the scale on the right side representing the probability of each dichotomized health indicator. Over two-thirds (68.3%) of the officers in this sample were classified in a Healthy profile with no significant health issues of any kind, i.e., with minimal emotional distress, limited evidence of neurocognitive functioning deficits, low perceived stress, low probability of having moderate to severe physical health problems, lower than average level risky drinking (probability = 0.3), prescription drug use and smoking (probability <0.1). They were also not likely to be at risk for suicide or to screen positive for PTSD (probability <0.1).
Latent Class Analysis: Model Fit Statistics to Determine the Number of Classes.
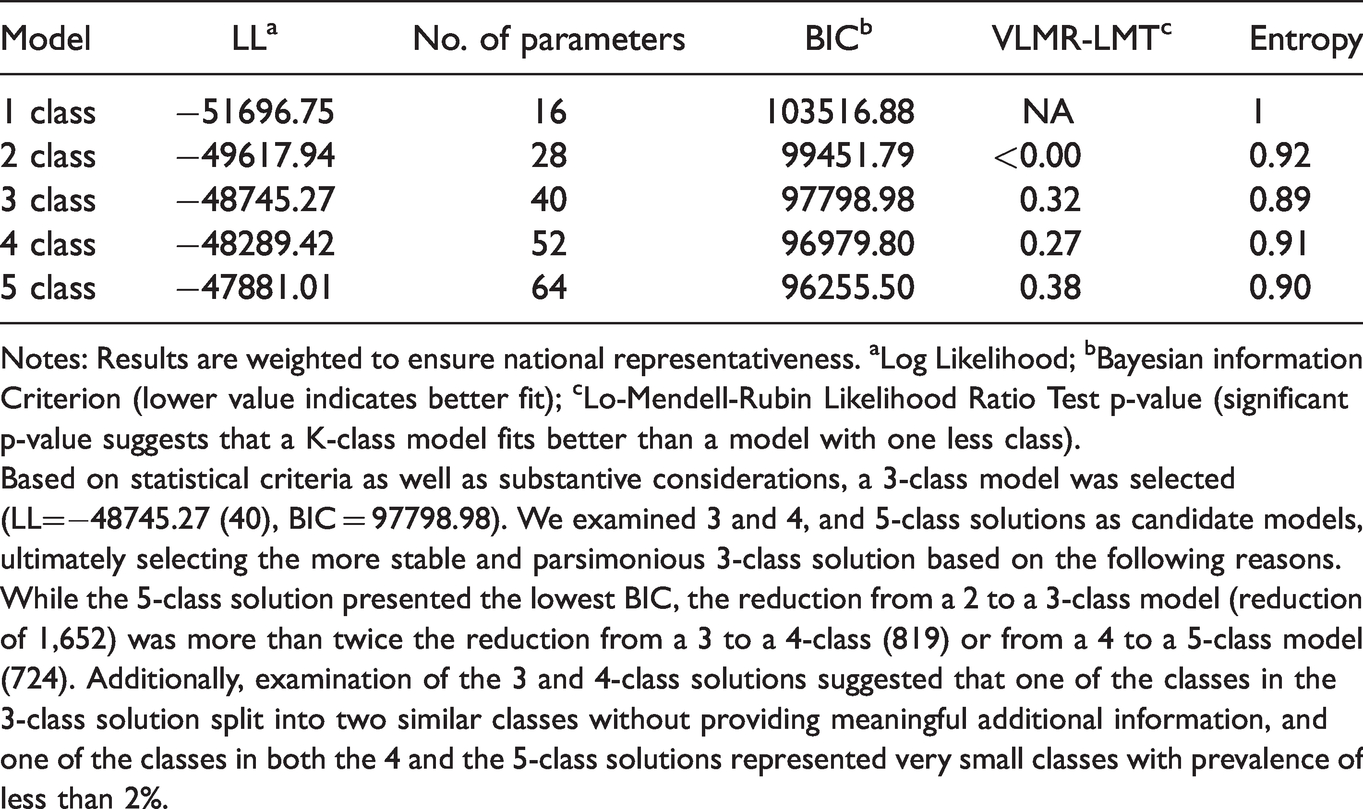
Notes: Results are weighted to ensure national representativeness. aLog Likelihood; bBayesian information Criterion (lower value indicates better fit); cLo-Mendell-Rubin Likelihood Ratio Test p-value (significant p-value suggests that a K-class model fits better than a model with one less class).
