
Abstract
Objectives
The aim of the present study was to report the outcome and postoperative complications of wound reconstruction in cats using axial pattern flaps (APFs) and subdermal plexus flaps (SPFs), and to assess associations between location, indication, flap type, postoperative complications and outcomes.
Methods
The surgical records of 52 cats undergoing 62 SPF or APF reconstructions were retrospectively reviewed between 2014 and 2025. Data collected included signalment, indication, location, flap type, postoperative complications and outcomes. Descriptive analyses and associations between variables were assessed.
Results
Chronic wounds were the most common indication (n = 53/62, 85.5%), followed by mass removal and acute wounds. Among APFs, the lateral caudal flap was the most employed (n = 7/30, 23.3%), while the skin fold flap was the most frequent SPF (n = 19/32, 59.4%). A significant association was observed between anatomical location and clinical indication (P = 0.028). Overall complication rates did not differ significantly between APFs and SPFs. The most frequently observed complications were necrosis (45.2%) in all flaps. No significant associations were identified between clinical indication and wound dehiscence. Flap dehiscence was significantly more prevalent in SPFs applied to the dorsal body (n = 7/8, 87.5%; P = 0.032).
Conclusions and relevance
APFs and SPFs demonstrated comparable overall complication rates in feline wound reconstruction, with chronic wounds being the most common indication. Anatomical location was associated with wound dehiscence only in the dorsal body, with more wound dehiscence in SPFs than APFs, emphasising the importance of careful flap selection for each body area.
Plain language summary
This study examined two types of skin flap surgery used to treat wounds in cats. These procedures involve moving nearby skin to cover and close wounds. We reviewed medical records from 52 cats that underwent a total of 62 surgeries between 2014 and 2025. Most procedures were performed to treat long-lasting wounds, while others followed mass removal or recent injuries. Both types of skin flaps showed similar results, with comparable rates of complications. The most common issue was partial loss of the flap. Several factors may have influenced wound healing, although the findings are limited by study constraints. For example, wounds located on the back and treated with a specific flap type were more likely to develop dehiscence after surgery. In summary, both techniques appear to be effective options for treating wounds in cats. Careful flap selection for each part of the body may help reduce the risk of complications.
Introduction
Skin flaps provide full-thickness skin coverage with blood supply and are commonly utilised to reconstruct wounds, particularly in areas with poor vascularity, high tension or limited immobilisation.1,2 Skin flaps are important in cats because thinner skin, less subcutaneous tissue and greater skin mobility increase the risk of delayed wound healing.3,4 Based on their vascular supply, skin flaps are categorised as axial pattern flaps (APFs) or subdermal plexus flaps (SPFs). APFs are supplied by a named direct cutaneous artery and vein, allowing for more predictable perfusion and use in larger or higher tension defects.1,5 In contrast, SPFs rely on the subdermal vascular plexus and lack a specific named vessel, which may limit flap length and durability.6,7 Insufficient blood supply may increase the risk of distal flap necrosis when excessive flap length is used. Various case reports have described these techniques, with APFs subclassified according to their named vascular pedicles and SPFs generally subdivided by flap movement and anatomical location (eg, skin fold flaps).5 –8
Previous larger studies in small animals have reported relatively high complication rates after skin flap surgery, with outcomes modulated by multiple factors.9 –11 Most studies combined dogs and cats, rendering it uncertain whether APFs and SPFs perform differently in cats.9,10 Cats have thinner skin and sparse subcutaneous fat compared with dogs, resulting in increased skin mobility.3,4 Cats also have a less dense subdermal plexus compared with dogs,12,13 which can make flap surgery more challenging by reducing blood flow during tension or stretching and increasing the risk of dehiscence or necrosis. The effects of surgical location and indication on flap outcomes in cats are also unknown. Feline-specific evidence is therefore essential to guide flap selection and perioperative care.
In the present study, the types, locations and indications of APFs and SPFs used in cats were described. Postoperative complications were compared between flap types. The indication and location on flap outcomes were evaluated.
