
Abstract
Biobehavioral research is becoming more established in nursing. This research paradigm includes a focus on the interactions of biological and behavioral variables and their impact on health outcomes. Nurse researchers have incorporated genomics as a research focus. However, biobehavioral and genomic approaches have often been viewed as separate paradigms. This article provides research exemplars from the liver transplantation population to illustrate how genomics can be integrated into a biobehavioral model of nursing research. Examples of how this integrated approach may be utilized to address gaps of knowledge are provided.
Keywords
Biobehavioral research in nursing focuses on the interactions among biological factors, behavioral factors, and outcomes associated with critical health experiences (McCain, Gray, Walter, & Robins, 2005). This framework brings together a number of factors and integrates them into a cohesive, more holistic model for addressing questions of importance to nursing. Biobehavioral models integrate both theoretical and empirical knowledge of psychobehavioral and physiological patterns that contribute to health outcomes. Although biobehavioral methods have become increasingly sophisticated over the past few years, research in nursing focused on genetics generally has not been well integrated into a larger biobehavioral framework. However, genomic-based research is well suited to and perhaps can be more rapidly advanced in the context of research programs with a biobehavioral focus (Conley & Tinkle, 2007).
Biological or behavioral approaches have often been independently used to examine health and illness with few frameworks incorporating both. One of the most widely used and comprehensive biobehavioral models, psychoneuroimmunology (PNI), postulates multidimensional interactions among psychosocial factors and physiological mechanisms of the neuroendocrine and immune systems. For example, the stress response involves both direct and indirect effects on the immune system such that numerous cytokines and other biochemicals such as endogenous opioids are elaborated by cells of the immune system (McCain et al., 2005; for a comprehensive review see Ader, 2007). With a few notable exceptions (e.g., the epigenetics and stress management studies of Witek-Janusek & Mathews [MPI]: R01 CA1125455 & R01 CA 134736), the multifactorial interactions of genomics and epigenetics even within the PNI paradigm have been largely overlooked to date. Herein we propose a comprehensive biobehavioral model that includes genomic factors.
There are several ways in which genomic factors may be included within a general model of biobehavioral nursing research: the evaluation of genotypes that may predispose an individual to certain conditions; gene expression or protein expression as biomarkers of direct or indirect influence on outcomes; and genotype, gene expression, or protein expression as measures of neuroendocrine or immunological function. Genomic factors may also be considered as biobehavioral cofactors, moderators (which may indirectly influence outcomes), mediators (which directly influence outcomes), or biomarkers of neuroendocrine or immunological function depending on the context of the investigation (Kraemer, Stice, Kazdin, Offord, & Kupfer, 2001).
The biobehavioral framework illustrated in Figure 1 represents a general biobehavioral model adapted from the ongoing work in the Center for Biobehavioral Clinical Research at Virginia Commonwealth University School of Nursing (P20 NR008988, McCain; P30 NR011403, Pickler). The general biobehavioral model includes antecedent biobehavioral cofactors that interact with moderators and mediators that influence neuroendocrine and immunological function. A biobehavioral conceptual model incorporating genomics allows the broadest view for incorporating the most recent biological scientific advances and behavioral approaches that have been a mainstay in nursing research. In this article, we describe the initial development of a biobehavioral liver transplantation research model that incorporates genomics. We discuss several salient pre- and posttransplantation issues to illustrate how an integrated biobehavioral model can enhance comprehensive research and integrative knowledge development in transplantation nursing science. This integrated biobehavioral model can be used to target the current gaps in scientific knowledge in this population, addressing the needs of transplant patients and improving their quality of life.
