
Abstract
Objectives
The aim of the present study was to describe the step-by-step fluoroscopy-assisted percutaneous placement of a cannulated screw (FAPPCS) for the fixation of bilateral sacroiliac luxation (SIL).
Methods
A retrospective study was conducted of the medical records of six client-owned cats diagnosed with bilateral SIL treated using the FAPPCS technique. Signalment, concurrent orthopaedic lesions, size of implant, pre- and postoperative imaging including measurements of screw placement, percentage of reduction and pelvic canal width ratio, hospitalisation time and recovery time were documented. Short- and long-term outcomes were assessed through standard postoperative clinical examination, radiographs and owner questionnaire.
Results
Six cats were treated for bilateral SIL. One minor functional complication (lameness) resolved spontaneously. No major complications were reported. Mean joint reduction was good (right side 96.2% ± 6.6%, left side 98.8% ± 2.9%). The mean absolute angle of deviation was 1.3°. Pelvic canal diameter showed no significant modification. Intraoperative fluoroscopy did not reveal any cranial, ventral or foraminal impingement. Long-term follow-up examinations revealed excellent and moderate functional recuperation in 5/6 and 1/6 cases, respectively. Recovery times were satisfactory: 16.6% fully recovered within 1 month, 50% between 1 and 2 months, and 33.4% took more than 2 months.
Conclusions and clinical relevance
The FAPPCS technique without the use of a guide is a viable salvage procedure for bilateral SIL in cats. Postoperative management and quality of life were considered good by most owners. When performing fluoroscopy-assisted bilateral SIL treatment, we recommend targeting the centre of the body of the sacrum before any attempt to reduce the ilium.
Plain language summary
Sacroiliac luxation is a common injury in cats after trauma, where part of the pelvis becomes unstable. In some cases, both sides of the pelvis are affected, making treatment more complex. This study describes a minimally invasive surgical technique using a single screw placed under C-arm guidance to stabilise both sides of the pelvis at the same time. Six cats with this type of injury were treated using this approach. The results showed that the technique allowed accurate positioning of the implant and good stabilisation of the pelvis. Most cats recovered well, with 5/6 returning to normal function and the majority recovering within 2 months. No major complications were identified during follow-up. This technique may offer advantages compared with traditional open surgery, including less tissue damage and potentially shorter surgical time. However, further studies with a larger number of cases are needed to confirm these results and better assess long-term outcomes.
Introduction
Sacroiliac luxation (SIL) is a traumatic separation of the ilium from the sacrum, with the ilium usually displaced craniodorsally. Approximately 33% of SIL cases in cats are bilateral.1,2
Treatment is conservative or surgical, based on clinical, neurological and imaging findings. 3 Surgery is recommended for severe pain, pelvic canal narrowing greater than 50%, and concurrent orthopaedic or neurological issues (41% of cases).4–7 Conversely, selected cases respond well to medical management.3,5
Several surgical techniques have been described, including open or closed reduction, three-dimensional-printed surgical guide, fluoroscopic-guided reduction and fixation with a trans-iliosacral rod, toggle suture, pin or screw.8–14
Minimally invasive surgery is known to reduce pain, blood loss, procedure time and hospital stay in both humans and cats.15–17 However, most feline studies focus on unilateral SIL.14,17–20 Bilateral luxations are often excluded from minimally invasive reductions owing to the challenge of achieving and maintaining reduction during implant placement. Using one implant for each ilium solves this problem, while a single implant prevents interference between opposing screws and improves placement accuracy.1,10
To our knowledge, no minimally invasive technique for bilateral SIL fixation using a single cannulated screw under C-arm guidance has been described. The objective of this study was to describe a safe and effective minimally invasive surgical technique for bilateral SIL fixation with a single implant and to evaluate its clinical outcome.
Materials and methods
Case selection
This retrospective study included cats with bilateral SIL treated using fluoroscopy-assisted percutaneous cannulated screw placement (FAPPCS). All were consecutive cases treated between July 2021 and February 2023 at Les Cordeliers Hospital, Meaux, France which required surgical treatment. The decision to pursue surgical stabilisation was based on a combination of clinical and radiographic criteria (pain severity, ambulatory status, degree of lameness, neurological findings, degree of iliac displacement, pelvic canal narrowing and/or concomitant pubic, and ischial fracture). The inclusion criteria required immediate postoperative radiographs. Cats with unilateral SIL or bilateral SIL treated non-surgically or with an alternative treatment were excluded.
