
Abstract
Objectives:
This randomized controlled trial was conducted to examine immune recovery following breast cancer (BC) therapy and evaluate the effect of mindfulness-based stress reduction therapy (MBSR) on immune recovery with emphasis on lymphocyte subsets, T cell activation, and production of T-helper 1 (Th1; interferon [IFN]-γ) and T-helper 2 (Th2; interleukin-4 [IL-4]) cytokines.
Method:
Participants who completed the study consisted of 82 patients diagnosed with Stage 0–III BC, who received lumpectomy and adjuvant radiation ± chemotherapy. Patients were randomized into an MBSR(BC) intervention program or a control (usual care) group. Immune cell measures were assessed at baseline and within 2 weeks after the 6-week intervention. The numbers and percentages of lymphocyte subsets, activated T cells, and Th1 and Th2 cells in peripheral blood samples were determined by immunostaining and flow cytometry.
Results:
Immune subset recovery after cancer treatment showed positive associations with time since treatment completion. The B and natural killer (NK) cells were more susceptible than T cells in being suppressed by cancer treatment. Women who received MBSR(BC) had T cells more readily activated by the mitogen phytohemagglutinin (PHA) and an increase in the Th1/Th2 ratio. Activation was also higher for the MBSR(BC) group if <12 weeks from the end of treatment and women in MBSR(BC) <12 weeks had higher T cell count for CD4+.
Conclusion:
MBSR(BC) promotes a more rapid recovery of functional T cells capable of being activated by a mitogen with the Th1 phenotype, whereas substantial recovery of B and NK cells after completion of cancer treatment appears to occur independent of stress-reducing interventions.
Women with a new diagnosis of breast cancer (BC) experience immune dysregulation, characterized by lower interferon (IFN)-γ and increased interleukin-4 (IL-4), interleukin-6 (IL-6), and interleukin-10 (IL-10; Witek-Janusek, Gabram, & Mathews, 2007). Immune regulation may explain in part why the level of distress experienced as a result of the diagnosis of cancer affects survival outcomes (Andersen et al., 2007; Sephton et al., 2009).
Chemotherapy and radiation therapy (RT) may differentially affect immune recovery. RT significantly reduces white blood cell, lymphocyte, and natural killer (NK) cell numbers and NK cell activity (Koukourakis, Zabatis, Zacharias, & Koukourakis, 2009; Standish et al., 2008; Yamazaki et al., 2002), which persisted for 6 weeks post-RT in one study (Standish et al., 2008). Witek-Janusek et al. (2008) reported increased levels of IL-4, IL-6, and IL-10 for 3 months after RT.
Chemotherapy alone reduced IL-2 (T-helper 1 [Th1]-type response) and cytotoxic T (cluster of differentiation [CD8+]) cells (Kang et al., 2009; Mozaffari et al., 2007, 2009; Solomayer et al., 2003), while IL-4 (T-helper 2 [Th2]-type response) was lower in the RT-only group (Kang et al., 2009). Immune recovery took up to 12 months in 80 BC patients who received either chemotherapy alone or chemotherapy and RT, with IL-6 and most CD+ subsets (except CD4+) recovering faster than NK cells, IFN-γ, and IL-2 (Kang et al., 2009). Mozaffari et al. (2007, 2009) found similar reductions in T cells among BC patients who received either RT alone or both RT and chemotherapy, with lower CD4+ levels during extended follow-up for patients who received both RT and chemotherapy.
Mindfulness-based stress reduction (MBSR) is a complementary and alternative medicine (CAM) therapy that has been used by some cancer patients for stress reduction. The overall goal of the MBSR program is to teach patients to take an active role in their stress management by learning mindfulness meditative practices along with the attitudinal foundations of nonjudging, patience, a beginner’s mind, trust, nonstriving, acceptance, and letting go (Kabat-Zinn, 1990). This mindful state enhances attention and awareness and promotes self-regulation, leading to relaxation.
From 2000 to 2009, MBSR was one of the most common clinical interventions investigated for patients with cancer (Brown & Ryan, 2003; Carlson & Brown, 2005; Carlson & Garland, 2005; Carlson, Speca, Faris, & Patel, 2007; Carlson, Speca, Patel, & Goodey, 2003, 2004; Carlson, Ursuliak, Goodey, Angen, & Speca, 2001; Garland, Carlson, Cook, Lansdell, & Speca, 2007; Hebert et al., 2001; Lengacher et al., 2009; Saxe et al., 2001; Shapiro, Bootzin, Figueredo, Lopez, & Schwartz, 2003; Speca, Carlson, Goodey, & Angen, 2000; Tacon, Caldera, & Ronaghan, 2004; Witek-Janusek et al., 2008). Of these oncology studies, five were randomized clinical trials (RCTs), all of which found that MBSR reduced psychological and physical symptoms (Carlson et al., 2001; Hebert et al., 2001; Lengacher et al., 2009; Shapiro et al., 2003; Speca et al., 2000). Only one RCT has tested immune responses to MBSR in a noncancer population (Creswell, Myers, Cole, & Irwin, 2009). Several nonrandomized, quasi-experimental studies assessed immune response to MBSR in cancer patients (Carlson et al., 2003, 2004, 2007; Saxe et al., 2001; Witek-Janusek et al., 2008), some of which used a nonrandomized control group (Witek-Janusek et al., 2008) or a single-arm design assessing responses over time (Carlson et al., 2003, 2004, 2007).
For the present study, we specifically chose women who had completed treatment because of the known immune-modulating effects of RT and chemotherapy. The study objectives were to determine in BC survivors (a) the natural history of lymphocyte recovery as measured by time since treatment, (b) if there was a difference in lymphocyte recovery due to treatment regimen or time since treatment, and (c) if an MBSR intervention and/or time since treatment alters differences in lymphocyte recovery.
Materials and Methods
Participants
We recruited a total of 84 women, aged 21 or older and previously diagnosed with Stage 0–III BC, who underwent surgery (lumpectomy) and received adjuvant RT and/or chemotherapy, from the H. Lee Moffitt Cancer Center and Research Institute, a National Cancer Institute-designated center at the University of South Florida, Tampa. All participants had completed treatment within the prior 18 months. Additional eligibility criteria included ability to read and speak English at the 8th-grade level. Exclusion criteria included Stage IV BC, history of mastectomy, severe psychiatric diagnosis (e.g., bipolar disorder), or treatment for recurrent BC. All participants provided written informed consent and the Institutional Review Boards at the University of South Florida, and the Moffitt Cancer Center approved the study protocol. Participants received $50 at the beginning and $50 at the completion of the study.
