
Abstract
Estimates suggest that 25–50% of family caregivers experience depression. Recent research has linked psychological stress and depression symptoms to increased cytokine activity. This study was designed to investigate the predictors of high cytokine levels and their influence with personality factors on depression in a caregiving population. The authors examined the relationship between caregiving burden and depression through the influence of sociotropy, autonomy, and cytokine levels in a sample of 106 caregivers who were actively caring for an elderly dependent in the community. Though the authors did not establish a mediation model, they found that the personality sub-factors of sociotropy, predicted tumor necrosis factor receptor (TNFR1) levels, while burden significantly predicted interleukin-6 and C-reactive protein (CRP) levels. Additionally, burden and TNFR1 levels predicted depression, with greater burden and TNFR1 levels predicting increased depression severity. Study findings point to a need for early interventions for caregivers to prevent increases in stress and cytokine levels and the development of depression.
Family caregivers save the health care system billions of dollars annually (Langa, Fultz, Saint, Kabeto, & Herzog, 2002). An estimated 17% of U.S. households are responsible for providing supportive care to a dependent or elder family member over 50 years of age (National Alliance for Caregiving [NAC] & American Association of Retired Persons [AARP], 2004), and the U.S. Bureau of the Census (2000) projects that the number of dependent elders in the U.S. will rise to 62 million by 2025. Unfortunately, caring for a family member does not come without personal cost. Estimates suggest that 25–50% of family caregivers develop symptoms of depression (Lu et al., 2007), a rate considerably higher than the 6.7% reported for the general population (Kessler, Chiu, Demler, & Walters, 2005).
Once caregivers develop depression, their ability to provide care is compromised and their own health is impaired (Deimling, Smerglia, & Schaefer, 2001). However, despite the large number of research studies that have investigated depression in the caregiving population and attempted to identify the factors that may put certain individuals at greater risk, there have been no consistent findings. Therefore, understanding the reasons for depression in the caregiving population, while also investigating why some caregivers develop stress yet avoid depression, is of great importance. Furthermore, developing a profile of caregivers who are more likely to become depressed as a result of their role will enable the creation of tailored interventions aimed at decreasing this risk.
One possible model to explain the individual differences in psychological outcomes related to caregiving may be Beck’s (1987) diathesis–stress model. The model includes two major personality factors, sociotropy and autonomy (Iacoviello, Grant, Alloy, & Abramson, 2009), and their associated dysfunctional assumptions that, along with an environmental stressor, place individuals at risk for depression (Sohlberg, Axelsson, Czartoryski, Stahlberg, & Strombom, 2006). According to Beck, dysfunctional assumptions are ideas individuals have that sustain their personality factors, sociotropy and autonomy. Previous research has provided no support for the role of dysfunctional assumptions in the development of depression in caregiving populations (Clark & Diamond, 2010). However, when facing a life stressor, particularly one that changes, challenges, or terminates personal relationships, individuals who are highly sociotropic are at an increased risk of depression (Sato & Gonzalez, 2009).This increased risk is due to the fact that highly sociotropic individuals value affection, approval, intimacy, and assistance from others. Conversely, individuals who are highly autonomic value self-reliance, mastery, and control and are at risk for depression when environmental events remove their sense of control over a situation (Bieling & Alden, 2001; Dasch, Cohen, Sahl, & Gunthert, 2008). Caregiving is an environmental stressor that would place individuals high on both of these personality factors at risk of depression, for the responsibilities involved in caregiving could (a) change the dynamic of close relationships and/or (b) reveal to the caregiver that they are not in control of the individual needing assistance (see Figure 1).
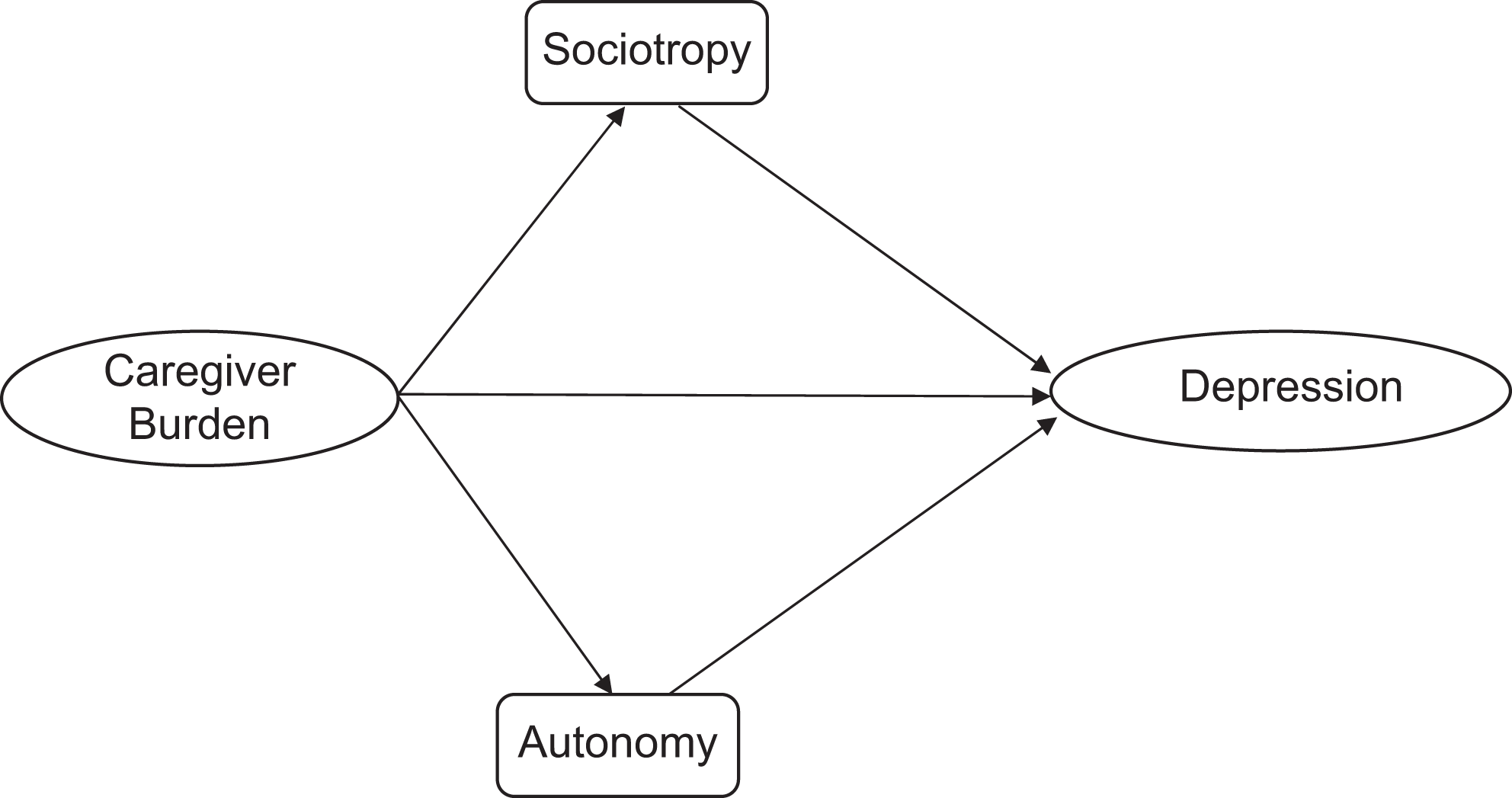
Beck’s diathesis–stress model for family caregivers, which demonstrates how burden influences the personality factors of sociotropy and autonomy, both of which are potential risk factors for depression.
