
Abstract
Maternal epidural analgesia is an increasingly common method of labor pain management (Declercq, Sakala, Corry, & Applebaum, 2006); yet, findings about its influence on the fetal stress response at birth have been few and inconsistent (Miller, Fisk, Modi, & Glover, 2005; Vogl et al., 2006). A surge in the fetal stress response at birth supports rapid newborn adaptation and may facilitate the initiation of alertness, feeding, and mother–infant interaction.
Fetal cortisol production is very low in early gestation, but a unique feed-forward system regulates the placental–fetal hypothalamic–pituitary–adrenal (HPA) axis resulting in a dramatic rise of fetal cortisol near term (Mesiano & Jaffe, 1997). Women also demonstrate tripling of plasma cortisol near term as a result of the rise in plasma corticotropin-releasing hormone (CRH), the fall in plasma CRH-binding globulin and cortisol-binding globulin, and resetting of CRH and adrenocorticotropin hormone receptor sensitivity, as pregnancy progresses (Mastorakos & Ilias, 2003). These high maternal/fetal cortisol levels are stimulated even further by the stress of normal labor and birth in response to the activation of maternal/fetal sympathetic–adrenal–medullar (SAM) and HPA axes (Miller et al., 2005; Vogl et al., 2006). This acute stress supports rapid newborn adaptation to birth in multiple systems through the surge of cortisol that becomes available to fetal tissue (Lagercrantz & Slotkin, 1986; Ramachandrappa & Jain, 2008). In adults and animals, acute stress-induced activation of SAM–HPA axes results in increased alertness and arousal (McEwen, 2007). In neonates, it is postulated that, as in adults, activation is related to increased infant alertness soon after birth (Desmond et al., 1963). Increased alertness is important in facilitating mother–infant social interaction (Feldman & Eidelman, 2006) and feeding behaviors (Medoff-Cooper & Ratcliffe, 2005; Pickler, Best, & Crosson, 2009; Walters, Boggs, Ludington-Hoe, Price, & Morrison, 2007). Yet, as far as we know, the relationship between fetal stress and newborn alertness has remained uninvestigated.
UA cortisol level is a marker of fetal HPA activation (Gitau, Menson, et al., 2001). UA cortisol levels are known to be high at the time of birth and to then rapidly decline (Lao & Panesar, 1989; Mears, McAuliffe, Grimes, & Morrison, 2004; Miller et al., 2005). A diurnal pattern of cortisol does not become evident until 8–12 weeks postbirth in term infants (Antonini, Jorge, & Moreira, 2000). Evidence clearly demonstrates that maternal cortisol levels decrease with epidural analgesia (Alehagen, Wijma, Lundberg, & Wijma, 2005; Miller et al., 2005; Vogl et al., 2006); however, study results differ with regard to whether epidural-induced decrease in maternal cortisol influences fetal cortisol level (Chan et al., 1993; Mears et al., 2004). While we know that the fetus can mount an independent HPA-axis response to stress (Gitau, Fisk, Teixeira, Cameron, & Glover, 2001), there is a gap in the literature as to how much variance is shared by maternal and UA cortisol levels at birth.
In this exploratory pilot study, we investigated relationships between (a) exposure to epidural analgesia and maternal and UA cortisol, (b) maternal and UA cortisol levels at birth, and (c) UA cortisol levels and infant alertness after birth.
Method
Participants
We conducted the study at an inner-city community hospital in the United States. After securing Institutional Review Board approval, we informed women about the study during their antepartum or early intrapartum care at the study site, obtaining a convenience sample between September 2007 and April 2008. After informed consent (conducted in English or Spanish), women self-selected to labor without any type of pain medication (the unmedicated group) or with epidural analgesia. The standardized epidural continual infusion mixture was 0.125% bupivicaine and 2 mcg/ml fentanyl. Women were eligible if they were ≥ 18 years of age and healthy, spoke English or Spanish, and were 37–42 weeks pregnant and expecting a vaginal birth. Women were excluded if they had depressive symptoms, either by self-report or medical chart review; a history in the current pregnancy of hypertension, gestational diabetes, endocrine or autonomic disorders, or illicit drug use; or a current infection with temperature > 100.4 F. Infants were eligible if they were full term, had no fetal distress, scored ≥ 7 on the APGAR, had a birth weight ≥ 2,500 g, were born cephalic without forceps or vacuum extraction, were healthy, and had no observable chromosomal abnormalities. Participants comprised 40 low-risk mothers and infants (n = 15 unmedicated, n = 25 epidural).
