
Abstract
Objectives
Tarsal tumours are rare, but previous reports suggest a predilection for round cell tumours (RCTs) and soft tissue sarcomas (STSs) in this region. This study aimed to determine the proportion of RCTs among feline tarsal neoplasms, refine classification through histological revision and immunohistochemistry (IHC), assess potential risk factors and evaluate clinical outcomes based on tumour histotypes.
Methods
A retrospective analysis of feline tarsal neoplasms diagnosed between 2010 and 2024 was conducted. Signalment, history, treatment and outcomes were collected for RCTs and STSs. All RCTs underwent histological review and IHC (CD3, CD20, CD79a, MUM-1, CD18, IBA-1, E-CAD). A diagnostic algorithm was applied to support the diagnostic process.
Results
A total of 34 cases were included: 18 RCTs and 16 STSs. In 39% of RCTs, the initial histotype was undetermined. After IHC and application of the diagnostic algorithm, 50% of cases were reclassified: seven plasma cell tumours, four progressive histiocytosis, three lymphomas, two histiocytic sarcomas and two undifferentiated RCTs. Male sex, older age and prior tarsal trauma were significantly associated with RCTs (P = 0.042, P = 0.048 and P = 0.009, respectively). Clinical signs and metastases at diagnosis were more frequent in RCTs (P = 0.019 and P = 0.001, respectively). RCT treatment included chemotherapy (n = 7), surgery (n = 5), surgery and chemotherapy (n = 2), prednisolone (n = 1) or none (n = 1); two cases lacked treatment data. All STSs were managed surgically without chemotherapy. Time to progression and median survival were significantly shorter for RCTs compared with STSs (139 vs 854 days; 173 vs not reached, respectively; P <0.001).
Conclusions and relevance
This study confirms that feline tarsal RCTs are a heterogeneous group of tumours with a poor prognosis. Risk factors may include male sex, older age and previous tarsal trauma. A standardised IHC panel combined with a diagnostic algorithm improved histotyping accuracy and should be adopted in clinical practice.
Keywords
Introduction
The feline tarsal region can be affected by a variety of neoplasms, including round cell tumours (RCTs),1–7 soft tissue sarcomas (STSs)8,9 and primary bone tumors.10–13
Over time, several heterogeneous RCT subtypes have been reported in this region, including plasma cell tumours, lymphoma, feline progressive histiocytosis (FPH) and histiocytic sarcoma.1,2,5,8,14,15 However, most of these cases have been described in the context of broader studies focusing on specific tumour histotypes, irrespective of their anatomical location or as isolated case reports.3–6,16 Furthermore, most of these studies did not utilise comprehensive immunohistochemical panels for diagnosis.1–4,6
The existing literature highlights the diagnostic complexity of RCTs, because of their overlapping histological features, making immunohistochemistry (IHC) essential for accurate identification.16–21 However, inconsistencies in phenotyping standards across laboratories, driven by factors such as costs, pathologist preferences and variability in IHC protocols, may contribute to the challenges in accurately classifying these tumors.14,18–21 Recent reports of CD3 and MUM-1 co-expression in feline tarsal and extratarsal plasma cell tumours add to the complexity,15,21 raising the question of whether the observed predilection of multiple RCT subtypes for the tarsal region is a true biological phenomenon or a result of incomplete or poorly standardised diagnostic approaches.
This diagnostic uncertainty has significant implications for understanding the biological behaviour and prognosis of feline tarsal RCTs, both of which remain poorly characterised. Consequently, therapeutic approaches are not standardised, and there are currently no consistently effective treatments for these neoplasms.1,2,16,22–26
This study retrospectively analysed all cases of feline tarsal neoplasms presented at our institution to determine the prevalence of RCTs. For each identified RCT, histological findings were reassessed using a comprehensive and standardised IHC panel to establish definitive diagnoses. The study also re-evaluated the clinical outcomes based on tumour histotype and explored potential risk factors contributing to the predilection of RCTs for the tarsal region.
Materials and methods
Study design
The hospital database of the Department of Veterinary Medical Sciences, University of Bologna, Italy was retrospectively searched to identify cats with tumours located in the tarsal region that underwent histological examination between January 2010 and December 2024.
All cases of RCTs underwent further histopathological and immunohistochemical review, as described below. In cases showing ambiguous morphology and negative immunoreactivity for all lineage-specific markers included in the primary panel, additional immunohistochemical stains for epithelial (cytokeratin) and melanocytic differentiation (Melan-A and PNL2) were performed. Cases showing positivity for these markers were excluded from the RCT group. When deemed necessary, special histochemical staining with Giemsa was also performed to exclude poorly differentiated or atypical mast cell tumours.
For cats diagnosed with RCTs or STSs, data were extracted from medical records, including signalment, feline immunodeficiency virus/feline leukaemia virus status, clinical signs, affected limb, tumour longest diameter, presence of ulceration, metastasis at diagnosis, hematological alterations, treatment and clinical outcome.
Referring clinicians and/or cat owners were contacted to gather additional information on vaccination sites, any history of trauma to the affected limb or to complete any missing data. The absence of any information was not considered an exclusion criterion for the study.