Ilium displacement percentage and other orthopaedic procedures were not exclusion criteria. Medical records were reviewed for signalment, history, clinical examination, radiographic evaluation, concomitant orthopaedic lesions, surgical records, hospitalisation details, survival to discharge, postoperative complications and follow-up data. Hospitalisation and discharge times were recorded.
Surgical technique
Anaesthetic protocols varied slightly between animals, with opioids (methadone hydrochloride, morphine sulfate or fentanyl citrate) administered during premedication, induction and/or as a continuous rate infusion. Anaesthesia was maintained with isoflurane in oxygen. All received amoxicillin-clavulanic acid (20 mg/kg IV). Preoperative radiographs guided selection of the screw (cannulated, self-drilling, self-tapping, partially threaded titanium, QuickFix; Arthrex) to span both ilial cortices.
Traction was applied to the pelvic limbs and pressure to the cranial ilial wings to achieve partial reduction (Figure 1). Force direction was guided by initial radiographs and confirmed by repeat imaging. Even if not maintained, this step minimised intraoperative manipulation of the pelvis. The patient was transferred to the operating room and placed in sternal recumbency on a positioning cushion, with hindlimbs hanging off the table with gravity and muscle relaxation providing passive caudal traction of the pelvis (Figure 2). Correct patient positioning, with the vertebral column aligned and parallel to the surgical table, was confirmed using two orthogonal fluoroscopic views to ensure the absence of axial rotation or pelvic obliquity. The surgical field was draped with incision film, which could be sutured to the skin to reduce imaging artefacts (Figure 2).
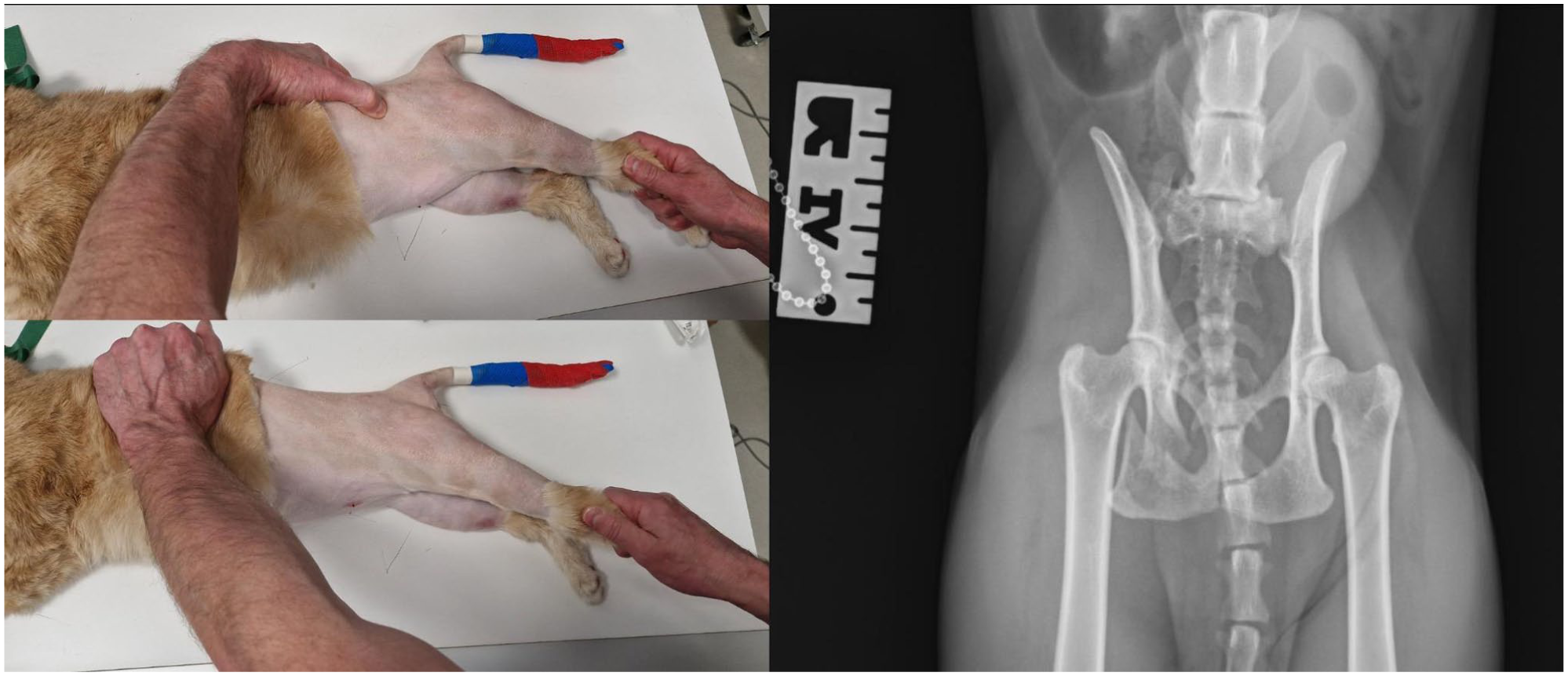
Traction to the pelvic limbs while applying suitable pressure to the cranial ilial wings to approximate partial reduction of the ilia relative to the sacrum

Surgical positioning in sternal recumbency on a positioning cushion allowing the posterior limbs to hang over the edge of the table. The surgical field was aseptically prepared and draped with an incision film
