
Abstract
Objectives
This study aimed to compare the prevalence and time to resolution of azotaemia between male cats presented with initial and recurrent urethral obstruction (UO), and to evaluate risk factors for extended duration of urethral catheterisation and hospitalisation.
Methods
A multicentre, retrospective study of male cats that underwent urethral catheterisation for UO was conducted. Cats were excluded if they did not have a UO on presentation, had previously diagnosed chronic kidney disease, had incomplete medical records or if they were referred by another clinic after decompression. Prevalence of azotaemia (serum or plasma creatinine >140 µmol/l) and time to resolution were compared between cats with initial and recurrent UO. Risk factors evaluated for extended duration of catheterisation and hospitalisation included signalment, history of UO, history of lower urinary tract signs (LUTS), diet, recent medications, lifestyle (indoor-only or indoor-outdoor), housing status (single or multi-cat) and azotaemia on presentation.
Results
Cats were less likely to be azotaemic on presentation if they had a history of UO (P = 0.015) or LUTS (P = 0.014). Azotaemic cats were 1.92 times more likely to undergo a longer duration of catheterisation compared with non-azotaemic cats (95% confidence interval [CI] 1.40–2.65; P <0.001) and 1.81 times more likely to have a longer hospitalisation (95% CI 1.28–2.57; P <0.001). Resolution of azotaemia was achieved in less than 48 h in 89/127 (70.1%) cats that were azotaemic on presentation (95% CI 61.3–77.9). Recurrent UO was not associated with longer time to resolution of azotaemia (P = 0.395).
Conclusions and relevance
Cats are less likely to present with azotaemia during recurrent UO episodes, which might be due to increased caregiver vigilance. Resolution of azotaemia occurred within 48 h for most cats. There was no difference in catheterisation and hospitalisation duration between cats with initial and recurrent UO.
Plain language summary
Urethral obstruction (a blockage that prevents a cat from passing urine) is a common emergency in male cats. When this happens, waste products can build up in the blood, leading to abnormal kidney values on blood tests. This might affect how long a cat needs to stay in hospital. It is unknown whether cats that have repeated blockages are more or less likely to develop abnormal kidney values than cats with a first-time blockage, or whether their recovery time differs. This study reviewed the medical records of male cats treated for urethral obstruction at several veterinary hospitals over a 5-year period. The researchers compared cats experiencing their first blockage with those that had had previous episodes. They looked at how often cats had abnormal kidney values, how long it took for these values to return to normal and which factors were associated with longer urinary catheter use or longer hospital stays. Cats that had had previous urethral obstructions or lower urinary tract problems were less likely to have abnormal kidney values when they arrived at the hospital. Cats that had abnormal kidney values were more likely to have a urinary catheter for longer and to stay in hospital for a longer period. However, having a previous obstruction did not affect how quickly kidney values returned to normal. In most cases, kidney values returned to normal within 48 h of treatment. Overall, cats with repeat urethral obstructions were less likely to have abnormal kidney values, possibly because caregivers recognised the signs and sought treatment earlier. Importantly, cats with repeat obstructions did not stay in hospital longer than cats with a first-time obstruction, meaning treatment time and costs are expected to be similar.
Introduction
Urethral obstruction (UO) is a common complication in cats with lower urinary tract signs (LUTS), with a substantial risk of recurrence in affected individuals.1,2 Causes of UO include urethral plugs associated with feline idiopathic cystitis or bacterial cystitis, urolithiasis, neoplasia, strictures and functional obstruction.3,4 The incidence of UO is in the range of 0.54–3.4%, with higher incidence reported in emergency than in general practice.5,6 Neutered male cats are at an increased risk of UO. 7
Common clinical signs in cats with UO include stranguria, dysuria, abnormal vocalisation, lethargy, anorexia and vomiting. 8 Perfusion abnormalities, hyperkalaemia, arrhythmias and cardiovascular shock are potential life-threatening consequences.2,8,9 The short-term prognosis for UO is favourable, with survival rates of over 90% reported in teaching hospital and referral populations.2,7,8 Reobstruction can occur, with the highest risk period being the first 30 days after discharge. 10 Risk factors for reobstruction include increasing age and urinary catheter diameter.10,11 Recurrent LUTS occur in 51% and death or euthanasia in 26% of cats with UO. 1 Recurrent obstruction is the most frequently cited reason for euthanasia, accounting for more than 80% of recorded deaths. 1 UO carries financial implications for caregivers, which can influence decision-making. Understanding factors that impact treatment costs and long-term clinical consequences, such as prolonged renal recovery, might assist in management planning and decisions regarding euthanasia.
Azotaemia is reported in up to 85% of cats presented for UO.2,12 Azotaemia does not carry an increased risk of reobstruction; however, azotaemic cats might require a longer duration of urinary catheterisation.4,10,11 Azotaemia is predominantly post-renal owing to increased hydrostatic pressure within the renal tubules and subsequent decrease in glomerular filtration rate (GFR).13,14 Resolution of azotaemia is typically seen after decompression, and presenting creatinine concentrations are not predictive of renal function after decompression. 14 Elevated urinary cystatin B concentrations have been observed in approximately half of cats with UO, suggesting a component of intrinsic renal injury. 15 Tubular damage can occur from ischaemia and inflammation after prolonged obstruction.15,16
It is unknown if renal recovery is complete after UO, and whether previous kidney injury affects hospitalisation time during recurrent episodes. Blood biomarkers used for evaluation of GFR have limited sensitivity; therefore, minor functional impairment cannot be identified.13,15 The impact of previous UO on the likelihood or duration of azotaemia in cats presenting with recurrent obstruction has not been evaluated. Given the potential for longer hospitalisation periods associated with azotaemia, it is important to understand differences between cases of initial and recurrent UO. This knowledge could aid in establishing expectations for the management of subsequent episodes and guide financial planning, which could reduce caregiver stress and improve long-term outcomes.
The present study aimed to compare the prevalence and time to resolution of azotaemia in male cats presenting with initial and recurrent UO. The study further aimed to evaluate risk factors for extended duration of catheterisation and hospitalisation.
Materials and methods
Case selection and data collection
A multicentre, retrospective, cross-sectional study was conducted of cats with UO that were presented to five small animal referral hospitals in Sydney, Australia. Cats with UO that underwent urethral catheterisation between January 2020 and December 2024 were identified by invoice items, including ‘male urinary catheter’, ‘urethral obstruction’, ‘urinary obstruction’ and ‘unblocking male cat’. For inclusion, cats were required to be male, presented as first opinion cases, meet the study definition for UO, have undergone placement of an indwelling urinary catheter and have a minimum of one serum or plasma creatinine concentration measured within 24 h of admission. Cats were excluded if they were female, had previously diagnosed chronic kidney disease (CKD) or if they were transferred from another clinic after initial urethral catheterisation or decompressive cystocentesis. Cases that did not meet the study definition of UO or had incomplete medical records were excluded. For cats presented to the emergency room more than once, only the first occurrence of UO recorded at that hospital was included. Cases were assessed for eligibility by a single author (VJS).
Deidentified data were collated into a spreadsheet. Extracted data included age, neuter status, breed, history, clinical signs and physical examination findings. Lifestyle (indoor-only or indoor-outdoor), housing status (single or multi-cat household) and prior history of LUTS reported by caregivers was documented.