In a previous study, we found that sociotropy and autonomy mediate the relationship between caregiver burden, a psychological stressor, and depression (Clark & Diamond, 2010). For that study, the concept of burden measured the psychological stress for the caregiving population. Those high on sociotropy or autonomy had a greater risk of developing depression when exposed to the psychological stress of caregiving than those who were not. This finding supports the diathesis–stress model, which states that the development of depression is triggered by the activation of dormant vulnerabilities (sociotropy and autonomy) by a stressor (caregiving burden; Husky, Mazure, Maciejewski, & Swendsen, 2007).
Past research has linked other personality factors to increased levels of stress reactivity (Schoofs, Hartmann, & Wolf 2008; Wirtz et al., 2007) and demonstrated that stress increases cytokine levels (Maes et al., 1998). Therefore, a possible mechanism by which those high in sociotropy and autonomy may be at an increased risk of developing depression is differences in cytokine levels. Kim and colleagues (2008) have linked psychological stress and depression symptoms to the inflammatory response system. Specifically, investigators have demonstrated that the pro-inflammatory cytokines tumor necrosis factor alpha (TNF-α), interleukin (IL)-6, IL1 receptor antagonist (IL1-ra), and C-reactive protein (CRP) have a potential role in the stress response as well as in pathophysiology of depression (Raison, Capuron, & Miller, 2006).
TNF-α plays a central role in the acute phase of the immune response and is responsible for many cellular processes including apoptosis, necrosis, cell survival, and inflammation (Keystone & Ware, 2010). TNF-α exerts its effects by binding to tumor necrosis factor receptor 1 (TNFR1) and TNFR2, which are also found in soluble form in the bloodstream as a response to receptor shedding. Investigators also believe that TNF-α plays a central role in the pathology of immune-mediated inflammatory diseases such as rheumatoid arthritis, psoriasis, and Crohn’s disease. TNF-α is also associated with depression. In a recent study, Grassi-Oliveira et al. (2009) reported that patients with recurrent major depressive disorder had significantly higher concentrations of soluble TNFR1 compared to healthy controls. The investigators also found TNFR1 levels (a common marker of TNF-α) to be associated with age, posttraumatic stress disorder-like symptoms, and depression severity.
Similarly, researchers have also linked IL-6 to depression. In an investigation of the effect of IL-6 on the hypothalamic–pituitary–adrenal (HPA) axis and depression, Jehn et al. (2010) found a significant difference in IL-6 plasma concentration between patients with depression and those without depression symptoms. This relationship was linear, with IL-6 concentrations increasing as the level of depressive mood increased. Capable of crossing the blood–brain barrier, IL-6 also acts to modulate neurotransmission and activate the HPA axis, the main pathway responsible for the body’s response to stress (Bremmer et al., 2008). Jehn et al. (2010) also found a relationship between circadian rhythms, which are controlled by the HPA axis, and plasma concentrations of IL-6. An increase in IL-6 concentration was significantly correlated with a flattening of cortisol levels across the day, evidence of disturbed HPA-axis functioning. This finding becomes significant when one considers the many research studies that have demonstrated the strong relationship between stress and depression (Robles, Glaser, & Kiecolt-Glaser, 2005).
IL-6 plays a major role in the activation of CRP (Kershaw, Mezuk, Abdou, Rafferty, & Jackson, 2010). Produced as a part of the acute-phase response, CRP triggers an inflammatory response and interacts with C1q to initiate the classical complement cascade (Du Clos & Mold, 2004). Investigators have implicated high levels of CRP in cardiovascular disease, myocardial infarction, and stroke, all conditions that are associated with higher than average rates of depression (Frasure-Smith & Lespérance, 2005; Kershaw et al., 2010). In fact, researchers have found CRP levels to be associated with depression in both healthy patients and those with coronary complications (Vaccarino et al., 2007). Panagiotakos et al. (2004) found that depressed participants had elevated CRP levels in a sample free of cardiovascular heart disease (CHD), and this association persisted when investigators controlled for confounding variables. Researchers have also linked a precursor to CRP, IL1-ra, to depression. In a recent meta-analysis Howren, Lamkin, and Suls (2009) found a significant association between levels of IL1-ra and depressive symptoms.