Procedures
Study design and random assignment
We used a two-armed randomized controlled design with randomization stratified by stage of cancer (0–III) and treatment received (RT alone vs. RT and chemotherapy). We randomly assigned consenting participants in a 1:1 ratio to either an MBSR(BC) intervention program or a control (usual care) group, whose members were waitlisted to receive the MBSR(BC) intervention (if desired) after 6 weeks.
MBSR(BC) intervention
We adapted the 6-week MBSR(BC) program used in this study from Kabat-Zinn’s original 8-week MBSR program. All of the original content was included in 6 weekly, 2-hr sessions taught by a licensed clinical psychologist trained in MBSR, who highlighted specific concerns common to women with BC, such as using mindfulness to adapt to emotional/psychological responses (anxiety, depression, and fear of recurrence) and physical symptoms, such as pain and difficulties with sleep. The intervention had three specific components: (a) educational material related to relaxation, meditation, and the mind–body connection; (b) meditative practices of sitting meditation, walking meditation, body scan, and gentle hatha yoga in group meetings, and homework assignments; and (c) discussion among group members related to barriers to practicing meditation, application of mindfulness in daily situations, and group support. Participants were instructed to record their daily meditation and yoga practice time in a diary.
Usual care/control group
The usual care/control group had standard posttreatment clinic visits. The investigators specifically asked participants in this group not to use or practice meditation, yoga techniques, or MBSR during the study. After completing the study, each control group participant was provided with a brief orientation to MBSR, a manual and CDs of the complete program and offered optional scheduled classes.
Data collection, procedures, and time points
We assessed immune outcomes in the intervention condition prior to the start of the MBSR(BC) program (baseline) and within 2 weeks of its completion and in the control condition at baseline and again 6–8 weeks from baseline.
Demographics and medical history
We collected standard demographic data and a detailed clinical history at baseline and recorded any changes at 6 weeks.
Immune Measures
Th1 and Th2 assessment and T cell activation
We determined an estimate of the number of Th1 and Th2 cells in peripheral blood samples by intracellular immunostaining of IFN-γ and IL-4 and flow cytometry, as previously described (Crucian et al., 1996). In brief, heparinized whole blood samples were stimulated to enhance cytokine production by incubating 1 ml amounts with either no stimulus (control) or the mitogen phytohemagglutinin (PHA; 20 μg/ml, Sigma, St. Louis, MO) for 2 hr followed by brefeldin A (1 μg/ml; BD Biosciences, San Jose, CA) treatment and incubation for an additional 4 hr. PHA not only induces the expression of IFN-γ and IL-4 but also promotes the expression of the CD69+ activation marker on T cells. To determine Th1 and Th2 cell percentages, samples were stained with anti-CD3 perCP and anti-CD69 APC (BD Biosciences) for 20 min. The red blood cells (RBCs) were lysed with ammonium chloride buffer and the remaining leukocytes washed and suspended in Cytofix/Cytoperm (100 μl; BD Biosciences) and incubated for 20 min at 4°C in the dark. The cells were then washed twice in Perm/Wash Buffer (BD Biosciences) and treated with either anti-IFN-γ FITC, anti-IL-4 PE, or isotype controls (BD Biosciences) and incubated for 30 min at 4°C in the dark. The samples were washed and analyzed by flow cytometry for CD3+CD69+ cells (activated T cells) that were either IFN-γ+ (Th1) or IL-4+ (Th2) using Cellquest software (BD Biosciences).
Assessing lymphocyte subsets by flow cytometry
The percentage of lymphocyte subsets (CD4+ and CD8+ T cells, CD19+ B cells, and CD16+56+ NK cells) was determined by four-color flow cytometry following staining with fluorescent antibodies (BD Biosciences). Cells were analyzed with a FACScalibur flow cytometer (Becton Dickinson) using MultiSet software. Interassay variability for laboratory leukocyte values ranged by less than 2 standard deviations (SD) from the mean values.
Statistical Methods
For each participant, we calculated ratios of selected immune variables, including % (CD4+/CD8+) and Th1/Th2 ratio (PHA). Since we created these ratios at the individual level, the mean of the ratio scores across all individuals (e.g., before and after MBSR[BC]) cannot be calculated by simply taking the ratio of aggregated means from the individual immune variables. To aid in interpretation across all biological measures, we calculated the median and SD for each marker and then created standardized change scores as follows: ([6-week median value–baseline median value]/common SD). Positive values indicate that the 6-week median value of the biomarker was higher than the baseline median value. The decision to use the median score at baseline and 6 weeks rather than mean scores was based on the fact that some mean values of immune measures (IL-4 PHA stimulation, Th1/Th2, and ratio-PHA stimulation) were positively skewed. We depicted plots of the standardized change scores in immune measures by random assignment.
We calculated Spearman rank correlation coefficients between each immune variable and the time since completion of cancer treatment at baseline for all 84 participants. Similarly, we calculated separate sets of correlation coefficients for the 51 participants treated with RT only and the 33 participants treated with both RT and chemotherapy.
To evaluate whether immune values at 6 weeks differed by random assignment, linear mixed models (Goldstein, 2003; Liang & Zeger, 1986) were fit. In each model, the immune variable of interest was the dependent variable, the main effects were random assignment (MBSR[BC] vs. control) and time (baseline or 6 weeks), and the interaction term was random assignment × time. All models included adjustment for age, race, stage of cancer, and time since treatment completion to minimize potential confounding. These models allowed for both within-participant and between-group analyses, as well as an appropriate correlation structure to account for within-person correlation of multiple immune measurements per participant. We also conducted the above analyses separately by time since treatment completion (using median-split to optimize statistical power), defined as <12 weeks (n = 41) versus >12 weeks (n = 43). A conventional Type I error rate of 0.05 was used for all analyses with no correction for multiple comparisons.
Finally, for measurement of %CD3+ IL-4 (Th2) and the corresponding Th1/Th2 ratio, 12 subjects pre-MBSR and 9 subjects at the 6-week assessment had 0 (nondetectable) values. In the primary analysis, the 0 values for %CD3+IL-4 were set to missing. In a secondary analysis, we imputed these values as 0.05 using the method described by Sepah and Bower (2009).
The trial was originally powered (80%, two-sided Type I error rate of 0.05) using measures of psychological and physical health status (rather than immunological measures) and a desire to detect a medium effect size (i.e., differences in means of the two treatment groups/SD; Cohen, 1988) of 0.60 or higher attributed to the MBSR(BC) program. The final study sample of 82 participants with baseline and 6-week data corresponded to a detectable effect size of 0.63 or higher. This effect size corresponded to the immune measures that were continuous variables, similar to the primary outcome measures of psychological and physical health status in the parent trial.