Clinicopathological data included presenting serum and/or plasma biochemistry, venous blood gas analysis, urinalysis, aerobic urine culture and serial serum and/or plasma creatinine concentrations. Time points were recorded for each creatinine measurement to the nearest 12 h. Radiographic findings were obtained where available.
To ensure standardisation and minimise misclassification from imprecise time records, durations of urinary catheterisation and hospitalisation were recorded to the nearest 12 and 24 h, respectively. Details of interventions, treatments, complications, urine output (UOP) and outcomes were included. Outcomes included discharge to home, euthanasia, death in hospital or transfer to general practice.
Definitions
A diagnosis of UO consisted of a firm, inexpressible bladder on physical examination. A history of LUTS was defined as any prior episode of clinical signs referable to the lower urinary tract (eg, stranguria or haematuria) occurring before the current presentation, with a period of clinical resolution and excluding signs considered to be part of the current episode. Azotaemia was defined as a serum or plasma creatinine concentration greater than 140 µmol/l in accordance with International Renal Interest Society guidelines for acute kidney injury (AKI) grade II and above. 17 Time of resolution of azotaemia (for cats presenting with azotaemia) was defined as the earliest time point at which the creatinine concentration measured 140 µmol/l or less. Time to resolution was defined as the number of hours between the initial creatinine measurement and the time of resolution of azotaemia. Post-obstructive diuresis (POD) was defined as a UOP greater than 2 ml/kg/h at any time point after urinary catheterisation.18,19 Iatrogenic bacteriuria was defined as bacteriuria detected on urine culture or sediment examination after urinary catheterisation when the initial urinalysis and culture were negative.
Equipment
Biochemistry data were obtained using in-house IDEXX Catalyst analysers. Venous blood gas analysis was performed using Radiometer ABL90 or IDEXX VetStat analysers. Urinalysis was performed in-house or at an external reference laboratory. In-house sediment examination included manual microscopy or assessment by IDEXX SediVue Dx. The presence of bacteriuria was determined by microscopy, point-of-care immunoassay (RapidBac) or urine culture. Urine culture results were preferentially used to assign bacteriuric stat.
Statistical analysis
The sample size necessary to detect a small-to-moderate difference in the proportion of cats presenting with azotaemia between cats with and without prior UO was estimated using a two-tailed z-test for independent proportions. A baseline proportion of 85% was used, with α = 0.05, 80% power and an allocation ratio of 5:1. The required overall sample size was 462 cats. Sample size calculations were performed using G*Power 3.1.