In addition to their potential role in the stress response as well as in the pathophysiology of depression, pro-inflammatory cytokine levels increase when individuals are exposed to acute or chronic psychological stressors (Raison et al., 2006; Steptoe, Hamer, & Chida, 2007). For example, Maes et al. (1998) measured stress perceptions and cytokine levels of students 1 month before and after their academic exams as well as the day before the exam. TNF-α, IL-6, and IL-1ra levels the day before the exam were significantly higher than those taken 1 month before and after the exam. Furthermore, those with higher stress perception levels the day before the exam had significantly higher cytokine levels than those who perceived their stress level a day before the exam as low. Thus the effect of stress on cytokine level appears to be dependent on the individual’s perception of the stress level. In addition, in a meta-analysis of psychological stress and cytokine research, Steptoe et al. (2007) found significant increases in circulating IL-6, TNF-α, and CRP levels following laboratory-induced psychological stress. Previous research studies (Chida & Hamer, 2008; Clark & Diamond, 2010; Schoofs et al., 2008; Wirtz et al., 2007) have also demonstrated that personality factors can influence how an individual perceives, experiences, and reacts to stress.
While we found no published research investigating the relationships between sociotropy and autonomy and the stress response, in the present study we hypothesized that, given research conducted on other personality traits, those high in sociotropy and autonomy might also have higher stress reactivity. When placed in a caregiving role, those high in sociotropy and autonomy might thus be more sensitive to the stress/burden of caregiving and thus have increased cytokine levels. These cytokine levels, as previous investigators have demonstrated (Grassi-Oliveira et al., 2009; Jehn et al., 2010), influence the individual’s risk of developing depression. Therefore, the overall objective of this study was to investigate the factors that might explain the high incidence of depression in the caregiving population. In line with this objective, our first aim was to investigate the predictors of high cytokine levels in a group of caregivers. Our second aim was to examine the relationship between caregiving burden and depression through the influence of sociotropy, autonomy, and cytokine levels.
Materials and Method
Setting and Sample
We recruited participants from the local senior clinic center, elders' day care center, and a geriatric outpatient clinic center in Las Vegas, Nevada, via posters and flyers. The sample consisted of 106 participants who were actively caring for an elderly dependent in the community for a minimum of 10 hr per week. We recruited this convenience sample through nonprobability sampling techniques. Individuals were excluded from the study if (a) they were unable to speak and read English, (b) they provided care for a dependent family member for less than 10 hr per week, or (c) their dependent care recipient was under 60 years of age. The institutional review board (IRB) approved all procedures and materials prior to the commencement of recruitment.
Procedure
Caregivers who showed an interest in participating in the study met the researchers, all of whom were registered nurses, during the dependent family member’s visit to the center. We explained the research study. If the caregiver met study criteria and agreed to participate, we obtained written informed consent. We collected a blood sample and then gave participants four questionnaires, including a demographic data sheet, to complete in the clinic waiting area. This recruitment process took place between August 2007 and March 2009. After participants completed the instruments, we reviewed their scores on the Center for Epidemiologic Studies Depression Index (CES-D). If a caregiver’s score demonstrated high symptomatology for depression, we referred them to community resources and suggested that they speak to a health practitioner.
Blood Analysis
We collected, labeled, and dated blood samples in 6 mL vacutainer specimen collection tubes (Becton Dickinson & Co. [BD]). We centrifuged (Fisher centrific centrifuge, San Diego, CA) the specimens for 15 min at 3300 rpm, having balanced all tubes with similar tubes containing similar volumes of Nanopure water before running the centrifuge. We then placed the plasma supernatant in 2 mL centrifuge tubes and put them in the Eppendorf mini centrifuge to spin for another 10 min at 2.8 rpm. We aliquoted the plasma supernatant into cryotubes and stored them in the freezer at −150°C. We sent samples to Microgen Laboratories in Houston, TX, for analysis. After thawing the samples to room temperature, technicians determined serum levels of IL-1ra, IL-6, CRP, and TNFR1 using commercially available enzyme-linked immunosorbent assay (ELISA) kits (R & D, Minneapolis, MN). We used TNFR1 to measure TNF-α activity because TNF-α is rapidly cleared from circulation and is, therefore, a less stable and reliable biomarker (Diez-Ruiz et al., 1995; Grassi-Oliveira et al., 2009). Technicians followed commercial ELISA manufacturer recommendations for all biomarkers and read the final readings using a SpectraMax Plus plated reader (Molecular Devices, Sunnyvale, CA).
Instruments
Demographic questionnaire
We used a demographic questionnaire to gather information on age, sex, ethnicity, education, employment status, relationship to elder, details of the care provided, as well as the general health of the elder and caregiver. We also asked the caregiver to self-report significant symptoms of depression.
Sociotropy and autonomy
We measured the personality factors sociotropy and autonomy using the Personal Style Inventory II (PSI-II; Robins et al., 1994), a self-report questionnaire with two 24-item scales, one measuring sociotropy and the other autonomy. The sociotropy scale measures how much a person values their interpersonal relationships and others' opinions, whereas the autonomy scale measures the degree to which people value having control and mastery over a situation. The PSI-II uses a 6-point Likert-type scale, and scores are summed to get a total score for each of the two 24-item scales. Additionally, sociotropy and autonomy comprise three subscales each. The sociotropy subscales are Desire to Please Others, Dependency, and Concern About What Others Think; while autonomy subscales are Perfectionism, Need for Control, and Defensive Separation. Robins et al. (1994) evaluated validity of the instrument in a number of studies, where a factor analysis determined that the PSI-II had two factors. Adequate convergent and discriminant validity were determined by comparing the PSI-II to the Dependency and Self-criticism subscales of the revised Depressive Experiences Questionnaire. The instrument has a test–retest reliability of 0.80 for sociotropy and 0.70 for autonomy (Robins et al., 1994). Cronbach’s alpha for the current sample was 0.85 for sociotropy and 0.87 for autonomy. Cronbach’s alpha for the sociotropy subscales were as follows: concern about what others think, 0.78; dependence, 0.71; please others, 0.74. Cronbach’s alpha for autonomy subscales were as follows: perfectionism, 0.71; need for control, 0.74; defensive separation, 0.77.