In this description, ‘side A’ refers to the initial side and ‘side B’ to the contralateral, as selected by the surgeon according to clinical preference.
Step 1: A 2 inch (5.1 cm), 14 G hypodermic needle was placed parallel to the table on side A to mark the sacral body’s centre (Figure 3a,b). The surgeon used forceps to avoid radiation exposure. Needle position was guided by fluoroscopic spot-film with a horizontal C-arm beam and inserted percutaneously. The 2 inch, 14 G needle ensured muscle penetration regardless of thickness. Orientation was approximate and refined later.

(a,b) Alignment of the needle parallel to the surgical table to locate the centre of the first sacral vertebra on side A. (c) Pin insertion after needle orientation and position
The key was centring the needle on the sacral body, without attempting to reduce the ilium on side A.
Step 2: The needle was held in place against the ilium facing the sacral body centre (Figure 3c). A 1 mm pin was inserted through the needle, parallel to the floor and perpendicular to the spine, reaching side B of the sacrum (Figure 4).
Step 3: Under orthogonal fluoroscopy, side B was reduced by applying traction to the pelvic limb or by depressing the cranial edge of the ilial wing (Figure 5a). Counter-traction and stabilisation of the pelvis were obtained by maintaining the trunk and contralateral hemipelvis firmly positioned against the surgical table. Once reduction was achieved, the pin was advanced through the ilium in side B to secure reduction (Figure 5b) and its position confirmed before and after crossing soft tissues.
Step 4: The pin was pulled towards side B (now reduced) to release side A, before being pushed back through the previously reduced side A (Figure 5c,d).
Step 5: A #11 scalpel blade was used to enlarge the pin exit through the soft tissues to facilitate subsequent drilling. A cannulated drill bit was guided over the pin to bore a hole through both the ilia and sacrum (Figure 6a). The cannulated screw was advanced from side A through the sacral body to side B (Figure 6b). When the screw advances into joint B, its tip may cause slight distraction. In this case, it was necessary to remove the screw, apply manual pressure with one hand against the ilium, and reinsert it to ensure that it re-engaged in the original hole (Figure 6c).