Descriptive analyses and statistical analyses were performed using SPSS Statistics (version 31.0.0.0; IBM) and Genstat (v 22; VSN International), respectively. Time variables were categorised to account for limitations in record precision. Time to resolution of azotaemia was categorised into less than 24 h, 24–47 h, 48–60 h and more than 60 h. Duration of urethral catheterisation was categorised into 12–24 h, 25–36 h, 37–60 h and more than 60 h. Duration of hospitalisation was categorised into 1–2, 3–4 and more than 4 days. Descriptive statistics were performed for patient signalment: age (<3, 3–5, >5–7 and >7 years), neuter status (yes/no), breed (domestic/pedigree), lifestyle (indoor-only/indoor-outdoor), housing status (single/multi-cat home), diet (wet, dry or mixed), LUTS history, medication history, clinicopathological data, radiographic findings, interventions, complications and outcomes. Medication history included whether cats had received non-steroidal anti-inflammatory drugs (NSAIDs), antimicrobials or prazosin in the 4 weeks before UO. A binomial confidence interval (CI) for the proportion of cats presenting with azotaemia and achieving resolution of azotaemia was calculated using the Clopper-Pearson method. Risk factors were analysed for azotaemic presentation. The effect of each variable listed above on the presence of azotaemia was assessed using logistic regression with an underlying binomial distribution. Each categorical outcome – catheterisation duration, hospitalisation duration and time to resolution – was analysed using ordinal logistic regression. Odds ratios, CIs and P values were obtained for all analyses. For all statistical analyses, P <0.05 was considered significant.
Results
Cats
A total of 863 cats that underwent urethral catheterisation were identified during initial data collection, and 601 cats were included in the study. The other 262 were excluded for reasons outlined in Figure 1. Of the included cats, 580 were neutered males and 19 were entire males (missing data, n = 2). The median age was 4.08 years (interquartile range [IQR] 2.75–7.00). There were 461 domestic and 128 pedigree cats (missing data, n = 12, see Table S1 in the supplementary material). Most cats were indoor-only (n = 286, 65.1%; missing data, n = 162) and from multi-cat households (n = 276, 64.6%; missing data, n = 174). Cats were most frequently fed a combination of wet and dry diets (n = 246, 63.4%; missing data, n = 213). A history of UO was reported in 100 cats (17.0%; missing data, n = 13), with a median of one prior obstructive episode (range 1–4). A history of LUTS was reported in 284 cats (48.5%; missing data, n = 16). A total of 76 cats (13.5%; missing data, n = 39) had been administered NSAIDs within the 4 weeks before presentation. History features are detailed in Table 1.