Histopathology and immunohistochemistry
For RCTs, the original haematoxylin and eosin (H&E)-stained slides were retrieved and microscopically reviewed to evaluate cellular morphology and assess additional features, including mitotic count (MC), presence of epitheliotropism, karyomegaly, multinucleation and amyloid deposition. MC was defined as the number of mitotic figures within an area of 2.37 mm2; karyomegaly was defined as the presence of nuclei exceeding 50 μm in diameter – identified at 10× magnification – and multinucleated cells were defined as neoplastic cells containing three or more nuclei. In cases where amorphous interstitial material suspicious for amyloid was observed, Congo Red staining was performed for confirmation.
Automated IHC was conducted using the Discovery ULTRA system (Roche; Ventana Medical Systems) at the diagnostic histopathology laboratory of Istituto Zooprofilattico Sperimentale delle Venezie, Padua, Italy. Detailed information regarding the panel of primary antibodies, dilutions, source, retrieval methods and detection systems is provided in Table 1. Briefly, 3 μm thick formalin-fixed and paraffin-embedded tissue sections from selected blocks were mounted on Superfrost plus slides, deparaffinised in aqueous-based detergent solution (Discovery Wash; Ventana) and underwent heat-induced antigen retrieval. After detection, sections were counterstained with Mayer’s haematoxylin (Hematoxylin II; Ventana), dehydrated and mounted using Eukitt (Kaltek). Each run included positive controls from feline tissues and tumour sections where primary antibodies were omitted (negative controls).
Panel of primary antibodies, dilutions, source, retrieval methods and detection systems
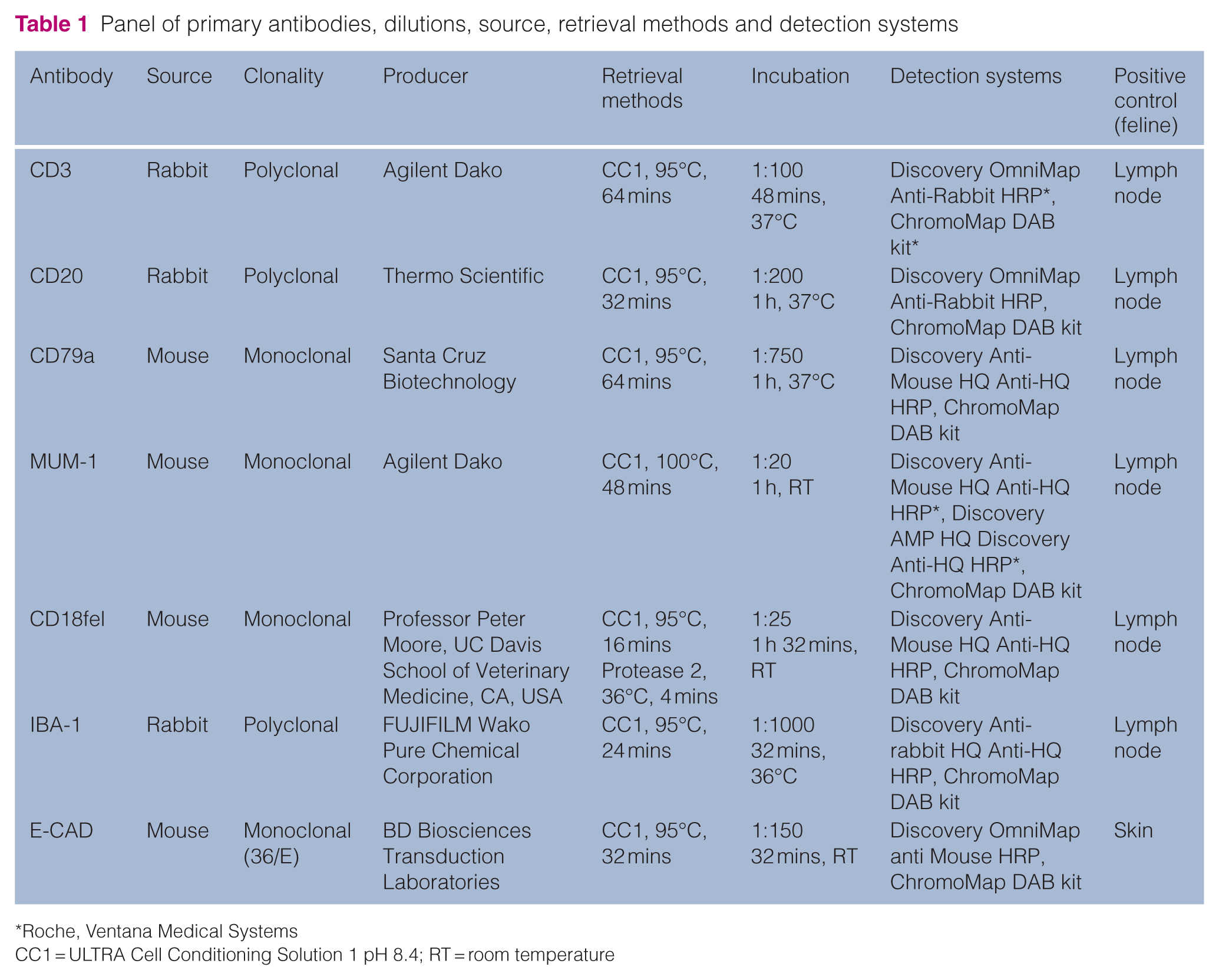
Roche, Ventana Medical Systems
CC1 = ULTRA Cell Conditioning Solution 1 pH 8.4; RT = room temperature
All histological and immunohistochemical evaluations were conducted by a board-certified veterinary pathologist (SS). Final diagnoses were established by integrating morphological and immunohistochemical findings, in accordance with current diagnostic criteria as reported in the diagnostic algorithm outlined in Figure 1.