Based on statistical criteria as well as substantive considerations, a 3-class model was selected (LL=−48745.27 (40), BIC = 97798.98). We examined 3 and 4, and 5-class solutions as candidate models, ultimately selecting the more stable and parsimonious 3-class solution based on the following reasons. While the 5-class solution presented the lowest BIC, the reduction from a 2 to a 3-class model (reduction of 1,652) was more than twice the reduction from a 3 to a 4-class (819) or from a 4 to a 5-class model (724). Additionally, examination of the 3 and 4-class solutions suggested that one of the classes in the 3-class solution split into two similar classes without providing meaningful additional information, and one of the classes in both the 4 and the 5-class solutions represented very small classes with prevalence of less than 2%.
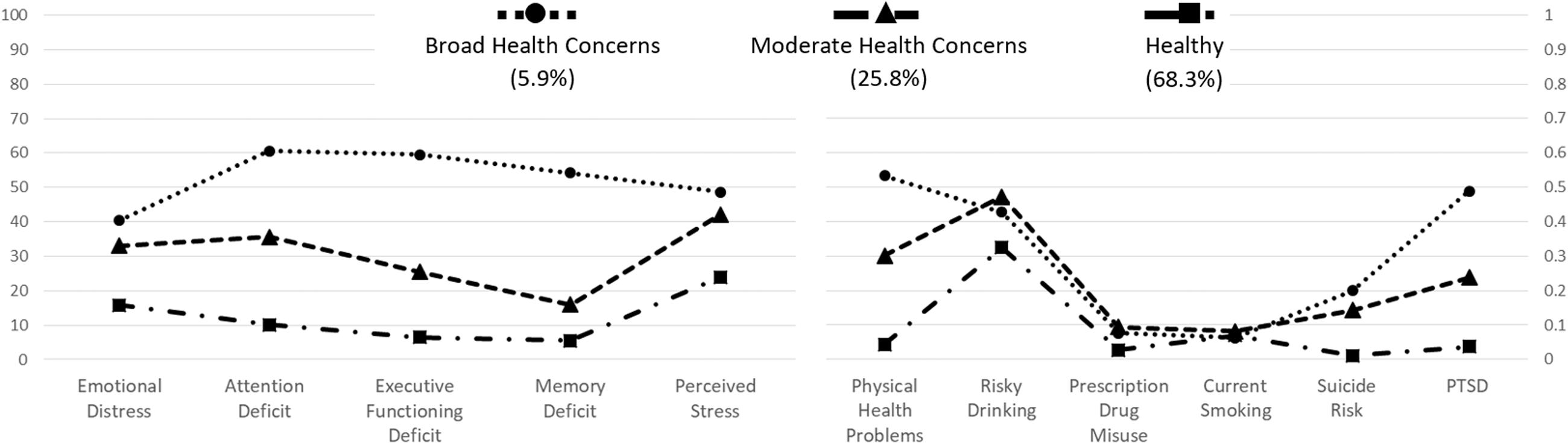
Latent Classes of Law Enforcement Officer Physical, Psychological, and Behavioral Health. Measures of perceived stress and attention, executive functioning, and memory deficits are rescaled to 0–100.
By contrast, 5.9% of the officers were classified in a Broad Health Concerns profile, given their reported experiences of a high level of mental, physical and behavioral health problems. For example, their attention deficit was as high as 60 on a 0–100 scale, translating to a 3.4 on a 1-5 scale, and they had close to 0.6 probability of screening positive for PTS. They also had a 0.6 probability of experiencing moderate to severe physical health problems and a 0.4 probability of risky drinking, although their probability of prescription drug misuse and smoking was only 0.1, similar to the probability within the Healthy profile.