Depression
We assessed depression with the CES-D (Radloff, 1977), a 20-item questionnaire using a 4-point Likert-type scale ranging from rarely or none (0) to most of the time (3). Unlike scales used for diagnosis at clinical intake, the CES-D is used to measure the overall level of depression in the general population. It assesses depression symptoms experienced in the past week in order to measure current levels of depressive symptomatology with an emphasis on depressed mood. Possible scores range from 0 to 60, with higher scores indicating greater depressive symptomatology. In caregiving and other medical studies, the CES-D scale demonstrated strong internal consistency, with a Cronbach’s alpha of 0.79–0.90 (King et al., 2001; Lee, Brennan, & Daly, 2001). In the current sample the CES-D had a Cronbach’s alpha of 0.87.
Caregiving stress
We assessed participants' level of psychological stress due to caregiving using the Burden Interview Index (BI), a 22-item questionnaire designed to measure specific areas of subjective caregiver burden (Zarit & Zarit, 1990). Participants rank their responses on a 5-point Likert-type scale (0 = never, 4 = nearly always) and responses are summed to produce a total score. Possible scores range from 0 to 88, with higher scores indicating a greater level of caregiver distress. Bachner and O’Rourke (2007) investigated internal consistency reliability for the Burden Interview in a meta-analysis and reported it to be 0.62–0.95 across the 138 studies, with an average Cronbach’s alpha of .86. The scale had a Cronbach’s alpha of .91 in this study. Predictive validity has been estimated by correlating the total score with a single global rating of burden (r = .71) and with responses to the Brief Symptom Inventory (r = .41; Zarit & Zarit, 1990).
Data Analysis
We used the Statistical Package for the Social Sciences software (SPSS, version 18) for data analysis. We performed the following data screening and assumption testing to ensure that data met the assumptions prior to analysis: collinearity diagnostics, residual analysis, and leverage values. We calculated descriptive statistics to summarize caregiver and dependent demographic characteristics and performed Pearson product–moment and point biserial correlations to assess relationships between study variables. We investigated partial and full mediation using Baron and Kenny’s (1986) procedure for establishing mediation.
To understand the distribution of cytokine levels, we calculated means and standard deviations and utilized them to plot the frequency distribution for IL-1ra, IL-6, CRP, and TNFR1. The data for cytokines TNFR1, IL-6 and IL-1ra did not meet the assumptions of parametric techniques. Therefore, we created additional variables for further analysis of these cytokines based on quartiles (i.e., top 25% was compared to the rest of the group, thus dichotomizing the data). We identified predictors of CRP using stepwise multiple regression and predictors of TNFR1, Il-6, and IL-1ra using logistic regression analysis. We conducted multiple linear regression analysis to investigate predictors of depression. Alpha was set at .05.
Results
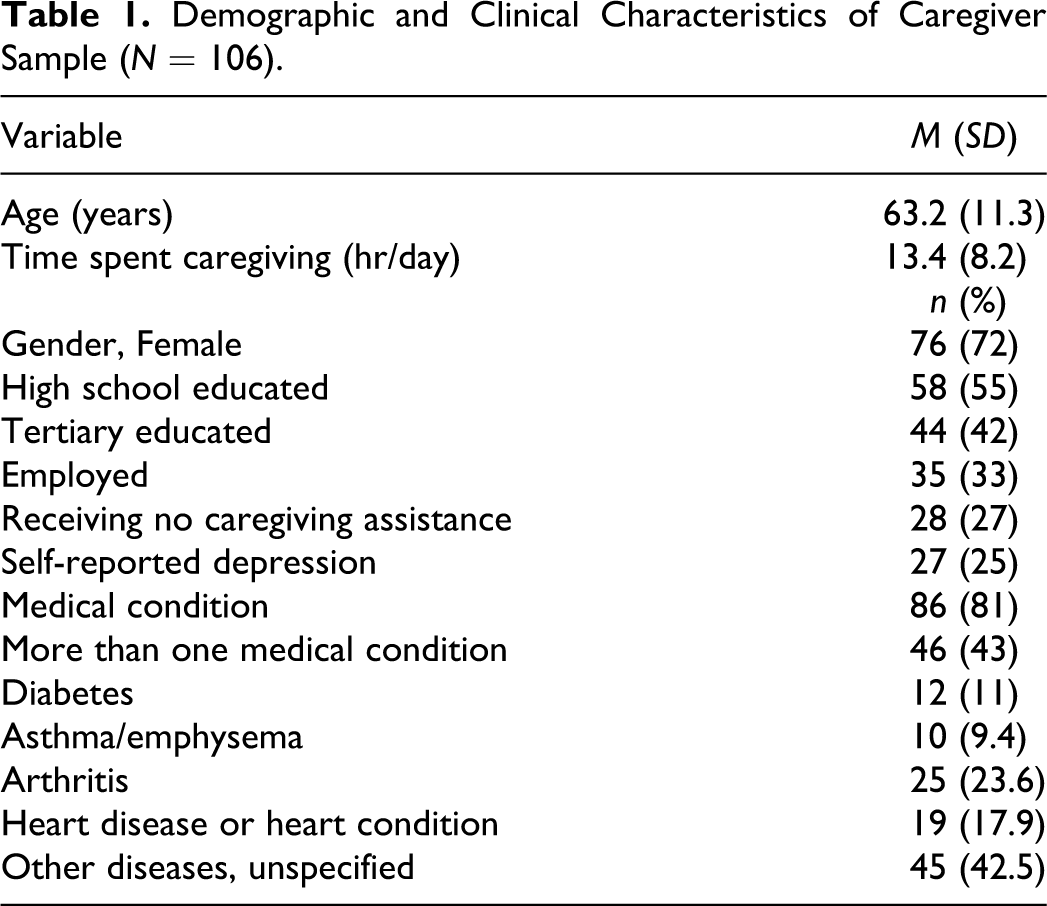
The sample of 106 caregivers primarily consisted of sons and daughters (49.1%, n = 52) and spouses (40.6%, n = 43), with the remaining caregivers being other family members including grandchildren and siblings. Participants carried out an average of five daily caregiving tasks for their dependents (see Table 1).
Demographic and Clinical Characteristics of Caregiver Sample (N = 106).