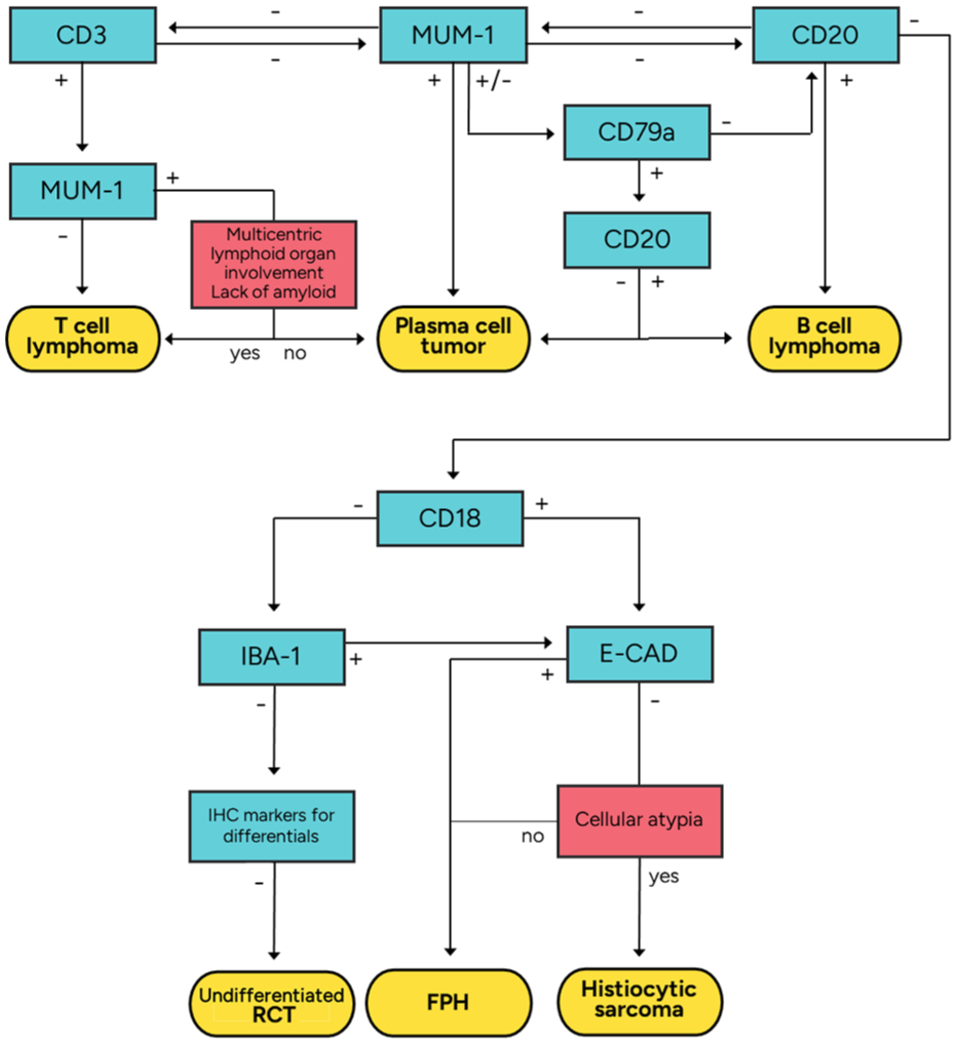
Diagnostic algorithm based on the morphological and immunohistochemical findings. FPH = feline progressive histiocytosis; IHC = immunohistochemistry; RCT = round cell tumour
Statistical analysis
When appropriate, data sets were tested for normality by the Shapiro–Wilk test. Values are presented as mean ± SD for normally distributed data or as median (range) in case of non-normal distribution.
Differences in demographic characteristics and potential risk factors between cats with tarsal STSs and those with RCTs were analysed using the Mann–Whitney U-test for continuous variables and the χ2 test or Fisher’s exact test for categorical variables.
Time to progression (TTP) was defined as the interval between the date of diagnosis and the occurrence of local recurrence, nodal or distant metastasis, or last follow-up if progression did not occur. Survival time (ST) was defined as the interval between diagnosis and the date of death or last follow-up, if death did not occur. Cats that died of causes related to the tarsal tumour were considered events. Cats that did not experience tumour progression or death were censored at the time of their last follow-up. Survival estimates were presented as medians with the corresponding 95% confidence intervals (CIs). Survival plots were generated according to the Kaplan–Meier product-limit method and compared by means of the log-rank test.
Data were analysed using SPSS software (IBM). P values ⩽0.05 were considered statistically significant.