Materials and methods
This retrospective study was conducted at Kasetsart University Veterinary Teaching Hospital, Bangkok. Surgical records of cats that underwent SPF or APF reconstruction were analysed between October 2014 and September 2025. Breed, age, sex, flap type and subtype, surgical location and clinical indication were recorded. Anatomical locations were categorised as head and neck, dorsal body, ventral body, proximal limb, distal limb and perineal region. The proximal limb was defined as regions proximal to the elbow and stifle, while the distal limb included regions distal to these joints.
The dorsal and ventral body regions were defined relative to a mid-horizontal plane dividing the body into dorsal and ventral halves. Wounds located on the lateral body wall were categorised based on their predominant position relative to this plane. Indications were classified as mass removal, acute wounds or chronic wounds. Mass removal referred to immediate reconstruction after tumour excision. Acute wounds were traumatic injuries treated surgically without prior unsuccessful wound management, whereas chronic wounds failed to heal within the expected time frame or after previous treatment. Chronic wounds were managed before reconstruction using standard wound care principles,14,15 including clipping and antiseptic preparation of the periwound area, repeated debridement as needed, lavage with balanced crystalloid solution or antiseptic solutions, and appropriate use of topical antiseptics, dressings and bandaging based on wound condition and exudate. Wounds were regularly re-evaluated, and flap reconstruction was performed once a healthy granulation tissue bed was achieved and infection was controlled, when feasible. All procedures followed standard skin flap techniques,5,7 with flaps maintained on a pedicle at the donor site.
Feline skin flap procedures
The skin flaps were classified as SPFs or APFs based on blood supply. Both types were performed using standard surgical techniques, keeping the flap attached to its original site (pedicle) to preserve blood flow. When a cat had multiple wounds, each flap was evaluated separately. All procedures were performed at a single institution by one of three board-certified surgeons (Diplomate Thai Board of Veterinary Surgery), with each case managed by a single surgeon. The surgeon decided whether to place a drain and drain types (ie, Penrose drains or Jackson–Pratt drains). The subcutaneous layer of flap was sutured to the recipient site routinely with a simple continuous pattern, using 3-0 or 4-0 monofilament absorbable suture (polydioxanone, PDS II; Ethicon). The skin was closed using 3-0 or 4-0 monofilament non-absorbable suture (nylon, Dafilon; B Braun) in a simple interrupted pattern.
Perioperative analgesia protocols were determined at the discretion of the attending anaesthesiologist but generally included opioids (eg, morphine, fentanyl, ketamine or fentanyl–ketamine constant rate infusion). Postoperative analgesia typically consisted of opioids (administered intravenously, subcutaneously or via transdermal fentanyl patches) and/or non-steroidal anti-inflammatory drugs (eg, robenacoxib, meloxicam or tofenamic acid), unless contraindicated.
Outcome assessments
Postoperative complications were recorded during hospitalisation and follow-up until the sutures were removed or the problem was resolved. These included oedema, bruising, wound discharge, skin necrosis, infection, dehiscence and the need for additional surgery. Wound discharge was defined as abnormal discharge from the surgical site and did not include expected drainage from surgically placed drains. Outcomes were classified as wound dehiscence, defined as partial or complete separation of the flap edges, and skin necrosis, characterised by dark black discoloration of the tissue requiring removal. Successful healing was defined as complete flap healing without separation or tissue death. Surgical site infections were recorded but not included in the outcome analysis, as the study focused on structural flap outcomes (eg, dehiscence vs successful healing).
Statistical analysis
A descriptive analysis was performed to summarise the signalment, flap type and subtype, surgical location, clinical indication, postoperative complications and outcomes. Fisher’s exact test was used to assess associations between location and clinical indication, flap type and postoperative complications, indication and wound dehiscence, and anatomical location and wound dehiscence. All analyses were performed using Stata version 12.1 (StataCorp), and P <0.05 was considered statistically significant.