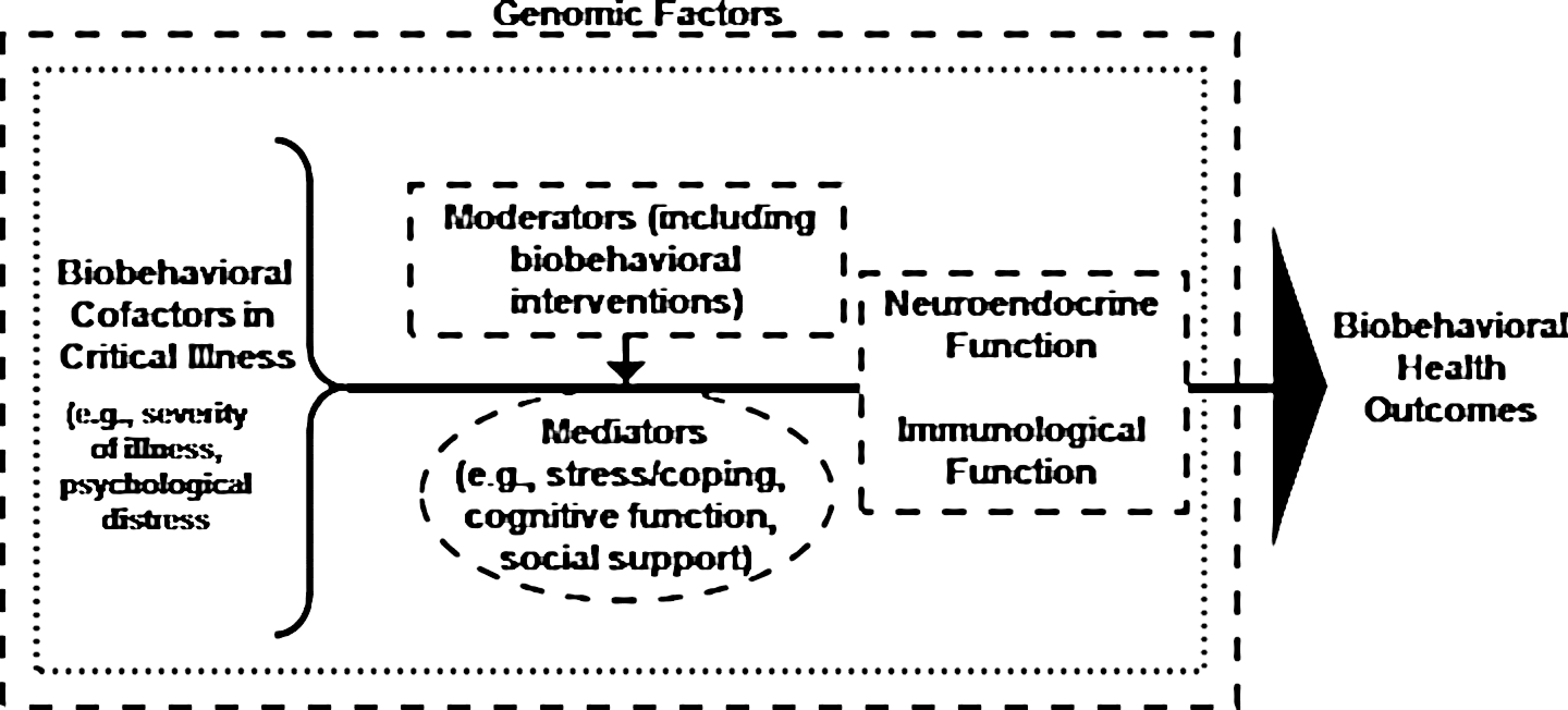
General biobehavioral model of nursing research. Critical illness has biobehavioral cofactors, such as illness severity, genomic factors, or psychological distress. There may also be moderators and/or mediators that affect the trajectory of the illness as well as neuroendocrine and immunological function. The small dotted line around the biobehavioral cofactors, moderators, mediators, and neurological and immunological function indicates that the interactions of these factors can have an impact on biobehavioral health outcomes. The larger dotted line represents the broader view of including genomics in the factors affecting biobehavioral health outcomes.
