
Abstract
Objective:
To describe the prevalence rate of ideational apraxia (IA) affecting self-feeding in people with dementia, confirm the stage of dementia at which IA most commonly occurs, and compare mealtime performance and nutritional status between people with dementia (PWD) with and without IA.
Method:
A cross-sectional design with between-subject comparison was used. Among the 395 potential participants recruited from dementia special care units at nine long-term care facilities in central and northern Taiwan, 98 met the operational definition of IA and were included in the PWD with IA group. From the remaining pool, 98 participants, matched for age and sex with the PWD with IA group, were randomly allocated to the PWD without IA group. Eating Behavior Scale (EBS) scores, food intake, total eating time, meal assistance, body mass index, Mini-Nutritional Assessment (MNA), and Mini-Mental State Examination scores were collected.
Results:
The prevalence rate of IA affecting self-feeding in our study population of PWD was 24.8%. PWD with IA had significantly lower EBS scores, had more food intake (p < .001), spent more time being fed by caregivers, needed more verbal and feeding assistance, and had lower MNA scores than PWD without IA. Decline in the self-feeding ability of PWD affected by IA most commonly occurred in the severe stage of dementia.
Conclusion:
When dementia progresses to the late stage, staff should pay special attention to residents’ mealtime performance and nutritional status. For PWD with IA, reassigning staff at mealtimes based on eating ability and providing memory training are recommended.
Ideational apraxia (IA) is a commonly described symptom in people with dementia (PWD). It is defined as the inability to conceptualize, plan, and execute a complex sequence of motor actions involving the use of tools or objects, in spite of adequate muscle power, sensation, and coordination (LeClerc & Wells, 1998). Emerging evidence shows that approximately 51–54% of PWD are affected by IA (Del Ser, Hachinski, Merskey, & Munoz, 2001; LeClerc, Wells, Sidani, Dawson, & Fay, 2004). There has been a lack of consensus over the stage of dementia at which IA occurs most commonly, with a number of researchers believing that IA occurs relatively late in the course of dementia (Rapcsak, Croswell, & Rubens, 1989), whereas others believe that it manifests in the early or middle stages (Benke, 1993; Derouesne, Lagha-Pierucci, Thibault, Baudouin-Madec, & Lacomblez, 2000; Dumont, Ska, & Joanette, 2000). PWD with IA show content errors, most frequently including omission, misuse, and mislocation, resulting from the sequential disorganization of multiple-step tasks and disturbances of single-tool use (De Renzi & Lucchelli, 1988; Poeck, 1983; Zadikoff & Lang, 2005). Therefore, PWD with IA have difficulty performing everyday self-care activities, including self-feeding using a utensil.
Authors have described several common mealtime difficulties in PWD who exhibit IA, for example, they may mix foods together inappropriately, perform actions in an improper sequence, use utensils inappropriately, not begin to eat when a meal tray is placed in front of them, or try to eat food that is still in wrappers or inedible objects (LeClerc et al., 2004; Keller, Gibbs-Ward, Randall-Simpson, Bocock, & Dimou, 2006). Further, mealtime performance may affect nutritional status. The majority of prior investigations examining meal preparation and eating ability in people with IA focused on stroke patients with hemisphere damage (Foundas et al., 1995; Poole, Sadek, & Haaland, 2011). Although LeClerc, Wells, Sidani, Dawson, and Fay (2004) studied the eating abilities of PWD with IA, established the Feeding Abilities Assessment (FAA), and reported on its reliability and validity, they did not explore the specific impact of IA on eating ability and its consquences (e.g., mealtime performance or nutritional status). The study was also limited by its small sample size and lack of a control group. The objectives of the present study were (1) to describe the prevalence rate of IA affecting self-feeding in PWD, (2) to compare cognitive function between PWD with and without IA and confirm the stage of dementia at which IA most commonly occurs, and (3) to compare mealtime performance (e.g., eating ability, food intake, eating time and meal assistance) and nutritional status between PWD with and without IA. To avoid a limitation of previous research, we utilized a larger sample for the present study.
Further, to better isolate the effects of IA, specifically, in this population, we investigated the differences between the two groups of PWD regardless of the severity of semantic memory impairments. For people in the early stage of dementia, semantic memory (stored semantic knowledge) is moderately impaired (Simard & van Reekum, 1999). The severity of the semantic deficit is significantly related to the ability to use a tool or object (Silveri & Ciccarelli, 2009). Accordingly, when semantic memory is moderately or severely impaired, PWD should be unable to deal with tools or objects with which they were previously familiar. However, some PWD suffering from semantic deficits are able to correctly perform everyday actions. Pilgrim and Humphreys (1991) proposed that there is more than one cognitive route for eliciting an action: (1) an indirect route involving access to the semantic memory and (2) a direct route that bypasses semantic knowledge and directly connects visual representations of tools or objects to associated motor actions. Silveri and Ciccarelli (2009) hypothesized that preserved procedural memory in PWD might account for their ability to use tools or objects. PWD may activate visuomotor information (the domain of procedural memory) derived from the physical characteristics of the tools or objects to connect them with an associated motor scheme (a direct route), even if access to semantics is impaired.