Maternal Cortisol Enzyme Immunoassay
We collected maternal saliva 11–16 min after birth. To counteract the mother’s dry mouth at birth, we stimulated salivary flow by having them chew on sugar- and citrus-free gum for 60 s. Previous investigators have shown that this procedure has no effect on the reliability of cortisol levels (r > .95 for rank ordering; Talge, Donzella, Kryzer, Gierens, & Gunnar, 2005). Participants then chewed on a Salivette® (Sarstedt, Germany) cotton wad for 60 s. We returned the cotton to the Salivette tube, placed it on ice, and stored it at –80 °C. We later thawed and centrifuged the samples to obtain a clean salivary sample and then froze them again until we assayed them all in one batch.
We measured salivary cortisol using an enzyme immunoassay (EIA) kit (Diagnostic Systems Laboratories, Webster, TX). We visualized the bound enzyme-linked portion of cortisol using a microtiter plate reader (SpectraMax 190, Molecular Devices, Sunnyvale, CA) at 405 nm absorbance after reaction with a chromagen. The EIA is highly sensitive with a minimum detection limit of 0.072 µg/dl and low antibody cross-reactivity with other steroids. Detection range was 0–10 µg/dl. Salivary samples required a 20-fold dilution (with zero standard) to fall within the kit’s standard curve. We thus multiplied results by 20 to obtain the final cortisol concentration. As a positive control, we measured nondiluted saliva from nonpregnant women of childbearing age in parallel with the diluted samples from participants, and cortisol concentrations from control women fell within the EIA standard curve. In addition, 2- and 10-fold diluted samples from women of childbearing age yielded predicted salivary cortisol values. Intra- and interassay coefficients of variation of the assay at the Core Biologic Research Laboratory at the University of Illinois at Chicago, College of Nursing, was 6.2% ± 5.4% (n = 4) and 5.3% ± 0.4% (n = 5), respectively. Pearson’s correlation coefficient was high between the EIA and radioimmunoassay from the same company (r = 0.99, p = .01, n = 5).
UA Cortisol EIA
UA blood was preferable in the present study to venous cord blood, as arterial blood should represent predominantly a fetal versus maternal source (Gitau et al., 2001). To obtain the sample, the birth attendant clamped and cut a section of cord (usually within the first minute after birth). The investigator, trained in collecting cord blood samples, used a heparinized 1 ml syringe to collect an arterial sample and avoid coagulation. The investigator centrifuged samples at the bedside and saved the resultant 10–100 μl plasma fraction, which we stored at –80 °C.
We measured UA cortisol concentration using a modification of the Active® Cortisol EIA from Diagnostics Systems Laboratory, Inc. (DSL-10-2000; Webster, TX), at the Core Biological Laboratory at the College of Nursing, University of Illinois at Chicago. We ran all samples in duplicate. Preliminary studies revealed that the cortisol concentration from pooled UA plasma was above the upper limit of the standard curve. Therefore, we diluted samples 5-fold using a zero standard from Diagnostic System Laboratory’s cortisol radioimmunoassay kit (DSL-2100-5), such that cortisol levels fell within the center third of the standard curve. To validate that the dilutions produced predicted values, we diluted a pooled plasma sample 2-, 4-, and 8-fold. Results correlated strongly with predicted values (Pearson’s correlation coefficient; r = .99). In addition, the 20 ug/dl standard supplied with the EIA kit diluted 4-fold produced a value of 5.4 ug/ dl when assayed. Intra-assay coefficient of variation was 3.2%.