Results
A total of 52 cats (28 males and 24 females) were included, most of which were domestic shorthairs (n = 47), followed by Persian (n = 4) and one Scottish Fold. The median age at the time of flap surgery was 24 months (range 5–120). Overall, 62 skin flaps were performed, comprising 30 APFs and 32 SPFs. Among the cats, 44 (84%) received a single flap, while three (6%) received two APFs, three (6%) received one APF and one SPF, one (2%) received one APF and two SPFs, and one (2%) received three SPFs. All cats receiving multiple flaps had separate wound sites. Of the eight cats requiring multiple skin flaps for wound closure, six underwent all flap procedures in a single surgical session, while two received additional flaps at later stages based on wound readiness. Among the 11 APFs, the lateral caudal flap was the most common (n = 7/30), followed by the caudal superficial epigastric and lateral thoracic flaps (Figure 1). Among SPFs, the skin fold flap was most common (n = 19/32), with the majority being inguinal (n = 18/19) and only one axillary fold flap identified, followed by single pedicle advancement and transposition flaps. The rotational flaps were infrequently performed.
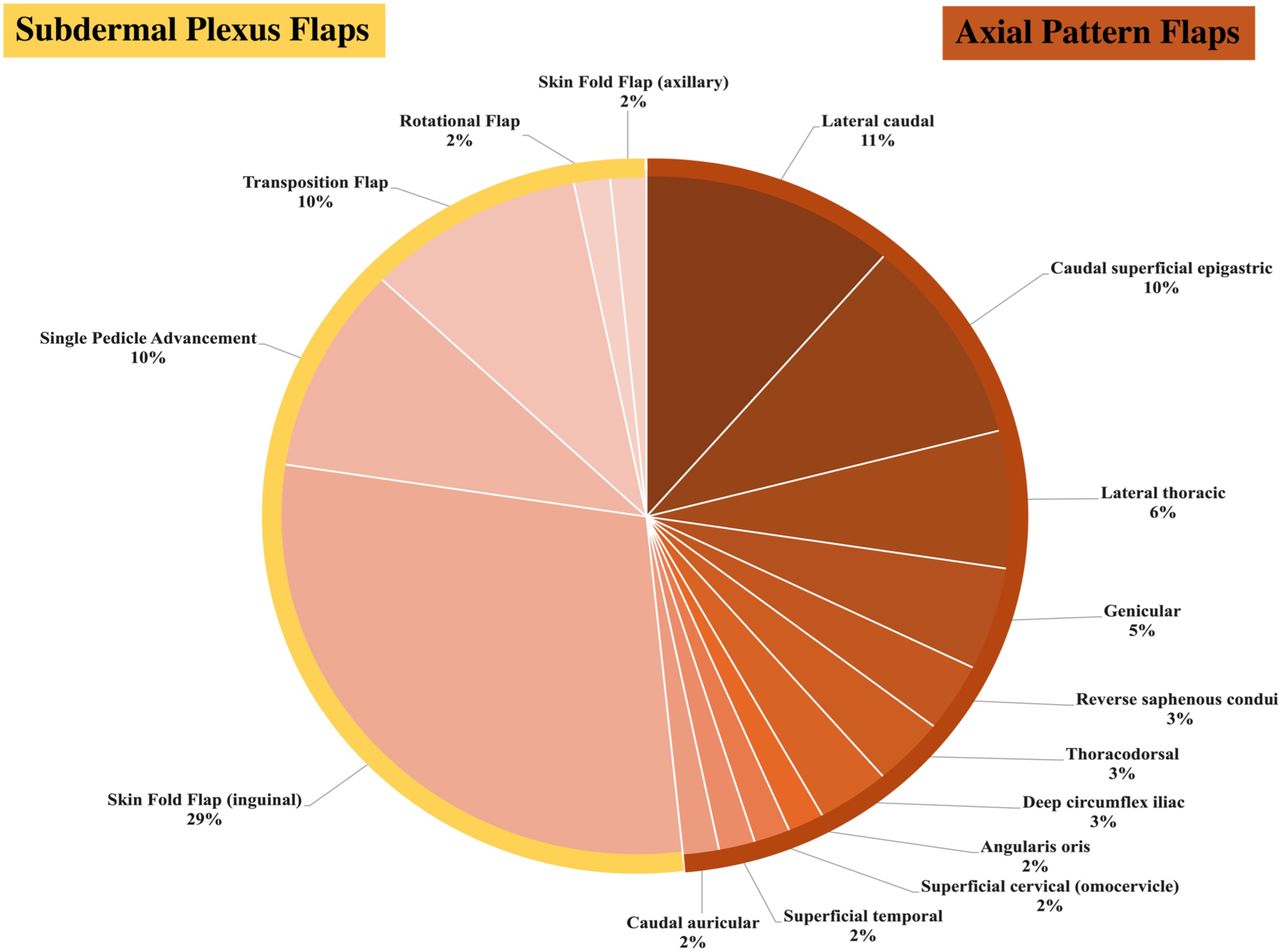
Distribution of axial pattern flaps and subdermal plexus flaps in cats
The APF and SPF groups did not differ significantly in baseline characteristics. The mean ± SD age was comparable between groups (37 ± 33 months for APFs vs 35 ± 27 months for SPFs; P = 0.218). Sex distribution was also similar, with equal numbers of males and females in the APF group (n = 15/30, 50% each) and a comparable distribution