Material and Method
Design
A cross-sectional design with between-subject comparison was used. After age and sex matching, the cognitive function, mealtime performance (e.g., eating ability, food intake, total eating time and meal assistance), and nutritional status of PWD with IA were compared with those of PWD without IA. All data were collected by six research assistants who had taken a 16-hr training course on dementia and related assessment tools and a 7-day clinical practice.
Participants
We recruited participants from dementia special care units at nine long-term care facilities in central and northern Taiwan. Participants met the following inclusion criteria: (1) a recorded diagnosis of dementia on their charts, (2) at least 1 month of residency in the facility, and (3) the ability to speak Chinese or Taiwanese. Participants who had visual or hearing difficulties, upper limb impairments, a history of stroke, nasogastric feeding tubes, or brain trauma were excluded from this study.
Participants who scored ≥1 on Section 1 of the FAA were classified as PWD with IA. These participants had lost some or all of their ability to perform a complex series of eating actions. Participants who scored 0 on the FAA were classified as PWD without IA. Of the 431 eligible participants, 36 were excluded because of refusal, hospitalization, or death during data collection. Of the remaining 395 participants, 24.8% (98 of 395) were classified as PWD with IA. We randomly selected age- and sex-matched participants from the remaining sample (n = 297; three age categories: ≤74 years, 75–84 years, and ≥85 years) to create the PWD without IA group. We analyzed data for a total of 98 pairs of patients (PWD with IA vs. PWD without IA).
Ethical Considerations
We obtained approval for this study from the Institutional Review Board of a medical center in Taiwan. In the beginning of the study, the principal researcher explained the purpose and procedures to the institutions’ managers, participants, and participants’ family members. Participants and family members were told that they could refuse to continue participation at any time, refusal would not affect the quality of care in the institutions and their privacy would be respected and protected. Before data collection, we obtained written informed consent from family members or guardians.
Measures
FAA
LeClerc and Wells (1998) developed the FAA to examine the abilities affected by IA in PWD during mealtime. The instrument consists of two sections: (1) an assessment of the presence or absence of the ability to initiate, follow through, and sequence the complex motor actions required for self-feeding and to use tools appropriately (7 items) and (2) an assessment of the type and amount of required nursing interventions corresponding to an individual’s current level of ability (LeClerc & Wells, 1998; LeClerc et al., 2004). The responses for all items on the FAA are yes (0) for retained abilities and no (1) for lost abilities (LeClerc et al., 2004). We used Section 1 of the FAA to classify participating PWD into the two comparative groups in the present study. The internal consistency reliability (Cronbach’s α) for the FAA subsections and total scale varied from .88 to .99 (LeClerc et al., 2004). The test–retest reliability (Pearson’s correlation coefficients) of Section 1 of the FAA and the interrater reliability (κ coefficients) of all FAA items were .99 and .98, respectively (LeClerc et al., 2004). In terms of content and construct validity, the FAA, with a content validity index of 0.80, could significantly differentiate between PWD and people without dementia (LeClerc et al., 2004). Lin, Chiu, and Chang (2006) translated the original FAA into Chinese and obtained good internal consistency reliability (Cronbach’s α = .99) on 93 residents with dementia. In the present study, the interrater reliability (intraclass correlation [ICC] coefficient) of the Chinese version of FAA Section 1 for all research assistants was 1.0.
Eating Behavior Scale
The Eating Behavior Scale (EBS) measures the ability of PWD to perform eating tasks (Tully, Matrakas, Muir, & Musallam, 1998). The tool assesses six types of sequential eating behaviors, including initiation, maintenance of attention, ability to locate food; appropriate use of utensils; ability to bite, chew, and swallow without choking; and termination of the meal. The assessor must determine whether the behaviors arise independently (3 points), with verbal prompts (2 points), with physical assistance (1 point), or completely dependently (0 point). Total EBS scores range from 0 to 18, with higher scores indicating better eating abilities. The tool has been reported to have a content validity index (CVI) of 1.0 and an interrater reliability (percentage agreement) of 95.9% (Tully et al., 1998). Additionally, the EBS score has been negatively correlated with the length of mealtime (r = −.66, p < .001) and positively correlated with Mini-Mental State Examination (MMSE) score (r = .82, p < .001; Tully et al., 1998). Lin et al. (2006) translated the original EBS into Chinese and reported internal consistency and reliability (Cronbach’s α) of .94 on 124 residents with dementia. The interrater reliability (ICC value) of the Chinese version of EBS for all research assistants in the present study was .99.
