
Abstract
Objectives
Serum amyloid A (SAA), the major acute-phase protein in cats, has potential, as in humans, to aid in the diagnosis and treatment of bacterial infections. This study compared SAA concentrations in cats with acute pyelonephritis (APN) with stable chronic kidney disease (CKD) and healthy cats. In cats with APN, SAA concentrations were monitored during antibiotic treatment to assess whether they correlated with clinical scores.
Methods
A multicenter study recruited client-owned cats with APN (n = 9), with stable CKD (n = 10) or healthy cats (n = 10). Cats with APN were monitored for 21 days during antibiotic therapy to assess SAA concentrations along with clinical scores.
Results
The majority of cats with APN were older (>10 years) and spayed females (8/10), with 5/9 having pre-existing CKD. Median SAA concentrations were significantly higher in cats with APN (235.3 mg/l, range 9.1–810) than in healthy cats (1.85 mg/l, range 1–2.7; P = 0.0008) and cats with stable CKD (1.45 mg/l, range 0.1–8.9; P = 0.0002). Cats with APN reached peak SAA concentrations (412 mg/l, range 18.6–810) within 48 h of presentation. In addition, with treatment and clinical recovery, median SAA concentrations returned to normal (3.1 mg/l, range 1–7.2) within 14 days. SAA concentrations were moderately correlated with clinical scores (rs = 0.650).
Conclusions and relevance
The results of this study offer additional insights into the potential benefits and limitations of monitoring SAA concentrations in cats with APN. Cats with APN experience increased SAA concentrations, supporting SAA as a diagnostic tool for identifying affected cats. Serial SAA monitoring may help assess clinical recovery or determine treatment failure.
Keywords
Introduction
Feline acute pyelonephritis (APN) is an antibiotic-responsive form of acute kidney injury (AKI).1–4 Diagnosing APN in cats remains challenging, in part, because of the often vague clinical signs as well as limitations associated with routine diagnostic tests.5,6 Subclinical bacteriuria and bacterial culture-negative APN in cats complicates clinical decision-making in cases with pre-existing chronic kidney disease (CKD).5,6 Furthermore, the lack of veterinary-specific, evidence-based guidelines likely contributes to antibiotic therapy lasting weeks, compared with days in humans with APN.4,7–9 In humans, biomarkers, including acute-phase proteins, further support the diagnosis and monitoring of bacterial inflammatory conditions, including APN.3,10–12 Serum amyloid A (SAA), the major acute-phase protein in cats, has shown potential for similar applications.13–18 Recent studies have found higher SAA concentrations in cats with APN than in those with other urinary tract diseases. 19 However, no studies have compared SAA concentrations in cats with stable CKD to those with APN or tracked SAA concentrations during antibiotic treatment.
This study aimed to evaluate the potential of SAA as a diagnostic and monitoring tool in cats with APN. The specific objectives were to establish whether SAA concentrations (1) were significantly higher in cats with APN than in healthy cats and cats with stable CKD, (2) decreased during antibiotic therapy in cats with APN and (3) correlated with clinical signs. We hypothesized that SAA concentrations would be higher in cats with APN, decline with antibiotic therapy and correlate with clinical scores.
Materials and methods
Patient selection
Cats of any age, sex or breed with APN, stable CKD or who were healthy were evaluated for inclusion. The cats were client-owned and presented to the University of Wisconsin Veterinary Care (UWVC) and Purdue University Veterinary Hospital. All study protocols were reviewed, approved and conducted in accordance with the University of Wisconsin’s Animal Care and Use Committee and Purdue University’s Veterinary Clinical Studies Committee. Written informed consent was obtained from all cat owners before enrolment.
Healthy cats were recruited from the UWVC primary care patient population presenting for wellness evaluations or from cats belonging to UWVC employees, students or house officers. Cats were eligible if they showed no signs of acute illness or pre-existing chronic diseases, serum creatinine (Cr) of 1.6 mg/dl or below, urine specific gravity of 1.035 or above, and a negative bacterial urine culture. Cats with stable CKD were eligible if they had a previous diagnosis of CKD (International Renal Interest Society [IRIS] stages 2–4), 20 no change in clinical signs, a stable Cr (<0.3 mg/dl increase from last documented Cr) and a negative urine bacterial culture. The clinical diagnosis of APN was based on consistent clinical signs, physical examination, imaging, and clinicopathologic and microbiologic assessments.5,6 All criteria used to support the clinical diagnosis of APN were required, including the following: (1) new azotemia defined as Cr ⩾1.6 mg/dl or an increase of ⩾0.3 mg/dl from baseline Cr in cats with CKD,21,22 without another identifiable cause; (2) consistent clinical signs (at least two): lethargy, hyporexia, anorexia, polydipsia, polyuria, vomiting or abdominal pain; (3) other laboratory findings (at least one): isosthenuria, cylindruria, glucosuria in the absence of hyperglycemia, peripheral neutrophilia with or without left shift; (4) an abdominal ultrasound consistent with APN;23,24 and (5) confirmed bacteriuria via urine sample collected by cystocentesis, based on urine sediment evaluation and/or a positive urine culture, defined by bacterial species isolated in 103 colony forming units (CFU)/ml or greater. Study exclusion criteria included cats with concurrent active or newly diagnosed diseases other than CKD, and cats for whom local veterinary records were unavailable for review to document their history and treatments before presentation.