Biobehavioral Research in Transplantation
An increasing number of people undergo liver transplantation for a wide variety of conditions. Advances in surgical and immunosuppression techniques have contributed to improved long-term outcomes (Scherer et al., 2007). Research related to immunosuppression, immune tolerance, and rejection is a significant focus in this population, with an emphasis on identification of recipients at risk for rejection or common complications associated with immunosuppression (Bathgate et al., 2000; Brouard, Ashton-Chess, & Soulillou, 2008; Drent, Moons, De Geest, Kleibeuker, & Haagsma, 2008; Goddard et al., 2001). Other important pretransplantation concerns include biobehavioral cofactors that represent antecedent factors; general factors such as demographics, physical activity, and nutrition; and clinical factors including underlying conditions such as hepatitis C (HCV) or the presence of a genetic liver disease such as α-1-antitrypsin deficiency.
Although enhancing health outcomes in transplant recipients is an emerging focus, few studies have examined these issues in the liver transplant population using a biobehavioral framework. Therefore, we developed a biobehavioral framework incorporating genomic factors in a liver transplant population (Figure 2 ). The framework includes pretransplantation biobehavioral cofactors, moderators, and mediators; their multifactorial interactions; and biobehavioral health outcomes. Genomic factors are included throughout the model.
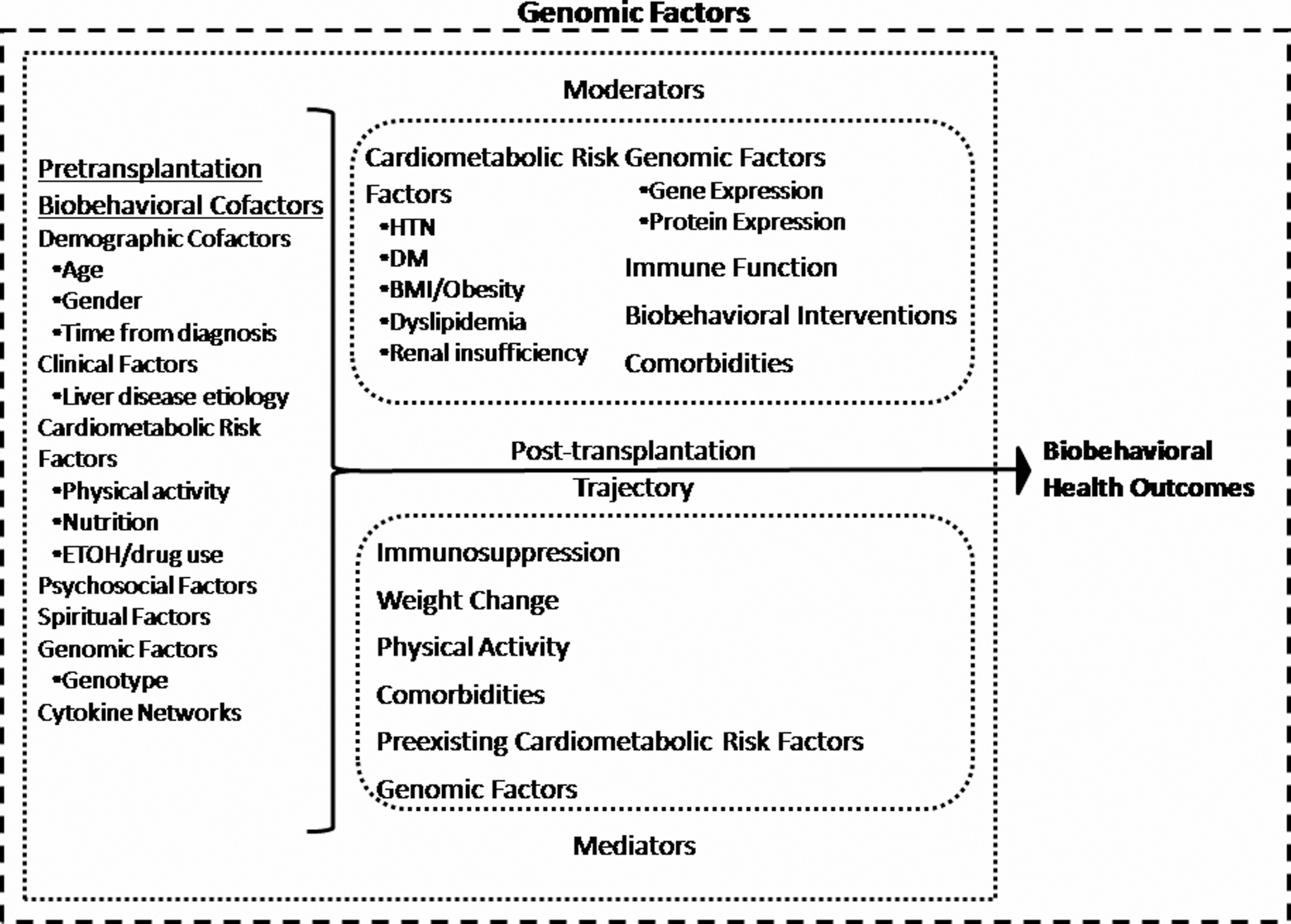
Biobehavioral model of nursing research incorporating genomics in a transplantation population. Pretransplantation biobehavioral cofactors interact with moderators and mediators across the posttransplantation trajectory. The interaction of these factors, which is represented by the smaller dotted line surrounding them, has an impact on biobehavioral health outcomes after transplantation. The larger dotted line surrounding pre- and posttransplantation factors and biobehavioral health outcomes indicates that genomic factors are integrated throughout all aspects of the model. BMI = body mass index; DM = diabetes mellitus; ETOH = alcohol; HTN = hypertension.