Results
Participants Characteristics
Of the 84 participants enrolled in the study, 82 (97.6%) completed both the baseline and 6-week assessments (Figure 1). We assigned 41 participants (48.8%) to the MBSR(BC) group (one was lost to follow-up) and the remaining 43 participants (51.2%) to the control group (one lost to follow-up). Mean age of participants was 58 ± 9 years, and 23 (27.4%) were 65 years of age or older. Further, 10 participants (11.9%) self-identified as Black, 61 (72.6%) as White Caucasian, 9 (10.7%) as White Hispanic, and 4 (4.8%) as Other. Also, 38 (45.2%) had at least a college degree, and 47 (56.0%) were employed. The median time since treatment completion was 19 weeks, and 43 participants (51.2%) were more than 12 weeks removed from treatment. The two groups (MBSR[BC] vs. control) were similar on baseline demographic characteristics, with the exception of Blacks being more often assigned to the control group versus the MBSR(BC) group (18.6% vs. 4.9% of the group populations, respectively, p = .05) and the MBSR(BC) group having more women aged 65 years or older (34.1% vs. 20.9%), though this difference was not significant (p = .08). Baseline assessments occurred 1–63 weeks from cancer treatment completion (median 15 weeks) in the MBSR(BC) group and 0–80 weeks (median 11 weeks) in the control group. A total of 9 participants in the MBSR(BC) group (22%) and 11 participants in the control group (26%) had completed their cancer treatment less than 6 weeks before entering the study. Only three patients were current smokers at study entry.
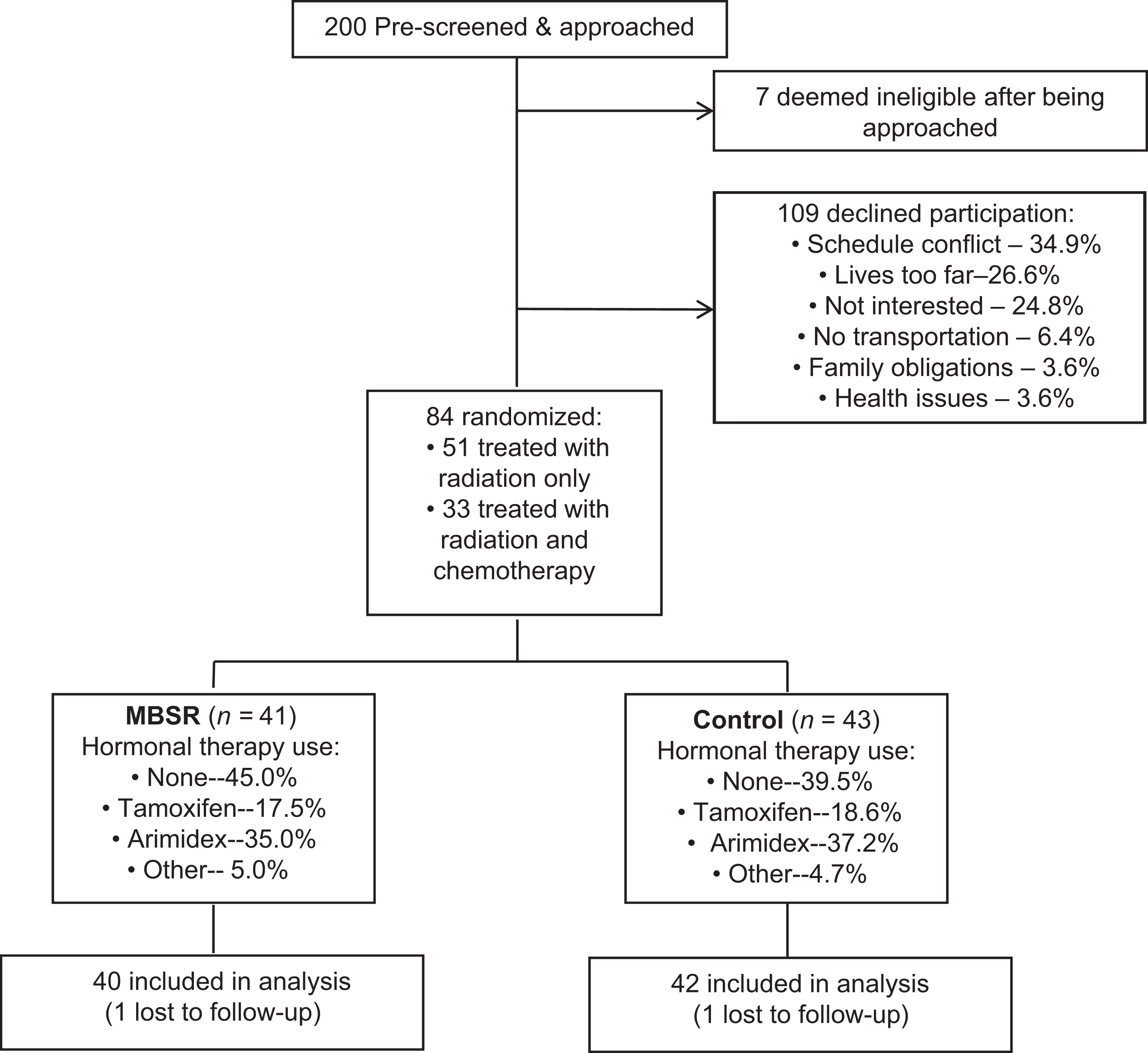
Recruitment flow chart. Flowchart showing recruitment and enrollment of 84 subjects into the trial, of whom 82 completed the study and were included in outcome analyses.
Treatment Regimens
More than half of the women had Stage I disease (53.6%). Of the remaining participants, 16.7% had Stage 0, 22.6% had Stage II, and 7.1% had Stage III disease. Just over 60% (60.7%, n = 51) of participants (median age = 61 years) had received RT alone, with the remaining participants (39.3%, n = 33; median age = 52 years) receiving both RT and chemotherapy (Table 1). Nearly all Stage II and III patients received both RT and chemotherapy. Only Stage II and III patients received conventional RT (external beam over 5–7 weeks) as opposed to Stage 0 and I patients who received accelerated RT. In all, 11% of patients received Herceptin, while 59% of patients were taking adjuvant hormonal therapy, with Arimidex being the most common type.
Baseline Characteristics of Participants by Random Group Assignment.