Study design
Healthy cats and cats with stable CKD were evaluated once at enrolment. All cat evaluations included age, breed, sex, neuter status, relevant medical history, current drug therapies, physical examination findings, complete blood count (CBC), biochemistry profile with electrolytes, urinalysis, urine culture, protein:Cr ratio (if indicated), blood pressure and SAA concentrations. Cats with APN underwent comprehensive evaluations, including an abdominal ultrasound. All ultrasound images were reviewed and interpreted by a single board-certified radiologist (KW). These cats were monitored over 21 days, with clinical evaluations, including physical examination, blood work (renal panel and CBC), urine culture and SAA concentration on day 0. SAA concentrations were also measured on days 1 and 2. Serial SAA assessments during hospitalization (days 0, 1 and 2) allowed monitoring of peak SAA concentrations within 24–48 h. 2 Additional clinical evaluations, including physical examination, blood work (renal panel and CBC), SAA concentrations and urine culture, were performed on days 7, 14 and 21. Subjective clinical scoring, based on the owner’s history and physical examination, was adapted from a validated urinary tract infection (UTI) symptom assessment questionnaire used in humans (Table 1). 25 All cats clinically diagnosed with APN were treated at the attending veterinarian’s discretion.
Clinical scoring used in cats with acute pyelonephritis to assess each cat at presentation and during subsequent serial visits, incorporating owner-provided information and physical examination findings to facilitate an objective assessment of each cat’s clinical status

Sample collection and analysis
Healthy cats and cats with stable CKD had 3 ml of venous blood drawn for routine blood work and SAA concentrations at a single visit. For the cats with APN, 0.5 ml of venous blood was collected during hospitalization (days 0, 1 and 2) for SAA concentrations. Additional blood samples (2–3 ml) were collected on days 7, 14 and 21 for recheck blood work and SAA concentrations. In all cats, urine (approximately 5 ml) was collected via cystocentesis at enrolment for urinalysis and urine culture. In cats with APN, recheck urine cultures were performed on days 7, 14 and 21. For SAA analysis, serum was separated from clotted blood, aliquoted, frozen (–20°C) and shipped on dry ice within the next business day to the University of Miami, Acute Phase Protein Laboratory for analysis using an immunoturbidimetric assay validated in cats. 26 High- and low-quality control samples were run before patient samples, and the instrument was recalibrated if quality control results were out of range. The SAA serum samples for each cat were submitted as clinical samples, with no information provided to the laboratory regarding the study group or treatments.
Statistical analysis
All continuous variables are reported as medians and ranges. SAA concentrations were compared using the Kruskal–Wallis test and Dunn’s test for multiple comparisons. The Spearman rank correlation coefficient (rs) was used to assess the relationships between SAA concentrations and clinical scores, and neutrophil counts and clinical scores. 27 Statistical significance was set at a P value <0.05.
Results
Demographic data, clinical scores and clinicopathologic values of the enrolled cats are summarized in Table 2.