About one in four officers (25.8%) in the sample were classified in a Moderate Health Concerns profile. Their level of neurocognitive deficits and their probability of having moderate/severe physical health problems or PTSD fell between the Healthy and Broad Health Concerns groups. However, their levels of perceived stress and emotional distress, and their probability of risky drinking and suicide risk were similar to those in the Broad Health Concerns profile. This group also had low probability of prescription drug misuse and cigarette smoking.
Officer Characteristics Related to Health Profiles
Several officer characteristics were significantly related to officer health profiles (Table 3). Compared to male officers, female officers were close to three times as likely to be in the Broad Health Concerns profile (AOR = 2.75; p-value<.001) and twice as likely to be in the Moderate Health Concerns profile (AOR = 2.10; p-value<.001) compared to the Healthy profile. Older officers were less likely to be in the Moderate Health Concerns profile vs. the Healthy profile; in other words, with each year of increasing age, officers were 4% less likely to be in the Moderate Health Concerns profile (AOR=.96; p-value=.01). Compared to white officers, Hispanic officers were 59% less likely to be in the Moderate Health Concerns profile than the Healthy profile (AOR=.41; p-value<.001). Officers who were currently working a rotating shift were twice as likely to be in the Broad Health Concerns profile as in the Healthy profile (AOR = 2.02; p-value = .01). Officers who were emotionally and/or physically abused before age 18 were 1.5 times as likely to be in the Moderate Health Concerns profile as in the Healthy profile (AOR = 1.48; p-value = .04), and those who were sexually abused were twice as likely to be in the Broad Health Concerns profile (vs. the Healthy profile; AOR = 2.15; p-value = .05). A higher count of exposures to critical incidents was significantly associated with increased likelihood of being in the Broad Health Concerns (AOR = 1.10; p-value<.001) and Moderate Health Concerns profiles (AOR = 1.07; p-value<.01) than in the Healthy profile.
The Association Between Law Enforcement Officer Characteristics and Health Profiles.
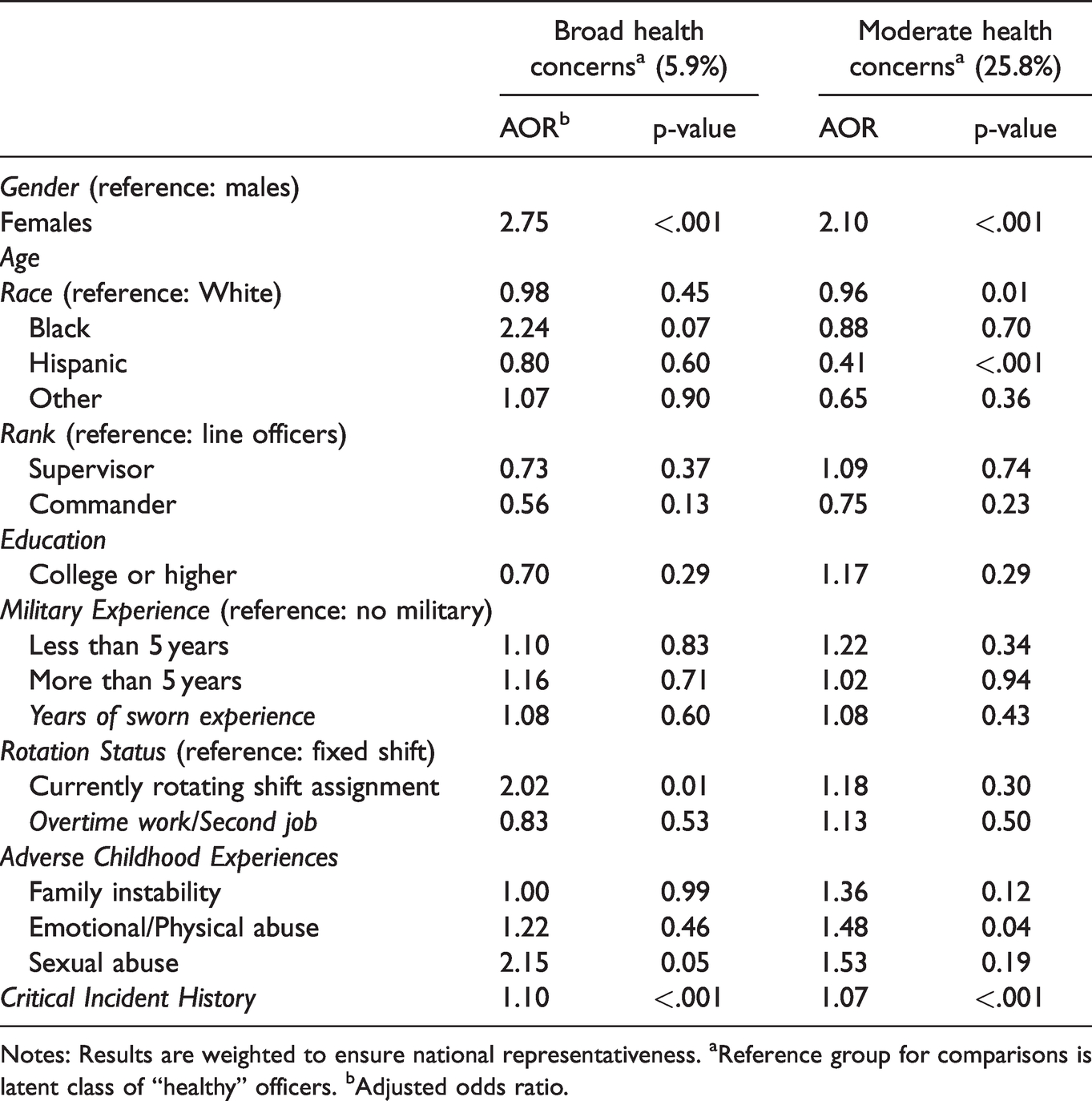
Notes: Results are weighted to ensure national representativeness. aReference group for comparisons is latent class of “healthy” officers. bAdjusted odds ratio.
Discussion