Results
Demographic information and clinical presentation
A total of 41 cases of feline tarsal tumours were retrieved. The initial diagnoses included 18 (44%) RCTs (undifferentiated round cell tumour, n = 7; plasma cell tumour, n = 4; lymphoma, n = 3; feline progressive histiocytosis, n = 3; histiocytic sarcoma, n = 1), 16 (39%) STSs (unspecified STS, n = 7; fibrosarcoma, n = 4; undifferentiated pleomorphic sarcoma, n = 2; perivascular wall tumour, n = 1; peripheral nerve sheath tumour, n = 1; liposarcoma, n = 1) and seven other tumours (hemangiosarcoma, n = 2; lipoma, n = 2; osteosarcoma, n = 1; synovial myxoma, n = 1; fibrolipoma, n = 1), which were excluded from the analysis as they were not classified within either of the two groups of interest. The 16 STSs had been previously graded according to the grading system proposed by Dobromylskyj et al, 27 as reported in the original histopathology reports (grade 1, n = 3; grade 2, n = 13).
Demographic information and clinico-pathological data are summarised in Table 2.
Demographic information and clinical presentation in 18 feline tarsal round cell tumours (RCTs) and 16 soft tissue sarcomas (STSs)
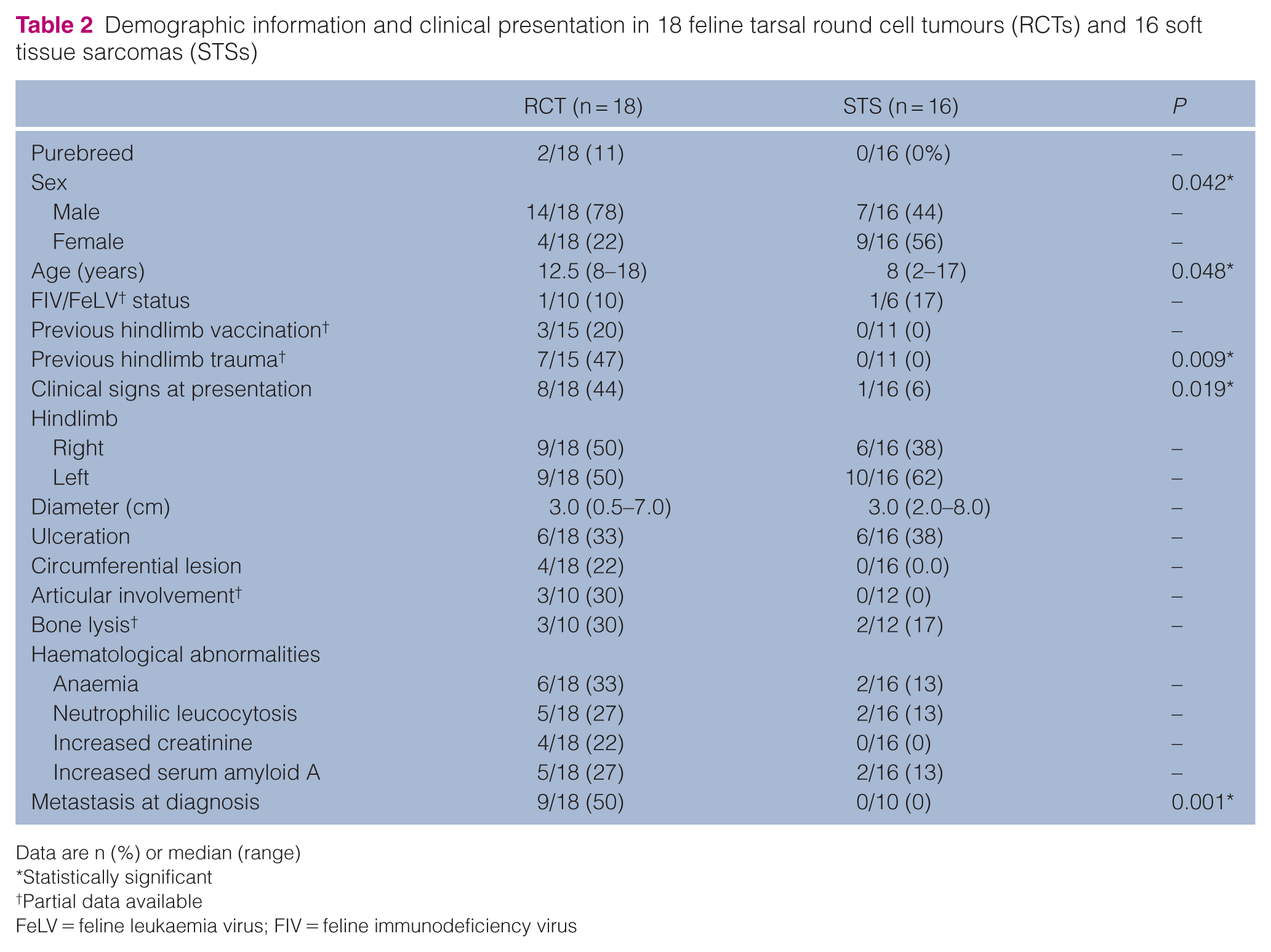
Data are n (%) or median (range)
Statistically significant
Partial data available
FeLV = feline leukaemia virus; FIV = feline immunodeficiency virus
A total of 18 cats had a diagnosis of tarsal RCT. Out of 15 cats with available data, seven (47%) had a history of prior limb trauma, including falls, dog bites, car accidents or fractures. In addition, three (20%) had received at least one hindlimb vaccination during their lifetime. Clinical signs at presentation were reported for eight (44%) cats, including lameness (n = 6), self-harming (n = 3) and asthenia (n = 1). Neoplasms presented as a circumferential mass in four (22%) cases, whereas the other tumours were positioned caudo-medially (n = 3, 17%), dorso-laterally (n = 3, 17%), medially (n = 3, 17%), dorsally (n = 2, 11%), caudally (n = 2, 11%) and laterally (n = 1, 5%). Bone lysis and articular involvement were identified in 3/10 (30%) cases that underwent diagnostic imaging. At diagnosis, nine (50%) cats exhibited cytologically confirmed nodal metastasis (popliteal and inguinal, n = 4; popliteal, n = 4; popliteal and internal iliac, n = 1) and one (7%) had splenic metastasis.