Summary and comparisons of feline population demographics and clinicopathologic values between the three groups of cats – healthy cats, cats with stable chronic kidney disease (CKD) and cats with acute pyelonephritis (APN) – who were recruited to assess serum amyloid A concentrations
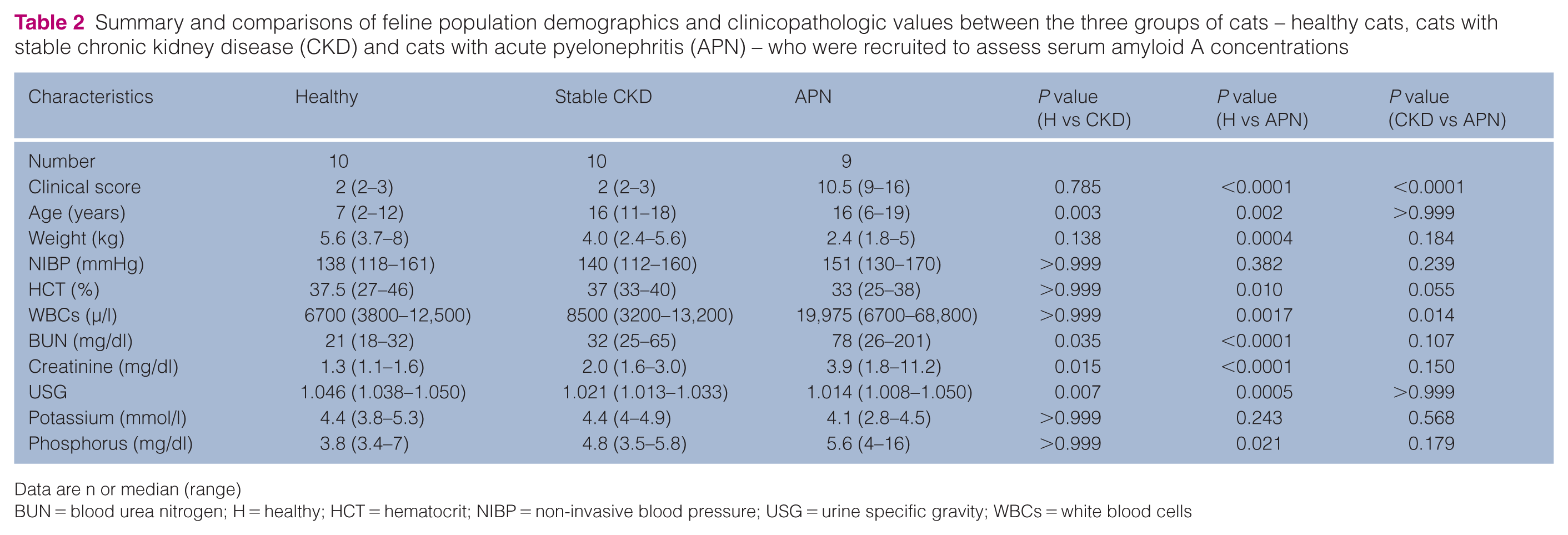
Data are n or median (range)
BUN = blood urea nitrogen; H = healthy; HCT = hematocrit; NIBP = non-invasive blood pressure; USG = urine specific gravity; WBCs = white blood cells
Healthy cats
Of the 14 healthy cats evaluated, 10 were enrolled; four were excluded based on their screening diagnostics. Breeds included domestic shorthair (DSH; n = 7), Persian (n = 1), domestic longhair (n = 1) and Ragdoll (n = 1), and consisted of four spayed females and six castrated males.
Cats with stable CKD
Of the 14 cats with CKD evaluated, 10 were enrolled; four were excluded after screening. Breeds included DSH (n = 9) and domestic medium hair (DMH; n = 1), and consisted of four spayed females and six castrated males. Cats were categorized as IRIS stages 2 (n = 9) and 3 (n = 1).
Cats with APN
Of the 11 cats with APN evaluated, nine were enrolled; two were excluded because of unavailable serum. A total of 10 APN episodes involving nine cats were included, with one cat experiencing separate APN episodes 1 year apart. Breeds included DSH (n = 7), DMH (n = 1) and Abyssinian (n = 1), and consisted of eight spayed females and one castrated male. Five cats had a history of CKD (IRIS stages 2 [n = 1] and 3 [n = 4]). Stable comorbidities included hyperthyroidism (n = 3) and chronic enteropathies (n = 2).
The presenting complaints of the cats with APN included lethargy (n = 9), anorexia (n = 9), vomiting (n = 4), weight loss (n = 3) and inappropriate urination (n = 2). The median duration of illness before presentation was 6 days (range 1–14). Antibiotic therapy (cefovecin [n = 1], amoxicillin-clavulanic acid [n = ]) was initiated by the primary veterinarian in two cats. At presentation, all cats were dehydrated (approximately 5–10%), two cats were febrile (103.3°F [39.6°C], 105.5°F [40.8°C]) and five cats had abdominal pain (non-specific [n = 4]; perirenal [n = 1]). Table 3 summarizes the upper urinary tract ultrasound findings in the cats with APN. One cat had a subcapsular effusion of the left kidney, cytologically consistent with marked septic suppurative inflammation and extensive necrosis.