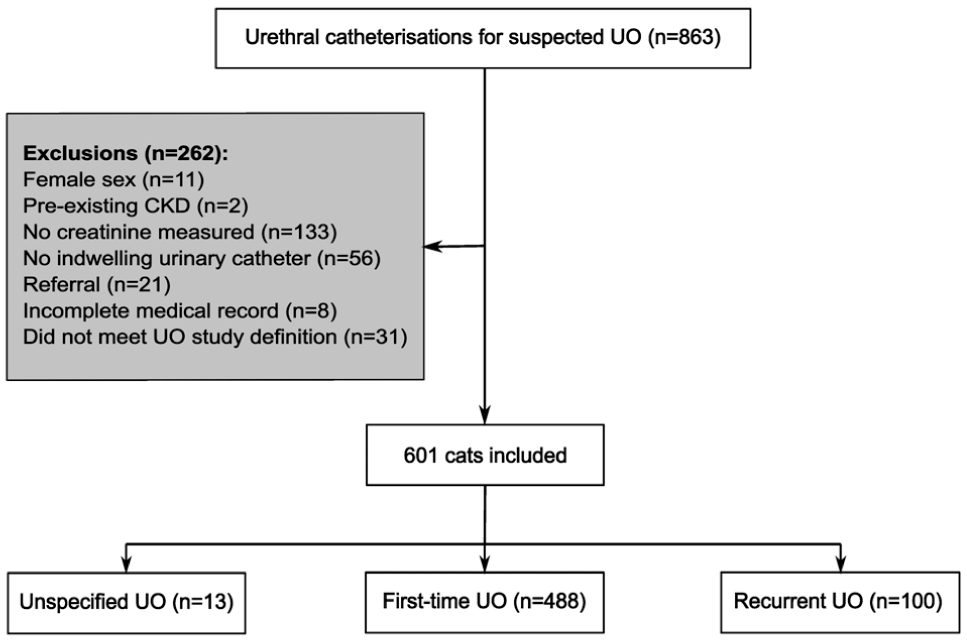
Flow diagram demonstrating inclusion and classification of male cats with UO. CKD = chronic kidney disease; UO = urethral obstruction
History features of cats with urethral obstruction
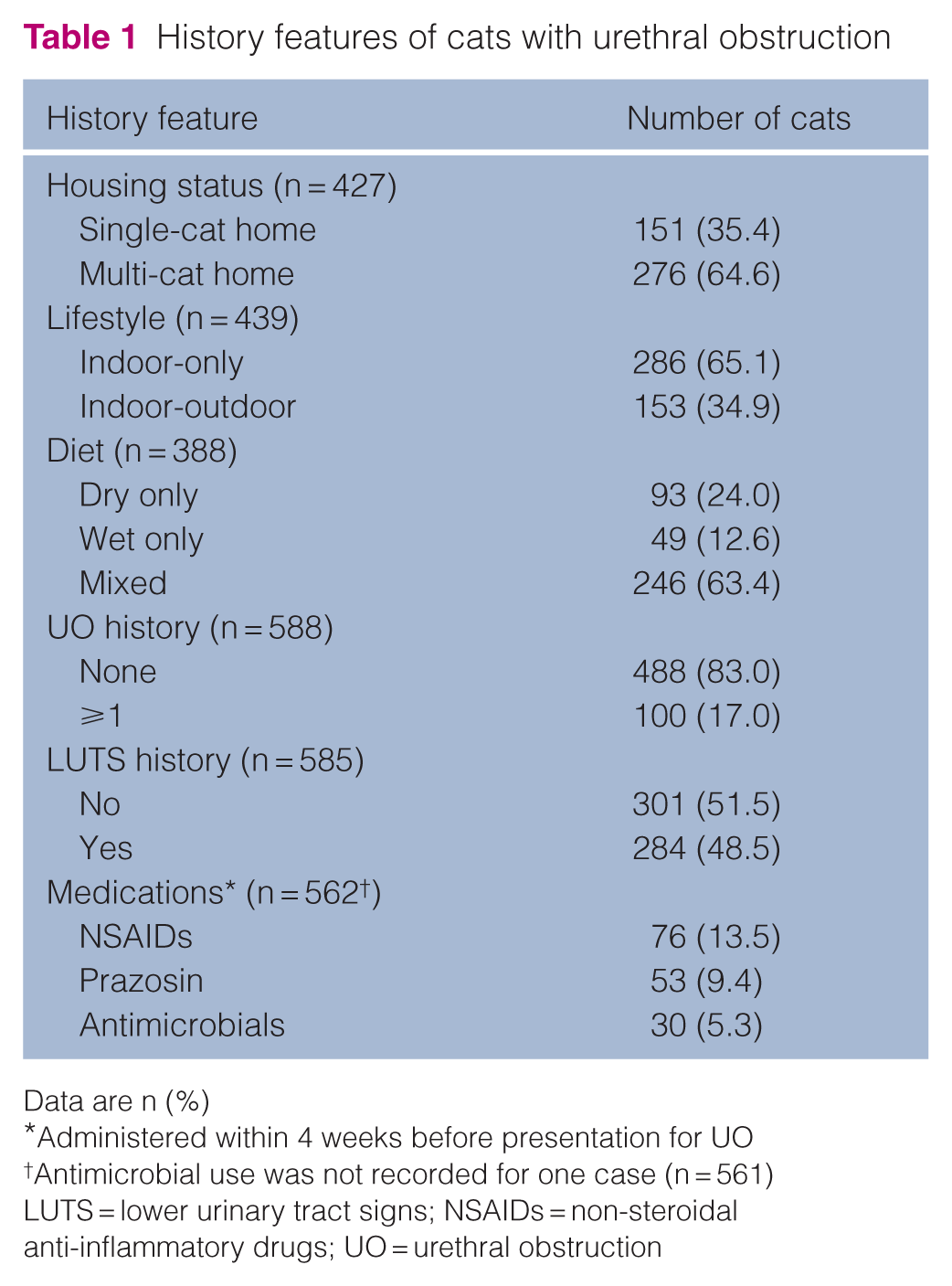
Data are n (%)
Administered within 4 weeks before presentation for UO
Antimicrobial use was not recorded for one case (n = 561)
LUTS = lower urinary tract signs; NSAIDs = non-steroidal anti-inflammatory drugs; UO = urethral obstruction
Diagnostic findings
Venous blood analysis, biochemistry and urinalysis findings are presented in Table 2. A total of 333 (55.4%) cats were azotaemic on presentation (95% CI 51.3–59.4). The median creatinine concentration on presentation was 156 µmol/l (range 57–3222; IQR 116–411). A total of 126 cats (21.7%; missing data, n = 21) were hyperkalaemic on presentation (95% CI 18.6–25.3). Urine sediment examination and culture findings are presented in Table 3. Initial urine samples were collected by cystocentesis or sterile catheterisation. Bacteriuria was present in 76 cases (15.6%; missing data, n = 113). Initial urine culture was performed for 360 cats, with 57 (15.8%) returning positive results. Escherichia coli (n = 33) was the most frequently isolated bacterium, followed by Staphylococcus felis (n = 10), Enterococcus species (n = 4), Streptococcus species (n = 3) and Pseudomonas species (n = 2). The following were isolated from one sample each: Enterobacter cloacae complex, Enterobacter hormaechei, Proteus species, Serratia marcescens, Staphylococcus pseudintermedius and Staphylococcus simulans.
Presenting clinicopathological data for cats with urethral obstruction
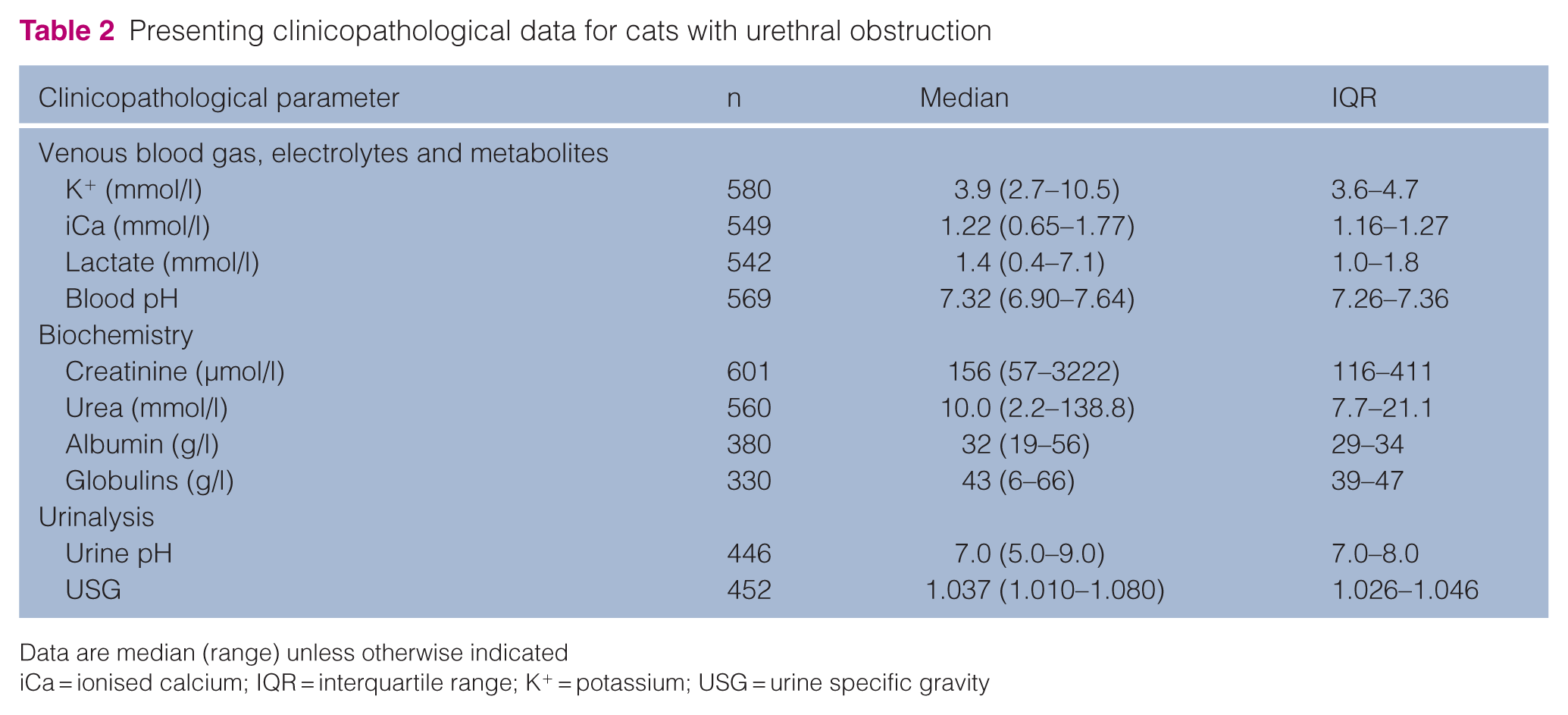
Data are median (range) unless otherwise indicated
iCa = ionised calcium; IQR = interquartile range; K+ = potassium; USG = urine specific gravity
Results of initial urine sediment examination and culture for cats with urethral obstruction
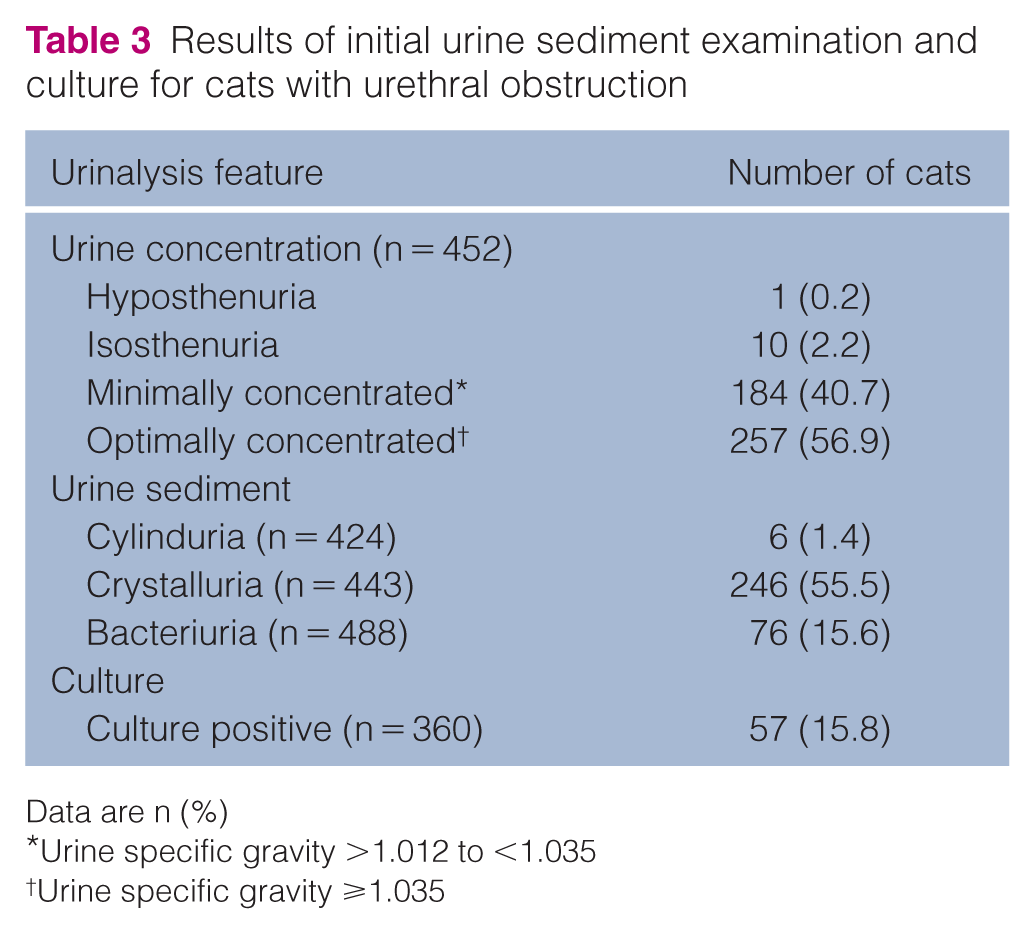
Data are n (%)
Urine specific gravity >1.012 to <1.035
Urine specific gravity ⩾1.035
At least one abdominal radiographic view was acquired in 488 (81.6%) cats. Radiopaque uroliths were identified in 53/481 cats (11.0%; missing data, n = 7).
Predictors of azotaemia
Cats were 1.7 times less likely to be azotaemic on presentation if they had a history of UO (95% CI 1.1–2.6; P = 0.015) and 1.5 times less likely to be azotaemic if they had a history of LUTS (95% CI 1.1–2.1; P = 0.014). No other significant associations were found (Table 4).