Moderators and mediators after transplantation can be challenging to define, given the current state of the science. For example, the presence of depression as a comorbidity may be defined as a moderator (perhaps affecting an individual’s ability to participate in activities that contribute to health promotion and disease prevention) or a mediator (if conceptualized as having an underlying inflammatory component affecting health outcomes). Immunosuppressive medications used to prevent rejection after transplantation are examples of mediators. Certain p450 genotypes may affect the metabolism of certain immunosuppressants and protect from or contribute to the risk of comorbidities. Gene expression as a marker of new-onset diabetes after transplantation (NODM) may be viewed as a moderator for the development of other biobehavioral outcomes including dyslipidemia and hypertension. In the following examples, we discuss the incorporation of genomic approaches into a biobehavioral framework by examining several important clinical problems in the liver transplantation population prior to and after transplantation.
Pretransplantation Concerns: Hepatocellular Carcinoma
In the liver transplant population, hepatocellular carcinoma is an important pretransplantation cofactor. Hepatocellular carcinoma is associated with poor survival rates because it is often identified at advanced stages, thus prohibiting liver transplantation as an option. However, if identified at earlier stages, liver transplantation is considered a good treatment option for hepatocellular carcinoma. Individuals with early-stage hepatocellular carcinomas have received priority for liver transplantation in the United States (Ioannou, Perkins, & Carithers, 2008) and have a good long-term prognosis after transplantation. However, current screening modalities lack sensitivity and specificity for early diagnosis of hepatocellular carcinoma (Mas et al., 2009).
Molecular techniques have been widely used to gain a greater understanding of the process of malignancy and metastasis (Chu, Holm, Byrnes, & Li, 2008). Researchers have identified discrepancies between genomic and proteomic regulation, highlighting the importance of examining this area for a greater understanding of the role of protein expression in malignancy and metastasis (Barginear, Bradley, Shapira, & Budman, 2008). Using proteomic approaches, a recent study identified potential biomarkers of hepatocellular carcinoma in the blood of patients positive for HCV with cirrhosis who were awaiting liver transplantation (Mas et al., 2009). Investigators compared protein expression in plasma between patients with HCV cirrhosis alone or HCV cirrhosis with hepatocellular carcinoma and were able to identify a subset of proteins that correlated with the presence of hepatocellular carcinoma. In addition, they identified a different subset of proteins that differentiated early-stage from advanced-stage hepatocellular carcinoma.