in the SPF group (male: 18/32, 56.2%; female: 14/32, 43.8%); with no significant difference between groups (P = 0.622). The proximal limb was the most common surgical location, whereas the perineum was the least (Table 1). Chronic wounds were the primary indication (n = 53/62, 85.5%), followed by mass removal (n = 8/62, 12.9%) and acute wounds (n = 1/62, 1.6%). A significant association was observed between anatomical location and indication (P = 0.028). Flap use for wounds after mass removal was most commonly performed in the head and neck region, whereas flap use for chronic wounds was more frequently observed in the dorsal body, ventral body and limb regions.
Locations and indications of feline skin flap surgery
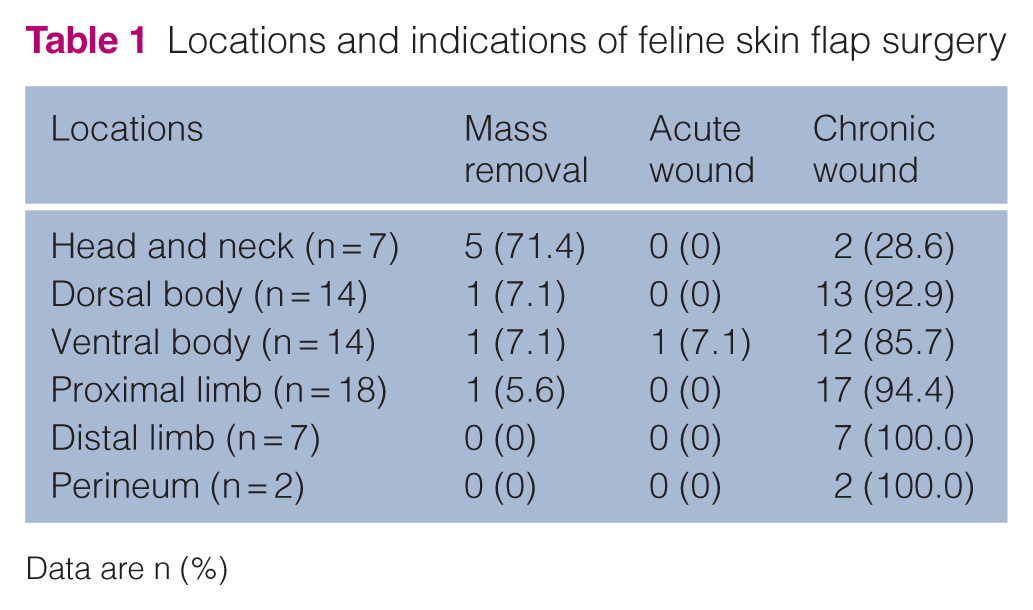
Data are n (%)
In total, 9/30 (30.0%) APFs and 13/32 (40.6%) SPFs had no postoperative complications. Accordingly, postoperative complications were identified in 21/30 (70.0%) APFs and 19/32 (59.4%) SPFs, with an overall complication rate of 64.5% (n = 40/62 flaps). There was no significant difference in complication rates between APFs and SPFs (P = 0.434). The most frequently observed complications were necrosis (n = 28/62, 45.2%), bruising (n = 25/62, 40.3%), oedema (n = 21/62, 33.9%) and dehiscence (n = 13/62, 21%), while wound discharge was less common (n = 3/62, 4.8%). Postoperative infection (Proteus mirabilis and Enterobacter cloacae) was found in one flap, which resolved with systemic antibiotics and wound treatment. Two cats required surgical revision: one for flap necrosis and one for wound dehiscence. Both healed uneventfully using a simple appositional technique.
