
Abstract
Caring, a core tenet of nursing practice, grew out of a holistic approach. Nurse theorists often note the establishment of a therapeutic relationship as the beginning point of caring, with subsequent nursing interventions reliant upon this relationship for effectiveness. Relational exchange serves as a source of either stress or healing between participants, and rarely is its impact neutral. Relational stress, in fact, has become a primary contributor to many disease processes in terms of promotion and progression and perhaps even initiation. Patient–provider relationships have a long history in medical and nursing literature as critical to providing effective interventions, but our understanding of relational dynamics between patients and providers remains fairly superficial. This theoretical article adapts a previously described biobehavioral model to illustrate the nature and centrality of caring relationships in nursing practice. The dynamic process of face-to-face engagement is deconstructed from a psychobiological standpoint in order to understand the physiological, emotional, cognitive, and behavioral impacts of relational interaction. This understanding is then applied to the patient–provider relationship. Finally, the utility of biomarkers of stress, positive emotion and resonance, and of disease is discussed relative to the patient-provider relationship. Methodological and interpretive challenges inherent in this line of research, along with suggestions to address such challenges, are also presented.
From the days of Florence Nightingale to the present, a holistic approach to health has informed nursing practice. From this value of holistic health, caring has emerged as a core tenet in nursing. Many have written and debated about caring, but there is a general consensus among nursing theorists and practitioners that the fundamental construct of caring lies in the qualities of intra- and interpersonal relationships. Relationships with patients, patients’ families, colleagues, administrators, the community, and oneself are the foundation of nursing care, with effective nursing interventions contingent upon the establishment of a therapeutic relationship. Recent developments from the field of neurophysiology validate that which nurses have sensed all along: The quality of our interactions with patients can impart direct biological health- or disease-promoting effects. Furthermore, the quality of the patient–provider relationship indirectly contributes to the success of interventions by altering perceptions of self-efficacy and social affiliation, influencing the development of depression and anxiety and of health-promoting behaviors. Caring, as a therapeutic construct, both motivates and is a consequence of health-promoting interactions. In this article, we present an adaptation of the extended biobehavioral interaction model, developed by Kang, Rice, Park, Turner-Henson, and Downs (2010), as a theoretical framework to guide thinking about how patient–provider relationships affect patients’ health. We also explain how this adapted model can inform biomarker research in nursing as a way to document and quantify the effects of relationships on health.
The Extended Biobehavioral Interaction Model and Its Relational Adaptation
The extended biobehavioral interaction model (Figure 1) comprises “clusters of psychosocial, behavioral, individual, and environmental factors that can individually and/or interactively influence biological (physiological) responses to shape health and health-related outcomes” (Kang, Rice, Park, Turner-Henson, & Downs, 2010, p. 736). The model incorporates three previously conceived models of stress: the physiological model of stress (Selye, 1974), the cognitive appraisal model of stress and coping theory (Lazarus & Folkman, 1984), and the stress, allostasis, and allostatic load model (McEwen, 1998, 2003). Combining the three models allows for the consideration, en masse, of adaptive processes, long-term cumulative effects of distress, and acute cumulative effects from multiple coexisting stressors occurring within a short period of time. The model emphasizes unidirectional and bidirectional causal relationships between clusters, as well as correlational associations between and within clusters where causality has not been established.
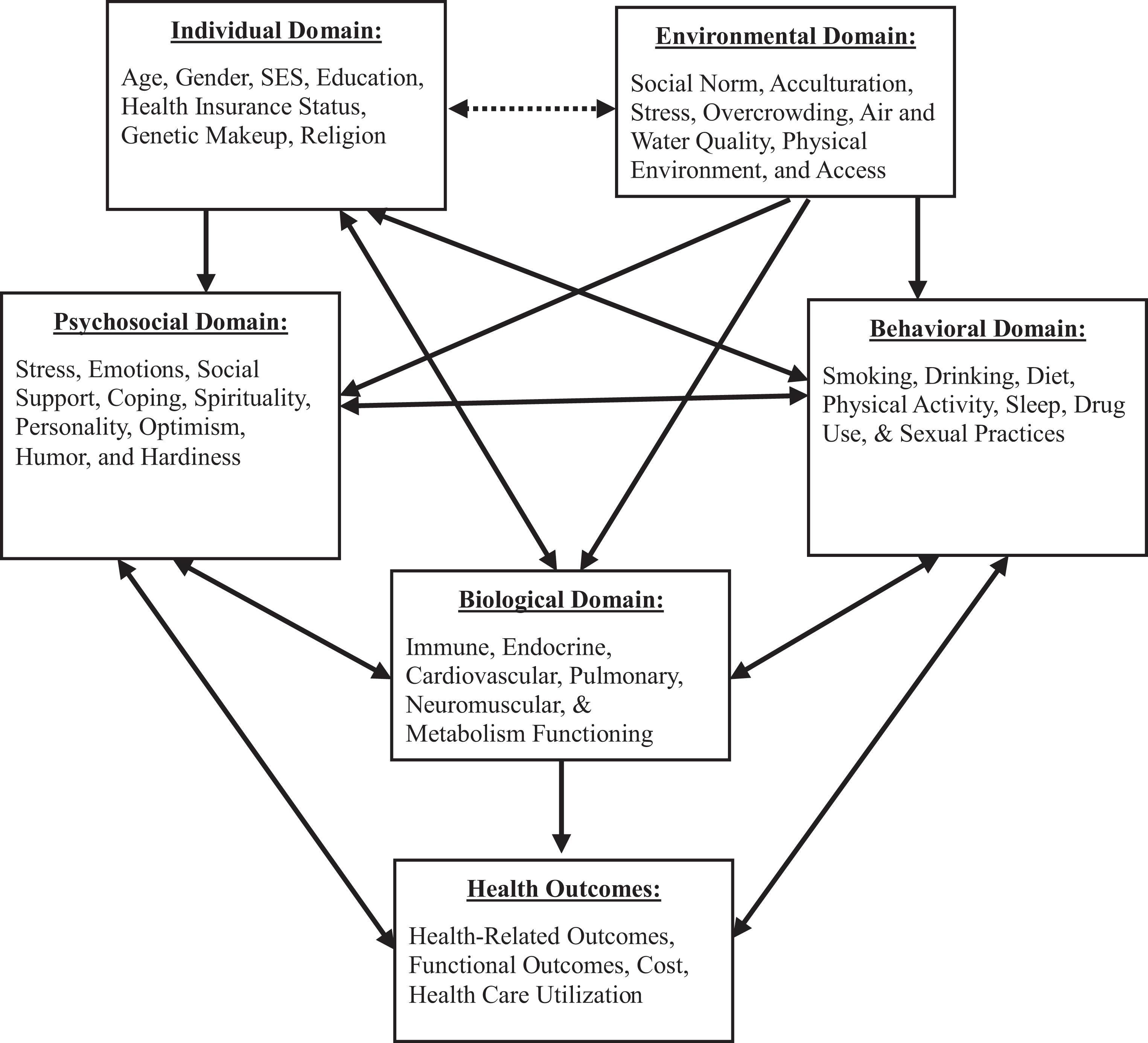
Extended biobehavioral interaction model. SES = socioeconomic status. This figure is an exact reprint of the model as first published in Kang et al. (2010). Copyright © 2010 by SAGE Publications. Reprinted by permission of SAGE Publications.