Fluoroscopic orthogonal views of progressive pin insertion in the centre of the first sacral vertebra across the 14 G needle

(a) The insertion of a 1 mm pin until it reaches side B of the sacrum. (b) Reduction of the ilium in side B into anatomical position by pelvic traction, with the hand folding over the cranial edge of the wing and pin advancement into the side B ilium to fix it; (c) pin pulling towards side B (now reduced) until the tip of the pin is disengaged from the ilium in side A; (d) side A ilium reduction and pin re-engagement through the ilium in side A
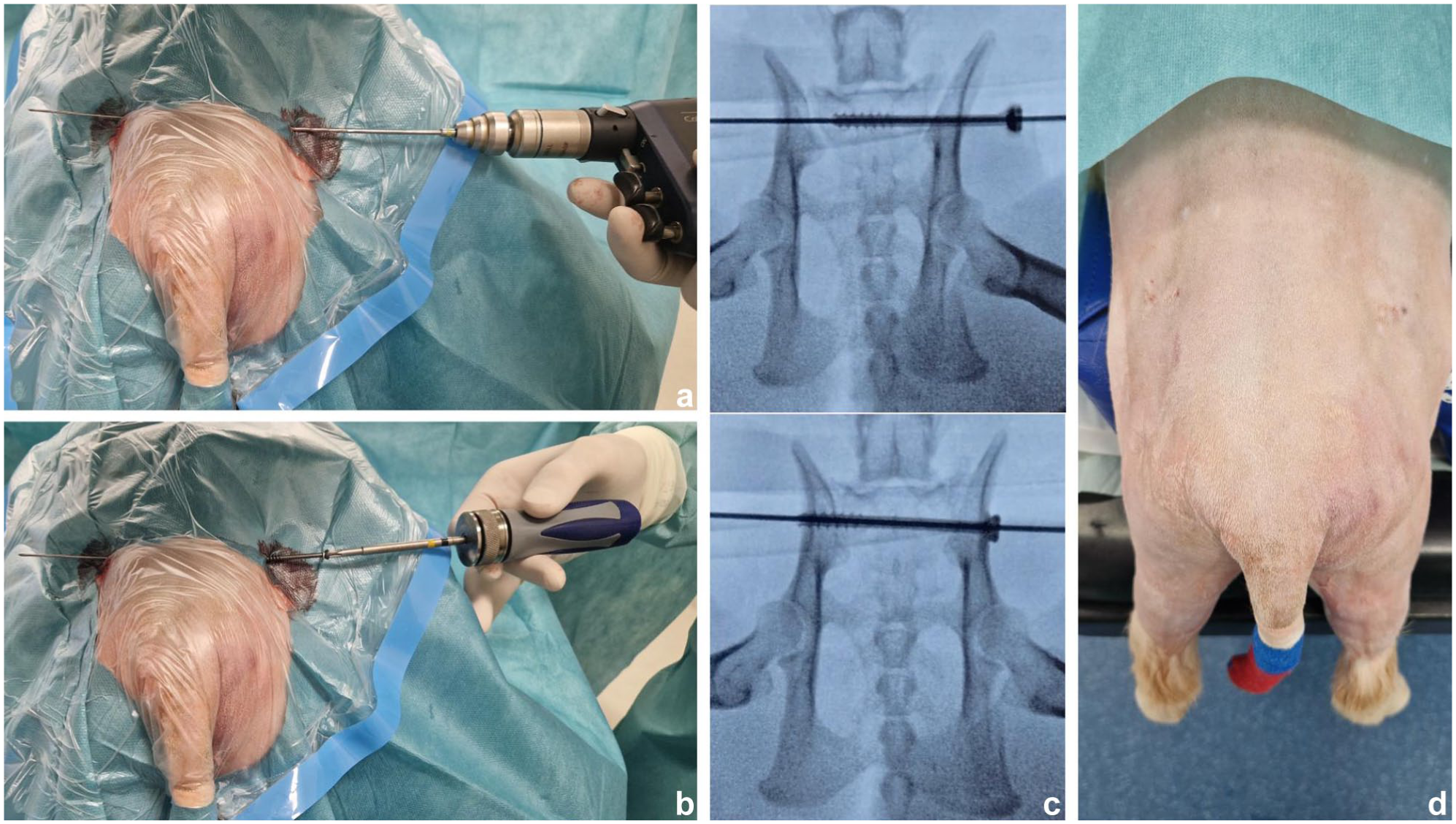
(a) Cannulated drill bit guided over the pin to bore a hole through both the ilia and the sacrum. (b,c) Cannulated screw advancement through the side A iliac wing, the sacral body and the side B iliac wing. (d) Aspect of the patient at the end of the surgery
The final position was verified fluoroscopically before pin removal and skin closure (Figure 6d). Detailed descriptions of the surgical technique are provided in Video 1 in the supplementary material.
Postoperative care
Postoperative analgesia was individualised and guided by regular pain assessment, with opioid administration adjusted according to clinical response. Cats were discharged once adequate pain control was achieved without ongoing opioid requirements and satisfactory ambulation was observed. Strict confinement was prescribed for 8 weeks, followed by gradual activity. Radiographic follow-up examinations were advised at 1 and 2 months postoperatively.