Results of logistic regression analysis of predictors of azotaemia in cats with urethral obstruction
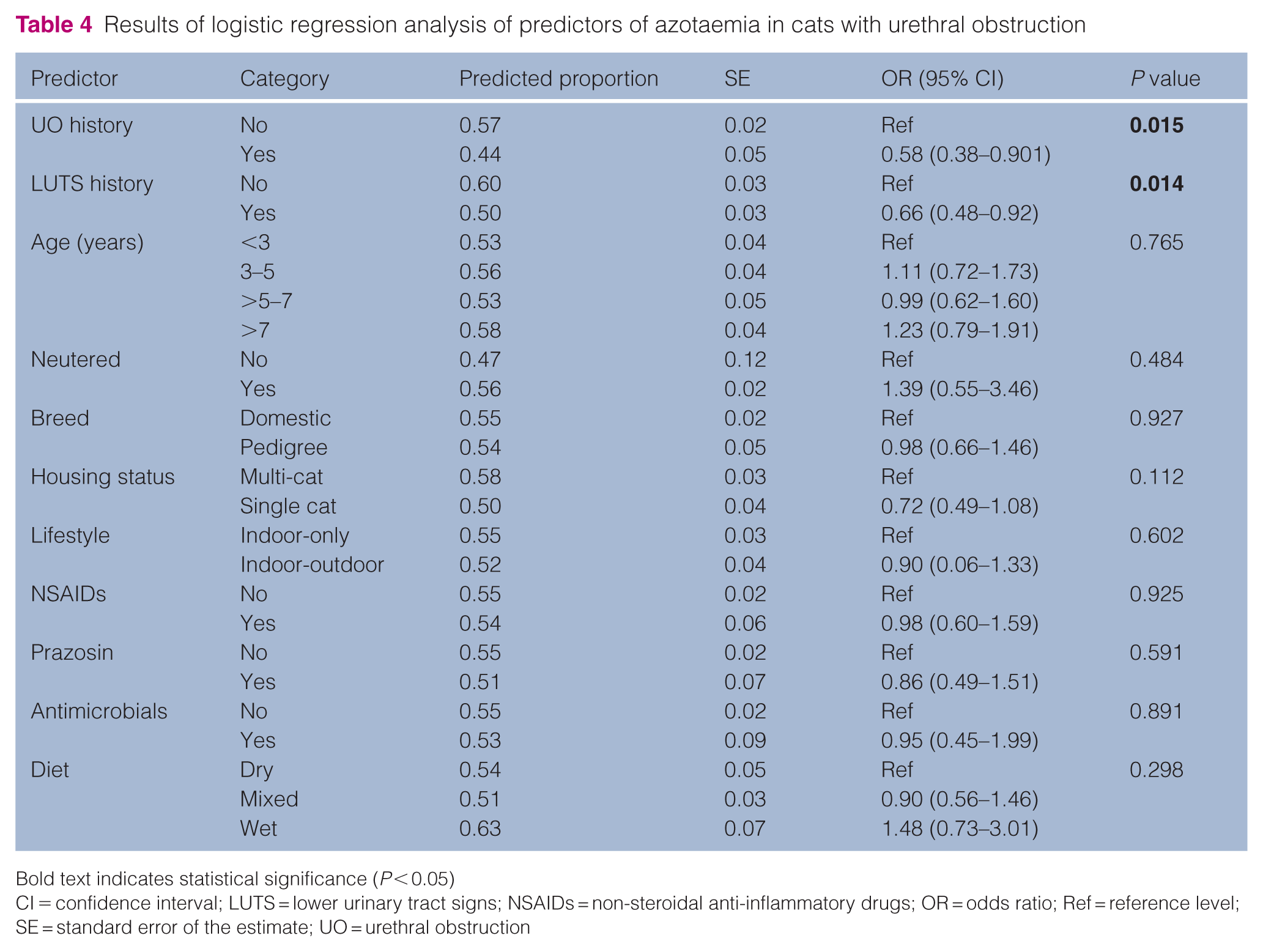
Bold text indicates statistical significance (P < 0.05)
CI = confidence interval; LUTS = lower urinary tract signs; NSAIDs = non-steroidal anti-inflammatory drugs; OR = odds ratio; Ref = reference level; SE = standard error of the estimate; UO = urethral obstruction
Complications, interventions and treatments
Complication rates, interventions and medications administered are presented in Tables 5 and 6. POD was a common finding, occurring in 389 cats (89.0%; missing data, n = 164). Urine output data were recorded for 436 cats. The median maximum UOP was 4.0 ml/kg/h (range 0.7–24.0). Frequently prescribed medications included alpha (α)1-adrenergic agonists (n = 201, 33.4%) and antimicrobials (n = 146, 24.3%). Of the 146 cats that received antimicrobials, 43 (29.5%) had positive urine cultures.
Complication rates in hospitalised cats undergoing treatment for UO
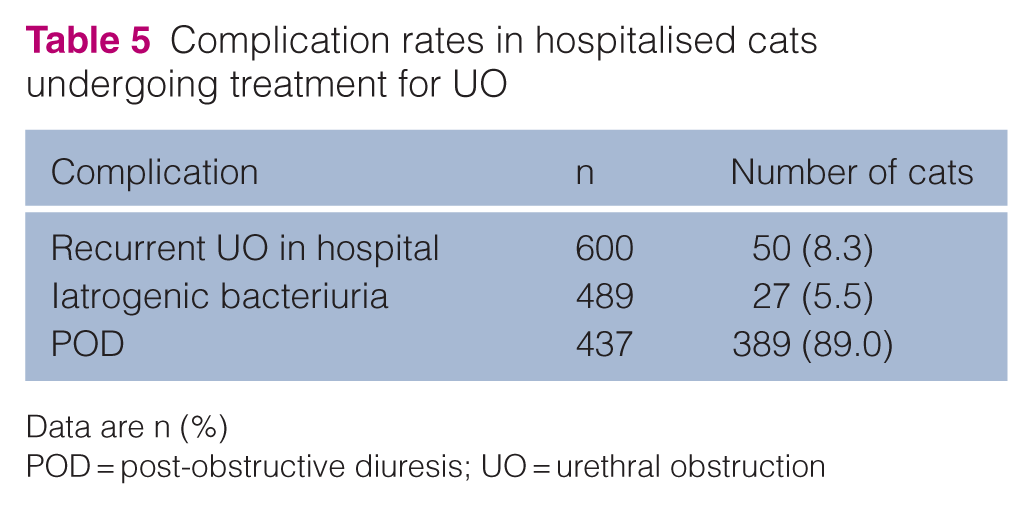
Data are n (%)
POD = post-obstructive diuresis; UO = urethral obstruction
Frequency of interventions and treatments in cats hospitalised for urethral obstruction
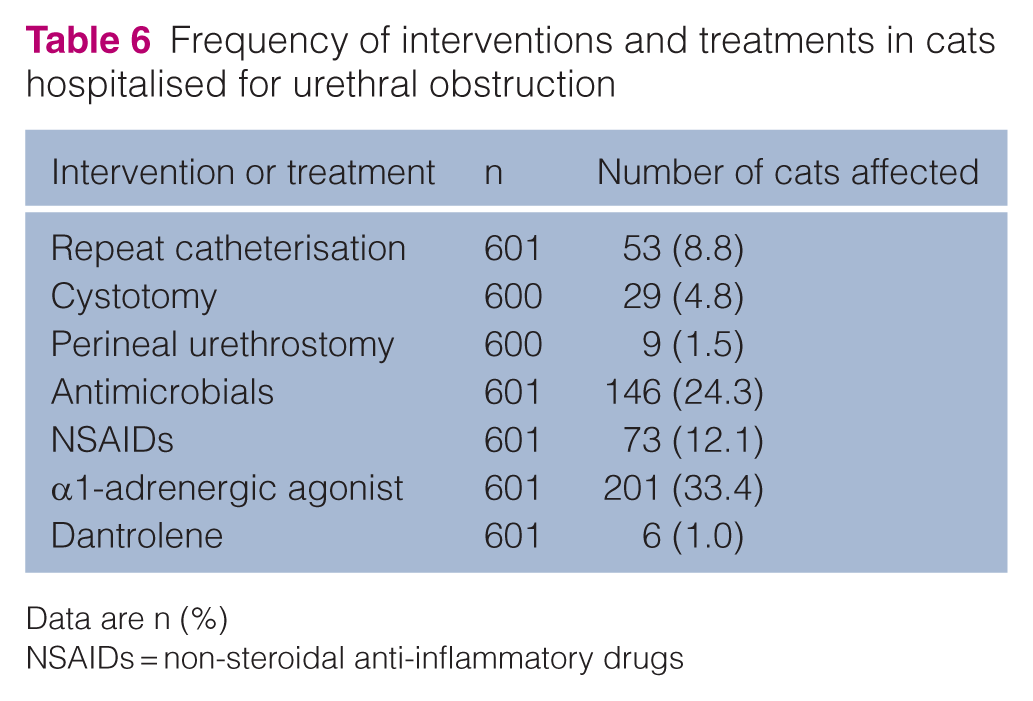
Data are n (%)
NSAIDs = non-steroidal anti-inflammatory drugs
Clinical outcomes
Cats that were azotaemic on presentation were 1.92 times (95% CI 1.40–2.65) more likely to undergo a longer duration of catheterisation compared with non-azotaemic cats (P <0.001). Cats that were azotaemic on presentation were 1.81 times (95% CI 1.28–2.57) more likely to have a longer hospitalisation compared with non-azotaemic cats (P <0.001). Cats that were hyperkalaemic (potassium ⩾5.0 mmol/l) on presentation were 2.21 times (95% CI 1.49–3.28) more likely to have a longer hospitalisation compared with eukalaemic cats (P <0.001). No other significant associations in relation to duration of catheterisation or hospitalisation were found (Tables 7 and 8). Of the 333 azotaemic cats, 227 cats had serial creatinine measurements. Of these, 127 cats were monitored until a creatinine concentration of 140 µmol/l or less was recorded. In the majority of cats for which resolution was documented, azotaemia resolved within 48 h (n = 89, 70.1%; 95% CI 61.3–77.9; missing data, n = 8). Resolution was achieved by 60 h in 116 cats (91.3%; missing data, n = 8; 95% CI 85.0–95.6). The median time to resolution was 24 h (range 12–144). There was no significant difference in time to resolution of azotaemia between cats with a history of UO and cats without prior UO (P = 0.395). No significant associations in relation to the time to resolution of azotaemia were found (Table 9). The overall case fatality rate was 1.5% (Table 10). A total of 590 cats (98.5%; missing data, n = 2) survived to discharge, including cats that were transferred to their general practitioner.