Kang et al. (2010) presented the relationship between distress (a psychosocial concept) and inflammation (a biological response) in cardiovascular disease (CVD), certain cancers, and chronic obstructive pulmonary disease (COPD) within this model. In this article, we propose adapting this model by inserting an additional cluster, relational domain, into the center of the diagram (see Figure 2). The addition of this domain provides a more complete conceptualization of individuals’ inseparability from, and dynamic interaction with, the moment-to-moment state of their environments. It also assists the researcher in planning a systematic approach toward understanding the associations among stress, inflammation, biomarkers, health outcomes, and relational interactions as they exist in a real-world, embedded context.
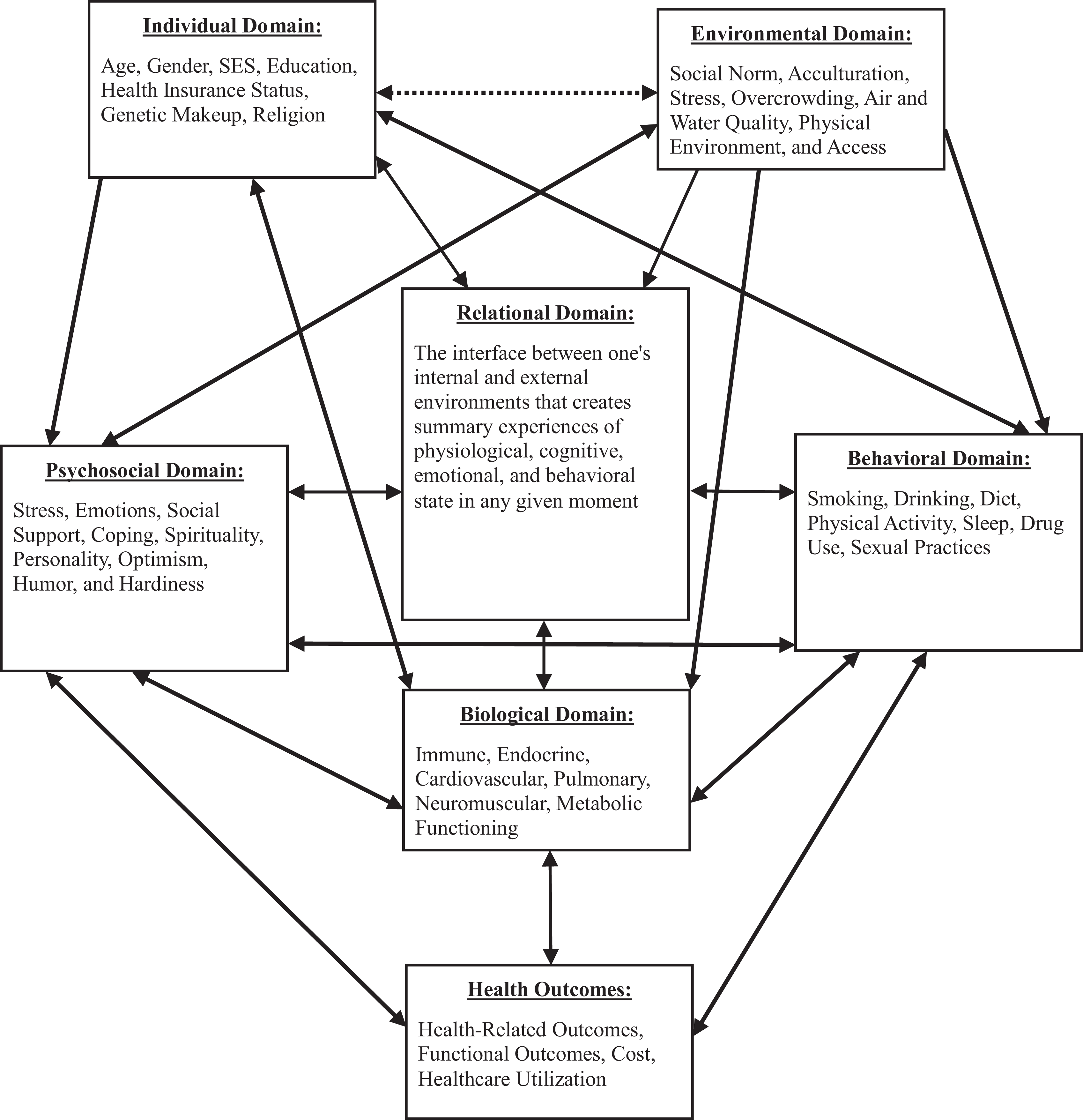
Adapted extended biobehavioral interaction model. This figure introduces an adaptation of the model presented in Figure 1 to include a relational domain. SES = socioeconomic status. Adapted from Kang et al. (2010). Copyright © 2010 by SAGE Publications. Adapted by permission of SAGE Publications.