Data collection and analysis
Demographic data (species, breed, age, sex and body weight), concomitant lesions and diagnostic results were recorded.
Outcome measures collected on radiographs taken before and directly after surgery included screw purchase ratio, degree of iliac displacement relative to the sacrum (ID), sacroiliac joint (SIJ) reduction, pelvic canal diameter ratio (PCD) and angle of deviation (AoD) (Figure 7).

(a) Preoperative radiographs of case 6 with bilateral sacroiliac luxation: ventrodorsal and lateral views. (b) Immediate postoperative radiographs (ventrodorsal and lateral views) demonstrating sacral lag screw placement in case 6, with annotated measurements: AB = sacral body width; CD = hemipelvis width corresponding to the smaller value, measured from the medial edge of the acetabulum to the central axis; DE = hemipelvis width corresponding to the larger value, measured from the medial edge of the acetabulum to the central axis; PCD = the ratio between pelvic width at cranial aspect of acetabuli (AB) and width of caudal aspect of sacral joint surfaces (CD + DE); i = articular surface of the ilium in contact with the sacrum); j = total articular surface of the sacrum; k = length of screw; l = width ilia wings and sacrum
ID was measured as the ratio of SIJ incongruence to total sacral articular surface length, expressed as a percentage, as described by Bird and de Vicente. 3
PCD was measured as described by Averill et al 21 and Leasure et al, 22 with a ratio greater than 1.1 considered normal.
Screw purchase was assessed using the ratio of screw depth (SD) to the combined width of the sacral body and both ilia cortices, with a ratio greater than 1 considered optimal. On the same radiograph, reduction of the SIJ was evaluated based on the relative difference between the articular surfaces of the ilium and sacrum.9,18 A postoperative SIJ reduction of 100% was considered optimal. The AoD was defined as the angle between a line perpendicular to the sagittal plane and the direction of the screw on ventrodorsal radiographs. Angles were considered positive or negative when the direction of the screw was cranial or caudal, respectively.9,12
Short-, medium- and long-term assessment of limb function
Types and duration of complications were recorded clinically and radiographically. Postoperative complications included events during hospitalisation and after discharge. Complications were classified as short (⩽6 days), medium (7–60 days) or long term (>60 days).
Owners were contacted between April 2023 and June 2023 using a questionnaire that was adapted from Bird and de Vicente 3 and Yap et al, 23 neither of which have been validated (S1 in the supplementary material). Owners were asked to assess the cats’ condition before and after surgery based on lifestyle modifications, daily functional abilities, urinary and faecal continence, jumping capacity, need for additional medication, presence of concurrent orthopaedic or non-orthopaedic conditions, and the time required to regain normal function. An average disability score (ADS) before and after the operation was established using the questionnaire, corresponding to the average of the scores assigned to all activities.
In addition, owners subjectively defined their animals’ recovery of locomotor abilities as follows: (1) excellent function with full locomotor ability, free of pain, lameness or the need for analgesic treatment; (2) moderate function with an activity similar to pre-trauma but with occasional lameness, pain or the need for analgesic treatment; or (3) poor function with no ability to recover expected activity.
Statistical analysis
Descriptive statistics (mean, median, SD, minimum and maximum) were calculated for key measures. One-sample Wilcoxon signed-rank tests were performed to compare each series against a predefined reference: 100% for SIJ reduction, 1.10 for PCD ratios, 100 for screw placement and 0 mm for AoD. Paired Wilcoxon signed-rank tests were used to evaluate within-subject differences between left and right SIJ reduction (immediate), between immediate and control follow-up SIJ reduction (each side), between preoperative and postoperative PCD ratios, between postoperative and control follow-up PCD ratios, and between immediate and control follow-up AoD engagement. All tests were two-sided, and statistical significance was set at P <0.05. Analyses were conducted in Python 3.11 using the SciPy library’s wilcoxon function.
Results
Demographics
Six cats were treated via FAPPCS for bilateral SIL between July 2021 and February 2023. The cohort included five (83.3%) crossbreeds and one Siamese. Mean age was 2.4 years (range 5 months to 5 years) and mean weight was 4.9 kg (range 4.1–7.15). There were three castrated males, two intact males and one spayed female (Table 1). All cases were traumatic in origin.