Infant Alertness
We defined the variable of interest, frequency of alertness, as the proportion of time spent in an alert state (i.e., eyes open, bright, and possibly scanning the environment) during a 9-min period. We used a condensed version of Thoman’s behavioral scale to code five behavioral states: sleep, sleep–wake transition, drowsy, alert, and non-alert waking activity (1990). We video recorded infants for 15 min beginning at 45 min after birth (5 min before, during, and after the initial feeding). See the article by Bell, White-Traut, and Medoff-Cooper (2010) for additional description of the method. To exclude influence from spitting-up episodes on behavioral states, we analyzed only the first 4 min after feeding along with the 5 min before feeding, resulting in a 9-min analysis period. The investigator (AB) and a research assistant (who was blinded to epidural exposure) separately coded all video recordings. During each 10-s epoch, observers coded the predominant behavioral state the infant exhibited. During training, we initially established intra- and interrater reliability at ≥ 90%. Thereafter, we maintained an average of 87% interrater agreement. Both raters simultaneously viewed cases for which there was < 87% agreement to discuss the differences and agree on a final rating.
Covariates
Potential covariates that may affect cortisol include race/ethnicity, duration of labor, and maternal perceived stress and depression. We characterized race/ethnicity as either Latino or Black in 37 mothers and 36 infants and as “Other” in 3 mothers and 4 infants (two non-Latino White mother–infant dyads, one Asian dyad, and one biracial infant). Since there is no gold standard of how to assess the beginning of active labor, we used the standard clinical assessment of progressive cervical change beginning at 4 cm. If women presented in labor beyond 4 cm, we calculated duration of labor as beginning when mothers reported the initiation of strong contractions less than 5 min apart. The following day after birth, women completed two questionnaires to measure recent stress and depression: the Perceived Stress Scale (Cohen, Kamarck, & Mermelstein, 1983) to measure perceived stress in the last month of pregnancy and the Edinburgh Postnatal Depression Scale (Cox, Holden, & Sagovsky, 1987) to measure depressive symptoms in the last 7 days of pregnancy. Researchers have shown that the 10-item Perceived Stress Scale correlates with patterns of change in cortisol levels throughout the day (Edwards, Hucklebridge, Clow, & Evans, 2003) and that the 10-item Edinburgh Postnatal Depression Scale correlates with infant cortisol levels and ability to orient in the first 24 hr after birth (Lundy et al., 1999).
Procedures
We obtained samples of maternal saliva and UA cord blood at birth and stored them for later processing using an immunoassay method. Nursing staff preference was for infants to be placed in a warmer for approximately 20 min before being swaddled and held by the mother. At 40 min after birth, infants rested undisturbed for 5 min in a portable crib in the mother’s room. In low lighting, we video recorded infants for 15 min. In the middle of video recording, we bottle fed infants for 5 min with minimal interaction. Nursing staff postponed routine injections and application of ophthalmic ointment until the data collection session ended.
Statistical Analysis
We performed statistical analyses (on 40 mothers and 40 infants) using Statistical Package for the Social Sciences (SPSS) version 17 (Chicago, IL). We considered an alpha of <.05 to be significant. We summarized demographic and outcome variables using descriptive statistics (mean, standard deviations, and frequency) and compared them between unmedicated and epidural groups. Univariate analysis included t test and Pearson correlation for continuous variables and chi-square test and Spearman correlation for categorical variables. We conducted multivariate analysis, controlling for appropriate covariates, using the generalized linear model (GLM) on three primary outcome variables: infant alertness, maternal salivary, and UA cortisol. We acquired a logarithmic 10 transformation for salivary and UA cortisol due to the skewness of data. Pitocin® was not a significant factor in any outcome analysis.
Results
Table 1 shows maternal and infant demographic characteristics, as well as outcome variables. There were more Latina women in the unmedicated group and more Black women in the epidural group. Duration of first stage of labor was significantly longer in the epidural (10 hr 55 min) versus unmedicated (8 hr 21 min) group. No other descriptive variables were significantly different between the two groups. For women who received epidural analgesia, the mean total dosage of bupivicaine was 99 mg (SD 65, range 13–234) and mean total dosage of fentanyl was 162 mcg (SD 104, range 21–374).