Of the dependent elders, 63% were female (n = 67), and they ranged in age from 61 to 91 years, with an average age of 80.7 years. Elders on average had 2.5 comorbid medical conditions, with 79.2% of the elders (n = 84) having Alzheimer’s disease or dementia, 23.6% (n = 25) diabetes, 13.2% (n = 14) emphysema/asthma, 44.3% (n = 47) arthritis, 40.6% (n = 43) hypertension, 34.9% (n = 37) heart conditions, and 18.9% (n = 20) diagnosed with another unspecified condition.
Mean scores were 79.4 (SD = 18.1) and 77 (SD = 16.3) for sociotropy and autonomy, respectively, 37.4 (SD = 15.5) for caregiver burden, and 17.3 (SD = 10.7) for depression. The self-reported depression rate was 25% (n = 27); however 54.7% (n = 58) of the participants scored above the clinical cutoff for depression on the CES-D. Table 2 displays zero-order correlations for the variables used in the study and Table 3 presents point-biserial and polychoric correlations of the demographic variables with the cytokines.
Zero-Order Correlation Matrix of Measured Variables.
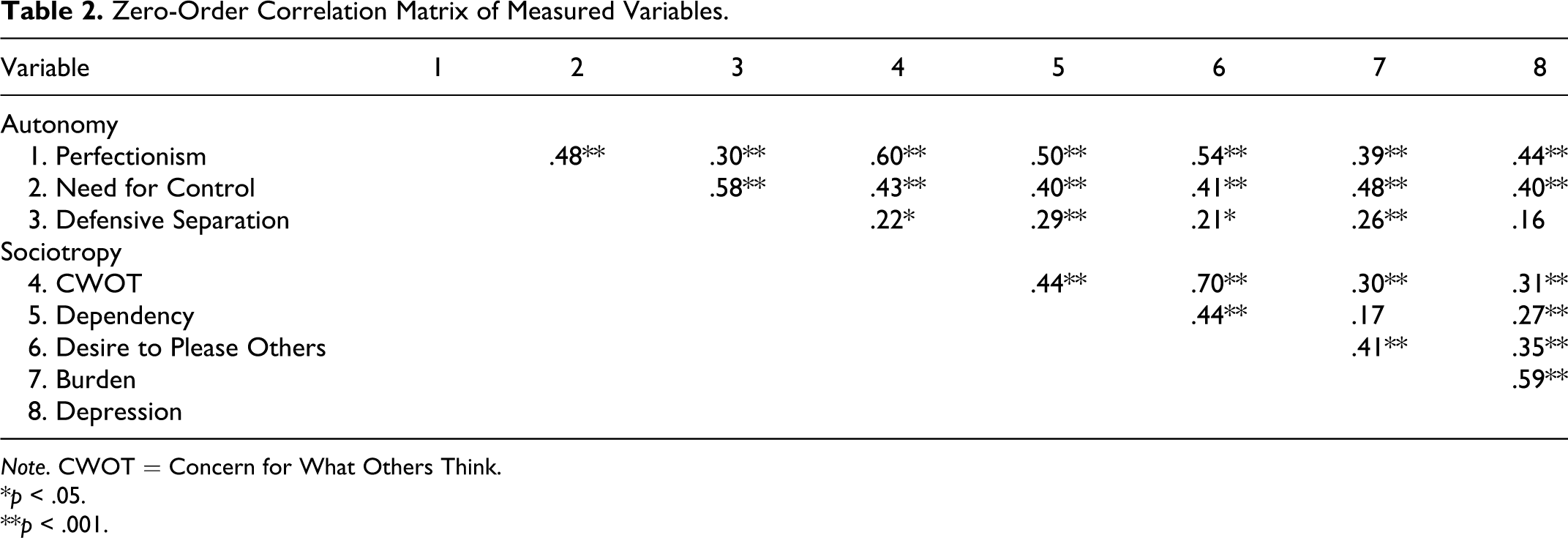
Note. CWOT = Concern for What Others Think.
*p < .05.
**p < .001.
Point-Biserial and Polychoric Correlation Matrix of Cytokines With Demographic Variables.
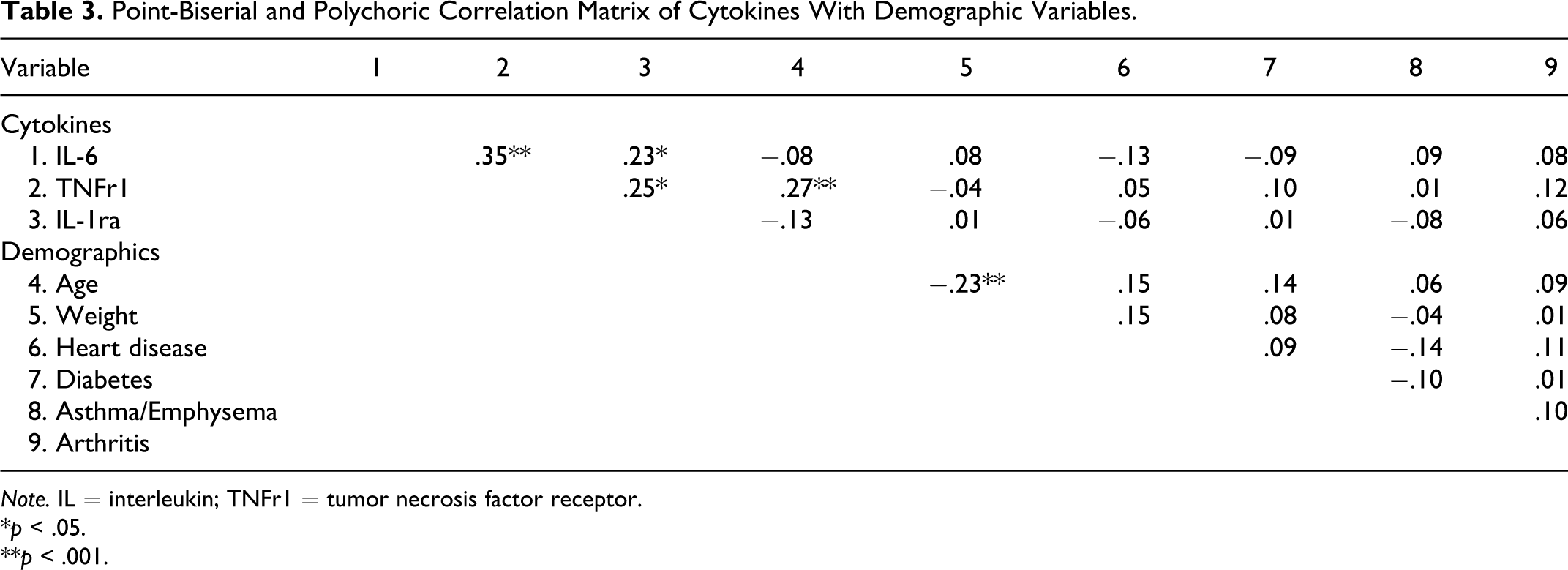
Note. IL = interleukin; TNFr1 = tumor necrosis factor receptor.