Postoperative complications varied by anatomical location (Table 2), with limb reconstructions showing a higher frequency than dorsal and ventral body wounds. Oedema and bruising were most commonly observed in the limbs. Skin necrosis was noted across several regions, including the dorsal body and limbs, whereas wound discharge was uncommon and limited to dorsal body flaps. The frequencies of oedema, bruising, skin necrosis and dehiscence were comparable between APFs and SPFs, with no statistically significant differences (Table 3).
Locations and postoperative complications of feline skin flap surgery

Data are n (%)
Postoperative complications in skin flaps performed in cats, by flap type (axial pattern flaps [APFs] vs subdermal plexus flaps [SPFs])
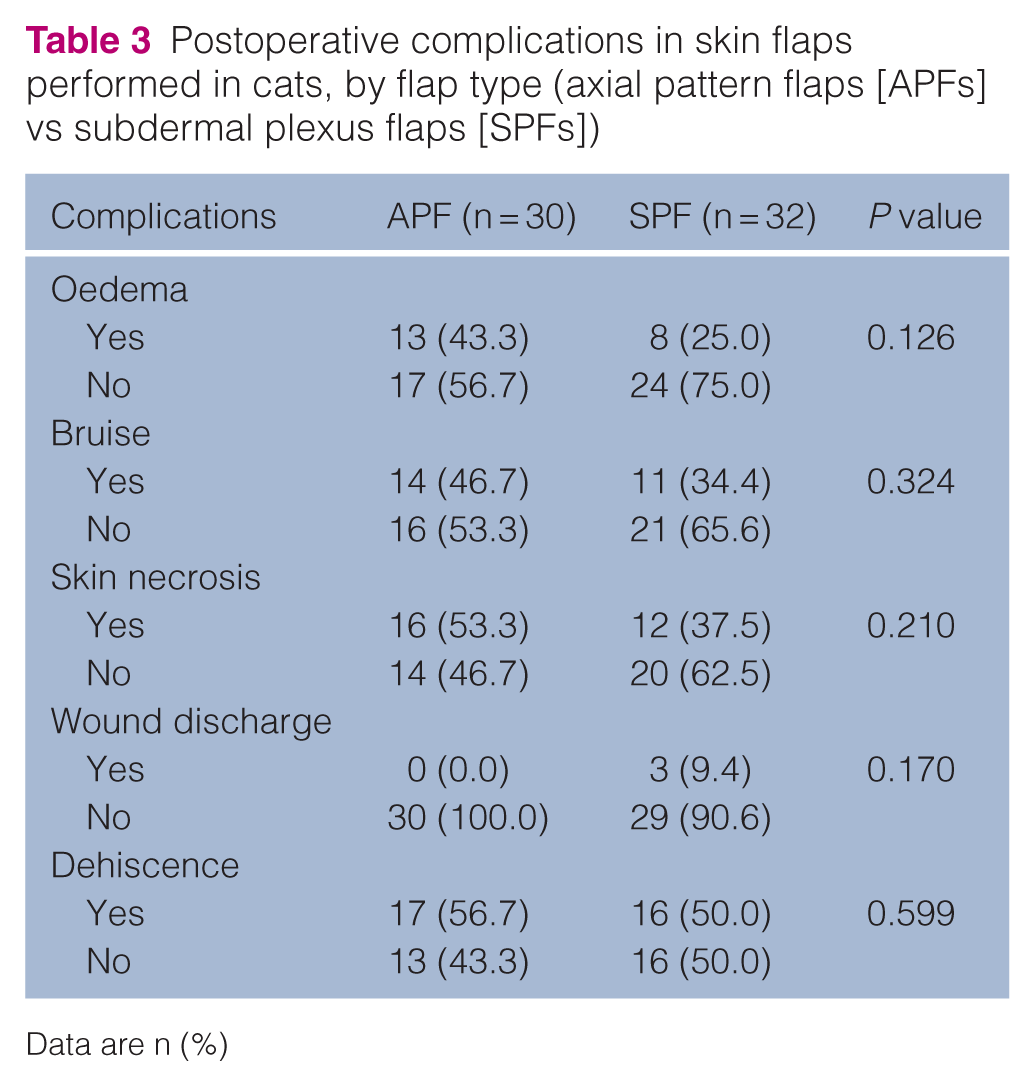
Data are n (%)
Wound dehiscence did not differ significantly among clinical indications (P = 1.000), with similar proportions observed in mass removal (50.0%) and chronic wounds (45.3%). Dehiscence was observed in the single acute wound case. Wound dehiscence varied by anatomical location (Table 4), and an association between anatomical location and wound dehiscence was identified only in the dorsal body, where SPFs had a higher rate of dehiscence than APFs. No significant differences were observed in other anatomical regions.
Association between anatomical location and wound dehiscence in feline skin flap surgery