The OSAW Initiative is the first nationally representative study of officer safety and wellness outcomes, building on prior research limited to specific departments, states or regions. Wellness indicators from the OSAW Initiative facilitate comparisons with U.S. general population estimates on the same measures. For example, the proportion of officers reporting moderate or severe physical health problems (14%) was about half the rate as reported by a primary care sample (Kroenke et al., 2002), and the OSAW sample of officers reported better neurocognitive performance (as an overall mean score) than reported by Gulf War veterans (King et al., 2006), likely reflecting differentials in veterans’ head injuries experienced in combat zones.
In terms of officers’ psychological health, the critical difference between officers and the general population appears to be on the measure of PTSD. OSAW findings suggest that the past year rate of PTSD among officers in the U.S. (11.6%) was nearly three times the estimated general population rate (4%) (Briere et al., 2016; Kessler et al., 2005; Kilpatrick et al., 2013). By contrast, other measures of psychological health suggest comparable or better rates relevant to general population samples. Officers reported slightly higher levels of emotional wellness (mean 78.3 on a scale of 0-100) than both a large primary care practice population in the Northeast U.S. (mean 74) (Bova et al., 2012) and a general population sample mean on the same measure (mean 72.6) several decades ago (Stewart et al., 1988). In contrast to findings from a systematic review across professions of a suicidality higher risk for first responders (Stanley et al., 2016), the current results suggest a lower rate of suicidality than found in other police studies (Bishopp & Boots, 2014) and in representative general population research. Importantly, general population estimates and the OSAW estimate are not directly comparable given different gender distributions; even within the OSAW sample, suicidality among female officers (7.0%) exceeds that of male officers (5.4%). The current nationally representative OSAW findings suggest that the prevalence of officer suicidality—while still disquieting, particularly among female officers (McIntosh et al., 2016)—may not exceed the rate of suicidality in the general population. The greater concern may lie with officers’ perceptions of stigma associated with help-seeking (K. D. Bradley, 2020; White et al., 2016), access to the ready means for suicide (i.e., firearms) and training that result in completed suicides (Violanti et al., 2013). Thus, there is a great need for attention to PTSD and subsequent behavioral choices.