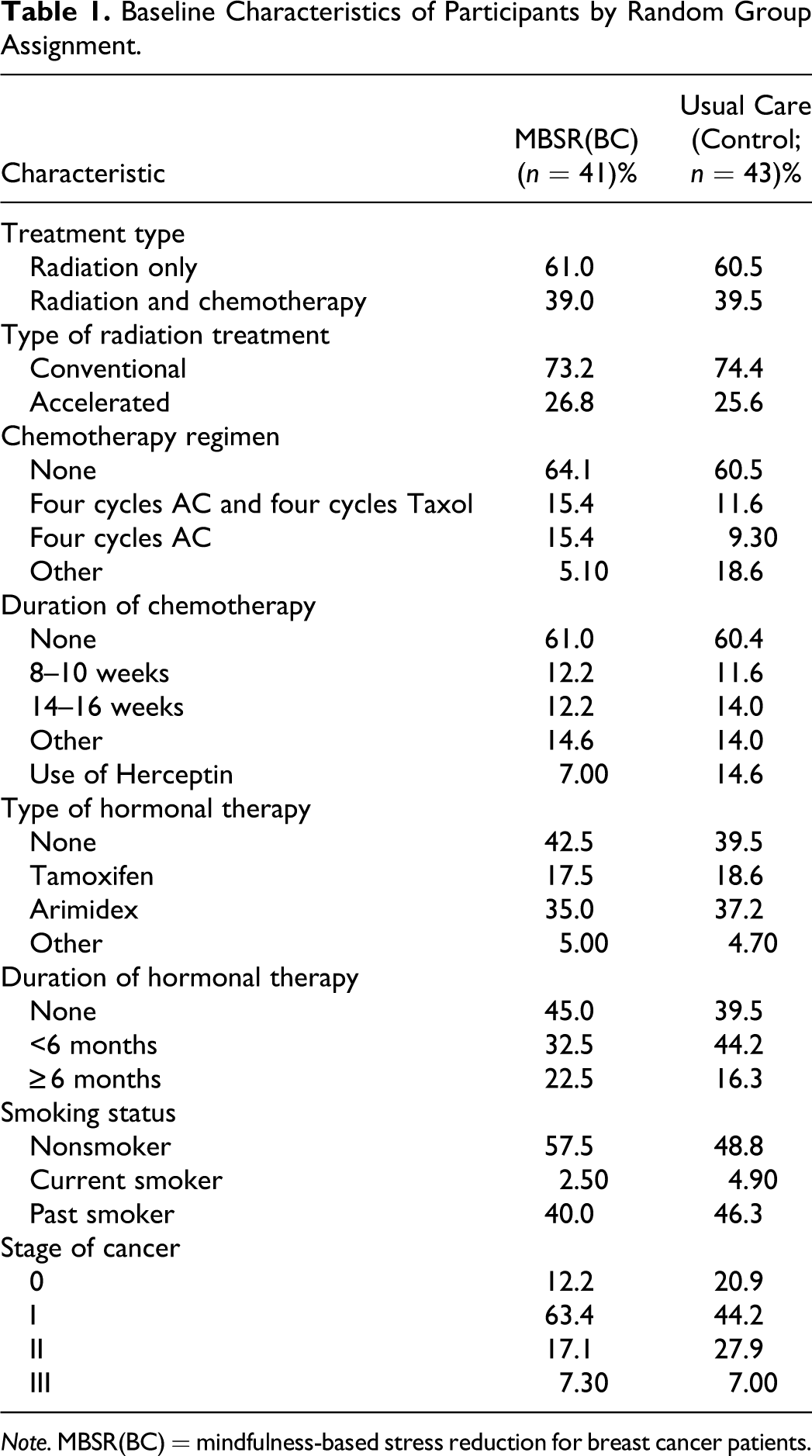
Note. MBSR(BC) = mindfulness-based stress reduction for breast cancer patients.
Association Between Time Since Treatment Completion and Lymphocyte Subset Recovery
Independent of group assignment, patients who were >12 weeks from BC treatment had significantly higher blood lymphocyte counts (p = .01) than patients who had completed treatment within the past 12 weeks (Figure 2). This difference in lymphocyte counts by time since treatment was driven mostly by higher levels of B cells (p < .0001) and NK cells (p = .008) in patients in the >12-week group. In contrast, T cell counts were similar (p = .37) in patients from both groups. Among patients who had completed treatment within the past 12 weeks, the median CD3+ (T cell) count was 842/µl of blood compared to a median B cell count of 76/µl corresponding to a T cell/B cell ratio of 11.1:1. In the >12-week group, the median CD3+ count was 883/µl compared to a median B cell count of 160/µl for a lower T cell/B cell ratio of 5.5:1. The similarity in T cell count within and after 12 weeks of cancer treatment completion and the higher T cell/B cell ratio in the <12-week group suggest that treatment with RT ± chemotherapy substantially reduced the number of B cells with minimal impact on the absolute number of T cells. Similar comparative results were obtained with NK cells.
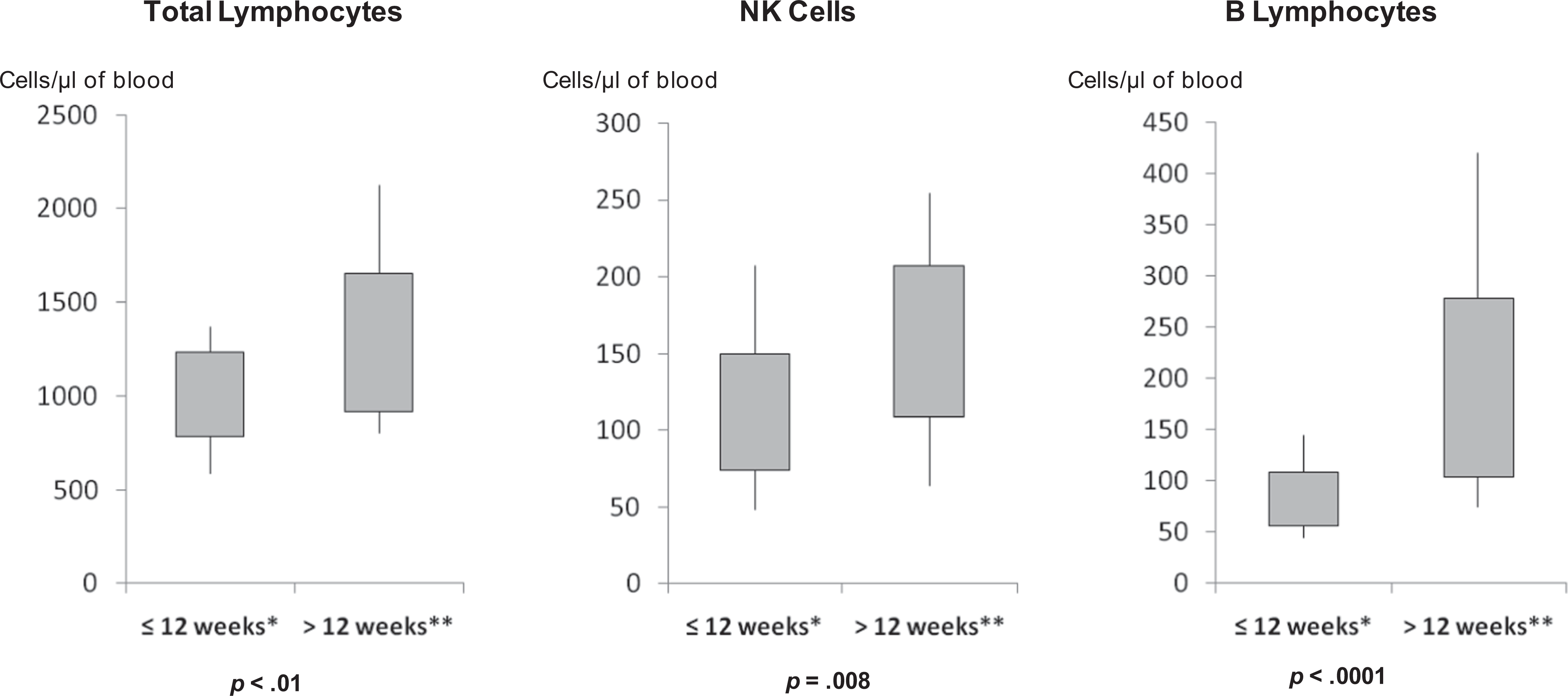
Cell counts at baseline by time since cancer treatment completion. Distribution of lymphocyte cell counts at baseline (prior to trial entry) by time since completion of RT ± chemotherapy for BC. The distributions are stratified by recent completers of treatment (≤12 weeks) versus others (>12 weeks). The shaded rectangles depict the interquartile range; the lower and upper ends of the vertical lines depict the 5th and 95th percentiles, respectively. These results are not presented by group assignment. *n = 41. **n = 43.