Demographic Characteristics of Study Participants and Outcome Variables
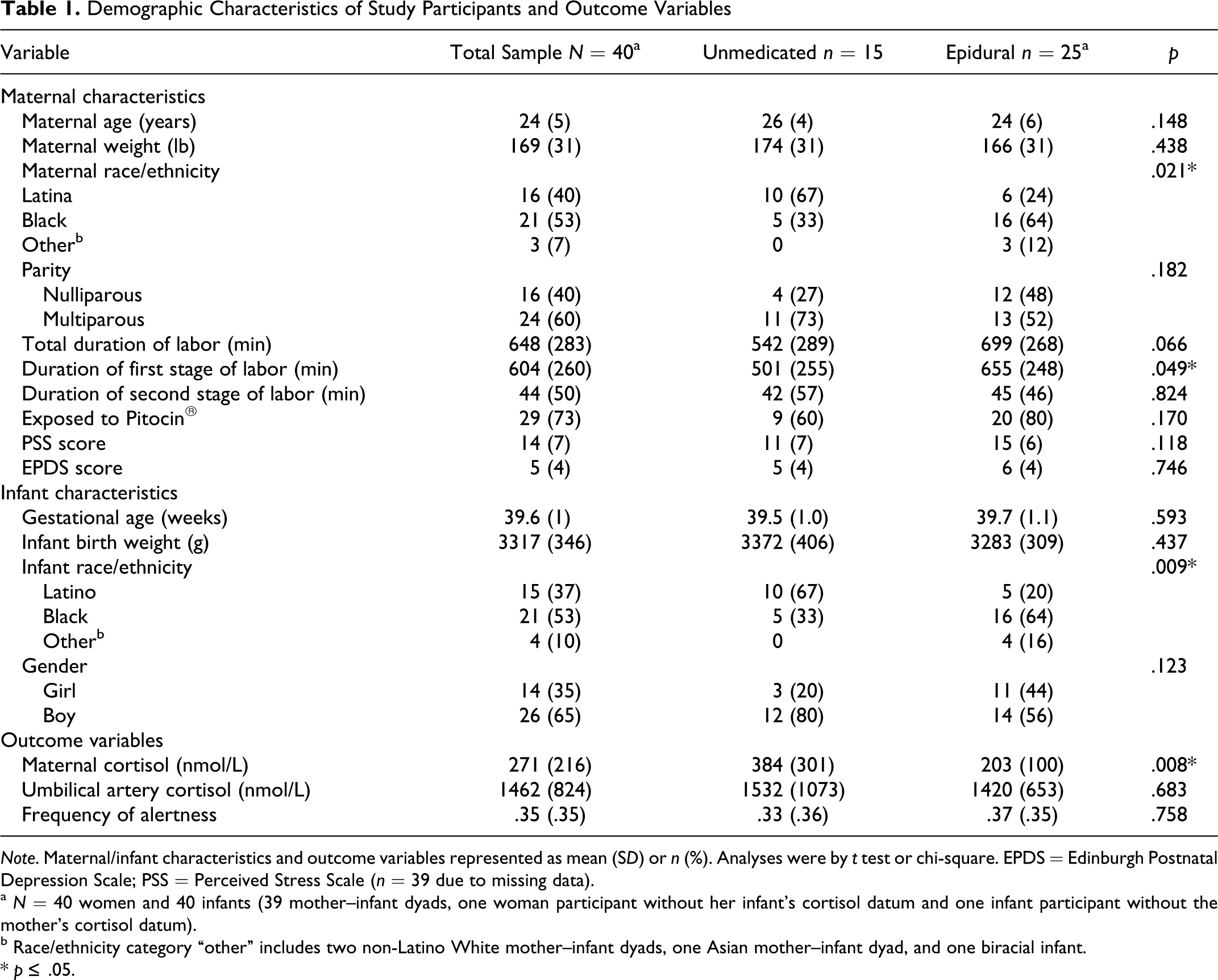
Note. Maternal/infant characteristics and outcome variables represented as mean (SD) or n (%). Analyses were by t test or chi-square. EPDS = Edinburgh Postnatal Depression Scale; PSS = Perceived Stress Scale (n = 39 due to missing data).
a N = 40 women and 40 infants (39 mother–infant dyads, one woman participant without her infant’s cortisol datum and one infant participant without the mother’s cortisol datum).
b Race/ethnicity category “other” includes two non-Latino White mother–infant dyads, one Asian mother–infant dyad, and one biracial infant.
* p ≤ .05.