We define the relational domain as the interface between an individual and his or her environment within which the mixing of beings occurs. One person’s relational domain mixes with another’s relational domain within a space that belongs to all the participants yet also belongs, ultimately, to none. It is a place of shared space and time that may be influenced by the participants and that profoundly affects, and is affected by, the participants’ many other domains. Relational healing transpires in the space created by the connection between the participants (Scott et al., 2008). Within the space of the relational domain, individuals perceive their environments, often unconsciously, as safe or unsafe, friendly or hostile, isolating or integrating, caring or indifferent. Ideally, this perception, termed neuroception (Porges, 2007) or interoception (Cameron, 2001), matches the degree of actual safety or threat contained in the environment (Kalisch, Wiech, Critchley, & Dolan, 2006). Neuroception occurs through our nervous system and is transduced into electrical (i.e., neural), chemical (i.e., endocrine), and biological (i.e., protein synthesis or other cellular activity) signals that provide physical, emotional, and mental experiences (Cameron, 2001, 2009). These sensed experiences are then formed (sometimes consciously, sometimes unconsciously) into behavioral responses, provoking further physical, emotional, and mental experiences.
Within the relational domain, the sensing of one’s environment results in an experience of physiological, emotional, mental, and behavioral states that is shaped by past experiences and actions and informs present actions and subsequent experiences (Immordino-Yang & Damasio, 2007). This summary experience, or “interaction entity,” occurs when components of the entity (physiological, emotional, mental, and behavioral) are bound together and stored in memory. Interaction entities exist as functional units and take on lives of their own as dynamic and emergent bodies, constantly responding to environmental changes. These entities are modified as learning processes, cognitive reappraisals, limbic/physiological regulation, and response expressions attempt to resolve the lack of integration inherent in emotional conflict, ambiguity, and unsuccessful behavioral responses (Etkin, Egner, & Kalisch, 2011; Siegel, 2009). An interaction entity is stored in memory until a similar stimulus enters the nervous system and reanimates it, linking new experiences with old and deepening learning, context, and coping in the process (Immordino-Yang & Damasio, 2007). The interaction entity is modified by this novel experience and stored in memory for future use. Interaction entities can be formed and reanimated through one’s own mental activity as well, indicating the importance of one’s intrapersonal relationship (i.e., relationship with oneself through one’s thoughts and behaviors).
The interaction entity is used to guide current and future behavioral responses, (unconscious) appraisal, conscious reappraisal, physiological regulation, learning, and adaptive behavior. It is our physiological state that sets limits on the possible range of behaviors and psychological experiences, which highlights the importance of effective physiological regulation in response to stressful situations (Porges, 2007). If we experience the interaction entity consciously, we may become mindful of the internal impact of the interaction and cognitively reinterpret the experience through intentionally engaging our mental processes (reappraisal; Etkin et al., 2011). Through mindfulness, we can loosen the influence of “top-down” mental constraints that prevent us from seeing with “fresh eyes” (Siegel, 2009). This awareness and interpretation yields a greater understanding of the event, helping us to make meaning from it, build resilience, and choose more effective and adaptive behavior (Garland, 2007). It is only through the fresh eyes of conscious awareness of our physio-cogno-emotional-behavioral state that our intention can inform a response. Even if we do not register the interaction entity consciously, the mind and body engage the experience, interpreting it, responding to it, and storing it in memory (Etkin et al., 2011).
Because the relational domain sits at the interface between one’s internal and external environments, many aspects of the other domains filter through the relational domain as one moves from one experience to another. Whereas genetic makeup (individual domain), smoking (behavioral domain), water and air pollution (environmental domain), and instrumental aspects of social support (psychosocial domain), for example, may exert direct influence upon the biological domain and health outcomes, many other factors (e.g., socioeconomic status [SES], acculturation, sleep, and coping) affect the biological domain indirectly as they move through the relational domain, exerting the forces of their history and context and being influenced themselves in return.
The Relational Domain in Perspective
In response to the modern-day epidemic of chronic illness, theoreticians, researchers, and clinicians have begun transforming their approach to health and sickness by decreasing the emphasis on a single agent–caused disease treated within a reductive and isolated context. Chronic illnesses often result from a multitude of causative factors that require equally numerous and diverse interventions, not to mention the further complexity of managing multiple comorbid chronic illnesses. We do not mean to imply that use of diagnostics and interventions obtained through technology and pharmacology should be diminished or discounted. Quite the contrary. Modern medicine is largely responsible for the dramatic increase in lifespan that has allowed us to live long enough to encounter chronic illness. However, it is the greater entity of health care, including all disciplines, payers, and administrators, that must continue in the tradition of medicine’s great innovations and adaptability by broadening the perspective through which we view and treat health and illness. A broader perspective invites context, individuality, embeddedness, and humanity into the health equation, maximizing efficacy of reductive interventions delivered within an empowering and non-isolating social environment.
Components of the Relational Domain
The components of the relational domain, which are summarized in Figure 3, are (1) contributors to relational quality, (2) relational quality itself, (3) psychophysiological consequences of relational quality, and (4) impact of relational psychophysiology on health outcomes. In order to explore each of these components more fully, it is helpful to understand the distinction between stress and distress, which we define in terms of the effect a particular challenge has on an individual. Stress is the activation of sympathetic, autonomic, and immunological systems toward adaptation to an environmental challenge that is not necessarily negative (Glaser & Kiecolt-Glaser, 2005; McEwen, 2005; Zingman, Hodgson, Alekseev, & Terzic, 2003). Research has established that some degree of stress is imperative to health and well-being, and short-term (less than 2 hr), resolvable stress stimulates physiological health and strengthens adaptive responses. Distress occurs when environmental demands exceed an individual’s perceived capacity to cope (Cohen, Janicki-Deverts, & Miller, 2007; Glaser & Kiecolt-Glaser, 2005). The point at which stress becomes distress is determined by the chronicity of the stressor, the degree to which it can be resolved, and the intensity of the stressor in relationship to one’s presumed capacity to cope (Glaser & Kiecolt-Glaser, 2005; McEwen, 2005).