*p < .05.
**p < .001.
Aim 1: Predictors of Cytokines
We performed a logistic regression with sociotropy, autonomy, and burden total scores serving as predictors of IL-6 levels (high vs. low). We included 89 cases in the analysis and excluded 17 due to missing data. The model explained 18.5% of the variance, χ2(3, N = 89) = 11.82, p < .05. Burden significantly predicted IL-6 levels, with sociotropy and autonomy not significantly contributing to the model. We also examined predictors of IL-1ra using logistic regression, with sociotropy, autonomy, and burden total scores serving as predictors. There was no statistically significant difference between the full model and a constant-only model, p = .52.
We again performed logistic regression analysis to investigate the predictors of TNFR1. The sociotropy and autonomy subscales served as predictors with level (high vs. low) of TNFR1 as the criterion. We did this to better understand the relationships of individual components of these constructs due to the lack of significance of the total scores in the previous analyses. In this analysis, we included 95 cases and excluded 11 due to missing data. Table 4 presents the results, with Dependency and Desire to Please Others being the significant predictors of TNFR1, χ2(6, N = 93) = 8.41, p < .05. The model explained 13% of the total variance. Neither the remaining sociotropy subscale nor any of the autonomy subscales reached statistical significance, all p values > .05.
Logistic Regression Test Statistic Results for TNFR1, IL-6, and IL-1ra.
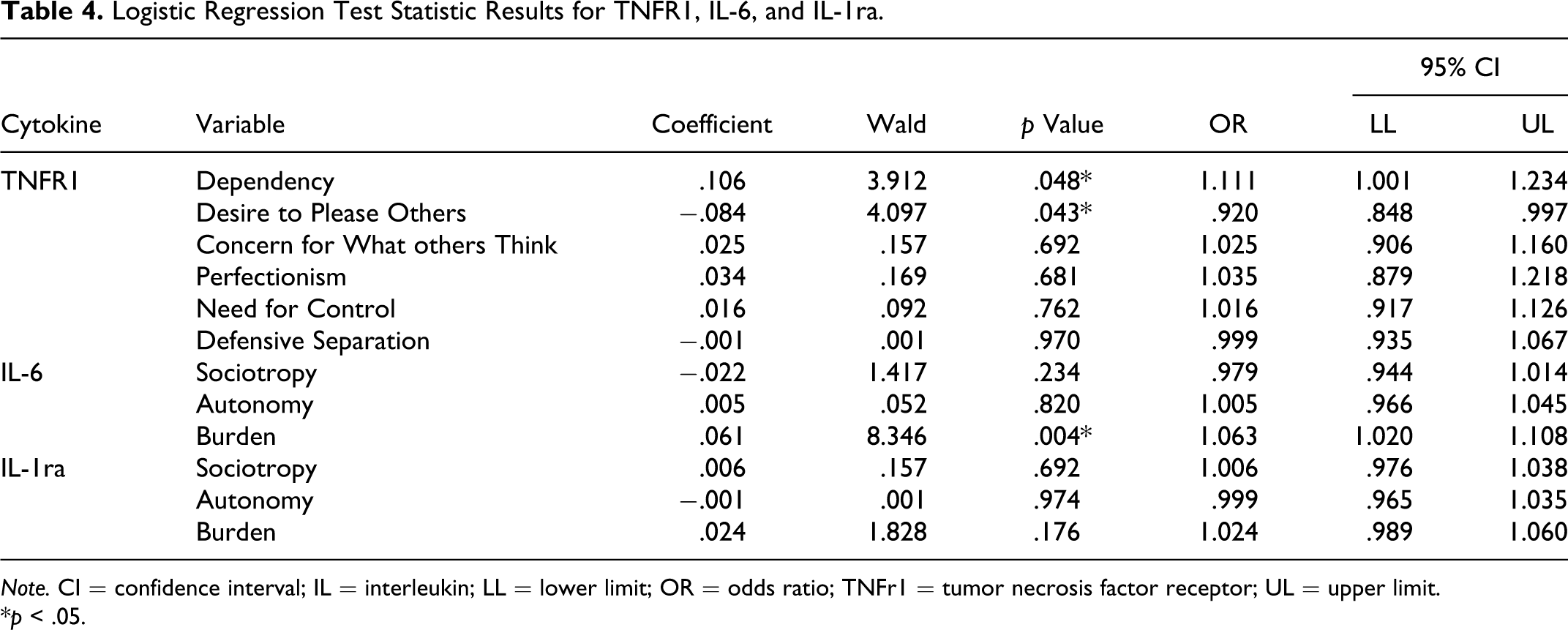
Note. CI = confidence interval; IL = interleukin; LL = lower limit; OR = odds ratio; TNFr1 = tumor necrosis factor receptor; UL = upper limit.
*p < .05.
We performed a stepwise multiple regression analysis to explore the predictors of CRP levels, including 95 cases in the analysis and excluding 11 due to missing data. The resulting model explained 4.1% of the variance in CRP levels, F(1, 94) = 3.96, p < .05. Burden was the only significant predictor, b = .053, β = .202 (CI95% .001, .106), p < .05, with increased burden scores corresponding to an increase in CRP levels. We excluded sociotropy and autonomy from the final model, as they had p values > .05.