Radiographic parameters assessed preoperatively (n = 6), postoperatively (n = 6) and at 4-week follow-up (n = 5) after fluoroscopy-assisted closed reduction and trans-iliosacral screw stabilisation of sacroiliac luxations

AoD = angle of deviation; ID = degree of iliac displacement relative to the sacrum; PCD = pelvic canal diameter; SIJ = sacroiliac joint
Preoperative evaluation followed standard trauma assessment protocols, including complete physical, orthopaedic and neurological examinations in all cats. Additional diagnostic investigations (blood tests, thoracic radiographs and/or point-of-care ultrasound) were performed as clinically indicated, based on patient stability and suspected concurrent injuries.
At presentation, severe acute pain was present in all cats. One cat was non-ambulatory with tetraparesis, while five cats were ambulatory with marked lameness.
Neurological examination identified proprioceptive abnormalities in two (33%) cats at the time of admission, including loss of deep pain sensation in the tail in one (17%) case. In three (50%) cats, proprioceptive assessment could not be reliably performed because of limited manipulation secondary to pain.
Concurrent traumatic lesions were frequently identified, with three (50%) cats presenting with cutaneous abrasions (S2 in the supplementary material).
Results of imaging studies
Ventrodorsal and lateral radiographs were acquired under general anaesthesia pre- and postoperatively.
Preoperative diagnosis and measurements
Concomitant orthopaedic lesions were present in four cats and included pubic fractures in three (50%) cats and an iliac fracture in one (17%) cat. In addition, case 2 presented suspected acute spinal cord injury, a cleft palate and a mandibular fracture. Two cats (33%) presented with no additional orthopaedic injuries (S2 in the supplementary material).
Preoperative PCD was greater than 1.1 in all cases, with a mean score of 1.46 ± 0.22. Four cases were identified with preoperative ID less than 50% on both sides. All four had concomitant pubic and/or ischial fractures. Mean preoperative displacement was 59% ± 32% on the right side and 48% ± 26% on the left side (Table 1).
Postoperative measurements
Case 4 presented with a transverse right ilium fracture, which was treated via osteosynthesis. Plate fixation was performed first, with the patient positioned in lateral recumbency, allowing anatomical reduction and stabilisation of the ilium before sacroiliac fixation. The patient was then repositioned in sternal recumbency, as describe in the ‘Materials and methods’ section, to perform the fluoroscopy-assisted sacroiliac screw placement. The plate was applied dorsally on the iliac body, which avoided interference with the trans-iliosacral screw trajectory. No adjustment of plate positioning was required, and no implant conflict was encountered intraoperatively. No penetration of the vertebral canal was observed during the various fluoroscopic checks or on postoperative radiographs in any patient. Screw diameters were in the range of 3.0–4.5 mm and lengths 40–44 mm, according to sacral length (S2 in the supplementary material). All screws exceeded 100% purchase, with a mean of 116% ± 8.9% (range 110–133) (P = 0.031).
Mean postoperative PCD was 1.40 ± 0.12. In two cats (cases 3 and 6), postoperative values returned to preoperative levels but remained greater than 1.1. Although postoperative PCD was on average 5.8% lower than preoperative values, this difference was not statistically significant (P = 0.345).
Considering each joint independently, anatomical reduction of SIL was in the range of 93–100% for the left side, with a mean value of 98.8% ± 2.9% (P = 0.317). Right SIJ reduction was in the range of 84–100% (mean 96.2% ± 6.6%; P = 0.180); 6/7 cases exceeded 90% (Table 1). Immediate postoperative reduction was similar on both sides (P = 0.414), with no systematic difference in alignment. No association could be demonstrated between the choice of side A or side B and the percentage of joint reduction (Mann–Whitney U-test for unpaired comparison, P = 0.548).
The AoD ranged from –2.59° to 1.17° (mean absolute 1.30° ± 0.91°; P = 0.31).
Short- and medium-term follow-up and complications
Time from admission to surgery and from surgery to discharge both averaged 1.33 days (ranges of 0–5 and 1–3, respectively). The surgeon’s subjective criteria, such as clinical instability, acute pain, urinary incontinence and neurological lesions, were used to determine the duration of hospitalisation.
All patients survived the surgery, and follow-up is recorded S3 in the supplementary material.