Summary of the upper urinary tract measurements and ultrasonographic findings at the time of diagnosis of acute bacterial pyelonephritis in cats (n = 9)
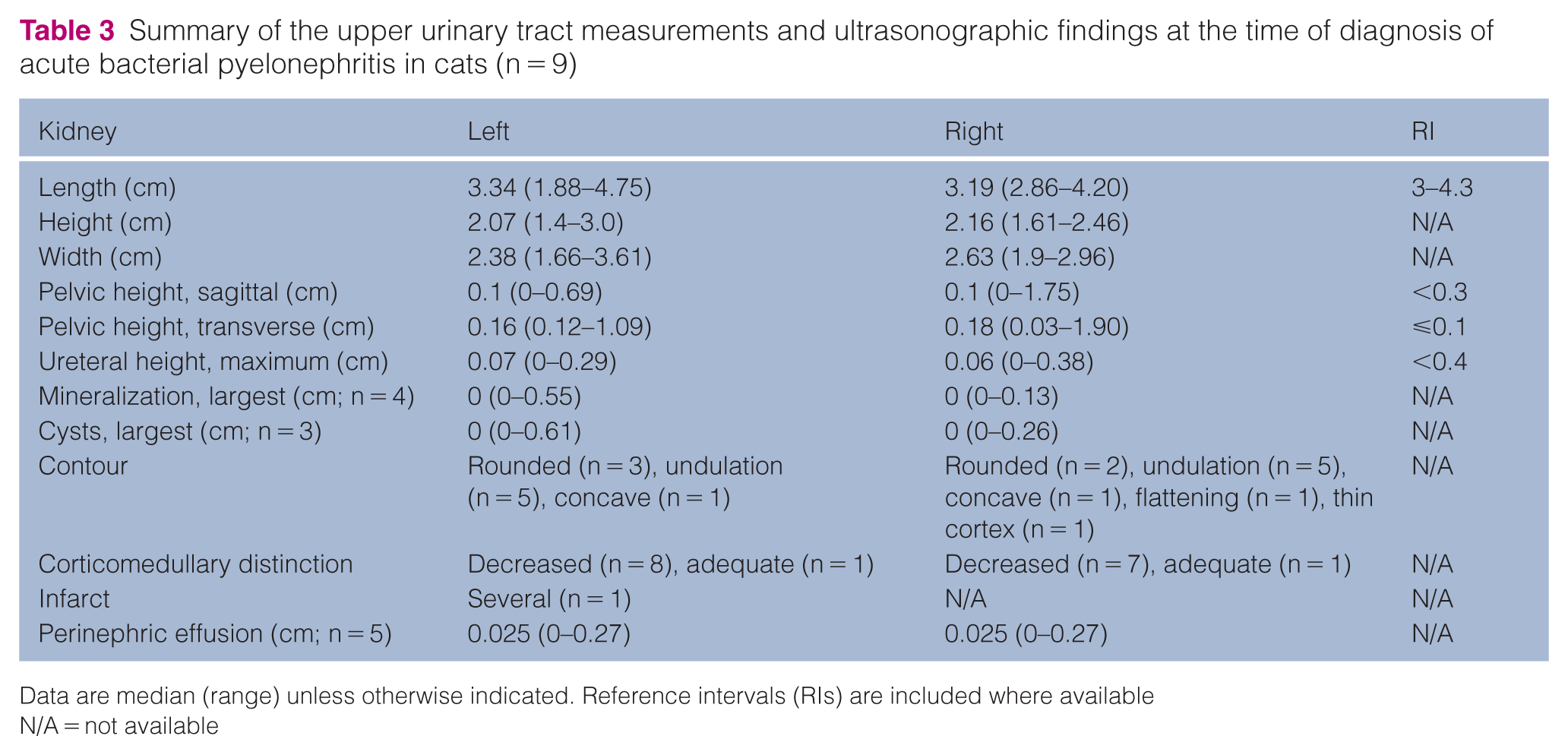
Data are median (range) unless otherwise indicated. Reference intervals (RIs) are included where available
N/A = not available
Two cats with bacteriuria had negative urine cultures. Both these cats had a history of CKD and were clinically diagnosed with APN based on clinical signs, progressive azotemia and a diagnostic work-up to exclude other causes. One of the culture-negative cats received cefovecin 24 h before presentation. Among the 8/10 occurrences of APN with positive urine cultures, bacterial isolates included Escherichia coli (>100,000 CFU/ml, n = 5), E coli (1000 CFU/ml, n = 1), Enterococcus faecalis (>100,000 CFU/ml, n = 1) and Staphylococcus felis (>100,000 CFU/ml, n = 1).
Cats were hospitalized for a median duration of 4.5 days (range 3–6) for supportive care, fluid therapy and initial antibiotic therapy. In eight cases, antibiotic treatment was adjusted to target specific pathogens based on urine bacterial culture and antibiotic susceptibility testing. During hospitalization and outpatient care, seven occurrences of APN were treated with enrofloxacin (median 5 mg/kg IV q24h, range 4.4–5.1) for a median of 4 days (range 2–6), followed by marbofloxacin (median 5 mg/kg PO q24h, range 3.1–5.6) for a median of 30 days (range 19–30). Marbofloxacin was used as pathogen-directed therapy in 6/7 cases. For the remaining three cases, one cat was initially treated with ampicillin-sulbactam (30 mg/kg IV q8h for 3 days) followed by pathogen-directed therapy with pradofloxacin (5 mg/kg PO q24h for 42 days). Another cat was initially treated with enrofloxacin (5.2 mg/kg IV q24h for 4 days), followed by pathogen-directed therapy with doxycycline (4.9 mg/kg PO q12h for 29 days). In the final case, treatment consisted of enrofloxacin (5 mg/kg IV q24h for 6 days) and ampicillin-sulbactam (32 mg/kg IV q12h for 2 days), followed by amoxicillin-clavulanic acid (15 mg/kg PO q12h for 6 days).