We calculated Spearman correlations between blood lymphocytes (as continuous variables) and time since cancer treatment completion (in weeks). Independent of group assignment, patients who were further from cancer treatment had higher absolute counts for CD8+ T cells, NK cells, and B cells. This was most pronounced in the NK and B cell subsets. Statistically significant Spearman correlations with longer time since treatment completion and absolute cell counts included total lymphocytes (r = .33, p = .002), CD8+ cells (r = .26, p = .02), NK cells (r = .41, p < .0001), and B cells (r = .59, p < .0001). Regarding T cell subsets, CD8+ cells also displayed a significant positive correlation over time. These data suggest that circulating B cells, NK cells, and CD8+ T cell subsets restore themselves over time after being reduced due to effects of RT ± chemotherapy.
Effects of Radiation and Chemotherapy on Lymphocyte Recovery
We stratified analyses by cancer treatment regimen to determine whether the type of treatment influenced the relationships between treatment completion and lymphocyte subset recovery. The percentage of patients on adjuvant hormonal therapy was similar between those receiving RT alone (61.8%) versus those treated with both RT and chemotherapy (56.2%). As seen in Figure 3, lymphocyte recovery was generally consistent irrespective of whether chemotherapy was used in conjunction with RT. That is, lymphocyte cell counts, particularly B cells, were higher in patients further removed from treatment completion (irrespective of whether chemotherapy was used), and there was seemingly more restoration of B cells compared to T cells. Statistically significant (p < .05) Spearman correlations with time since treatment completion (by treatment type) and absolute cell counts are as follows for RT only and RT ± chemotherapy, respectively: total lymphocyte (r = .38; r = .41), NK cells (r = .52; r = .37), and B lymphocytes (r = .55; r = .61). The percentages of activated cells and Th1 and Th2 cells fluctuated with time since treatment but not significantly. These results indicate that chemotherapy treatment may have a negligible effect when paired with RT on the quantitative and qualitative aspects of peripheral lymphocyte recovery following treatment.
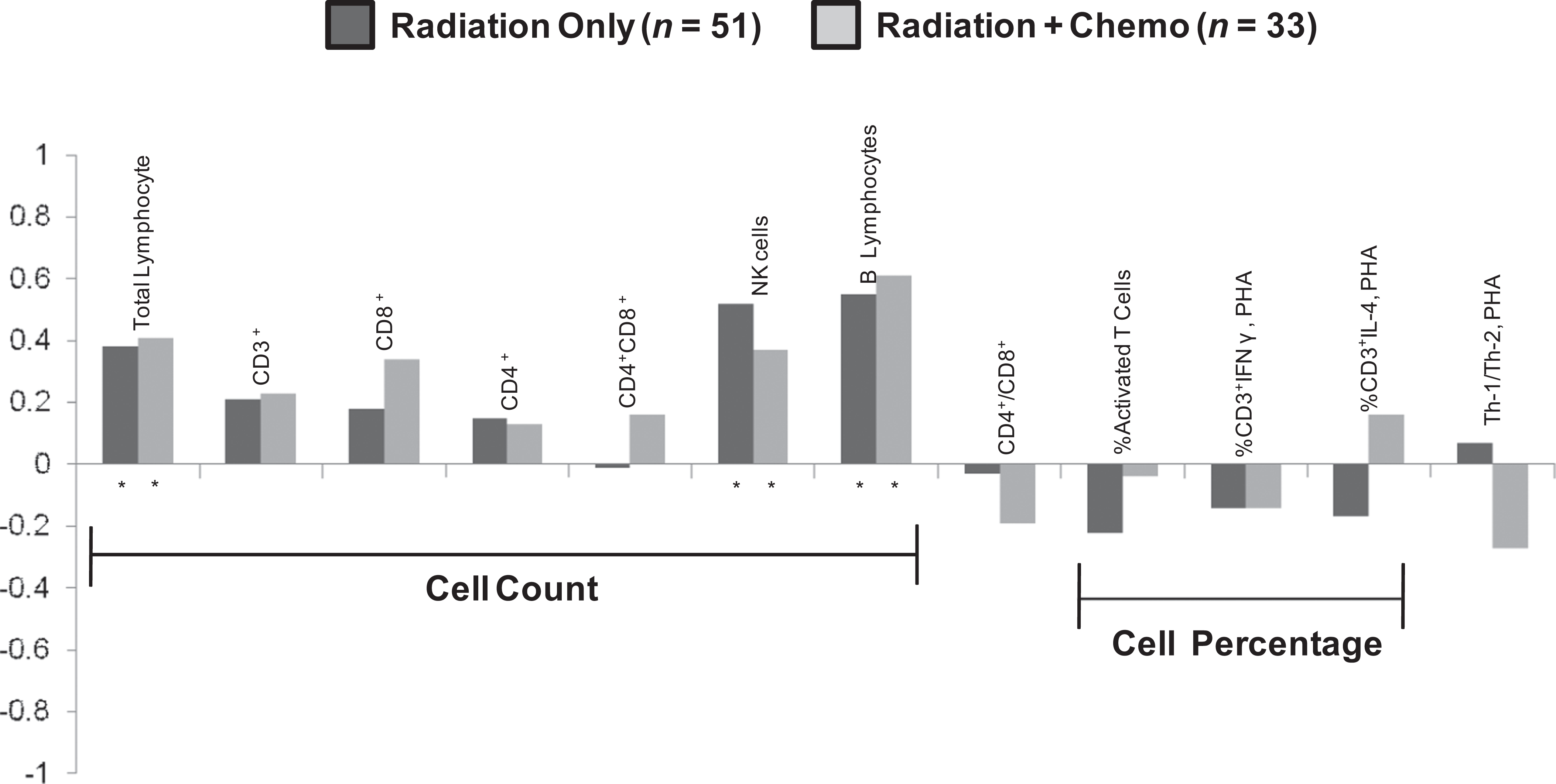
Spearman correlations with time since treatment completion (by treatment type). Positive correlations indicate that higher baseline immune marker values are associated with longer time since treatment completion. Dark shading indicates Spearman correlation coefficients between lymphocyte cell counts/percentage of lymphocytes at baseline (prior to trial entry) and time (weeks) since completion of RT, while light shading indicates a treatment regimen of RT ± chemotherapy. *p value < .05.