Five cases were monitored during the short-term period, via telephone or clinical examination, without any complications reported.
During the medium-term follow-up, case 5 showed lameness at day 21 postoperatively, which resolved spontaneously. All cats were reassessed clinically or by phone 30–60 days postoperatively. Follow-up radiographs were not performed for case 2. Five cats were presented for first radiographic follow-up at a median of 33 days (range 28–40) postoperatively. No implant loosening was noted. No statistical difference was found between immediate and control follow-up values (paired Wilcoxon test, P value) for PCD (mean 1.36 ± 0.09; P = 0.0625), SI reduction (left: 100%, right: 95.6% ± 6.39%; P = 0.180) or AoD (mean 1.03° ± 0.83°; P = 0.0625). Postoperative control differences were minimal.
One cat had a second medium-term radiographic follow-up at 71 days postoperatively. No implant loosening or change in PCD, SI reduction or AoD was observed between the first and last radiographic follow-ups.
Mid- and long-term follow-up and questionnaire
All cats underwent mid- and long-term follow-up via owner interviews at a mean of 342 days (range 141–415) postoperatively. Pre-trauma ADS was 0 for all cats. None required anti-inflammatory or analgesic treatment at mid- and long-term follow-ups. No FAPPCS-related complications were noted. Urinary and faecal continence was preserved in all cats. The mean ADS was 0.50 ± 0.52 (P = 0.068) (S4 in the supplementary material). Case 4, the one presenting a right iliac fracture, had a mean disability score of 1.17. The owner described extremely rare phases of pain (1 day every 2–3 months) with incapacity to run or climb. Outside of these episodes, the patient displayed normal ability without lameness or pain. All cats recovered fully: one (16.6%) within 1 month, three (50%) within 1–2 months and two (33.4%) after 2 months.
Owner evaluations showed excellent function in five (83.3%) cats and moderate function in one (16.6%) cat (case 4). No cat was rated as having poor recovery.
Discussion
FAPPCS for bilateral SIL was feasible, safe, and effective; 5/6 cats recovered excellently.
Although fluoroscopic repair is common for unilateral SIL, bilateral cases often need open surgery because of landmark limitations and ilial mobility.11,13,14,17,19,22,24–26 In a cadaveric study, Han et al 27 identified new surgical landmarks for minimally invasive repair. To address this, minimally invasive techniques typically treat each joint separately. Moreover, to enable screw penetration and reduce opposing forces, smaller diameter implants (1.5–2.0 mm cortical screws) were used compared with previous recommendations.11,13,22,26
To our knowledge, no previous technique combines a single implant with a minimally invasive approach for bilateral SIL. With FAPPCS, immediate reduction reached 96.2% (right) and 98.8% (left), exceeding previously reported values (range 87.7–97.5%).9,12,22,25,27,28 This accuracy likely reflects the advantages of fluoroscopic guidance and simultaneous percutaneous manipulation of both ilia, which overcomes pelvic rigidity. Our technique allows reduction to be maintained during pin insertion. In addition, immediate pin fixation also reduces positional errors by maintaining reduction during cannulated screw placement.
The size of the implants used deserves discussion. A recent publication by Jourdain et al 29 demonstrated the efficacy of 2.4 mm partially threaded, headless compression screws for the treatment of unilateral SIL. AOFoundation guidelines recommend that the screw should occupy 40% of the sacral diameter. According to Burger et al, 30 and with an average sacral height of 5.9 mm in cats, 2.4 mm matches the AO’s 40% rule. 2 However, maximum heights of 9 mm and 7.1 mm were reported in the studies. For such individuals, a 3.5 mm screw would meet AO criteria. Bearing in mind that undersized screws increase the risk of loosening, whereas improperly placed oversized screws may increase the risk of iatrogenic injury, implant selection is critical for appropriate surgical management. However, implant selection should not rely solely on body weight, as this may lead to over- or underestimation in animals with atypical body condition scores (eg, obese or underweight patients). Instead, individualised implant selection based on preoperative assessment of sacroiliac articular morphology and sacral dimensions, in accordance with minimum AO recommendations, is advised to ensure adequate bone purchase while minimising associated risks. In the present study, all screws were accurately placed without canal or foraminal breach, regardless of patient size. These observations were supported by the mean AoD (1.30° ± 0.91°), which was lower than values previously reported by Pratesi et al 9 (+1.6°) and Froidefond et al 12 (+3.4°), indicating good to excellent craniocaudal screw orientation within the sacral corridor. Thus, a well-positioned implant of larger diameter may provide better resistance to pull-out, shear and bending forces, which could justify the use of 3.5 mm screws.31,32
In dogs, beyond the bending and shearing forces observed, ground reaction forces generate upward and rotational loads at the SIJ.33,34 Although not demonstrated in cats, SI rotation is likely similar. Cats show higher peak vertical and propulsion forces, suggesting similar or greater mechanical and rotational loads.35,36 This is further supported by comparative anatomical studies in wild cats. 37 Small cats show wider inter-iliac angles and lower joint congruence, which may enhance SIJ mobility and agility during movement. These findings suggest a shared SIJ rotational biomechanical pattern in cats and dogs. Therefore, controlling rotational forces is essential in SIJ stabilisation.