During antibiotic treatment, Cr (Figure 1) and neutrophil counts (Figure 2) decreased and then stabilized without a significant change; however, clinical scores decreased significantly (Figure 3). Bacteriuria resolved by day 7 in 9/10 occurrences of APN. One cat remained bacteriuric after a lapse in antibiotic treatment while boarded, with recurrence of clinical signs on day 14 and an increase in SAA concentrations (501 mg/l) after normalization on day 7. This cat had progressive bacteriuria due to persistent E faecalis (>100,000 CFU/ml) and isolation of Staphylococcus hominis (>100,000 CFU/ml). Antibiotics were restarted, and SAA concentrations reduced to 7.8 mg/l by day 21. Interestingly, in another cat, when the owner mistakenly discontinued antibiotics, not only did the Cr increase, but SAA concentrations also rose from 7.1 mg/l (day 14) to 32.9 mg/l (day 21). A third cat experienced an increase in SAA (51.4 mg/l, Cr 3.3 mg/dl) on day 21, after having normalized on day 14 (2.6 mg/l, Cr 4 mg/dl). In 2/3 of these cats with a complicated course and clinical decline, the owners elected euthanasia within 1 month of the study completion.

Serum creatinine concentrations vs time (days) in cats with acute pyelonephritis. There was no significant decrease in creatinine concentrations between days 0 (study enrolment), 1 (P >0.999), 2 (P >0.999), 7 (P >0.999), 14 (P >0.999) and 21 (P >0.999) during antibiotic treatment. Day 0 represents the time of clinical presentation/diagnosis; days 1 and 2 represent consecutive days after diagnosis and are the first 48 h of hospitalization; days 7, 14 and 21 represent consecutive days after diagnosis and are associated with outpatient treatment

Neutrophil counts vs time (days) in cats with acute pyelonephritis. There was no significant difference in neutrophil counts between days 0 (study enrolment), 7 (P >0.999), 14 (P = 0.133) and 21 (P = 0.051) during antibiotic treatment. Day 0 represents the time of clinical presentation/diagnosis; days 7, 14 and 21 represent consecutive days after diagnosis and are associated with outpatient treatment
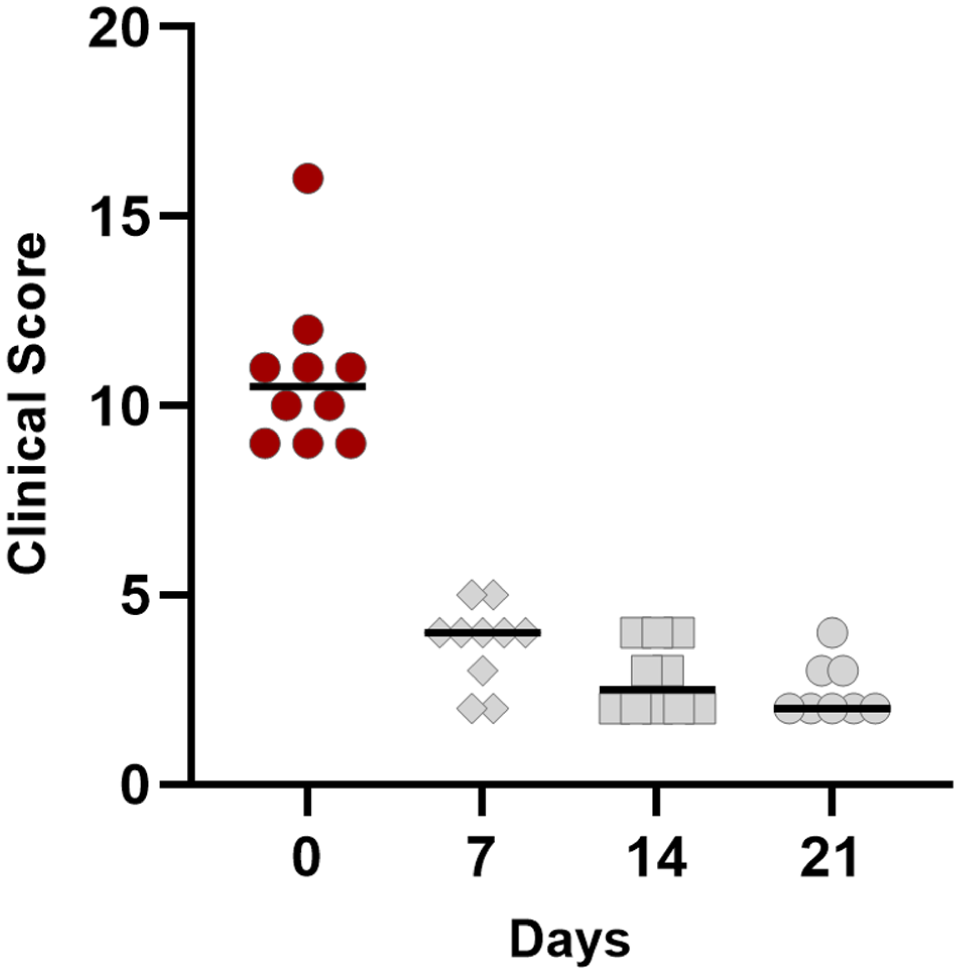
Clinical scores vs time (days) in cats with acute pyelonephritis. During antibiotic treatment, there was a significant decrease in clinical scores from day 0 (study enrolment) to days 7 (P = 0.021), 14 (P = 0.0001) and 21 (P <0.0001). There was no significant decrease in clinical scores between days 7 and 14 (P >0.999), 7 and 21 (P = 0.536), and 14 and 21 (P >0.999). Day 0 represents the time of clinical presentation/diagnosis; days 7, 14 and 21 represent consecutive days after diagnosis and are associated with outpatient treatment
SAA concentrations
Figure 4 compares SAA concentrations among the healthy cats, cats with stable CKD and cats with APN. There was no significant difference in SAA concentrations between the healthy cats (median 1.85 mg/l, range 1–2.7) and cats with stable CKD (median 1.45 mg/l, range 0.1–8.9; P >0.999). Cats with APN had significantly higher SAA concentrations (median 235.3 mg/l, range 9.1–810) compared with both healthy cats (P = 0.0008) and cats with stable CKD (P = 0.0002). In cats with APN, the median peak SAA concentration was 412 mg/l (range 18.6–810), occurring at a median of 2 days (range 0–7) after presentation. Peak SAA concentrations occurred within 48 h in 7/10 cats (Figure 5). During antibiotic