Maternal cortisol was significantly higher in the unmedicated group as compared to the epidural group. In the unmedicated group, maternal cortisol significantly increased, as duration of second stage labor increased (rp = .58, p = .024), while in the epidural group there was no significant difference associated with duration of the second stage (rp = .21, p = .316). Across the entire sample, maternal cortisol did not correlate with duration of labor. Maternal cortisol was not related to scores on the Perceived Stress Scale (rp = .00, p = .996) or the Edinburgh Postnatal Depression Scale (rp = −.11, p = .483). There was no difference in UA cortisol or infant alertness between the unmedicated and epidural groups. For the entire sample, UA cortisol was significantly related to duration of the first (rp = .34, p = .032) and second stages of labor (rp = .49, p = .001) and of total labor (rp = .39, p = .023).
Maternal and UA cortisol were highly correlated in the unmedicated group (rp = .74, p = .002) but not in the epidural group (rp = .06, p = .776). Maternal cortisol level explained 55% of the variance in UA cortisol in the unmedicated group (p = .002), but there was no significant shared variance in the epidural sample (p = .776). Overall, UA cortisol was positively associated with infant alertness in both groups, and the entire sample illustrated a significant correlation of .41 (p = .008) between UA cortisol and frequency of infant alertness. We observed no relationship between maternal cortisol and infant alertness.
Table 2 summarizes the results of multivariate analyses for three outcome variables: maternal salivary cortisol, UA cortisol, and frequency of alertness. In Model 1, epidural group (p = .003) was a significant predictor of maternal cortisol, but race/ethnicity (p = .083) and duration of labor (p = .080) were not. Although the interaction between race/ethnicity and epidural group was not statistically significant due to the small sample size, there was a trend that the difference in maternal cortisol level between Latina and Black women was larger in the unmedicated than in the epidural group (Figure 1 ).
General Linear Model Results for the Outcome Variables Maternal Cortisol, Umbilical Cortisol, and Frequency of Alertness
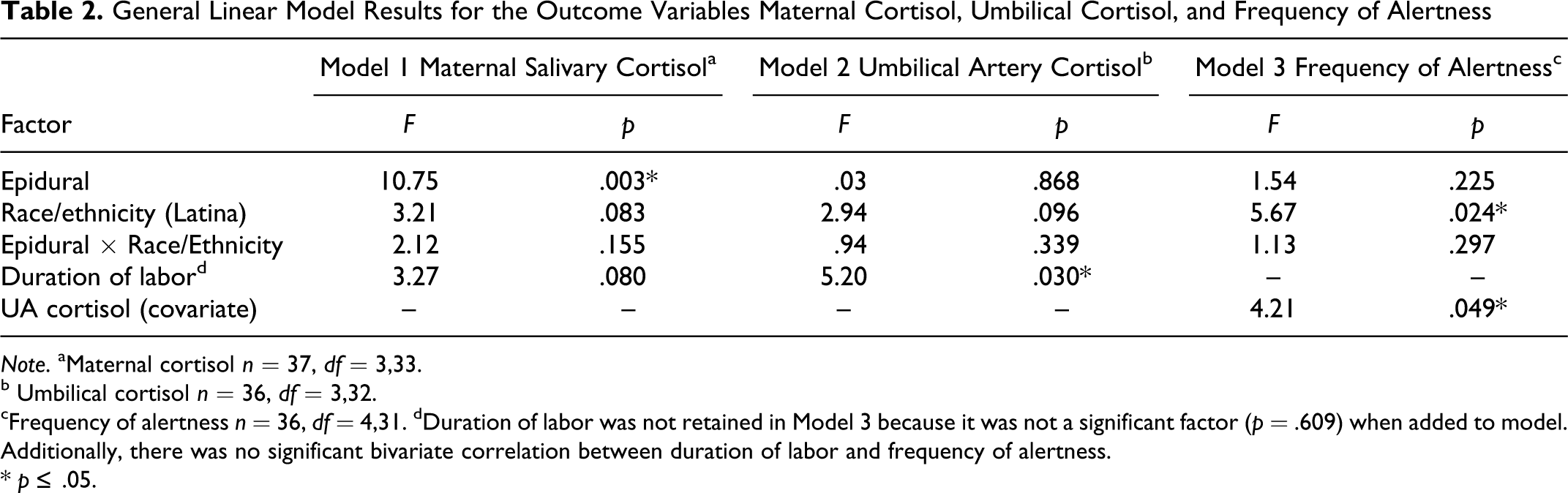
Note. aMaternal cortisol n = 37, df = 3,33.
b Umbilical cortisol n = 36, df = 3,32.
cFrequency of alertness n = 36, df = 4,31.
dDuration of labor was not retained in Model 3 because it was not a significant factor (p = .609) when added to model. Additionally, there was no significant bivariate correlation between duration of labor and frequency of alertness.