Officers in the OSAW sample report current smoking of combustible cigarettes (7.2%) at about half the 2018 rate of adults (13.7% overall; the adult male current smoking rate is 15.6%, relevant to the gender imbalance in law enforcement) in the general population (Creamer et al., 2019). Of greater concern, officers’ rate of prescription drug misuse (4.7%) appears to be similar to the reported rate of misuse in the U.S. population (age 12+) of at least 4.3% (Hoots et al., 2018). This is potentially a serious problem, as misusing opioids and other prescription drugs could affect an officer’s decisions on important matters (e.g., use of deadly force) or in safely operating police vehicles. Also of deep concern is officers’ alcohol use. Officers’ risky drinking in the past year exceeded the problem in the general population (Dawson et al., 2005), particularly among female officers for whom the screened rate of risky drinking was nearly twice that of a general population sample (K. A. Bradley et al., 2007).
Coinciding with the current study is the timely release of a systematic review and meta-analysis of law enforcement studies of officers’ mental health outcomes, limited to studies that used validated scales with at least 100 officers (Syed et al., 2020). While the Syed et al. results included prevalence estimates of PTSD (14.2%), suicidality (8.5%), and risky drinking (25.7%), the data were drawn from law enforcement samples from all over the world, few of the samples were generalizable, and measurement across the included studies varied. Still, the results do not contradict our OSAW estimates, nor our interpretations in comparison with general population samples.
The comorbidity of psychological disorders and behavioral health choices is well-established for general population samples (Jacobsen et al., 2001; Kessler et al., 2005; Stickley et al., 2020; Swendsen & Merikangas, 2000), but this is the first representative study to investigate comorbidity of behavioral health along with physical and psychological outcomes for law enforcement officers. The person-centered approach used in the study allowed us to simultaneously consider physical, psychological, and behavioral health. Consistent with our study hypotheses regarding potential profiles of health and wellness, over two-thirds of the sample may be described as generally healthy across the measured indicators of well-being, with the exceptions of risky drinking and prescription drug misuse, potentially a maladaptive coping strategy for the inevitable stress of the job. At the other end of the spectrum, a very small proportion of officers (about one in twenty or 5.9%) present as a profile with Broad Health Concerns. These officers are not only reporting their sense of high stress, poor mental health, managing trauma symptoms, risky drinking, and moderate to severe health problems, they also have a high risk of deficits in neurocognitive functioning, and may require support to be able to perform their public safety duties to expected standards. The remaining quarter of officers in this sample, the Moderate Health Concerns profile, represent the middle ground: officers who are reporting high levels of stress but less trauma symptomology. Their neurocognitive performance is closer to that of the Healthy profile officers, and they report less physical and mental health symptomology. However, it is important to attend to the risk that these officers may be self-medicating with alcohol (Leino et al., 2011), given their probability of risky drinking, which may have long-term implications for performance and health outcomes (Gershon et al., 2009).
We also examined officer sociodemographics and professional history characteristics and the extent to which there are sub-groups of officers with particular characteristics that are associated with specific profiles of officer wellness. Central to policing, and consistent with past research (Gershon et al., 2009; Weiss et al., 2010), greater exposure to critical incidents was associated with classification in both higher risk profiles. Also consistent with expectations, working a rotating shift (Demerouti et al., 2004; Violanti, 2012) and managing a history of abuse in childhood (Hughes et al., 2017) were associated with broad health concerns. Previous research regarding officer suicidality has also pointed to associations with critical incident history, shiftwork, and alcohol misuse (Chae & Boyle, 2013). That female officers were twice as likely to be classified in the profiles of moderate and broad health concerns is consistent with the additional challenges of working in a male-dominated occupation (Franklin, 2005; Shelley et al., 2011) and other research that found that organizational stressors and lack of social support were related to female, but not male, officers’ metabolic health problems (Tara A. Hartley et al., 2011).