treatment, SAA concentrations significantly decreased by days 14 (median 2.35 mg/l, range 1.0–501; P = 0.011) and 21 (median 1.5 mg/l, range 1.1–51.4; P = 0.002). In 9/10 occurrences of APN, SAA concentrations decreased to a median of 3.1 mg/l (range 1–7.2) within a median of 14 days (range 7–21), which was not significantly different from cats with stable CKD (P = 0.130). SAA concentrations showed a moderate positive correlation (rs = 0.650) with clinical scores (Figure 6). Interestingly, neutrophil counts showed a strong positive correlation (rs = 0.737) with SAA concentrations in cats with APN (Figure 7).
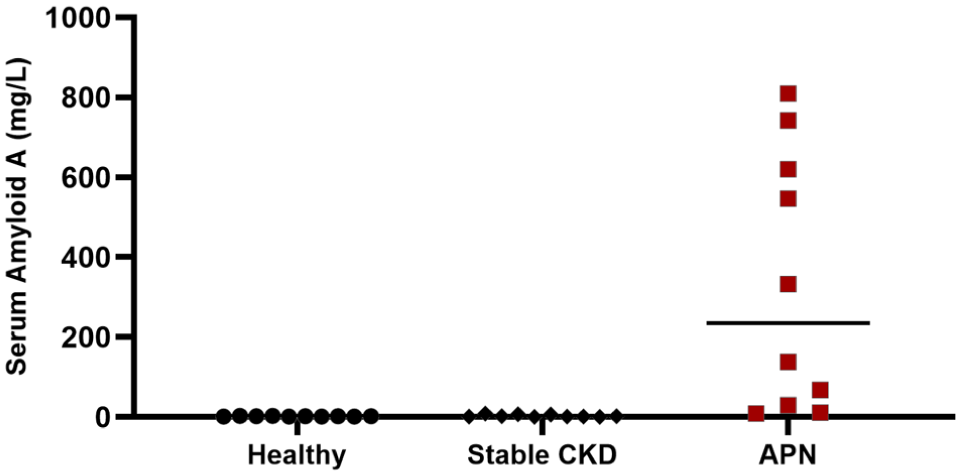
Serum amyloid A (SAA) concentrations in healthy cats (n = 10), cats with stable chronic kidney disease (CKD) (n = 10) and cats with acute pyelonephritis (APN) (n = 9). At the time of diagnosis, cats with APN had significantly higher SAA concentrations compared with healthy cats (P = 0.0008) and cats with CKD (P = 0.0002). There was no significant difference in SAA concentrations between healthy cats and cats with CKD (P >0.999)

Serum amyloid A (SAA) concentrations vs time (days) in cats with acute pyelonephritis. During antibiotic treatment, SAA concentrations significantly decreased from the time of diagnosis (day 0) to day 14 (P = 0.011) and day 21 (P = 0.002). There were no significant differences between day 0 and days 1 (P >0.999), 2 (P >0.999) or 7 (P = 0.692). In addition, there were no significant differences between days 7 and 14 (P >0.999), 7 and 21 (P = 0.722) or 14 and 21 (P >0.999). Day 0 represents the time of clinical presentation/diagnosis; days 1 and 2 represent consecutive days after diagnosis and are the first 48 h of hospitalization. It was not possible to obtain a serum sample from all cats on days 1 and 2; days 7, 14 and 21 represent consecutive days after diagnosis and are associated with outpatient treatment

Serum amyloid A (SAA) concentrations vs clinical scores in cats with acute pyelonephritis (APN). At the time of APN diagnosis (day 0) and during antibiotic treatment (days 7, 14 and 21), SAA concentrations showed a moderate positive correlation with clinical scores (rs = 0.650)

Neutrophil counts vs serum amyloid A (SAA) in cats with acute pyelonephritis (APN). At the time of APN diagnosis (day 0) and during antibiotic treatment (days 7, 14 and 21), neutrophil counts were strongly positively correlated with SAA concentrations (rs = 0.737)
Discussion
This study measured SAA concentrations at diagnosis and during serial evaluations over 21 days to better understand the potential clinical use of SAA as a biomarker in cats with antibiotic-responsive APN. The results show that SAA concentrations were significantly higher in cats with bacteriuria and a working diagnosis of APN compared with healthy cats and cats with stable CKD, supporting the idea that SAA may be a useful biomarker in cats with APN. Unlike other studies in cats, this is the first to report SAA concentrations during antibiotic therapy in cats with APN. Most cats with APN reached peak SAA concentrations within the first 48 h after initial presentation. In addition, with treatment and clinical recovery, SAA concentrations dropped to normal within a median of 14 days (Figure 5) and were moderately correlated with clinical signs (Figure 6).