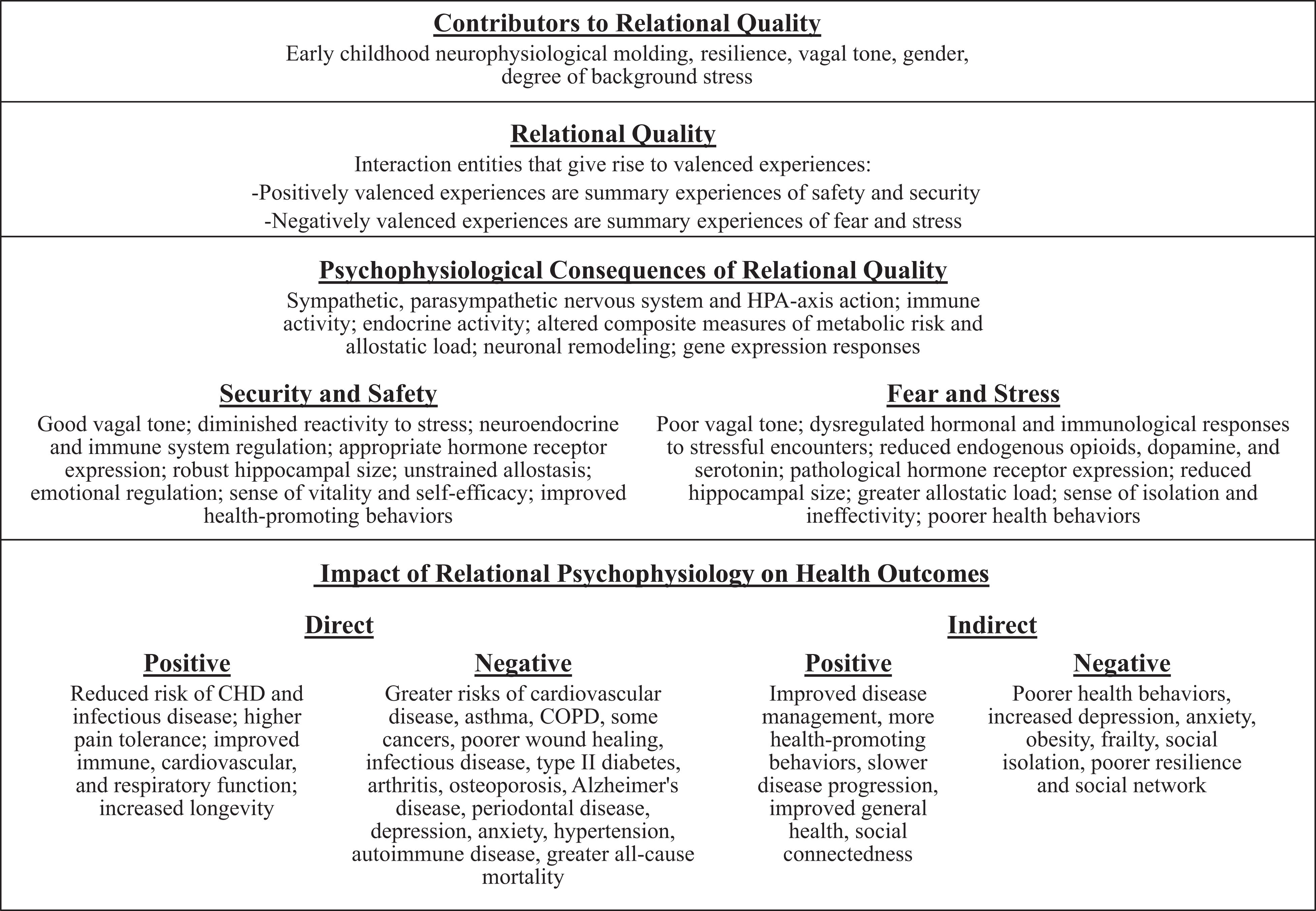
Components of the relational domain. This figure illustrates and defines the four components of the relational domain. CHD = coronary heart disease; COPD = chronic obstructive pulmonary disease; HPA = hypothalamic-pituitary-adrenal.
Contributors to Relational Quality
Factors that contribute to one’s capacity to relate include early childhood neurophysiological molding, resilience, vagal tone, gender, and the degree of background distress.
Early-childhood neurophysiological molding
Early life environments become biologically embedded, often increasing the impact of cumulative and prolonged distress (McEwen, 2010b). The infant’s early developing right hemisphere responds to the primary caregiver’s psychobiological regulation/dysregulation, modeling connections with the limbic and autonomic nervous systems and providing the foundation for the infant’s life-long stress response (Schore, 2001). The capacity of adults to relate socially, through hippocampal, prefrontal cortex, and amygdalar molding, begins in utero (Engert et al., 2010). Stress hormones modulate brain function by changing the number and structure of neurons (i.e., dendritic remodeling) and genomically driven sensitivity to sex and metabolic hormones (McEwen, 2010a). Early-life distress dynamically controls DNA methylation in postmitotic neurons, generating stable changes (epigenetic marking) in arginine vasopressin expression that lead to neuroendocrine and behavioral profiles consistent with depression in later years (Murgatroyd et al., 2009). Cold, neglectful, or uncaring caregiver interactions influence epigenetic regulation of hippocampal glucocorticoid receptor (GR) expression (Oitzl, Champagne, van der Veen, & de Kloet, 2010) and the development of a proinflammatory phenotype in adolescence (G. E. Miller & Chen, 2010). Roth, Lubin, Funk, and Sweatt (2009) presented evidence of an epigenetic molecular mechanism that potentially underlies lifelong, transgenerational perpetuation of changes in gene expression and behavior caused by early abuse and neglect. There is, however, also great diversity in individual responses to stress, both acute and chronic, despite early life histories.