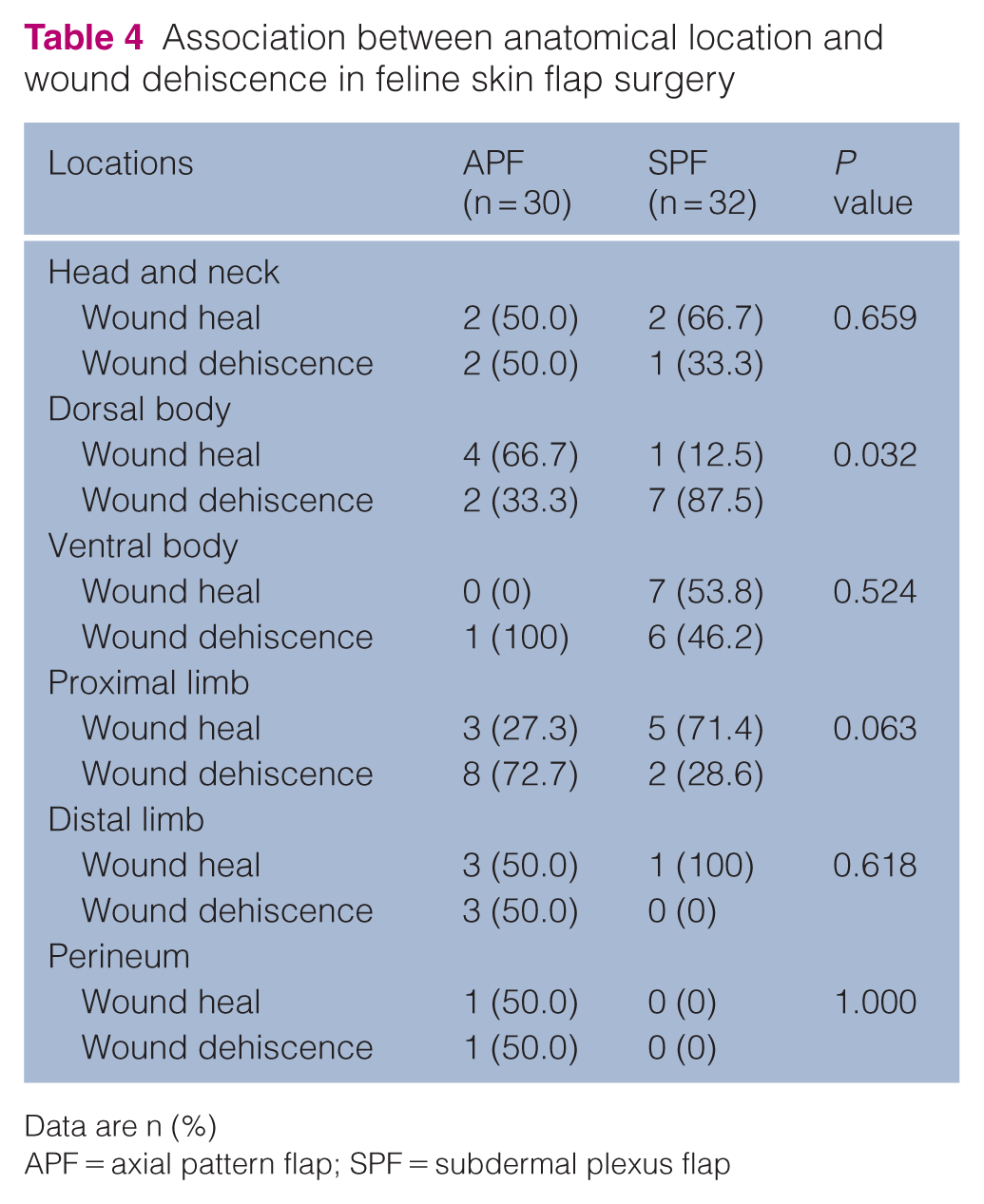
Data are n (%)
APF = axial pattern flap; SPF = subdermal plexus flap
Discussion
In the present study, chronic wounds represented the most common indication for flap surgery in cats, while mass removal and acute wounds were substantially less frequent. This finding is consistent with previous reports in small animals, where chronic wounds more often require flap reconstruction than acute injuries.9,10 In this study, chronic wounds were generally managed to achieve a healthy granulation tissue bed before flap reconstruction, when possible. The high proportion of chronic wounds in cats likely reflects species-specific differences in wound healing. Compared with dogs, cats form granulation tissue more slowly and show delayed epithelialisation and wound contraction. 13 Once wounds become chronic and fail to respond to conservative management, adequate blood supply emerges as a major limiting factor, making skin flap reconstruction an effective option in feline patients. No significant association was observed between clinical indication and wound dehiscence in this study; however, this finding should be interpreted with caution given the imbalance in group sizes and the very low number of acute wound cases.