In total, 16 cats were diagnosed with STS. Data on previous trauma to the affected limb and hindlimb vaccination were available for 11 (69%) cases, with no reported history of injuries or vaccinations.
One (6%) cat was asthenic, whereas lameness or other clinical signs were not observed. No neoplasm presented as a circumferential mass. Bone lysis was observed in 2/12 (17%) cases that underwent diagnostic imaging, while no joint involvement was detected in any of the cats. None of the cats had metastasis at first presentation.
Male cats were significantly more common in the RCT group than in the STS group (78% vs 44%; P = 0.042), and cats in the RCT group were older (median age 12.5 years vs 8 years; P = 0.048). A history of previous trauma to the affected limb was significantly associated with a diagnosis of RCT (P = 0.009). Clinical signs at presentation and the presence of metastases at diagnosis were also more frequent in the RCT group (P = 0.019 and P = 0.001, respectively).
Histopathology and immunohistochemistry
Based on the proposed diagnostic algorithm (Figure 1), 18 RCTs were reclassified as follows: seven (39%) plasma cell tumours, four (22%) FPHs, three (17%) lymphomas (two T-cell lymphoma, one B-cell lymphoma), two (11%) histiocytic sarcomas and two (11%) undifferentiated RCTs. Initial and final diagnoses are listed in Table 3. Overall, the final diagnosis differed from the original histological diagnosis in nine (50%) cases. The median MC was 8 (range 0–24; lymphoma: 18; undifferentiated RCT: 11.5; histiocytic sarcoma: 8.5; plasma cell tumour: 6; FPH: 3.5). Multinucleation was observed in seven cases (plasma cell tumour, n = 4; FPH, n = 2; histiocytic sarcoma, n = 1), karyomegaly in six cases (plasma cell tumour, n = 4; histiocytic sarcoma, n = 2), epitheliotropism in four cases (FPH, n = 2; lymphoma, n = 1; undifferentiated RCT, n = 1). The presence of amyloid was documented with Congo red staining in two cases with a final diagnosis of plasma cell tumour.
Histological and immunohistochemistry review in a population of 18 feline tarsal round cell tumours (RCTs)
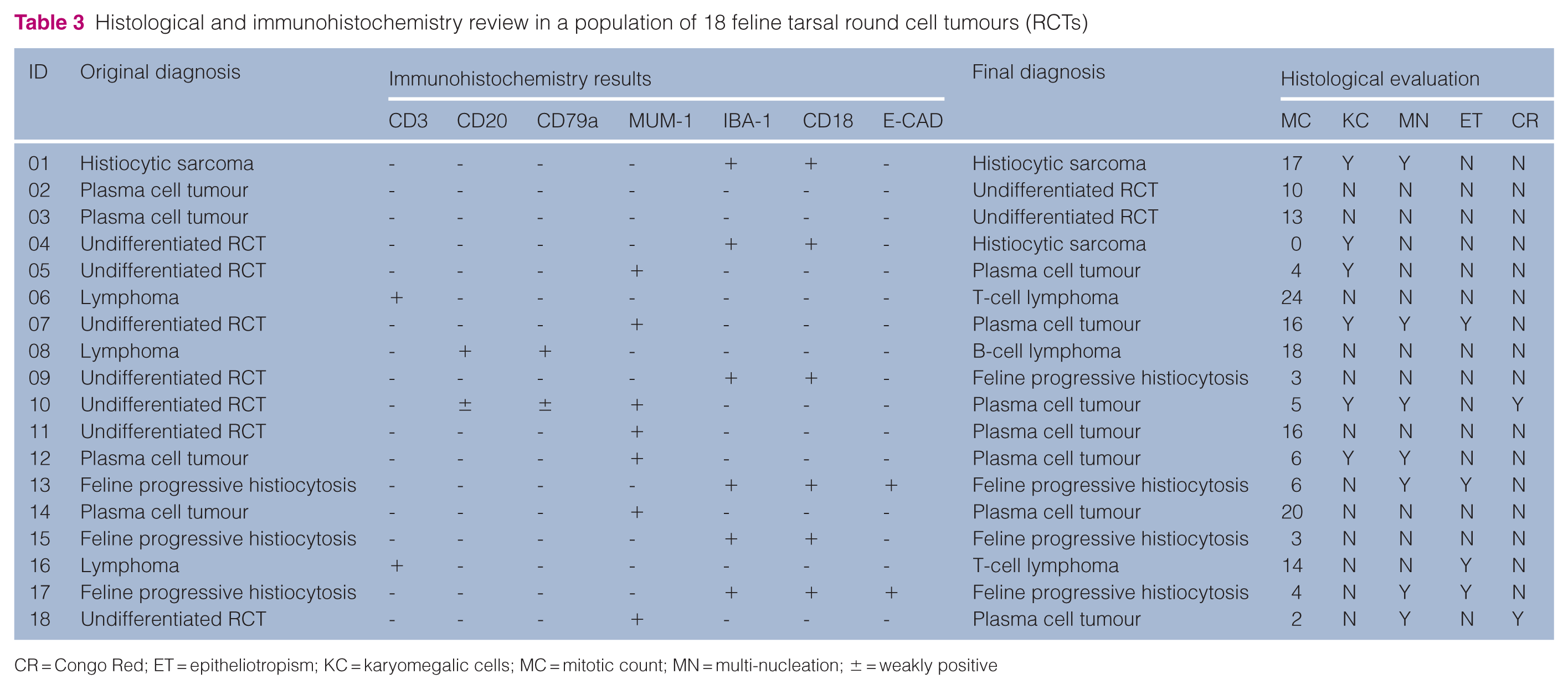
CR = Congo Red; ET = epitheliotropism; KC = karyomegalic cells; MC = mitotic count; MN = multi-nucleation; ± = weakly positive
The data summarised above are presented in Table 3, while representative images of H&E-stained sections and immunohistochemical findings are shown in Figure 2.