Resilience
The ability to bounce back from distress is termed resilience (Smith, Tooley, Christopher, & Kay, 2010). Individuals’ degree of resilience varies enormously based on genetic endowment and early life experiences that capitalize on, or degrade, this endowment (Alfieri & Borgogni, 2010; McEwen, 2003). Biological resilience takes into account the multiple factors that interact in various ways within an individual and lead to multiple pathways toward adjustment or maladjustment, such as genetic, demographic, environmental, sex-linked, social, humoral, psychological, and functional factors (Alfieri & Borgogni, 2010; Calkins, Blandon, Williford, & Keane, 2007).
McEwen (2003) explained resilience in terms of the theory of allostasis. The term allostasis was coined to clarify ambiguities associated with the word stress and, most generally, is defined as “achieving and maintaining stability through change” (McEwen, 2005). Allostasis, then, is the dynamic systemic regulation where homeostatic control (regulation among separate processes necessary to maintain life, such as blood pressure, heart rate, etc.) is maintained by an active process of adaptation during exposure to physical and behavioral stressors (McEwen & Gianaros, 2010). Resilience in terms of allostasis refers to the structural plasticity of the brain and body, which includes neurogenesis, reversible dendritic remodeling, and downregulation of GRs that protects hippocampal nerve cells from permanent damage (McEwen, 2010a). Endogenous mediators of resilience, such as oxytocin, estrogens, steroids, and other hormones, genes, and dehydroepiandrosterone, also critically contribute to allostasis. Greater resilience is associated with greater resistance to the conversion of allostasis to allostatic load (i.e., the cost of adaptation, where acute responses to stress are overused or inefficiently managed, resulting in wear and tear on the body [McEwen, 2005]). Although early life experiences are one of the most important predictors of resilience and contributors to allostatic load, an individual’s present environment can reshape the brain and body structure and function toward adaptation (Logan & Barksdale, 2008).
Vagal tone
The vagus nerve is a critical structure that provides physiological and emotional experiences of social interactions. Extending from the brain stem to innervate the enteric nervous system, the vagus nerve is a nerve complex rather than a single nerve (Cameron, 2009). It is both afferent and efferent (both sensory and motor) and is central to the parasympathetic component of the autonomic nervous system, providing rapid continual feedback between the brain and the body for homeostasis and allostasis. Vagal afferents more strongly involve emotive (rather than sensory) aspects of pain and have low thresholds for activation. Vagal functioning can modulate (dampen) the sympathetic–adrenal stress response in threatening social circumstances, allowing for the possibility of peaceful conflict resolution, affiliation, and interpersonal connection (Porges, 1997, 2007). The “smart vagus,” a myelinated vagal branch, supports sustained social contact in the mid of a conflictual situation through applying the "vagal brake." By exerting inhibitory, modulatory, or calming influences on sympathetic arousal, the vagal brake makes the flow of intense social interaction possible without activating the fight-or-flight response. Such positively valenced interactions provide energy, motivation, and clarity (Curtis & Cicchetti, 2003; Jordan, Hartling, & Walker, 2004; J. B. Miller, 1986; Porges, 2007). The threshold at which the smart vagus is triggered to regulate the heart and other organs, known as vagal tone, varies greatly among individuals (Porges, 1998, 2007). A person with poor vagal tone has difficulty suppressing emotions, making engagement difficult. Poor vagal tone is characterized by emotional dysregulation, physiological hyperreactivity to environmental and visceral stimuli, and social withdrawal behaviors. Vagal tone is likely formed in infancy and early childhood relative to attachment insecurity with a caregiver, individual temperament, and genetic makeup (Porges, 1997).
Gender
Gender also contributes to relational quality through hormone-driven neurological modeling and physiological stress responses. Hippocampal neurons possess receptors for estrogens and androgens, making this structure highly plastic during sexual differentiation and later adult life (McEwen, 2010a). The prefrontal cortex and hypothalamus also demonstrate differential structural molding based on steroidal regulation. Steroid hormones regulate gene expression both directly and indirectly, imparting gender differences in neuroprotection after strokes and seizures and in cognitive functioning such as learning and memory (McEwen, 2010a). Taylor and colleagues proposed a gender-based distinction in the affiliative neurocircuitry in women to “tend and befriend” in times of relational absence or distress rather than to “fight or [take] flight” (Taylor, 2006; Taylor et al., 2000). This gender difference arises through the action of the hormones oxytocin in women and vasopressin in men, as well as through opioid and dopaminergic pathways (Taylor, Saphire-Bernstein, & Seeman, 2010). “Tend and befriend” is a human stress response to affiliate for protection and adaptation when threatened or stressed (Taylor, 2006).
Chronic background distress
Chronic background distress modifies the way one’s physiology responds to acute stressors. Episodic stress, when encountered in the mid of chronic interpersonal distress, accentuates cortisol output and reduces expression of GR mRNA, leading to wear and tear on the body (G. E. Miller & Chen, 2006). Conversely, exposure to episodic stress within a supportive environment toughens the body and protects it against subsequent stressors (Marin, Martin, Blackwell, Stetler, & Miller, 2007). Chronic distress is cumulative. Poverty thus affects stress regulation through cumulative risk exposure (such as substandard housing, and family turmoil; Evans & Kim, 2007). Women with one or more first-degree relatives with breast cancer demonstrate higher cortisol responses to work distress than do women without a family history of breast cancer (Dettenborn et al., 2005). Illness, particularly chronic illness, is another example of chronic background distress. “Personal injury or illness” ranked sixth on a list of stressors’ relative impact on respondents’ lives in one study (Holmes & Rahe, 1967). Chronic medical illness can force a patient to reexamine self-perceptions, often requiring a permanent reconceptualization of the self (Groves & Muskin, 2005). Such identity crises can provoke anxiety, disorientation, and a sense of isolation. Pain, sleep disturbances, disability, and job loss can also contribute to an illness being experienced as stressful. When the stress of a medical encounter occurs amid the background distress of a chronic illness, the chances of physiological dysregulation during the encounter increases, altering the patient’s capacity to interact effectively, assimilate new information, share in decision making, remember instructions, and adhere to recommendations.