Change in Lymphocyte Levels by Group (MBSR [BC] vs. Control)
Between the baseline and 6-week assessment periods, absolute cell counts for lymphocytes increased to a similar extent (p = .91), regardless of group assignment (Table 2). Pre–post intervention changes in most lymphocyte subsets also were similar between participants in the MBSR(BC) and control groups. The two exceptions that achieved statistical significance (p < .05) were (a) a decrease in the mean percentage of activated T cells in the control group (from 29.1% to 20.9%) compared to a slight increase (from 26.0% to 28.0%) in the MBSR(BC) group (p = .002) and (b) a reduction in the mean Th1/Th2 ratio (log transformed) in the control group (from 2.51 to 2.05) not observed in the MBSR(BC) group (from 2.25 to 2.53; p = .03). However, in the secondary analyses, where nondetectable %CD3+IL-4 (Th2) values were imputed to a value of .05, the comparison of the mean Th1/Th2 ratio (log transformed) by random assignment did not achieve statistical significance (p = .12). Nonetheless, in aggregate, these selected statistically significant results suggest that MBSR(BC) influences a more rapid recovery of functional T cells capable of being activated by mitogen with the Th1 phenotype, whereas substantial recovery of B cells and NK cells after completion of cancer treatment appears to occur independent of stress-reducing interventions such as MBSR.
Comparison of Lymphocyte Marker Values Before and After MBSR Intervention.
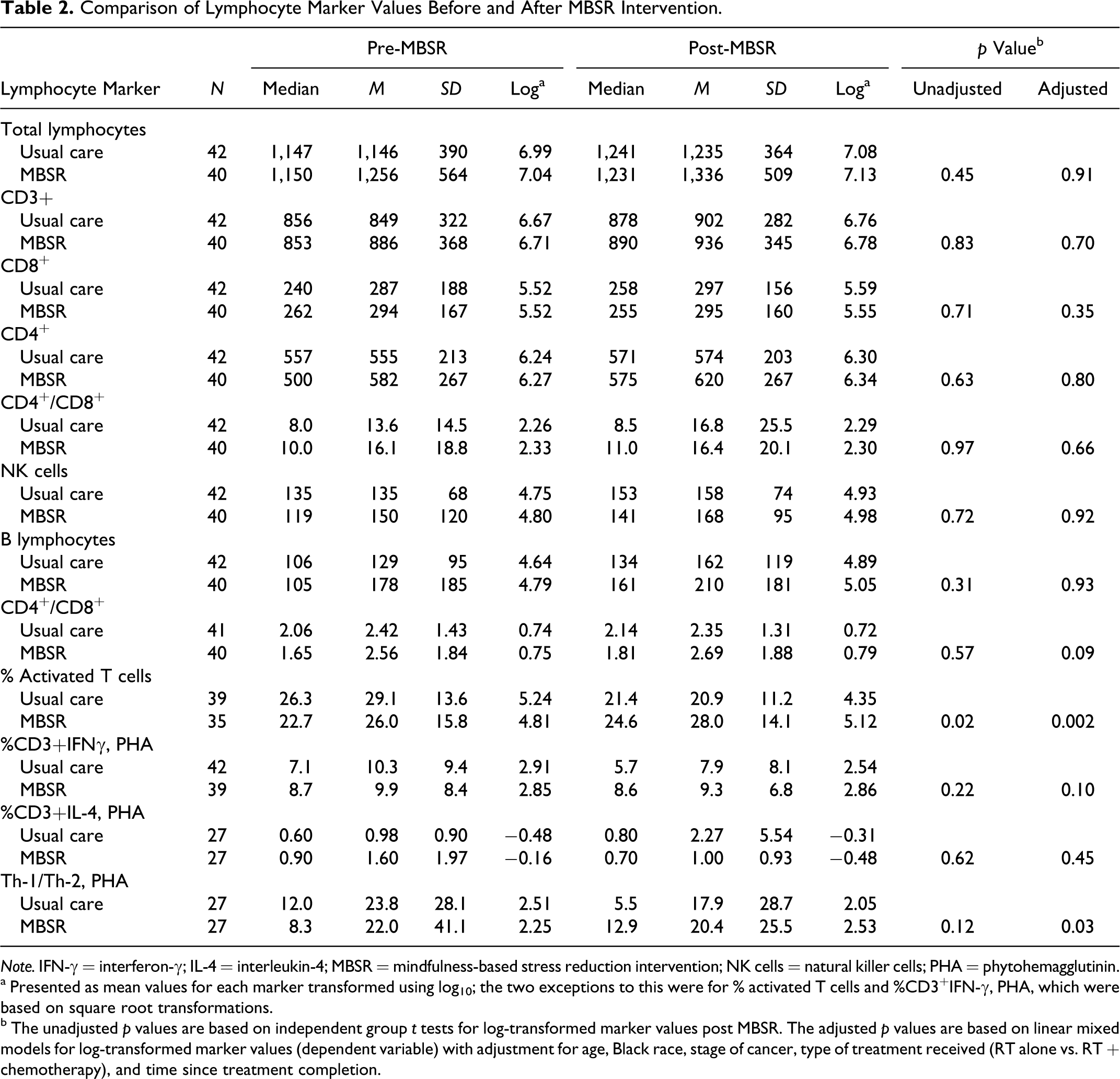
Note. IFN-γ = interferon-γ; IL-4 = interleukin-4; MBSR = mindfulness-based stress reduction intervention; NK cells = natural killer cells; PHA = phytohemagglutinin.
a Presented as mean values for each marker transformed using log10; the two exceptions to this were for % activated T cells and %CD3+IFN-γ, PHA, which were based on square root transformations.
b The unadjusted p values are based on independent group t tests for log-transformed marker values post MBSR. The adjusted p values are based on linear mixed models for log-transformed marker values (dependent variable) with adjustment for age, Black race, stage of cancer, type of treatment received (RT alone vs. RT + chemotherapy), and time since treatment completion.