Results of ordinal logistic regression analysis of predictors of longer duration of catheterisation in cats with urethral obstruction
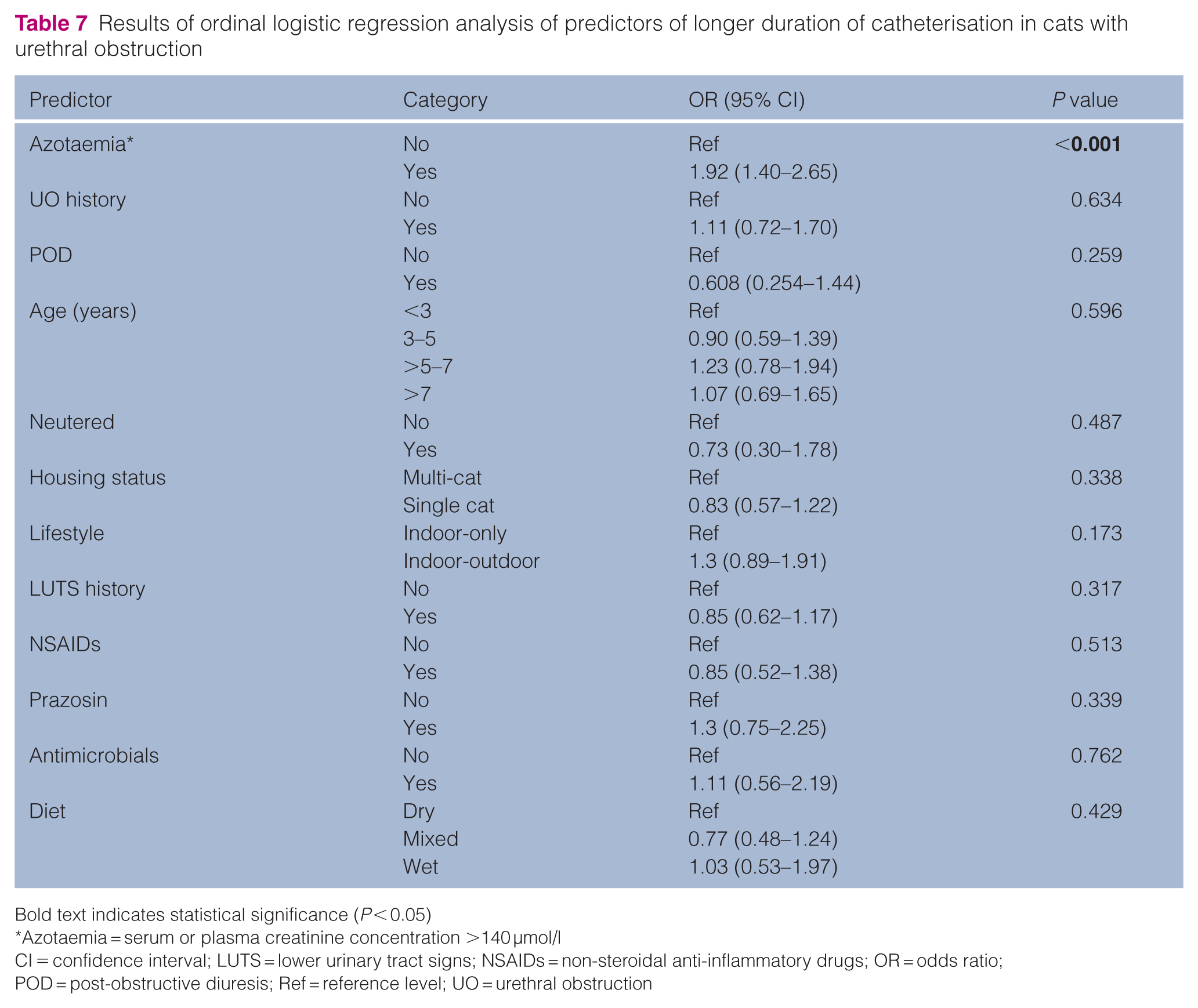
Bold text indicates statistical significance (P < 0.05)
Azotaemia = serum or plasma creatinine concentration >140 µmol/l
CI = confidence interval; LUTS = lower urinary tract signs; NSAIDs = non-steroidal anti-inflammatory drugs; OR = odds ratio; POD = post-obstructive diuresis; Ref = reference level; UO = urethral obstruction
Results of ordinal logistic regression analysis of predictors of longer duration of hospitalisation in cats with UO
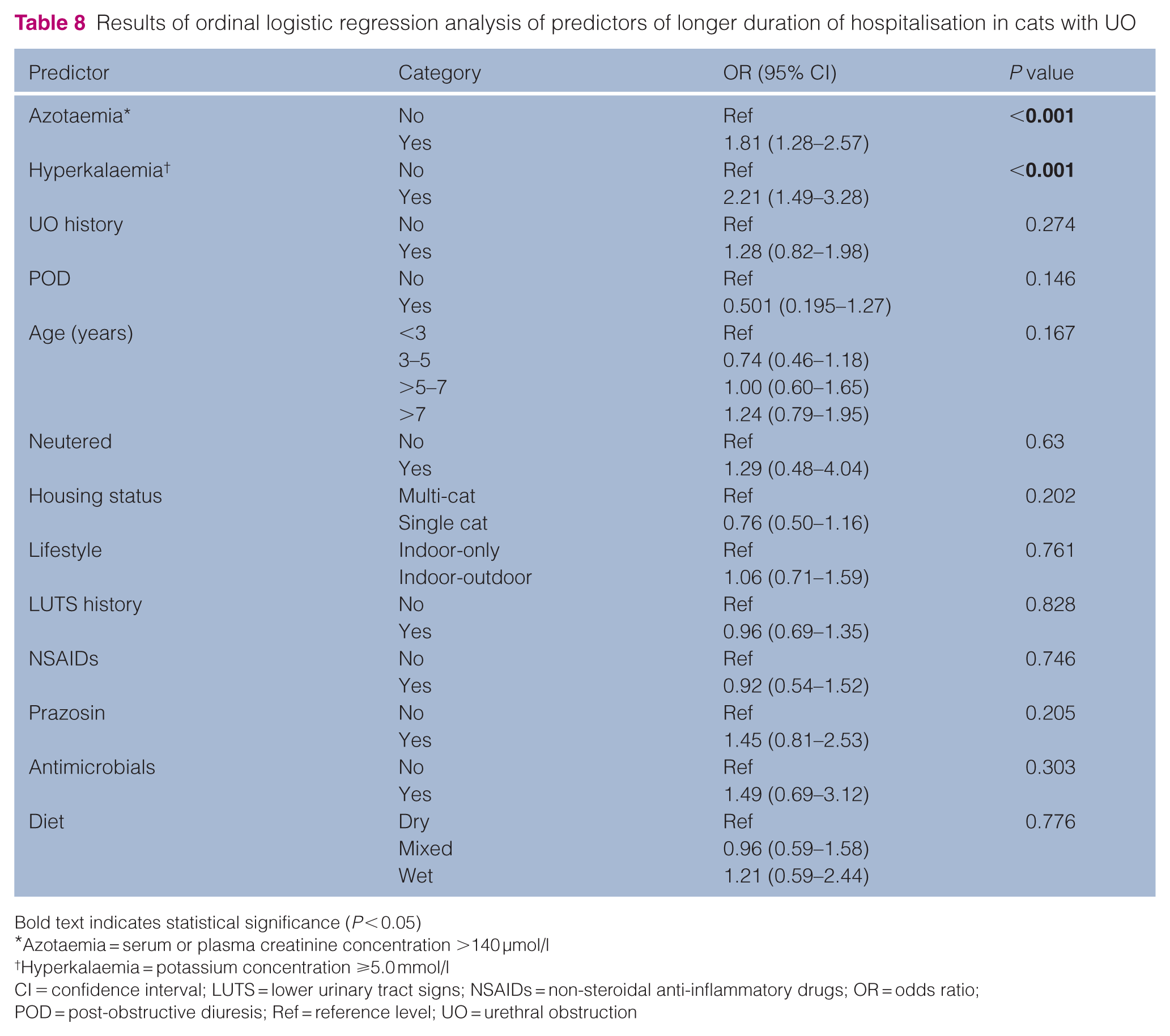
Bold text indicates statistical significance (P < 0.05)
Azotaemia = serum or plasma creatinine concentration >140 µmol/l
Hyperkalaemia = potassium concentration ⩾5.0 mmol/l
CI = confidence interval; LUTS = lower urinary tract signs; NSAIDs = non-steroidal anti-inflammatory drugs; OR = odds ratio; POD = post-obstructive diuresis; Ref = reference level; UO = urethral obstruction
Results of ordinal logistic regression analysis of predictors of time to resolution of azotaemia in cats with UO
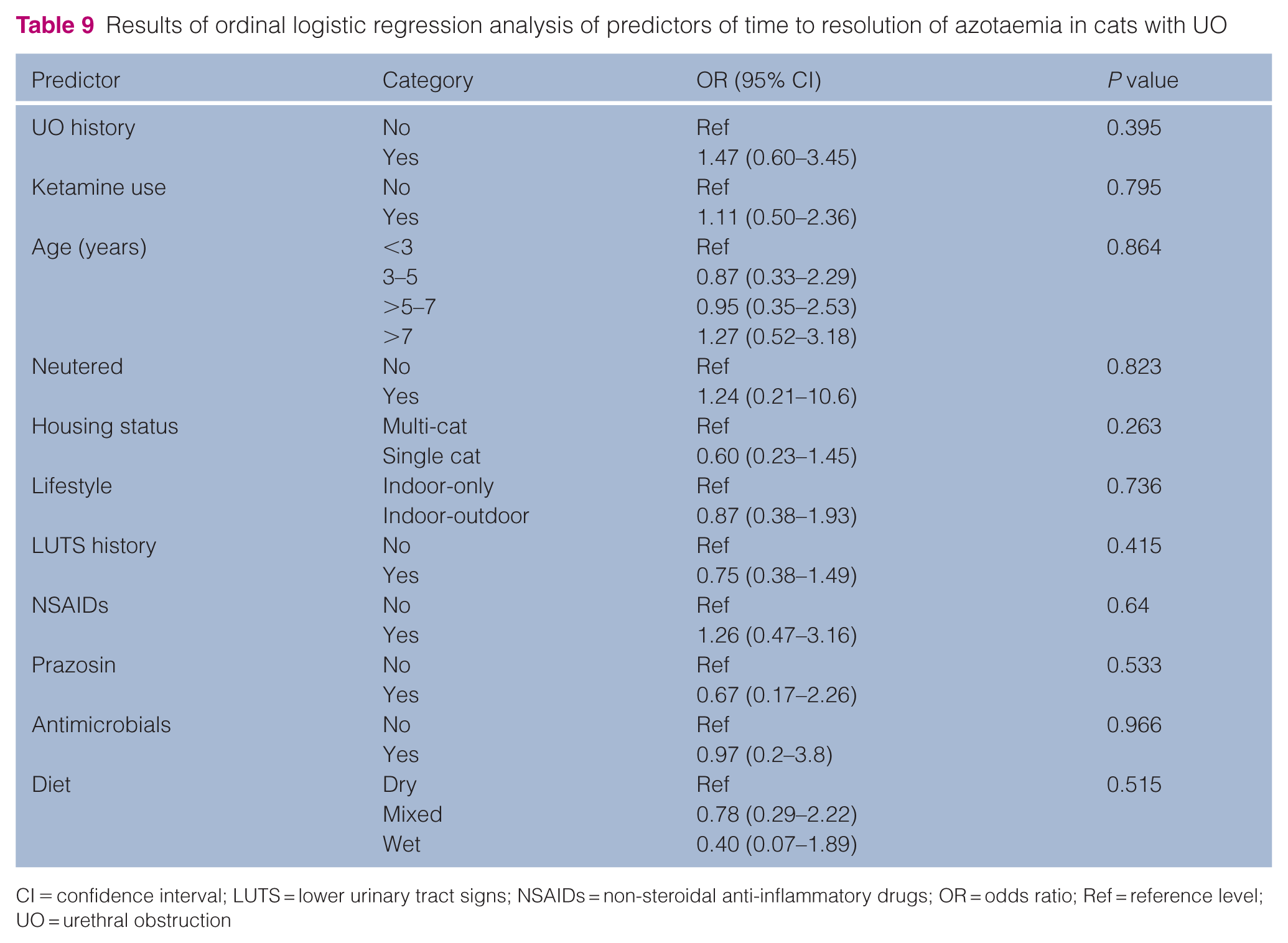
CI = confidence interval; LUTS = lower urinary tract signs; NSAIDs = non-steroidal anti-inflammatory drugs; OR = odds ratio; Ref = reference level; UO = urethral obstruction
Survival outcomes in hospitalised cats undergoing treatment for urethral obstruction
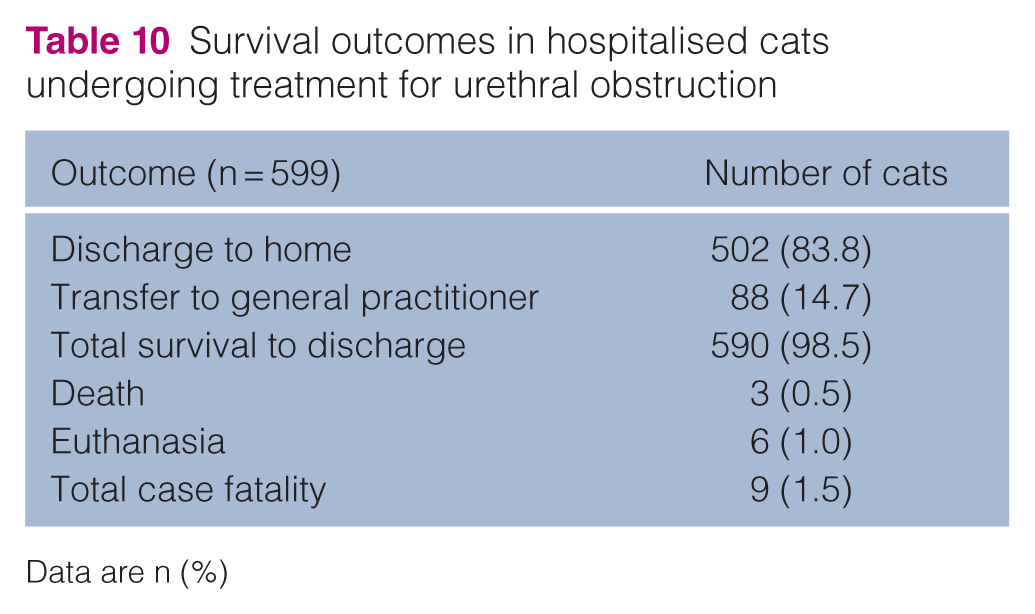
Data are n (%)
Discussion
In the present study, cats with recurrent UO were less likely to have azotaemia on presentation than cats without prior UO. Although azotaemic cats were more likely to undergo longer durations of catheterisation and hospitalisation, no such difference was found between cats with recurrent UO and those presenting for initial obstruction. In addition, there was no association between recurrence status of UO and time to resolution of azotaemia. These findings suggest that catheterisation duration and associated hospitalisation costs are not expected to be greater for subsequent UO episodes.
There was a lower prevalence of azotaemia in cats presenting with recurrent UO compared with cats presenting for initial UO. Cats with a history of LUTS, with or without prior UO, were also less likely to present with azotaemia. The reduced risk of azotaemia in cats with recurrent UO and those with a history of LUTS might reflect increased vigilance in caregivers of previously affected cats. Overall, the prevalence of azotaemia in cats with UO was lower than previously reported rates of 77.1–85%.2,12 This discrepancy might be explained, at least in part, by differences in sampling timeframes between studies. In the present study, initial creatinine concentrations were measured within 24 h of presentation. In some cases, sample collection might have occurred after decompression, which could have led to an underestimation of azotaemia. Increased awareness of clinical signs might lead to earlier intervention, with cats presented to the emergency room before the onset of azotaemia. Lifestyle and housing status were not associated with increased likelihood of azotaemia, which suggests that recognition of illness in indoor-outdoor cats or those in multi-cat homes was not delayed in this cohort.