Relational Quality
Relational quality is the experience of an interaction entity in terms of its valence. By valence, we mean the attractiveness (positive valence) or aversiveness (negative valence) of an event or situation (Frijda, 1986). In this article, we define positive valence as interactions that yield summary experiences of safety and security and negative valence as interactions that yield summary experiences of fear or distress. Relational quality hinges on its contributors (described in the previous section), which limit the possible outcomes of an interaction based on an individual’s physiological state (Porges, 2007). Individuals experience relational quality within the relational domain through the active (as opposed to latent) interaction entities previously described.
Relational interaction refers to the alchemical processes (Holmyard, 1990; Jung, 1970) that occur between and within individuals. 1 The mere presence of another being in the room alters us (Uchino, Cacioppo, & Kiecolt-Glaser, 1996). We transmit and mingle our essential selves when we relate to each other, altering the other and becoming altered ourselves in the process. Our anatomical and physiological makeup is designed for relational engagement (Cozolino, 2006). Wide variations in individual capacities and interest in engagement exist, and engagement occurs on many different levels. But it is this momentary mixing of beings that is the central feature in the relational domain that impacts our health and well-being.
Psychophysiological Consequences of Relational Quality
It is the body’s stress system that orchestrates the response of the body and of the brain to the environment (Goldstein & Kopin, 2007). Based on whether interactions are perceived as safe and secure or fearful and distressing, specific consequences to one’s psychophysiology ensue. Although we separate positively and negatively valenced experiences into exclusive categories for the purpose of simplification, in actuality experiences are often bivalenced, where both positive and negative appraisals are activated simultaneously. Activating both systems at the same time does not nullify, void, or neutralize the experiential outcome but rather often leads to agitation, indecision, and ambivalence. Each response system has distinct neural circuits (receptors and sensory afferents, separate spinal interneuron circuits, and distinct motor neuron pools), which are independent of one another, though they do interact (Howell, Kern, & Lyubomirsky, 2007; Norman et al., 2011). Psychophysiological indices of both systems include sympathetic nervous system and hypothalamic-pituitary-adrenal (HPA)-axis activity, immune processes, endocrine functioning, composite indicators of metabolic risk and allostatic load, neuronal remodeling, and gene transcription responses.
Security and safety
Experiences of safety and security invoke psychophysiological activity that may be independent of, or coactive with, negatively valenced appraisals. Positively valenced experiences are not merely the absence of negativity or distress and do not necessarily exist as polar opposites on the same continuum. Positive appraisals have neurobiological correlates that are distinct from negative appraisals and can benefit health (Howell et al., 2007; Nelson & Cooper, 2005; Norman et al., 2011). Steptoe, Dockray, and Wardle (2009) reviewed the biological consequences of positively valenced affect states. Lower cortisol levels exist in people with higher levels of positive affect, independent of gender, age, SES, body mass index, smoking, ethnicity, waist/hip ratio, employment status, time of waking, psychological distress, and depression (Steptoe, Wardle, Marmot, & McEwen, 2005). Likewise, a higher cortisol awakening response (CAR; indicative of an excessive stress response) followed by a slower rate of recovery to baseline correlates with lower amounts of positive affect. Daily positive emotions “undo” cardiovascular activation following day-to-day experiences of negative emotions in older adults, lending support to the idea that positive emotions broaden and build enduring resilience to negative emotional experiences (Fredrickson, 2004; Ong & Allaire, 2005). Positive emotions can also aid recovery from the negative cardiovascular effects of negative emotion (increased heart rate and blood pressure), enhancing coping (Tugade, Fredrickson, & Feldman Barrett, 2004).
Positive affect is associated with increased cellular immune competence in the form of natural killer cell cytotoxicity (Lutgendorf, 2001). Greater antibody response to hepatitis B vaccination is associated with trait-positive affect. Researchers have also noted inverse associations between positive affect and plasma interleukin-6 (IL-6) and C-reactive protein concentration in women (Steptoe, Gibson, Hamer, & Wardle, 2007). IL-6 levels also show inverse associations with other positive affective resources, such as purpose in life and positive relationships (Friedman, Hayney, Love, Singer, & Ryff, 2007).
Fibrinogen, one of the main constituents of vascular thrombi, is a biological measure relevant to both inflammation and hemostasis. Fibrinogen influences CVD through its effects on blood viscosity, cell proliferation, and platelet aggregation (Rauch et al., 2001). Researchers have observed inverse associations between fibrinogen stress responsivity and positive affect, with less happy participants mounting substantially larger fibrinogen stress responses than the happiest group (Steptoe et al., 2005). Fibrinogen stress responsivity is also more prolonged in people with low positive affect.
Neurotransmitters, hormones, and opioids in the brain are often elevated in people experiencing positive affect. Physiological activation of dopamine, oxytocin, vasopressin, endorphins, and serotonergic compounds soothes the vagal system and structurally shapes the brain and body to seek and succeed in prosocial behavior (Porges, 1997; Taylor, 2006; Taylor et al., 2000; Uvnas-Moberg, 1997). Positive social interaction modulates neuronal damage, inflammation, and corticoid steroid secretion—three important determinants of disease progression and long-term outcomes (Karelina & DeVries, 2011).
Fear and distress
Researchers have been intensely interested in the human stress response for the past half century and have paid particular attention to social distress, including poverty and social isolation, as a primary stressor of contemporary Western society (Karelina & DeVries, 2011; Sapolsky, 2005, 2010). Chronic psychosocial distress, and acute distress in the midst of chronic distress, can tax the body's adaptive ability beyond its capacity, leading to adverse health outcomes (Cacioppo et al., 2000). Psychophysiological responses to stress differ based on the severity and chronicity of the stressor and whether it is perceived as a threat or a challenge (McEwen, 2005).