The skin fold flap was the most commonly utilised flap type in this study, consistent with previous work. 16 The high elasticity of feline skin, particularly in the axillary and inguinal regions, makes skin fold flaps suitable for covering defects in various locations. Among APFs, the lateral caudal flap was employed most frequently, followed by the caudal superficial epigastric flap. The lateral caudal flap was frequently used for defects on the caudodorsal body, especially in chronic wounds. This flap provides a large amount of donor skin and a reliable blood supply from the lateral caudal artery and vein, making it suitable for dorsal body reconstruction.17,18 The caudal superficial epigastric flap was found to be the second most used. It represents a versatile option in cats, with greater distal reach in the hindlimb compared with dogs.19 –21 Both flaps have demonstrated favourable outcomes in cats, supporting their use in feline reconstructive surgery. 22
The proximal limb was the most common site requiring flap reconstruction, consistent with previous reports.9,10,16 This region presents substantial challenges because of high tension, limited skin availability and constant movement. 4 Limb wounds may expose joints or other vital structures; therefore, skin flaps provide the reliable, vascularised coverage needed in this area. Distal limb wounds are particularly difficult to manage because of limited subcutaneous tissue, high mobility and variable blood supply, 23 which may contribute to delayed healing and complications such as oedema, bruising and flap necrosis.