Azotaemia at presentation was associated with a longer duration of catheterisation and hospitalisation. Hyperkalaemia at presentation was also associated with a longer duration of hospitalisation. Occurrence of POD was not associated with these outcomes; however, the degree of POD could not be assessed because of data limitations. Current consensus guidelines recommend urinary catheterisation for 24–36 h, noting that azotaemic cats need more time. 4 Resolution of azotaemia and electrolyte abnormalities is often a primary criterion for catheter removal and hospital discharge, influencing clinician decision-making. Azotaemia is a risk factor for severe POD, which is associated with increased hospitalisation duration. 18 POD can persist for several days, during which ongoing polyuria could result in continued fluid and electrolyte losses, necessitating prolonged fluid therapy. 19 Accordingly, the absence of an observed association between POD and outcome measures in this study should be interpreted cautiously. Despite the lower prevalence of azotaemia in the recurrent UO group, there was no difference in catheterisation or hospitalisation duration between cats with initial and recurrent UO. This suggests the difference is not large enough to influence overall outcomes between groups. Recurrent UO was not associated with a longer time to resolution of azotaemia. Only a small number of cats underwent serial monitoring of creatinine concentrations; therefore, the present study was likely underpowered to detect a difference in resolution time between groups.
For azotaemic cats that were monitored to resolution of azotaemia, the majority achieved resolution within 48 h of presentation and over 90% achieved resolution within 60 h. Longer times to resolution were observed in a small number of cats. Future prospective studies could allow for more detailed evaluation of renal function recovery in cats with UO, including risk of persistent azotaemia and long-term outcomes. Neither the prevalence of azotaemia at presentation nor the time to resolution was affected by prior administration of NSAIDs, antimicrobials or prazosin. Importantly, the administration of NSAIDs before UO did not adversely affect outcomes. In addition, although dry diets are a risk factor for UO and LUTS, they did not appear to adversely affect outcomes in the present study.2,20