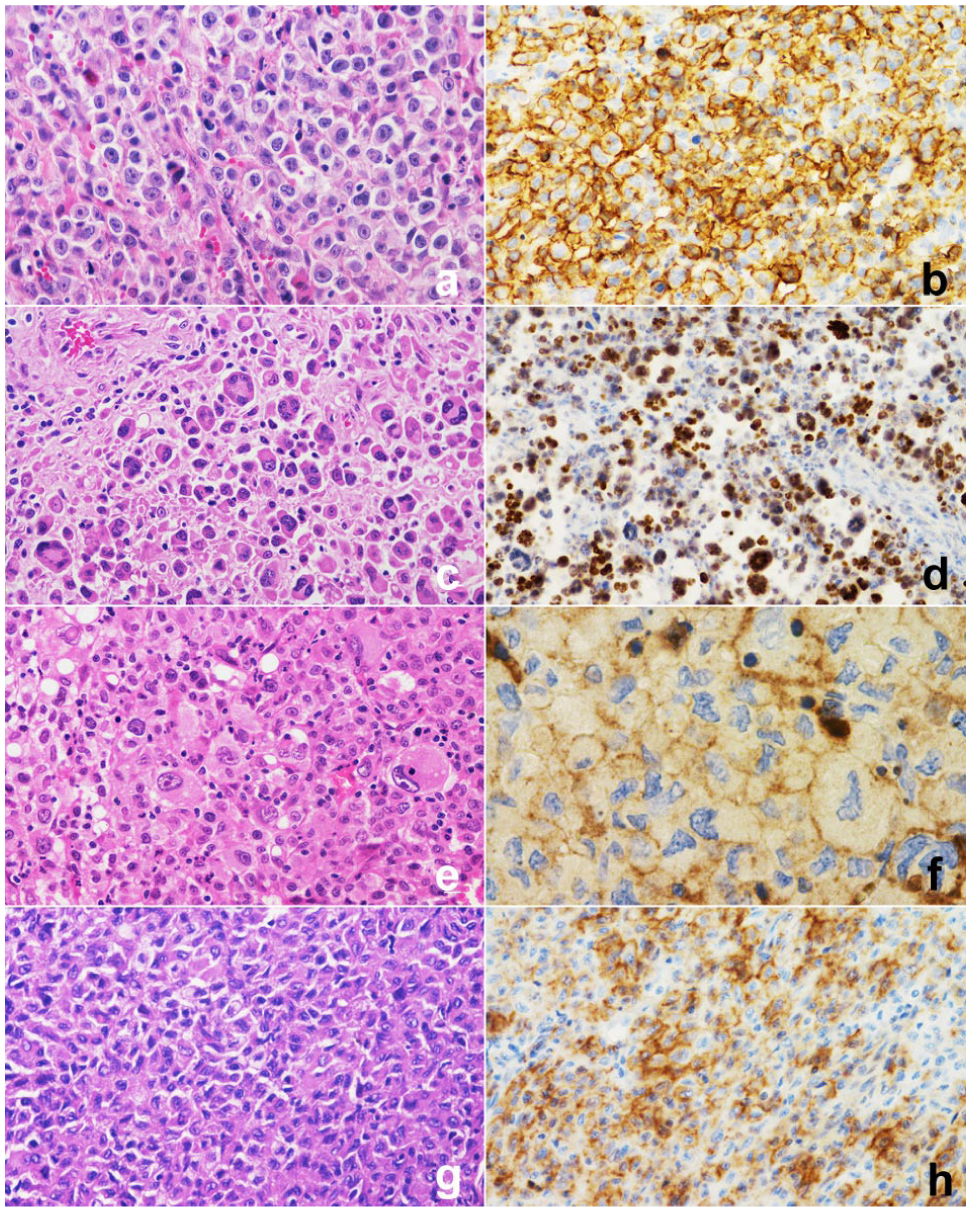
Representative examples of histological sections stained with haematoxylin and eosin (H&E) and immunohistochemistry (IHC) preparations from four cases of tarsal round cell tumours. (a) Lymphoma; H&E; 40×. (b) Lymphoma; CD20 IHC; 40×. (c) Plasma cell tumour; H&E; 20×. (d) Plasma cell tumour; MUM-1 IHC; 20×. (e) Histiocytic sarcoma; H&E; 40×. (f) Histiocytic sarcoma; IBA-1 IHC; 40×. (g) Feline progressive histiocytosis; H&E; 40×. (h) Feline progressive histiocytosis; E-Cadherin IHC; 40×
Treatment and outcome
RCT group
Among cats with plasma cell tumours, 4/7 (57%) had lymph node metastasis at first presentation. Three (43%) cats received melphalan and prednisolone, two (29%) underwent hindlimb amputation and adjuvant melphalan and prednisolone, one (14%) cat was treated with prednisolone alone and one (14%) underwent marginal excision followed by amputation after local recurrence. Tumour progression was observed in all cases (distant, n = 2; local, n = 2; nodal and distant, n = 2; local, nodal and distant, n = 1). Nodal and distant metastases were confirmed cytologically in all cases. All cats died because of cancer-related events after a median time of 81 days (range 8–356).