Compared with other studies, the clinical features of cats with APN in this study were similar, and SAA concentrations were higher in these cats.19,28 However, despite similarities among groups of cats with APN across studies, this study reported a greater increase in SAA concentrations, with over a 200-fold increase in cats with APN, and peak SAA concentrations were observed within 48 h after hospital admission. The increases in SAA concentrations at diagnosis and the time to peak concentrations observed in this study align with those previously reported in humans with pyelonephritis.10,29,30 The observed differences in the magnitude of the rise in SAA concentrations in this population of cats with APN may be influenced by the duration of illness before presentation, disease severity or analytical differences in the SAA assay used.19,28,31 In this study, cats with APN had a median illness duration before clinical presentation of 6 days, whereas in the previous feline study, in which the duration of illness was reported, the median illness duration before presentation for cats with confirmed or suspected APN was 48 days. 19 As observed in this study, peak SAA concentrations may take up to 48 h in cats with a relatively short duration of illness. This may be clinically important because SAA concentrations in cats with APN might not have peaked or reached a specific cutoff value associated with APN at presentation, especially in cats showing acute clinical signs.
A recommended SAA concentration cutoff of above 51 mg/l has been suggested to support a diagnosis of APN in cats showing consistent clinical signs and bacteriuria. 19 Using this SAA concentration target, 8/10 occurrences of APN in this study had SAA concentrations exceeding the cutoff at the time of diagnosis. Peak SAA concentrations in two cats were 18.6 mg/l and 45.2 mg/l on day 7. Both cats had previously diagnosed pre-existing CKD and showed consistent clinical signs, worsening azotemia, evidence of bacteriuria supporting their clinical diagnosis of APN and a work-up ruling out other underlying causes. Interestingly, the cat with the peak SAA of 18.5 mg/l had an E faecalis bacteriuria. Despite responding well initially to antibiotics selected based on sensitivity results, this cat continued to have persistent E faecalis bacteriuria. The patient developed a concurrent S hominis bacteriuria with recurring clinical signs, and the SAA concentration rose further to 501 mg/l. The cat with a peak SAA of 45.2 mg/l had rods identified in the urine sediment with a negative urine culture at presentation. The bacteriuria and clinical signs resolved, and the SAA normalized by day 14 of antibiotic treatment. The unexpectedly lower SAA rises in these two cats may not represent the true peak SAA concentrations. In both cases, the highest SAA concentration may have occurred after discharge but before the reassessment on day 7 because of intermittent SAA checks after hospital discharge. Alternatively, the lower SAA concentrations might be bacteria-dependent or related to an AKI complicated by an unidentified, non-antibiotic-responsive etiology. Because the study involved only a small number of cats, it was underpowered to determine why the peak SAA concentrations were lower than expected in these two cats. However, this finding is noteworthy and suggests that further research is needed to understand SAA concentrations and how they may assist in diagnosing APN in cats.