The retrospective design placed limitations on data collection and availability. Although laboratory reports were time-stamped in the provided records, the timing of sample collection was not documented, which could have produced errors in the assessment of resolution times. Furthermore, resolution times were likely over-estimated because of significant gaps between sampling times. In many cases, resolution could have occurred earlier than recorded. Hospitalisation and catheterisation times were difficult to precisely identify and included cases that were transferred to a general practitioner for ongoing care. Overall treatment duration was likely underestimated for both groups.
All creatinine measurements in this study were undertaken on the same type of analyser, which mitigated measurement bias associated with non-standardised equipment. Only a proportion of cases included serial measurements, which limited statistical power. A small number of cats were monitored to complete resolution of azotaemia, likely due to cost constraints, restricted follow-up and variable treatment endpoints. As such, incomplete renal recovery could not be evaluated. Although cats with reported CKD were excluded from this study, previous medical histories were not available for assessment. Given the prevalence of CKD in cats, it is likely that a proportion of included cats were affected.21,22 The impact of pre-existing CKD on renal recovery in UO is unknown.
Prospective studies would more precisely evaluate resolution of azotaemia and duration of treatment. Post-discharge follow-up of azotaemic cats would facilitate assessment of long-term outcomes, including persistence of any reduction in renal function after recovery from obstruction. Evaluation of urinary biomarkers in affected cats could aid understanding of intrinsic renal injury and recovery after UO. In addition, identification of risk factors for adverse outcomes and reduced welfare could enhance guidelines for the care of cats with LUTS and UO. Incorporating caregiver surveys could aid understanding regarding the decision to euthanase, identifying areas of care that need to be addressed to reduce overall fatality.
Conclusions
Cats are less likely to present with azotaemia during subsequent UO episodes, which could be due to caregiver experience. Resolution of azotaemia occurred within the first 48 h for most cats. There was no difference in catheterisation and hospitalisation duration between cats with initial and recurrent UO; therefore, the costs of medical management are anticipated to be similar. The results of this study suggest that current guidelines and treatment expectations are applicable to cats with recurrent UO.
Supplemental Material
Table S1
Breed distribution of cats with urethral obstruction
Footnotes
Supplementary material
The following file is available as supplementary material:
Table S1. Breed distribution of cats with urethral obstruction.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognized high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.