* p ≤ .05.
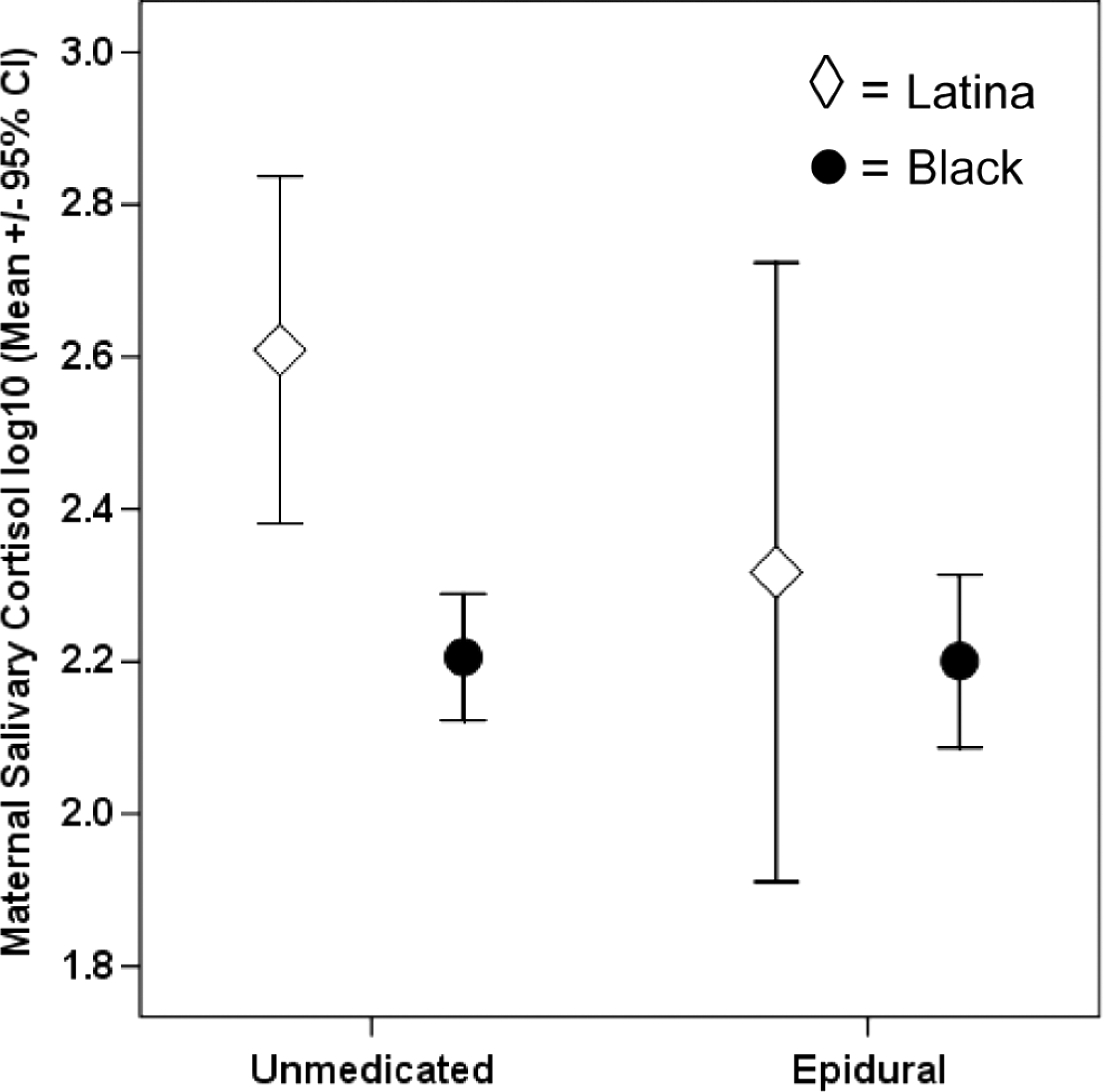
Maternal salivary cortisol (log10 mean ± 95% CI) by epidural exposure and race/ethnicity (n = 10 unmedicated Latina women, 5 unmedicated BLACK women, 6 epidural Latina women, and 16 epidural Black women).