For the subgroup of patients who had completed cancer treatment within 12 weeks of enrolling in the trial, absolute cell counts of both T and B cells increased during the 6-week trial period (Figure 4A). Interestingly, there was a significant increase (p < .05) in the number of CD4+ cells over the 6-week trial period in the patients in MBSR(BC) group who had completed treatment within 12 weeks, which we did not observe in the control group. This finding suggests that MBSR(BC) therapy may have a positive effect on the recovery of helper T cells during the early recovery period following cancer treatment therapy.
Finally, for patients who had completed cancer treatment more than 12 weeks before enrolling in the trial, lymphocytes increased, albeit to a lesser extent (Figure 4B) compared to recent completers of treatment (Figure 4A). Among patients further from cancer treatment, there were two significant differences between the MBSR(BC) and control groups. The percentage of activated T cells increased in the MBSR(BC) group yet decreased in the control group, and the Th1/Th2 ratio decreased in the control group compared to a slight increase in the MBSR(BC) group (p = .03). We observed similar results in the secondary analyses, where nondetectable %CD3+IL-4 (Th2) values were imputed to a value of .05 (p = .04).
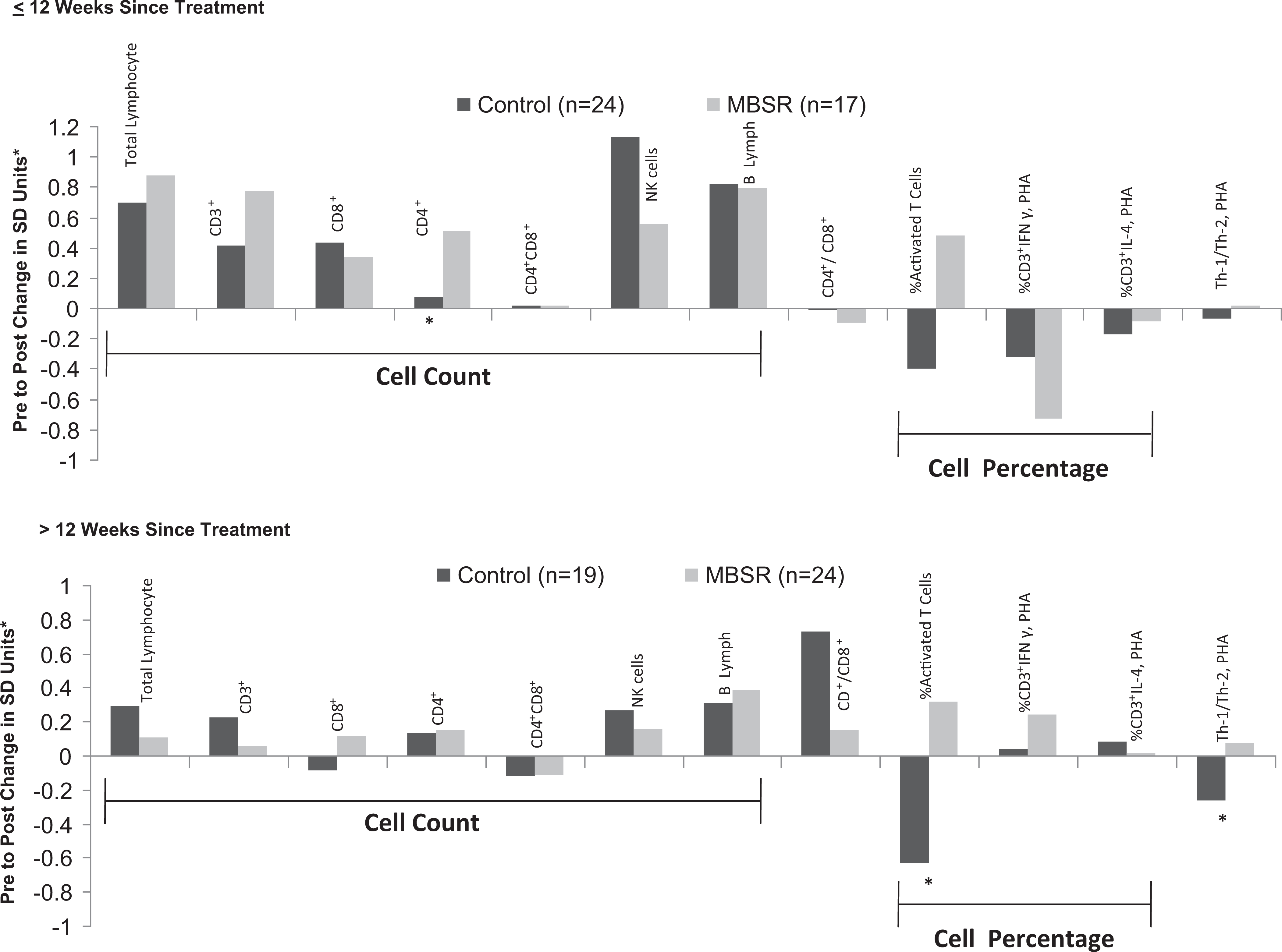
Standardized changes in lymphocyte cell counts and percentages from baseline to 6 weeks by group (dark shading = control; light shading = mindfulness-based stress reduction [MBSR] intervention). The data are stratified by recent completers of treatment: (Figure 4A. ≤ 12 weeks versus others (Figure 4B. [>12 weeks]). The standardized values (y-axis) were calculated as ([6-week median value–baseline median value]/SD); hence, positive values depict higher values at 6 weeks compared to baseline. The asterisks below the columns depict p values based on linear mixed models (*p < .05).
Discussion
To our knowledge, this is the first RCT to prospectively assess lymphocyte recovery after BC treatment with the stress-reducing effects of MBSR. Consistent with other studies assessing immune outcomes after treatment (Mozaffari et al., 2009; Strender et al., 1983), our findings show that time, alone, has a restorative effect on lymphocyte levels. Thus, investigators attempting to isolate the effects of a stress-reducing intervention require both a randomized control group and control of treatment timing or consideration for the elapsed time since cancer treatment completion for such studies.
In the present study, we had three key findings regarding immune recovery in women who have undergone treatment for BC. First, in terms of the natural history of lymphocyte recovery following conventional BC treatment, RT ± chemotherapy appear to directly suppress lymphocyte numbers, with a greater impact on B and NK cells than on T cells. On average, as the BC patient is further removed from treatment (RT ± chemotherapy), the number of B and NK cells increases to a greater extent than the number of T cells. This time effect appears to occur independent of a stress-reduction intervention such as the MBSR(BC) that we used in the present study. Kang et al. (2009) reported a similar recovery of NK cell percentages after BC treatment along with an increase in CD8+ T cells.