Treatment and follow-up data were available for 3/4 (75%) cats with FPH. None had metastasis at presentation. Two underwent marginal excision, and one received lomustine and prednisolone. Tumour progression occurred in two cases, both of which died because of disease 196 and 366 days after presentation. The third cat was euthanased because of unrelated renal disease after 367 days.
At the time of diagnosis, all three cats with lymphoma had lymph node involvement (popliteal and inguinal, n = 2; popliteal, n = 1) and one (33%) also had splenic involvement. Two cats received cyclophosphamide, doxorubicin, vincristine and prednisolone (CHOP) chemotherapy, and the third cat was treated with lomustine and prednisolone. Tumour progression was documented in all cases, with cats succumbing to cancer-related events at 27, 47 and 171 days after initial presentation.
Treatment and follow-up data were available for 1/2 (50%) cats with histiocytic sarcoma. This cat had lymph node metastasis at diagnosis and subsequently developed cytologically proven nodal and hepatic dissemination, surviving 283 days without receiving any treatment.
Of the two cats with undifferentiated RCT, one (50%) had lymph node metastasis at first presentation. Both cats underwent marginal excision followed by amputation after developing local recurrence and died from cancer-related causes 71 and 173 days after initial presentation.
Overall, the median TTP for cats with RCTs was 139 days (95% CI 0–280) and the median ST was 173 days (95% CI 33–313). Tumour-related events accounted for the death of 14/15 (93%) cats, with a one-year survival rate of 6.7%.
STS group
Follow-up data were available for 12/16 (75%) cats. All underwent surgery (hindlimb amputation, n = 7; marginal excision, n = 5). None received adjuvant chemotherapy. In 4/5 (80%) animals treated with marginal excision, local recurrence was observed after 322, 329, 425 and 854 days, and was successfully managed with hindlimb amputation. No nodal or distant progression was reported.
The median TTP was 854 days (95% CI 27–1681). Among the amputated cats, one died 2 days after surgery because of postoperative complications; another cat died of cardiopulmonary arrest in the absence of progression 47 days after surgery. All the remaining cats were alive and free from metastasis at the end of the study, after a median follow-up period of 638 days (range 73–1354). The median ST was not reached, and the 1-year survival rate was 80%.
Both TTP and ST were significantly shorter among cats with RCTs compared with those with STSs (P <0.001).
Discussion
Although several case series and reports have suggested a predilection of different RCT histotypes for the feline hock region, many of these studies lack the comprehensive immunophenotyping necessary to reach a definitive diagnosis.1–6,28 As a result, clinicians must rely on inconsistent prognostic information based on inaccurate classification.
The primary diagnostic challenge lies in differentiating lymphoma from plasma cell tumours, particularly because of the reported co-expression of CD3 and MUM-1 in feline plasma cell tumours of the tarsal region, which complicates the application of conventional diagnostic criteria. 15 This overlapping immunophenotypic profile raises concerns about the potential misclassification of cases when relying on standard immunohistochemical panels. To date, feline tarsal lymphoma has been described as non-epitheliotropic, with immunophenotyping conducted in only two-thirds of reported cases and without incorporating MUM-1 IHC. Furthermore, amyloid production was observed in two cases diagnosed as lymphoma, including one that lacked lymphoid marker expression. 1 Conversely, the only published study on feline tarsal plasma cell tumours relied solely on MUM-1 as the marker for case inclusion. 2 These diagnostic limitations underscore the need for expanded immunohistochemical panels and molecular analyses to improve diagnostic accuracy in feline tarsal RCTs.
In this retrospective study, we aimed to determine the proportion of RCTs in a series of feline tarsal neoplasms and to classify them accurately using a comprehensive IHC panel. In addition, we evaluated the clinicopathological characteristics of these tumours and compared their biological behaviour to that of tarsal STSs, which are also frequently observed at this anatomical site.29–31
Our results were consistent with the existing literature,1,2,15,16 confirming that the hock region is frequently affected by RCTs, representing 44% of cases in our series.
As expected, IHC proved essential for the differential diagnosis of feline tarsal RCTs. Based on histopathology alone, 39% of the neoplasms were initially categorised as undifferentiated RCTs. However, incorporation of IHC within a structured diagnostic algorithm allowed identification of the tumour histotype in 89% of cases, resulting in a revision of the initial diagnosis in half of the cases. This highlights the critical role of IHC in reducing diagnostic ambiguity.