Aim 2: Predictors of Depression
The mediation model was not statistically significant (z = 1.77). Therefore, we used multiple linear regression to ascertain which indicators were good predictors of depression. We regressed depression on autonomy, sociotropy, burden, and the cytokines TNFR1, IL-6, IL-1ra, and CRP. This model explained 45% of the variance in depression, F(7, 80) = 9.24, p < .001. As shown in Table 5, burden and TNFR1 were the only significant predictors. Thus, the greater the burden and TNFR1 level of a caregiver, the higher her or his depression score.
Linear Regression Test Statistic Results for Depression.
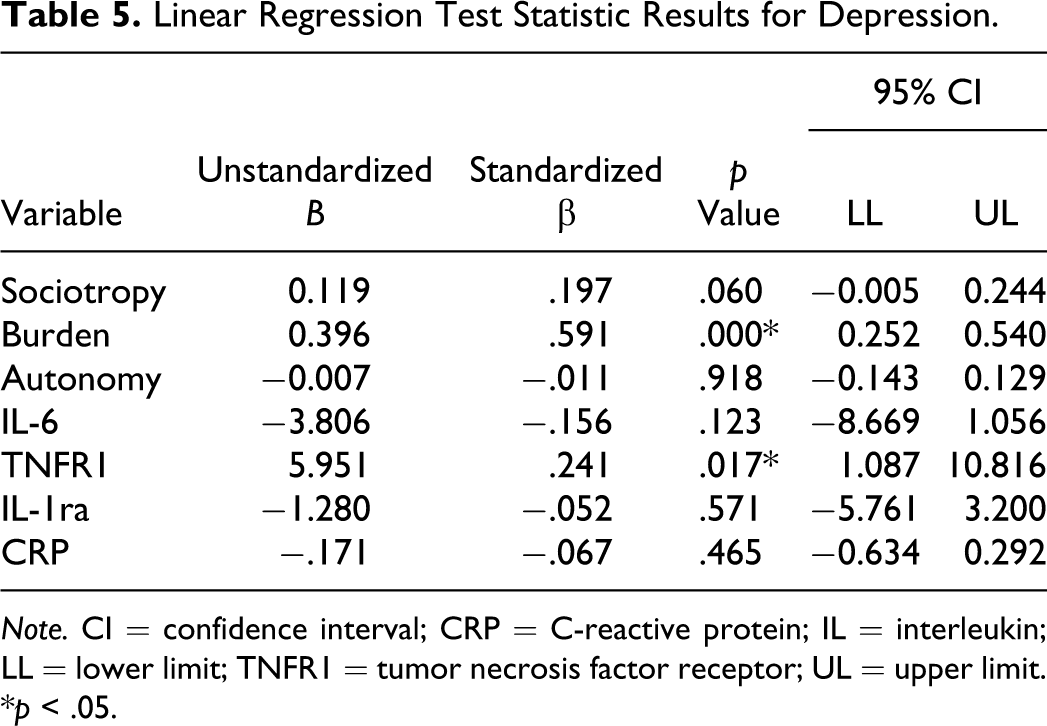
Note. CI = confidence interval; CRP = C-reactive protein; IL = interleukin; LL = lower limit; TNFR1 = tumor necrosis factor receptor; UL = upper limit.
*p < .05.
Discussion
In past research, high scores on the personality factors sociotropy and autonomy provided an explanation as to why some caregivers experienced depression while others with similar caregiving situations did not (Clark & Diamond, 2010). However, findings of the present study do not support the mediating effects of sociotropy and autonomy on caregiver burden’s influence on depression that Beck (1987) identified in his diathesis–stress model. In our mediation model, neither sociotropy nor autonomy was a significant mediator of depression. We thus found no evidence to support our hypothesis of increased risk for depression in individuals high on these factors. This result could be due in part to sample characteristics. The caregivers had a mean age of 63.2 years, and 81% (n = 86) reported having medical conditions, themselves. Furthermore, caregivers spent a significant portion of their time—an average of 13.4 hr per day—caring for their dependent. A large number of them (n = 84; 79.2%) were caring for a dependent with Alzheimer’s or dementia, which can be highly stressful and work intensive (Polk, 2005). These facts taken together suggest that the sample for this study was under a heightened level of burden, which may have negated the proposed buffering effect of being low on the psychological risk factors of sociotropy and autonomy.
Consistent with previous research on cytokines, we found that the extent of caregiver burden predicted CRP and IL-6 levels, with higher burden scores associated with higher levels of both. While we did not directly test this relationship, the fact that IL-6 is a major stimulator of CRP production provides a reasonable explanation. Since burden measures psychological stress due to caregiving, our results support previous findings that exposure to environmental stressors affect an individual’s cytokine levels (Robles et al., 2005). Though this effect has been inconsistent in direction, the effect of stress on cytokine levels can be attributed to the interaction between the HPA axis and the immune system (Raison et al., 2006). Glucocorticoid hormones related to the HPA axis can reduce the synthesis of pro-inflammatory cytokines, yet when the glucocorticoid signals are disrupted, as when an individual is under stress, this restraint is reduced, possibly resulting in overproduction of cytokines (Robles et al., 2005).
In the current study, we found no statistically significant predictors of IL-1ra, nor was IL-1ra a significant predictor of depression. However, a high score on the sociotropy Dependency subscale and a low score on the sociotropy subscale Desire to Please Others predicted soluble levels of TNFR1. The Dependency subscale gauges an individual’s reliance on his or her relationships with others (Robins et al., 1994). Those high in dependency could experience increased stress from the isolation associated with the responsibilities of caregiving. This increased stress would initiate the biological stress response and might consequently influence cytokine production. Conversely, those high on the sociotropy subscale Desire to Please Others had lower TNFR1 levels. These individuals place an increased emphasis on their relationships, putting the needs of others before their own, and are overly helpful and generous in order to sustain their relationships (Robins et al., 1994). It may well be that being high on this trait could be constructive in caregiving, since caring for and helping others is an essential aspect of the role. Conversely, those low on this trait could have a harder time adapting to caregiving as the associated behaviors are not such a significant part of their natural disposition. This finding provides further evidence that personality factors that affect how an individual reacts to an environmental stressor also affect the individual’s biological stress response.