Cortisol and cytokine responses to acute laboratory stressors are most pronounced in situations of social threat, such as threats to social standing or potential rejection or social isolation (Dickerson, Gruenewald, & Kemeny, 2009). Delayed cortisol recovery predicts increased blood pressure and impaired clotting processes and contributes to subclinical atherosclerosis (Steptoe & Marmot, 2006). Severe and stable social distress can also lead to both immunosuppression and chronic systemic inflammation (G. E. Miller, Chen, & Cole, 2009). Social relationships impact intracellular signaling mechanisms (e.g., C-reactive protein, cytokines, etc.) and inflammatory biomarkers, which have been observed across the lifespan in both healthy and ill participants (Kiecolt-Glaser, Gouin, & Hantsoo, 2010). IL-6, a proinflammatory cytokine, promotes the production of C-reactive protein, an important predictor of coronary heart disease, and both compounds are related to psychosocial factors such as chronic distress, social isolation, and childhood adversity (Danese, Pariante, Caspi, Taylor, & Poulton, 2007; Loucks, Berkman, Gruenewald, & Seeman, 2006).
Depression and anxiety, which both result from and contribute to chronic distress, show consistent physiological relationships with systemic inflammation; dysregulated sympathetic, autonomic, and parasympathetic activity; altered brain chemistry, and reduced hippocampal volume (Kiecolt-Glaser et al., 2010; McEwen, 2008; Sapolsky, 2004). Other negative emotions, such as fear, disgust, and anger, narrow individuals’ capacity to consider the broader range of actions they might take (e.g., to play, explore, savor, and integrate; Fredrickson, 2004), with the narrower range of negative action tendencies (fight, flee, expel, attack) often triggering autonomic activity. Even the anticipation of negative emotion can trigger a narrowing of focus so that a person will avoid incorporating new information (Baumeister, Vohs, DeWall, & Zhang, 2007). Researchers have shown that the experience of shame specifically, elicits increases in proinflammatory cytokine activity, an immunological marker of inflammatory processes (Dickerson, Kemeny, Aziz, Kim, & Fahey, 2004). Certain proinflammatory cytokines can exert central effects that lead to reduced exploratory behavior and social disinterest in humans and animals, perhaps explaining the observation that disengagement is a prime attribute of shame (Dickerson et al.,2004; Kemeny, 2009).
McEwen (1998, 2003) described the cost of adapting to distress as allostatic load. Allostatic load is the consequence of allodynamic regulatory wear and tear on the body, which promotes ill-health and involves not only consequences of the stressful experiences themselves, but also the changes in lifestyle resulting from a state of chronic distress (McEwen & Gianaros, 2010).
Impact of Relational Psychophysiology on Health Outcomes
The greatest indicator of the importance of relationships to health rests, ultimately, in their impact on health outcomes. As discussed above, negatively valenced relational interactions are associated with inflammatory and HPA-axis activity. Recent research implicates the inflammatory process as critical to many disease processes including CVD, type 2 diabetes, Alzheimer’s disease, asthma, arthritis, osteoporosis, periodontal disease, infectious disease and wound healing, with inflammation reliably predicting increases in all-cause mortality in older adults (Kiecolt-Glaser et al., 2010). Inflammation promotes CVD by altering endothelial functioning. In type 2 diabetes, inflammation reduces insulin signal transduction, thereby impairing blood sugar control. Most cancers are thought to have an inflammatory component due to the ability of inflammation to facilitate tumor promotion, survival, proliferation, invasion, angiogenesis, and metastases. In addition, cortisol interacts with inflammatory activity in a range of chronic diseases, including type 2 diabetes, hypertension, coronary heart disease (CHD), depression, and autoimmune conditions (McEwen, 2007; Raison & Miller, 2003; Steptoe, Dockray, & Wardle, 2009). High levels of circulating IL-6 predict future CHD and type 2 diabetes and are related to obesity, depression, and frailty in older adults (Papanicolaou, Wilder, Manolagas, & Chrousos, 1998).
On the positive side, positive affect is associated with reduced risk of CHD (Boehm, Peterson, Kivimaki, & Kubzansky, 2011). It also has significant associations with healthy behaviors such as exercising regularly, not smoking, and eating a healthy diet; with protective psychosocial factors such as greater social connectedness, perceived social support, optimism, and preference for adaptive coping responses; and with improved immune functioning, higher pain tolerance, and decreased endocrine system response (Howell et al., 2007; Steptoe et al., 2009). Additionally, positive affect promotes increased longevity and improved general health and cardiovascular and respiratory functioning. Slower disease progression and longer survival in chronic illness are other benefits of positive affect and well-being (Howell et al., 2007). Indeed, positive affect may be part of a broader profile of psychosocial resilience that reduces risk of adverse physical health outcomes (Steptoe et al., 2009).
Implications for Patient–Provider Relationships
Researchers have proposed that the relationship between provider and patient can impart lasting biological healing effects, even after only one visit (Adler, 2007; Clark, 2003; Jensen, Bäck-Pettersson, & Segesten, 1993; MacLeod, 1994; Suchman & Matthews, 1988; Summers, 2002). How can this be? After all, nearly all studies of the health effects of relationships focus on intense and/or regular interactions over long time frames, such as between spouses or within a psychotherapeutic setting. Contact with a primary care provider is often sporadic and sometimes short term, especially as practice settings adopt approaches where practitioners work in groups and share patients. We propose that such healing occurs within the shared relational domain of the patient and provider, as illustrated in the adapted expanded biobehavioral interaction model we presented above.