In the context of translation to practice, these protein subsets may aid in the identification of select candidates, such as those with smaller tumor size and no extrahepatic spread, who can benefit from liver transplantation. Ongoing research in this area focuses on identification of prognostic biomarkers that may be used for earlier diagnosis of hepatocellular carcinoma (Mas et al., 2009). However, application of these proteomic techniques to posttransplantation surveillance for recurrence of hepatocellular carcinoma has not yet been addressed. Current genetic research in hepatocellular carcinoma is focused on the identification of biomarkers of disease. Additional understanding of biobehavioral factors may help to identify possible biobehavioral strategies to reduce the risk of hepatocellular carcinoma development or to enhance early detection, thereby improving survival in this population.
Early Posttransplantation Outcomes: Rejection, Graft Loss, and Pharmacogenomics
A majority of liver transplantation studies incorporating genetics have focused on outcomes related to rejection, graft loss, and pharmacogenomics (Brouard et al., 2008). Polymorphisms of the tumor necrosis factor-α gene (Bathgate et al., 2000; Fernandes et al., 2002) have been linked with acute rejection. Other polymorphisms have been associated with the amount of immunosuppression required after transplantation (CYP3A5; Fukudo et al., 2008) or poorer long-term graft outcomes (SDF1 [now CXCL12]; Schröppel et al., 2002 and CTLA-4; Marder et al., 2003). Interestingly, certain polymorphisms in CTLA-4 have been associated with better graft survival, while other polymorphisms in this same gene were associated with worse graft survival (Marder et al., 2003).
A recent study examined polymorphisms in certain p450 genes that are involved in metabolizing calcineurin inhibitors, a class of immunosuppressants widely used after transplantation and associated with nephrotoxicity (Smith et al., 2008). Renal dysfunction after liver transplantation is common, with approximately 80% of recipients developing some degree of chronic renal insufficiency within 5 years after transplantation (Sethi & Stravitz, 2007). Cytochromes p450 2C8 and 2J2 are expressed in the kidney and involved in the metabolism of vasoprotective metabolites that help maintain blood pressure homeostasis and vascular smooth muscle tone. It is hypothesized that decreased production of these vasoprotective metabolites increases the risk of the development of renal dysfunction in the presence of calcineurin inhibitors. Smith and colleagues (2008) described a specific genotype polymorphism that increased the risk of nephrotoxicity 3 or more years after liver transplantation. The risk of nephrotoxicity was further increased when one of the two primary calcineurin inhibitors was used as the primary immunosuppressant medication. Interestingly, a genotype that conferred protection from nephrotoxicity was also identified. The study thus documents a gene−environment interaction between a specific cytochrome P450 polymorphism and the use of calcineurin inhibitors after liver transplantation that increases the risk of posttransplantation nephrotoxicity.
In the future, pretransplantation evaluation for this polymorphism may become useful in developing a posttransplantation plan of care that minimizes the risk of nephrotoxicity. The plan may include avoidance of certain immunosuppressant medications that increase nephrotoxicity risk and may also include biobehavioral modifications, such as diet and exercise, to reduce the impact of other factors, such as hypertension, known to increase nephrotoxicity.
Posttransplantation Comorbidities: Diabetes
Investigating factors that are detrimental to posttransplantation health outcomes is an emerging area of interest in nursing research. Biobehavioral outcomes may include other common comorbidities associated with liver transplantation such as NODM, hypertension, dyslipidemia, and chronic renal insufficiency. These comorbidities can lead to decreased survival and diminished quality of life (Sethi & Stravitz, 2007).
More recently, investigation has focused on NODM. Changes in patterns of gene expression across the entire genome have been identified in liver transplant recipients who developed NODM (Driscoll et al., 2006), a diagnosis which is clearly associated with poorer long-term outcomes posttransplantation. The biologic basis for this comorbidity, which is most likely multifactorial, has not been well described. Evaluation of whole-genome expression is an initial step in gaining a greater understanding of the development of, and an individual’s response to, NODM. Over time, this information may be beneficial in earlier identification of NODM or identification of persons at risk of this complication so that appropriate biobehavioral interventions can be applied to reduce or perhaps prevent the occurrence. The biobehavioral model can be used as a framework for addressing this question.