In line with previous research in caregiving populations, we found a high incidence of depression in our caregiver sample, with 54.7% of caregivers displaying clinical levels. Interestingly, when we asked them, only 25% of the caregivers self-reported depression. This finding reflects the huge disparity in the general population between the total number of people with depression, and mental illness more generally, and the fraction of this number who have been diagnosed or are receiving treatment for their disorders (Ani et al., 2008).
Caregiver burden and soluble TNFR1 levels were significant predictors of caregiver depression. While limited in explanatory power, these results assist in providing a preliminary profile of at-risk caregivers: those high in burden and TNFR1 are at increased risk for depression. Congruent with previous research demonstrating an association between cytokines and depression (Grassi-Oliveira et al., 2009), high levels of the cytokine TNFR1 predicted depression severity in the present study. There are a number of mechanisms by which cytokine levels could affect an individual’s mood. Researchers have shown that levels of pro-inflammatory cytokines such as TNFR1 increase in response to the environmental stressor that precedes depression (Maes et al., 1998). This increase in blood cytokine levels has a profound effect on the metabolism of brain serotonin (Myint & Kim, 2003). TNFR1 can reduce the production of serotonin by stimulating the activity of indoleamine 2, 3-dioxygenase, an enzyme that converts the serotonin precursor tryptophan to kynurenine. With less tryptophan available for serotonin synthesis, serotonin concentrations in the brain decrease. Alterations in neurotransmitter levels are thought to be a common cause of depression.
TNFR1 may also affect depression through its interaction with the HPA axis. Hyperactivity of the HPA axis in depressed patients has been a consistent finding in biological psychiatry (Barden, 2004). Researchers have posited that this hyperactivity is caused by dysregulation of the corticotropin-releasing hormone–adrenocorticotropic hormone–cortisol (CRH–ACTH–cortisol) negative feedback system. Normally, elevated levels of CRH trigger the release of ACTH, which stimulates the adrenal glands to release cortisol. Once cortisol levels reach a critical threshold, the cortisol inhibits further release of CRH, completing the negative feedback cycle. Disruption to this system leads to hypersecretion of CRH and cortisol, which researchers have implicated in the development of depression (Barden, 2004; Schiepers, Wichers, & Maes, 2005). Elevations in cytokine levels, including TNFR1, can impair the function of the HPA-axis negative feedback system by downregulating cortisol receptors in the brain (Schiepers et al., 2005). This downregulation results in continued production of CRH despite heightened levels of cortisol.
Consistent with previous research, we found in the current study that burden, a psychological stress related to caregiving, influenced the development of depression. Psychological stress has long been connected to HPA-axis functioning, as the HPA axis is the primary stress-response system (Piazza, Almeida, Dmitrieva, & Klein, 2010). Researchers posit that caregiver burden leads to depression through the dysregulation of the HPA-axis negative feedback system, as discussed above. Acute and chronic stress can cause prolonged activation of the HPA axis, leading to increased cortisol levels and depressive symptoms.
This finding of the influence of burden on depression, despite the lack of mediation effects from sociotropy and autonomy, could be evidence of a clinically and psychologically relevant “tipping point” where, when experiencing enough psychological stress and caregiver burden, individuals will develop depression regardless of the presence or absence of latent vulnerabilities. The considerable influence of caregiver burden on depression in our sample suggests that attempting an intervention when individuals are already entrenched in the caregiving role, let alone already displaying depressive symptoms, is much too late. The effects of burden in this sample, predicting both cytokine levels and depression, suggest that intervention should occur before heightened levels of burden are experienced.
Current interventions usually focus on helping the caregiver cope with known caregiver burden and stressors (Gallagher-Thompson & Tong, 2007; Martin-Carrasco et al., 2009). For many intervention studies, the assumption is that the caregiver is experiencing at least some degree of caregiving stress and therefore would be motivated to voluntarily participate in intervention programs. However, as caregivers reach a critical level of burden, they are already experiencing heightened levels of cytokines, which has a significant effect on their health and well-being and places them at risk for not only depression but also for a number of other chronic diseases (Schulz & Sherwood, 2008). Though we did not address the issue of timing in the present study, those at beginning of the caregiving experience are likely to have minimal levels of burden. Therefore, perhaps early in the caregiving experience is a more optimal time to intervene with education about caregiving and coping strategies.
Limitations
A significant challenge when using cytokine data is that it tends to be skewed and kurtotic (Corwin, 2000). For the present study, we were unable to normalize the data through transformation techniques, so we transformed the cytokine variables, except for CRP, into dichotomous variables, which may have limited our ability to detect some of their effects. As researchers begin to use biological markers to explain and predict health care outcomes, they need to consider sample composition and look for innovative analytic methods to assist with nonnormal data.
Cytokines are also influenced by a number of factors including age, chronic disease, medication, and life events. Unfortunately, we could not control for all possible confounding factors due to limitations of data collection. For instance, many caregivers could not recall the names of the medications they were taking. Similarly, we did not collect data on major life events since we were already asking the caregivers to complete five instruments along with a blood draw. While established life event instruments are quite onerous, in hindsight we could have had 1 item asking if any significant stressor like job loss or death had occurred in the last 3 months. In some studies, age and chronic illnesses have influenced cytokine levels. We did not control for these factors in the current analysis and, as such, results should be interpreted with caution. While correlations between the variables in this study suggest that these factors had minimal effect, researchers in future studies should further investigate the effect of these potential confounders.
Finally, due to the study inclusion requirements and the invasiveness of blood collection the size of our sample was restricted. This negatively affected our statistical power, which may explain our inability to establish either partial or full mediation (Baron & Kenny, 1986). However, despite this lack of power, our findings do suggest some important predictors of depression, which highlights the need for further research in this area.
Conclusion
Few psychosocial models include biological markers. By examining cytokines along with caregiver burden, personality factors, and depression, this study extends the diathesis–stress model of caregiving and our understanding of depression. Our findings demonstrate the important influence cytokines have on the psychological health and well-being of the caregiver. Increasing our understanding of the impact of the caregiving experience as a significant stressor can help improve and refine health care professionals' screening practices for psychological and chronic diseases among the caregiving population.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the New Investigator’s Award from the University of Nevada, Las Vegas.