In Model 2, neither epidural group (p = .868) nor race/ethnicity (p = .096) were significant predictors of UA cortisol. Duration of labor was a significant predictor of UA cortisol (p = .030), with longer labors resulting in higher UA cortisol. Post hoc power analysis revealed that this pilot study had 5% power to detect differences in UA cortisol by epidural group (adjusting for duration of labor). A sample size of 1,571 per group would be needed to detect a significant difference in UA cortisol by epidural group (adjusting for duration of labor) with 80% power.
In Model 3, epidural group (p = .225) was not a significant predictor of infant alertness. Latino infants exhibited a greater frequency of alertness than Black infants (p = .024), and there was no significant interaction between epidural group and race/ethnicity. UA cortisol was significantly related to alertness (p = .049), with higher UA cortisol resulting in a greater frequency of alertness.
Discussion
Our findings corroborate those of previous investigations in which women with epidural analgesia have lower cortisol levels at birth than unmedicated women (Alehagen et al., 2005; Miller et al., 2005; Vogl et al., 2006). Our finding of 55% shared variance in maternal/fetal cortisol levels in an unmedicated sample suggest that high levels of cortisol produced by unmedicated women during labor and birth contribute to high levels of fetal cortisol exposure, as demonstrated by high UA cortisol at birth. The limited evidence available in the literature on the relationship between maternal and fetal cortisol levels at birth is inconsistent due to differences in drug exposure and sampling techniques (Gitau, Fisk, et al., 2001; Lao & Panesar, 1989; Sippell, Becker, Versmold, Bidlingmaier, & Knorr, 1978). In this regard, it is a strength of our study that we measured UA cortisol as opposed to umbilical vein or mixed umbilical blood because, even though it is challenging to obtain, arterial blood more accurately represents fetal cortisol exposure.
We hypothesized that UA cortisol concentration would be higher in the unmedicated compared to the epidural group. Therefore, it may seem incongruent that we found no difference. However, an unavoidable limitation of our study was that we measured cortisol at a single time point, at birth, while in fact the fetus was exposed to maternal cortisol throughout labor and delivery. Total cortisol exposure (or area under the curve for fetal cortisol exposure) would be affected by both cortisol concentration and length of labor. Our results confirm that higher UA cortisol at birth was related to duration of labor. We also found that in the unmedicated group (but not the epidural group) maternal cortisol increased as duration of second stage labor increased. Miller, Fisk, Modi, and Glover’s (2005) finding of a strong association between UA cortisol and duration of second stage corroborates ours. In addition, we found that in the unmedicated group maternal cortisol explained over half the variance in UA cortisol, while there was no relationship between the variables in the epidural group. Given that all of these factors are contributing to fetal cortisol exposure, it is difficult to prove or disprove our original hypothesis using our single time point measurement. Examination of the effect of epidural medication on UA cortisol will require further investigation with a larger sample size and control of more variables.
A major finding of this investigation is that the most alert infants were those who had the highest UA cortisol levels at birth. Cortisol facilitates rapid metabolic adaptation to the stress of birth (Lagercrantz & Slotkin, 1986; Ramachandrappa & Jain, 2008). Infants exhibit a higher frequency of alertness in the first few hours after birth than at any other time in the neonatal period (Wolff, 1965). The literature describes the benefits of newborn alertness. For instance, alert newborns are more available for social interaction (Feldman & Eidelman, 2006), and aroused newborns (in both alert and non-alert waking activity) are able to seek and initiate breastfeeding (Walters et al., 2007). Yet, while there is strong evidence to support numerous benefits of the alert state during infancy (e.g., improved feeding outcomes [Pickler et al., 2009], optimal sucking behavior [Medoff-Cooper & Ratcliffe, 2005], and enhanced mother–infant interaction [Feldman & Eidelman, 2006]), there is little research documenting antecedents and consequences of increased infant alertness soon after birth. The characteristics of our sample included labor lengths that were not extreme (M = 10 hr 48 min, SD = 4 hr 43 min), thus the relationship between cortisol and alertness cannot be generalized to infants exposed to extremely long labors. Further biobehavioral nursing research is warranted on factors contributing to infant alertness soon after birth and subsequent benefits to the mother–infant dyad.