Previous studies have identified antecedent factors that may contribute to the risk of developing NODM (Driscoll, 2007), including age, ethnicity, weight, and family history of diabetes. In addition, underlying diseases such as alcoholic liver disease or HCV have also been linked with increased risk of NODM. In the study mentioned above, the gene expression profiles that represent NODM are an example of how genomic factors may be incorporated as markers for biobehavioral outcomes. This information may provide clues related to significant morbidity, mortality, and quality-of-life outcomes (see Figure 2).
Behavioral Factors: Pre- and Posttransplantation
In addition to the biological focus mentioned above, other investigations have focused on behavioral factors in transplantation populations. Behavioral factors such as physical activity, nutrition, and smoking can also be considered as pretransplantation critical cofactors as well as moderators and mediators during the posttransplantation trajectory. Medication adherence is one behavioral factor that researchers have examined in selected renal or adolescent transplant-recipient populations. These studies report increased nonadherence among adolescent recipients and increased risk of graft loss with nonadherence for both populations (Pinsky et al., 2009). Among the few medication adherence studies in the liver transplant population, decreased adherence was associated with poorer long-term outcomes (O’Carroll, McGregor, Swanson, Masterton, & Hayes, 2006). An additional study examined medication adherence within the context of quality of life, and investigators reported no association between decreased quality of life, symptom experience, and medication adherence (Drent et al., 2008). However, few studies have focused on medication adherence and included genomics within the context of a biobehavioral approach.
Another important transplantation research focus involves health-promoting behaviors. The negative consequences of certain factors such as smoking or obesity on transplantation outcomes have been documented (Dick et al., 2009; van der Heide, Dijkstra, Porte, Kleibeuker, & Haagsma, 2009). When compared with age- and gender-matched controls, liver transplant recipients are at greater risk of cardiovascular and cerebrovascular events and bone disease (Mells & Neuberger, 2009). Lifestyle modification is often suggested as an intervention to address these complications (Guckelberger, 2009). In one randomized control trial, investigators evaluated an exercise and dietary counseling intervention in liver transplant recipients and reported improved exercise capacity and body composition in the intervention group. However, no additional clinical outcomes data, such as hypertension or dyslipidemia status, were provided (Krasnoff et al., 2006). Yet the role of immunosuppression related to the development of some common posttransplantation complications such as hypertension must be considered. Hypertension in transplant patients is a consequence of the renal arteriolar constriction associated with calcineurin inhibition from the primary class of immunosuppressants used posttransplantation (Charlton, 2009). Few studies have examined the complex interplay of biobehavioral and genomic factors relative to these common complications after liver transplantation.
Conclusion
In this article, we have presented an overview of the biobehavioral paradigm with several examples of how to integrate genomic variables into an expanded biobehavioral framework of liver transplantation. Similar to previous biobehavioral frameworks, such as PNI, this model targets the intersection of biological and behavioral components with the addition of genomic factors throughout the model. Because many of the genomic and proteomic technological advancements are recent, there are numerous opportunities for exploratory and hypothesis-driven biobehavioral research projects incorporating genomics in the field of transplantation. The exemplars above provide only a glimpse of how genomic methods have been used in transplantation research and one can readily see how this is an area primed for future growth. Viewing genomics as a methodology within a biobehavioral framework, rather than as a stand-alone program of research, makes it easier to envision the advancement of a wide variety of programs of research that can enhance the health and well-being of transplant recipients.
Footnotes
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: P20 NR008988; McCain, Center for Biobehavioral and Clinical Research, VCU School of Nursing. P30 NR011403; Pickler, Center of Excellence for Biobehavioral Approaches to Symptom Management, VCU School of Nursing. Driscoll, C. J., Stability of blood gene expression in new onset diabetes after liver transplant, a pilot study funded by award P20 NR008988 (McCain, PI), National Institute of Nursing Research, NIH; Pilot Study PI, 2008-2009.