In support of antibiotic stewardship, all cats had urine cultures performed. Cats with positive bacterial cultures received pathogen-directed antibiotic therapy, guided by antibiotic susceptibility results. Treatment with a fluoroquinolone was the most prescribed antibiotic in this group of cats with APN, aligning with published veterinary antibiotic guidelines. 8 Although urine cultures were performed in all cats, two cats had no bacterial growth. Despite negative urine cultures, these cats remained in the study and were treated with empirical antibiotic therapy based on clinical findings supporting the diagnosis of APN and a work-up that ruled out other causes of bacteriuria. This situation often occurs, especially when antibiotic treatment is started before urine collection for culture, making treatment decisions more challenging in cats suspected of having APN. During antibiotic treatment, in 9/10 occurrences of APN the cats showed clinical improvement, with resolution of bacteriuria within 7 days, normalization of SAA concentrations within 7–21 days, and a moderate positive correlation between SAA concentrations and clinical scores. Interestingly, despite others reporting significantly increased SAA concentrations in cats with CKD, 16 many of the cats in this study had pre-existing CKD with a median Cr of 2.3 mg/dl at the time of clinical recovery, yet SAA concentrations dropped to a median of 1.5 mg/l. Other studies have not assessed SAA concentrations in cats with APN during antibiotic treatment. However, the findings of this study are consistent with the timeline for normalization of SAA concentrations in people with APN undergoing antibiotic therapy and experiencing clinical recovery. 10
The three cats with more complicated clinical courses showed increased SAA concentrations after SAA dropped to below 10 mg/l. This unexpected rise in SAA concentrations during antibiotic treatment, after initial improvement, may indicate clinical relapse, as 2/3 of these cats had their antibiotics mistakenly discontinued. In one study of humans with APN, those with elevated SAA concentrations after initial improvement were classified as non-responders.10,32 Similarly, the observed increase in SAA concentrations during treatment in the three cats with APN in this study suggests that serial SAA monitoring may be clinically useful for identifying cats with APN who have a more complicated clinical course or are experiencing treatment failure.
Study limitations include the small number of cats with APN, further complicated by the diversity of bacterial isolates cultured and variability in hospitalization duration and treatment decisions. The small number of cats with APN reported in this study may limit the study’s conclusions and its generalizability to the broader population of cats clinically diagnosed and treated for APN. However, at the expense of a small sample size, the study’s inclusion/exclusion criteria were designed to recruit a defined population of cats with APN, excluding those with concurrent problems, and in alignment with the International Society for Companion Animal Infectious Diseases guidelines. 8 This is a challenging clinical population to identify, as most cats with APN are older and more likely to have multiple problems. In addition, diagnosing APN in cats remains clinically challenging, in part because pyelocentesis is required but rarely performed to obtain a definitive diagnosis; clinical signs, such as lethargy, anorexia, vomiting or fever, are often vague, and there may be limitations associated with routine diagnostic tests, including false-negative bacterial urine cultures and non-specific ultrasonographic findings. Other limitations include the intermittent intervals between SAA measurements and the adapted clinical scoring used to monitor each cat’s response. Our approach was to use a practical clinical monitoring method over the 21-day study period, recognizing that blood sampling can be difficult and often limited, especially in ill cats. Clinical recovery is inherently a subjective contributing bias because it relies on the owner’s knowledge of their pet’s normal behaviors and activities, combined with the veterinarian’s physical examination. To standardize the evaluation of clinical status in this study, a non-validated clinical scoring system adapted from a validated UTI symptom assessment questionnaire used in humans was used to convert each cat’s subjective assessment into a clinical score for comparison. 25 The validated feline Acute Patient Physiologic and Laboratory Evaluation (APPLE) score was not used because it does not account for owner-observed clinical signs or include the common indicators used to diagnose APN in cats. 33 Despite these study limitations, the variability and challenges associated with clinical assessments reflect real-world situations encountered when managing cats with APN.
Conclusions
The current interest in using SAA monitoring in cats with AKI lies in identifying the subset of cats with antibiotic-responsive disease, thereby improving treatment choices and clinical outcomes. The results of this study offer additional insights into the potential benefits and limitations of monitoring SAA concentrations in cats with APN. This study further supports the conclusion that SAA concentrations are significantly increased in cats with APN and may serve as an additional diagnostic tool for veterinarians to identify affected cats and monitor each cat’s systemic response to treatment, including supporting assessment of clinical recovery and detection of treatment failures.
Footnotes
Acknowledgements
The authors would like to thank the faculty, technicians, staff and students at University Wisconsin Veterinary Care for their interest and active participation in the study.
Author note
This work was presented in part as a research abstract at the 2024 International Society for Companion Animal Infectious Diseases Symposium, Vancouver, BC, Canada.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was made possible through funding from the University of Wisconsin, School of Veterinary Medicine, Companion Animal Fund.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognized high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). For any animals or people individually identifiable within this publication, informed consent (verbal or written) for their use in the publication was obtained from the people involved.