As we described above, the mechanisms through which the quality of the patient–provider interaction promotes healing are allostatic and affect (emotional) regulation. Such interactions quiet (regulate) an activated autonomic nervous system, which is physiologically healing, and form a bond between patient and provider based on their shared goals. One further mechanism of therapeutic interest is cognitive appraisal/reappraisal. Cognitive reappraisal is a conscious reframing of an event or situation that alters one’s perception of that event or situation. Reappraisals are mental activities characterized by changes in the nature of self-talk. In order for reappraisal to be therapeutic, mindful awareness of current appraisals and self-talk must exist (Garland, 2007). Patients and practitioners, together, may be able to discover cognitive appraisals that are hindering progress toward healthful action. In these cases, it is recognition of the interaction entities of their patients on the part of practitioners that allows the patient to create a more constructive reappraisal (Etkin et al., 2011). Mental (cognitive) activity is a significant source of distress for many people and is an important route through which interventions can improve emotional and physiological patterns and health. These biological and cognitive mechanisms provide experiences of safety or distress, which, in turn, determine a patient’s ability to attend to, think about, and act on his or her own behalf. Thus, face-to-face encounters, which exist within the relational domain, can be instrumental in promoting or inhibiting the extent to which a physical or pharmacological intervention is effective (van Dulmen & Bensing, 2002).
Biomarker Use in Relational Aspects of Nursing Research
Biomarker research focused on the effects of social relationships on health and disease include correlational, observational, and experimental study designs (Kiecolt-Glaser et al., 2010). Researchers have also incorporated biomarkers in population-based studies to understand the effects of SES on disease disparities (Seeman, Epel, Gruenewald, Karlamangla, & McEwen, 2010; Worthman & Costello, 2009). Nursing research can also employ biomarkers to clarify understanding of functional aspects of the relational domain within the patient–provider relationship. The basic hypothesis informing this approach is:
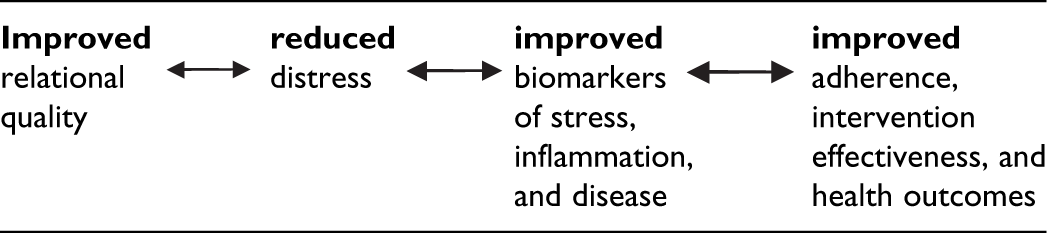
This sequence illustrates a bare bones conception of this approach in order to focus attention on the effects relational consequences have on biology and health. Researchers must incorporate the entire adapted expanded biobehavioral interaction model, however, in the execution of a research study to account for the complexity of disease and healing.
The main challenge in designing effective studies in this area lies in quantifying relational valence (security vs. distress) as a naturally occurring independent variable. In a laboratory or office setting, investigators can induce and manipulate positive and negative relational interactions. While such methods may be a good starting point, they do not capture authentic patient–provider interactions, which arise naturally and may be affected by contextual factors from the other domains. How, then, can researchers identify cohorts naturally and consistently displaying positive or negative relational interactions? Do such cohorts even exist, given the individual diversity that occurs within stereotyped groups? Perhaps the only way to quantify relational interaction is by defining patient exposure (relational resonance vs. disconnection) based on patient satisfaction scores and then artificially delineating cutoff points or comparing extremes from Likert-type assessment scales to biomarker measures.
Further challenges for this approach include the time conundrum and issues of causality and relevancy. How can we link biomarker measures during a single interaction to health outcomes? How do we know changes in biomarker measures relate to the interaction in question? Do/does our biomarker/biomarkers of choice accurately reflect the degree of stress, inflammation, or disease in relation to the “dose” or strength of valence of a given relational interaction? What is the half-life of any given relational interaction, as individual variation in biological responsiveness and recovery may confound or nullify any discernible effects? How can we isolate the physiological effects of relational interaction from the physiological “noise” resulting from the rest of life’s activities?
Given these important issues, we propose the use of a “variable focus” framework (Steptoe et al., 2009) to explore the biological/physiological effects of the patient–provider relationship in a way that reflects the degree of magnification through which we view the interaction. For instance, a zoomed-in focus may detail a specific interaction and include physiological, cognitive, and emotional measures based on that interaction. Biomarkers appropriate for this approach include those indicative of immediate and short-term physiological reactivity, such as cortisol, HPA-axis compounds, immunological measures, and markers of vagal functioning as well as assessment of recovery rates and differential degrees of reactivity in relation to background stress levels, stress level of the encounter in question, and embedded factors born during the childhood years. Within this focus level, more specific aspects of relational interactions may also be investigated, such as experiences of shame, objectification, empathy, and humor and effects of cognitive reappraisal. A mid-distance focus might investigate multiple interactions between the same dyad over time. Biomarkers conducive to this approach include composite measures indicative of allostatic load and biomarkers of disease. A zoomed-out focus might investigate interventions targeted at increasing relational capacity or social integration or fostering resilience. Biomarkers useful to this avenue of study include repeated measures of allostatic load, markers of disease, and brain imaging (e.g., changes in hippocampal size).
The adapted expanded biobehavioral interaction model provides a framework for research design by accounting for the multitude of confounding variables that may mask, mediate, or moderate the true effects of the relationship in question. For instance, researchers must collect demographic information, personal and familial health history, health behaviors, medication use, environmental factors (place of residence and work), job satisfaction, current familial context and environment, social network, and childhood environment since all these domains impact interactions within any given health care encounter. Furthermore, remembering that “it takes two to tango” elevates the biobehavioral profile of the providers to a level of significance as well, for they, too, bring their past to the relationship. Studying provider distress as it influences relational quality at work, as quantified through measurement of biomarkers, may be yet another avenue of interest for nurse researchers.
Biomarker research in patient–provider relationships is a complex and ambitious undertaking, requiring the best that translational research has to offer. However, given the recent explosion of information regarding the physiologically embedded social nature of humans and the increasing awareness of the importance of social interaction, it is a task worth the time, money, and effort it will take. The adapted expanded biobehavioral interaction model can provide a framework for such research. Through a systematic and scientifically sound approach, we may deepen our understanding of, and further validate, the power of caring that is so basic to nursing practice.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.