Nevertheless, IHC does not invariably allow a definitive diagnosis. Davidson et al 21 also emphasised the intrinsic difficulty in definitively classifying a subset of feline RCTs, despite the use of an extensive immunohistochemical panel, with some tumours remaining categorised as undifferentiated. In that study, as in ours, relatively few IHC markers were consistently expressed in all tumours of a given final diagnosis, and many markers lacked strict lineage specificity. 21 In addition, IHC results may be influenced by several factors, including tissue fixation, antibody selection and staining protocol, and some anaplastic tumours may lack expression of all tested markers.16,17,19,20 Consequently, a small proportion of neoplasms may remain unclassified despite extensive immunophenotyping, as observed in two cases in this study. In such instances, rare mesenchymal neoplasms with round cell morphology, including rhabdomyosarcoma, may also enter the differential diagnosis; however, the absence of characteristic morphological features and the atypical anatomical localisation made this interpretation unlikely in our cases.
Interestingly, in this study the final diagnoses encompassed all the previously reported histotypes, including plasma cell tumour, FPH, T-cell lymphoma, B-cell lymphoma and histiocytic sarcoma. Co-expression of MUM-1 and CD3 was not observed in our cases, in contrast to recent reports,15,21 probably due to the limited number of cases. In cases positive for both MUM-1 and CD3, the presence of amyloid, clonal rearrangement of the immunoglobulin gene or serum monoclonal immunoglobulin may also be evaluated. 15
In agreement with previous findings, interpretation of IBA-1 labelling proved challenging, as variable numbers of IBA-1-positive cells may be present within non-histiocytic tumors. 21 These cells likely represent tumour-associated macrophages or dendritic cells rather than true neoplastic histiocytic populations. This reinforces the importance of using broad IHC panels and interpreting immunoreactivity in conjunction with its distribution pattern and cell morphology.
In our study, feline tarsal RCTs were more commonly observed in older cats compared with STSs, with a male predisposition. This aligns with previous reports on tarsal B-cell lymphomas and plasma cell tumors.1,2
In addition, nearly half of the cats with RCTs had a history of local trauma, whereas no previous injuries were reported in cats with STSs. These findings suggest possible hypotheses about the pathogenesis of tarsal RCTs. The hock region is subjected to continuous mechanical stress in hopper-animals like cats: the feline calcaneal bone has a more prominent tuberosity compared with its canine counterpart, providing increased leverage but also contributing to local stress and a higher susceptibility to inflammation. 32 In male cats, this anatomical feature is further accentuated, as the calcaneus extends more compared with females. 33 Additionally, the hock region in cats is particularly vulnerable to injuries caused by car accidents, falls or dog bites, especially in male cats, which are at higher risk because of their larger roaming territories.34,35 Trauma and inflammation have been linked to RCTs in cats;36–38 however, their role in the development of feline tarsal RCTs remains speculative and requires further investigation in larger populations.
In this study, nearly half of the cats with RCTs exhibited local clinical signs at first presentation, such as limping and self-trauma. In contrast, clinical signs were uncommon in cats with STSs.
In addition, more than half of the cats in the RCT group presented with metastatic disease at the time of diagnosis, highlighting the aggressive nature of these tumours. Metastases were mainly identified in the regional lymph nodes, with only one cat having splenic involvement. In contrast, no evidence of metastasis was detected in any of the cats within the STS group, suggesting a more localised disease process in these tumours.
In our study, tarsal RCTs appeared to have a poorer prognosis compared with STSs, with shorter TTP and ST. Although hindlimb amputation proved to be an effective treatment for tarsal STSs, resulting in no local recurrence, it did not achieve comparable disease control in cats with RCTs. These findings suggest biological differences between RCTs and STSs;1–5,39–41 however, we recognise that the small sample size limits the strength of these conclusions and that these findings should be validated in larger cohorts.
As a result of the limited number of cases, no statistical comparison could be made regarding the biological behaviour among RCT histotypes. Nevertheless, descriptive observations indicated marked variability: lymphomas exhibited the most aggressive clinical course, characterised by large, circumferential masses, multifocal nodal involvement at diagnosis, rapid progression and short survival. In contrast, cats with FPH exhibited a more indolent disease progression, with survival times approaching 1 year.
The main limitation of this study lies in the small sample size, which is consistent with the low incidence of tarsal neoplasms. In addition, follow-ups were not available for all cases, reducing the statistical power for data analysis. Finally, the cases were collected over a period of 15 years, leading to variations in diagnostic and therapeutic approaches. These factors hindered direct comparison among histotypes and complicated the evaluation of treatment response.
Conclusions
Feline RCTs arising in the tarsal region appear to predominantly affect elderly male cats, and local trauma and inflammation may contribute to their development. IHC is essential for establishing a definitive diagnosis and reducing the rate of ambiguous classifications. Using a standardised diagnostic algorithm integrating histopathology and IHC allowed accurate classification of tumour histotypes in our cohort. Further studies involving larger and more homogeneous populations are necessary to identify the most effective therapeutic strategies.
Footnotes
Author note
The data that support the findings of this study are available on request from the corresponding author.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.