As a side note, several studies have reported lymphocyte recovery as percentages of lymphocytes (Kang et al., 2009) or as percentages of patients with recovery to or above baseline immune responses (Carlson et al., 2007) rather than as absolute cell counts. In our view, reporting percentages of immune markers among all lymphocytes in the absence of actual cell counts can be difficult to interpret and may be a source of inconsistent results across the literature.
Second, in terms of treatment regimen, our data suggest that RT alone confers immunosuppressive effects similar to those conferred by RT combined with chemotherapy. We found this to be the case independent of time since treatment completion, which we adjusted for statistically. Still, this result may require further study. While RT and chemotherapy are known to cause a decrease in circulating lymphocytes among BC patients (Mozaffari et al., 2009), our data are inconsistent with prior published data. Mozaffari et al. (2009) reported significantly lower lymphocytes after completion of treatment and out to 1 year among 21 BC patients who received RT + chemotherapy compared to 20 patients who received RT alone. The largest differences by treatment regimens were for CD4+ and CD8+ subsets and occurred as these markers generally increased (recovered) over time in the RT group but not in the RT + chemotherapy group. The explanation for the inconsistency with our results is unclear.
Third, with respect to stress-reducing interventions, we found a significant increase in PHA-induced T cell activation and the Th1/Th2 ratio in those patients enrolled in the MBSR(BC) program after 12 weeks since treatment completion. This finding suggests that MBSR(BC) confers some beneficial effects on immune recovery but only at a time somewhat removed from cancer treatment and immune depression.
Witek-Janusek et al. (2008) found no differences in %NK cells and CD+ subsets at any time point between the MBSR group and control group; however, 1 month post-MBSR intervention, the MBSR group had increased NK cell activity and IFN-γ and decreased production of IL-4 and IL-10 by activated peripheral blood mononuclear cells (PBMCs) compared to baseline and to the control group. The immune responses in the MBSR group were more similar to a cancer-free sample of women, suggesting normalization of immune dysregulation over time.
Similar to our findings, but in HIV-1-infected adults, Creswell et al. (2009) found sustained CD4+ T lymphocyte levels post MBSR, whereas the 1-day control intervention group showed declining levels of CD4+ T lymphocytes. The authors concluded that MBSR may help buffer CD4+ T lymphocytes decline in this population.
An obvious next step would be to examine the mechanism by which MBSR(BC) improves immune recovery. As a documented stress-reducing intervention (Kabat-Zinn, 1990), MBSR is likely to alter (lower) levels of the major stress hormones of the hypothalamic–pituitary–adrenal (HPA) axis, including glucocorticoids and catecholamines, which are responsible for unfavorably upregulating IL-10, IL-4, and transforming growth factor-beta (TGF-β) at the expense of inhibiting IFN-γ, IL-12, and tumor necrosis factor-alpha (TNF-α; Calcagni & Elenkov, 2006). Our study did not measure glucocorticoids and catecholamines before and after MBSR, making this a logical line of future inquiry.
No other studies testing MBSR have included measurement of intracellular Th1/Th2 responses or activated T cell responses, which is a measure of functional ability of T cells to respond to antigens. Other investigators have found contradictory effects of MBSR on numbers or percentages of immune cell recovery. Carlson, Speca, Patel, and Goodey (2003) found no significant changes in lymphocyte subsets (NK, T, or B cells) after an 8-week MBSR program but did find an unexpected decrease in IFN-γ and a corresponding increase in T cell production of IL-4. When the investigators followed these same participants out to 1 year, percentages (not absolute counts) of NK cells (CD65+) increased and then decreased and B cells (CD19+) increased, whereas percentage of T cells (CD3+), T-helper cells (CD4+), IFN-γ, and TNF all decreased over time (Carlson et al., 2007). Only one other study on the effects of MBSR on immune recovery in cancer included a randomized control group of a noncancer population (Creswell et al., 2009), and none of these studies controlled for the time since treatment.
Clinical Implications
Our data indicate that among BC survivors who have recently completed treatment, MBSR may facilitate recovery of T cell immune responses during this important transitional period. However, the clinical relevance of these findings is unknown. Activated T cell responses may provide some level of resistance against infection through better recognition of antigens and more robust activation of macrophages and differentiation of B cells and cytotoxic T cells. A major factor influencing the outcome of infections, particularly those from viruses and intracellular bacteria, is the shifting to a Th1 response and production of IFN-γ and other proinflammatory cytokines (Calcagni & Elenkov, 2006). BC patients have lowered immune responses, making them more susceptible to these pathogens (Campbell, Scott, Maecker, Park, & Esserman, 2005; Caras et al., 2004). The higher Th1/Th2 ratio associated with MBSR(BC) could, theoretically, increase tumor immunity (Schroder, Hertzog, Ravasi, & Hume, 2004). Thus, while speculative, our findings of improvements in T cell activity and a shift toward a Th1 phenotype with MBSR(BC) provide a rationale for long-term longitudinal follow-up of BC patients following MBSR and other evidence-based stress-reducing interventions.
Although our study population was heterogeneous, we believe that our results are generalizable to the BC population at large. Patients received RT, chemotherapy, and hormonal treatments consistent with recommendations in National Comprehensive Cancer Network (NCCN) guidelines, and treatment regimens were consistent with current clinical practice (National Comprehensive Cancer Network [NCCN], 2006).
Limitations
The primary limitation of this study is a lack of long-term follow-up after completion of cancer treatment (e.g., out to 1 year) to evaluate serial within-participant changes over time in lymphocyte counts and functional activity. To address this limitation, we examined between-participant variation in time since treatment completion in order to infer patterns of change in lymphocytes over time (i.e., natural history). Nonetheless, the ideal natural history design in order to minimize confounding is long-term serial measurement of the same participants. In addition, our sample size of the minority of patients who received accelerated (partial) breast irradiation therapy was not large enough to separately evaluate the effect of this therapy on lymphocyte recovery.
Conclusion
In summary, compared to a usual care control regimen, use of a 6-week MBSR(BC) program favorably increased T cell activity and the Th1/Th2 ratio among Stage 0–III BC patients who were more than 12 weeks removed from treatment. Our data indicate that B cells and NK cells are more susceptible than T cells to being suppressed by BC treatment irrespective of whether RT is paired with chemotherapy. Future studies require control for the timing of treatment. The net clinical impact of these observations warrants further investigation.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by the National Cancer Institute: grant number R21CA109168.