Findings from our representative sample study may challenge other expectations. For example, while prior police research had identified a higher risk of trauma symptomology for Hispanic officers (Marmar et al., 2006), these nationally representative OSAW results suggest that Hispanic officers are 59% less likely to fall into the profile of Broad Health Concerns regarding mental, physical, and behavioral outcomes. Additionally, the finding that increasing age was associated with greater likelihood of being classified in the Healthy profile is counter to expectations of increased health issues resulting from longer exposures to stressors (Geronimus et al., 2006). For example, in the absence of adaptive coping skills, long-term exposures to stress leads to poor health outcomes among female officers (Andrew et al., 2017). However, selective mortality or retirement (Crimmins et al., 2003; Violanti et al., 1998) in the OSAW cohort may have resulted in older officers who have better coping skills and thus, broadly, a healthier psychological, physical, and behavioral wellness profile.
Importantly, concurrent with descriptive research on officer wellness and risk factors, prevention research with officers is underway across the globe. Although reviews of intervention studies—targeting stress and behavioral risk factors for poor health outcomes—found multiple weaknesses in design and limited impact (Lees et al., 2019; MacMillan et al., 2017; Patterson et al., 2012; Rachele et al., 2014; Wolkow et al., 2013), the level of attention to developing working models for integration into law enforcement agencies is promising. For example, psychological skill training may have an impact on officers’ memory (Page et al., 2016), and research assessing the impact of workplace resilience training also points to moderate effectiveness (Leppin et al., 2014; Vanhove et al., 2016) across sectors and for police performance (e.g., Andersen & Gustafsberg, 2016). The current study adds to the field of prevention in terms of identifying psychological, physical, and behavioral comorbidities requiring attention.
Limitations
Interpretation of these study results should consider limitations of the study design. First, these data were self-reported by the officers, and while we relied on validated scales and screeners, we did not have independent diagnostic results for officer health outcomes. For reasons mentioned above, there may have been more reluctance in this population to reveal their mental, physical, or behavioral health histories. Second, while the officers’ response rate to this OSAW survey compared well with other national convenience samples of police officers (Fraternal Order of Police [FOP], 2019) and nationally representative panels recruited for longitudinal research participation (Fontes et al., 2015), particularly without a monetary incentive (Nix et al., 2019), results should be considered in the context of potential bias introduced by officers’ choice whether to participate in the study. Third, with cross-sectional data we could not investigate causal mechanisms of the reported outcomes; an example of the challenge this presents is the bidirectional association between alcohol abuse and depression (Pacek et al., 2013). Additional longitudinal research is needed to examine officer safety and wellness outcomes in terms of the breadth of outcomes, the impact of agency-level characteristics, and time-ordered associations between stressors, coping strategies, and health outcomes.
Conclusion
Practitioners and policymakers alike have long recognized the importance of creating and maintaining a cadre of officers who are in good shape physically and mentally to implement the public safety mission of law enforcement (Abdollahi, 2002; U.S. Department of Justice, 2015, 2020). Results from the baseline OSAW Initiative data highlight that, despite the strains of the job, over two-thirds of U.S. law enforcement officers present as low risk on measures of general physical health, psychological health, neurocognitive functioning, and behavioral health. While celebrating these officers’ resilience is important, attending to their continued wellness over their careers is an essential component of public safety and appreciation for those who help to ensure public safety. Moreover, nearly a third of police officers already appear to exhibit moderate to broad risk profiles, which may contribute to the elevated morbidity and mortality apparent after long careers in law enforcement. These nationally representative results underscore local studies that have highlighted the need for additional medical and mental health assistance to place officers on a safer path to overall wellness. This study indicates the breadth of the need for policymakers and agencies to provide resources to meet these officers’ needs earlier in their careers, to mitigate stressors and build resilience.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Footnotes
Acknowledgments
We would like to express our sincere gratitude to the agencies and dedicated officers who participated in this research. Further thanks are due to the members of our Expert Panel who collaborated in the design and review of the survey instrument: Timothy Baysinger, Sarah Creighton, Stephen James, Tara Kelley-Baker, Sandra Ramey, Elizabeth Stanley, Darrel Stephens, Bryan Vila, and John Violanti. We would like to thank PERF staff Jeremy Barnum, Sean Goodison, Nathan Ballard and Adam Kemerer and NORC staff Meghan O’Leary, Amanda O’Keeffe, Jackie Sheridan, Katie Archambeau, Julie Banks, and Steven Pedlow.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Institute of Justice 2016-IJ-CX-0021.