Larger implant diameter alone may not counteract rotation.26,34 In such cases, the addition of a second positional screw has been proposed to enhance construct stability in unilateral or bilateral (but individually addressed) cases.27,38 However, load-bearing forces may differ in bilateral cases, possibly explaining the higher rate of loosening observed compared with unilateral cases (up to 26%). 38 Given these considerations, the rotational forces exerted on a single trans-iliosacral implant warrant further investigation to clarify their mechanical impact.
Clinical outcomes were good to excellent in 83.3% of cats; 50% recovered within 2 months and 16.6% within 1 month. SI reduction was not correlated with recovery time. Although suspected to be beneficial, the impact of surgical stabilisation on recovery time, pain or pelvic width remains unproven. The absence of a control group limits comparison with open surgery outcomes. We identified several limitations in our study, mainly due to its retrospective nature, which affected data collection. There was no standardised radiographic technique, possibly affecting measurements. Postoperative radiographic follow-up was dependent on owner compliance. As most cats showed a favourable clinical evolution at approximately 1 month postoperatively, owners generally declined additional imaging beyond this time point. The use of owner questionnaires is highly subjective. Owners’ long-term assessment of patients’ conditions can vary according to the length of time between the interview and the trauma. A large number of cases would therefore be required to obtain a meaningful statistical comparison.
In addition, no formal assessment of a learning curve could be performed for surgical time, AoD or percentage of reduction because of the limited sample size and retrospective nature of the study. However, from an operator perspective, only a small number of cases appeared necessary to become familiar with the technique, which was subsequently perceived as reproducible and associated with shorter surgical times compared with open approaches. This observation remains subjective and requires confirmation in larger prospective studies.
Conclusions
This study supports the feasibility and clinical effectiveness of fluoroscopy-guided closed reduction using a single trans-iliosacral screw for bilateral SIL, without a guide. To the authors’ knowledge, this is the first report of a minimally invasive technique combining bilateral treatment with a single implant.
A broader clinical evaluation, preferably with a prospective study, may be required to establish the learning curve, and compare functional restoration time and complication rates with those of an open approach, or to compare implants.
Supplemental Material
Video 1: Step-by-step surgical technique for fluoroscopy-assisted single transiliac screw placement.
S1: Owner questionnaire used for long-term functional outcome assessment after fluoroscopy-assisted single transiliac screw stabilisation.
S2: Patient demographics, clinical presentation, concomitant injuries, additional orthopaedic procedures and implant characteristics.
S3: Summary of clinical and radiographic follow-up outcomes after fluoroscopy-guided closed reduction with transiliac screw fixation.
S4: Summary of owner-reported functional outcome and average disability score assessment.
Footnotes
Supplementary material
The following files are available as supplementary material:
Video 1: Step-by-step surgical technique for fluoroscopy-assisted single transiliac screw placement.
S1: Owner questionnaire used for long-term functional outcome assessment after fluoroscopy-assisted single transiliac screw stabilisation.
S2: Patient demographics, clinical presentation, concomitant injuries, additional orthopaedic procedures and implant characteristics.
S3: Summary of clinical and radiographic follow-up outcomes after fluoroscopy-guided closed reduction with transiliac screw fixation.
S4: Summary of owner-reported functional outcome and average disability score assessment.
Conflict of interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Stéphane Bureau is a paid consultant for Arthrex.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all the animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.