An interesting subfinding was that maternal cortisol appeared to be higher in Latina women than Black women; however, the unmedicated group contributed the most to this difference, as there was no difference in cortisol levels between Latina and Black women in the epidural group. This finding is of interest, as mounting evidence suggests racial/ethnic differences in HPA-axis function in women and adolescents (Cohen et al., 2006; DeSantis et al., 2007). While there are few reports of racial/ethnic differences in HPA-axis function during pregnancy, Glynn, Schetter, Chicz-DeMet, Hobel, and Sandman (2007) reported that throughout pregnancy Black women exhibit significantly lower cortisol levels than non-Latina White women, even when the authors adjusted for potential confounders. Additionally, Latino infants were more alert than Black infants. While exploring the effects of race/ethnicity was not an aim of this study, our findings support the need for further investigation of the effect of race/ethnicity and other sociodemographic antecedents on HPA-mediated newborn behaviors.
There are several limitations of our study. Sample size was small and the study underpowered to detect interactions. Although lighting was controlled, there was variability in the amount of auditory and tactile stimuli that infants received in the 40-min period between birth and video recording of behavioral states. Some variability was controlled by the nursing staff preference of having all infants in the warmer for approximately 20 min before being swaddled and held by the mother and by the study protocol that all infants rested undisturbed for 5 min before the start of video recording. As it is not feasible to randomize women into unmedicated or epidural groups, women in our study self-selected to labor with epidural analgesia or with no pain medication. This situation resulted in more Black women in the epidural group and more Latina women in the unmedicated group. While our method of identifying when active labor began was based on standard practice, identification of the start of active labor is not an exact science, thus it did introduce some variability (Neal et al., 2010).
Attempts to replicate these results should thus include a larger sample, control of potential stressors immediately after birth, additional measures of antenatal maternal cortisol and postnatal infant cortisol, and sociodemographic factors that influence maternal HPA function. Given that the literature suggests that a high frequency of alertness has many benefits to the mother–infant dyad, investigators should further study perturbations of infant alertness soon after birth, as these may also affect perinatal outcomes.
Conclusion
While epidural analgesia did not directly relate to level of infant cortisol, multiple factors contributed to higher UA cortisol at birth. High levels of cortisol produced by unmedicated women during labor and birth contributes to high UA cortisol at birth. In addition to a maternal influence on fetal HPA function, evidence of duration of labor influencing UA cortisol levels suggests there is fetal HPA independence, as maternal cortisol levels were generally not affected by this variable. Importantly, this is the first known study to examine and report that fetal cortisol at birth is related to infant alertness soon after birth. Increased alertness in the transitional newborn has important implications for facilitating mother–infant interaction, attachment, and establishment of early breastfeeding. Based on the known benefits of increased infant alertness (e.g., seeking and initiating breastfeeding, improved feeding and sucking outcomes, and mother–infant interaction) documented at times other than the immediate postbirth period (Feldman & Eidelman, 2006; Medoff-Cooper & Ratcliffe, 2005; Pickler et al., 2009; Walters et al., 2007), our report of a relationship between UA cortisol and newborn alertness warrants replication. Further examination of antecedents contributing to degree of fetal cortisol exposure and subsequent biobehavioral relationships between UA cortisol and newborn behavioral state will facilitate development of nursing interventions to improve emerging patterns of meaningful mother–infant behaviors. Our study results support a systems model, whereby activation of the fetal stress response at birth facilitates successful neonatal adaptation in the transition to extrauterine life.
Footnotes
Acknowledgments
The authors thank S. Porto, MD, D. Delves, CNM, and H. Pournajafi-Nazarloo, PhD, for their assistance.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research and/or authorship of this article: The author, AFB, discloses the following financial support: NIH/NINR F31 NR009912, Midwest Nursing Research Society/Council for the Advancement of Nursing Science Dissertation Grant, Harris Foundation Scholarship, and Mercy Hospital OB/GYN Education Fund, Chicago, USA.