The ventral body was another common location for chronic wounds requiring flap reconstruction. Cats rely heavily on an intact subcutaneous layer for normal wound healing. 3 Although this area normally contains abundant subcutaneous tissue, loss of this layer due to trauma, infection or repeated debridement can impair wound healing. In contrast, the dorsal body has minimal subcutaneous tissue and highly mobile skin because of the cutaneous trunci reflex. This combination may increase stress on flaps and likely contributes to higher rates of necrosis and dehiscence, particularly in the SPF group. Minor necrosis that did not require immediate surgical intervention and was managed conservatively until suture removal was observed in some cases. SPFs depend on a limited microvascular supply and are inherently more susceptible to complications in high-motion or high-tension areas.6,7,9,11
Postoperative complications were common in both APFs and SPFs, with no significant difference in overall complication rates between flap types in this study. Complications occurred in 59.4% of SPFs, with only 1/32 (3.1%) cases requiring revision surgery. This is comparable to previous feline studies, in which up to 43% of SPFs had complications, most of which were minor and managed medically. 9 Surgical location affected outcomes in this study. SPFs on the dorsal body had significantly higher rates of dehiscence than APFs, possibly due to limited vascular supply and biomechanical stress from tail and joint movement.17,18 In contrast, APFs have a more reliable blood supply, supporting better survival in such areas. Preoperative planning and appropriate flap choice may help reduce dehiscence and improve outcomes in cats.
However, complications still occur in APFs. Previous studies reported 83% of APFs with complications, with 38% requiring additional surgery. 10 In this study, 70% of APFs had complications, but only 3% required revision, suggesting most are mild and manageable. In addition to necrosis and dehiscence, other complications included oedema and bruising, which were most commonly observed in the limbs, and occasionally in the head and neck, likely due to changes in vascular or lymphatic drainage. These were self-limiting and did not require further surgery. Wound discharge was rare, occurring only in dorsal body wounds reconstructed with SPFs. This finding is consistent with the limited skin vasculature in cats. 12 Overall, wound discharge was clinically insignificant in this study. Standardised classification systems of complications and outcomes, such as those described by Jones and Lipscomb 9 and Field et al, 10 facilitate comparison between studies. However, interpretation in the present study was limited by its retrospective design, as detailed subclassification was not consistently documented, precluding reliable reclassification using these systems. Given the exploratory aim, analysis of individual complications suggested that certain types were more frequent at specific anatomical locations, and wound dehiscence appeared to be associated with SPFs in particular regions. These findings may provide clinically relevant insights for future studies.
This study has several limitations, including its retrospective design, relatively small sample size, and variation in surgical techniques and postoperative management, which may have influenced the outcomes. In addition, the distribution of clinical indications was imbalanced, with chronic wounds representing the majority of cases, limiting the ability to perform meaningful comparative analysis between indication types. Flap dimensions and sizes, including length:width ratio, were not consistently recorded in the medical records, precluding their evaluation, despite their potential influence on perfusion and complications such as distal necrosis.
Conclusions
This study demonstrated that APFs and SPFs have comparable overall complication rates in feline wound reconstruction, with no significant differences in the frequency of individual complication types. Chronic wounds were the most common indication for reconstruction, and flap selection varied according to anatomical location. Although most complications occurred at similar frequencies between flap types, wound dehiscence in the dorsal body area was more common in SPFs than APFs in cats. These findings suggest that careful flap selection for each body site may influence outcomes and help reduce postoperative complications in cats.
Footnotes
Acknowledgements
The authors gratefully acknowledge the staff at the Kasetsart Veterinary Teaching Hospital, Bangkhen, and the cat owners who participated in this study.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.