Food intake
After participants finished a meal, research assistants estimated and recorded the proportion of the meal participants had finished. For example, if a participant had four types of food on the meal tray, accounting for 80% of a meal and a bowl of rice accounting for 20% of a meal and ate all of two types of food and a half bowl of rice, a food intake of 50% would be recorded. A food intake estimate of over 75% for a meal was defined as “eating a full meal” (Reed, Zimmerman, Sloane, Williams, & Boustani, 2005). The interrater reliability (ICC value) of food intake estimates for all research assistants in the present study was 1.0.
Total eating time
Research assistants used a stopwatch to measure total eating time during a meal for each participant, beginning the watch when a meal tray was placed in front of the participant and stopping it when the meal tray was removed or the participant left the dining table. Research assistants recorded the amount of time participants spent self-feeding and the amount of time participants were fed by caregivers during the meal. The interrater reliability (ICC value) of eating time measures for all research assistants was 1.0.
Meal assistance
Research assistants observed and recorded the total number of meals in which each participant received verbal assistance, physical assistance, or feeding by caregivers. The interrater reliability (ICC value) on observations of meal assistance for all research assistants in the present study was .95.
MMSE
The MMSE is widely used in clinical settings to quantitatively detect cognitive changes over time and with treatment (Folstein, Folstein, & McHugh, 1975). The Chinese version of the MMSE, translated by Yip et al. (1992), demonstrated good internal validity (Cronbach’s α = .91). Using the Chinese version of the MMSE, we classified dementia in participants of the present study as mild (scores of 18–23), moderate (12–17), or severe (0–11; Folstein et al., 1975; Guo et al., 1988).
Body mass index
The research assistants used the scales in the dementia special care units to measure body weight. Each scale was calibrated once a month. Additionally, we asked the research assistants to keep the measuring time and conditions as similar as possible between subjects (e.g., measuring 2 hr after a meal and removing shoes and heavy coats). The heights of the participants on annual physical examination reports were recorded. We calculated body mass index (BMI) as the body weight (kg) divided by the square of the height (m).
Mini-Nutritional Assessment
The Mini-Nutritional Assessment (MNA) comprises 18 items, including anthropometric measures (weight loss; BMI; and mid-arm and calf circumference in Items B, F, Q, and R), a dietary questionnaire (number of meals consumed; food and fluid intake; and feeding autonomy within the past 24 hr in Items J, K, L, M, and N), a global assessment (mobility; presence of acute stress; presence of dementia or depression; lifestyle; and medication in Items C, D, E, G, and H), and a subjective assessment (self-perception of health and nutrition in Items O and P; Guigoz, Vellas, & Garry, 1996). Lower MNA scores indicate poorer nourishment. The MNA scoring classifies an individual into one of the three categories: (1) adequately nourished (scores
Demographic characteristics
Data related to age, sex, education, number of comorbid diagnoses, time since dementia diagnosis, and time since institutionalization were gathered from participants’ charts.
Procedure
FAA and mealtime performance (i.e., EBS, food intake, total eating time, and meal assistance) were measured by the following method. Trained research assistants concurrently and continuously observe 5 participants at their usual mealtime in the dining room. For each participant, research assistants observed a total of three meals over a 2-day period, comprising a combination of lunches and dinners (2 lunches and 1 dinner or 1 lunch and 2 dinners). Research assistants completed the FAA and EBS according to the most commonly observed eating performance across the three observed meals. The food intake and total eating time for the three observed meals were averaged. The number of meals during which participants received each type of assistance (verbal assistance, physical assistance, or fed by caregivers) was summed and averaged for each group. The MNA was completed by reviewing charts, interviewing residents and nursing aides, and measuring mid-arm and calf circumference, in addition to observing participants at mealtimes. All participants were interviewed to complete the MMSE.
Statistical Analysis
The data were analyzed using SPSS, Version 18.0 (SPSS, Inc). An α level of .05 was used for determining statistical significance. The differences in demographic characteristics and outcome variables between the two groups were analyzed using chi-square and independent t-tests.
Results
Demographic Characteristics and Cognitive Function
As mentioned, the prevalence rate of IA affecting self-feeding in PWD in the present study was 24.8% (98 of 395). A total of 196 residents with a mean age of 81.3 years (standard deviation [SD] = 7.1) were included in the comparative analysis. Most (55.6%) participants were male. The highest proportion of participants (25.5%) had a primary school education. The average number of months since dementia diagnosis and duration of institutional care was 40.9 (SD = 43.0) and 39.1 (SD = 43.0), respectively. The average number of comorbid diagnoses was 2.1 (SD = 1.4). The average Barthel Index score demonstrated moderate dependency (63.7 points) for PWD without IA and complete dependency (15.1 points) for PWD with IA. As shown in Table 1, the above-mentioned characteristics were not significantly different between PWD with and without IA, except for the Barthel Index scores. The groups did, however, differ in cognitive function, with the MMSE scores of PWD with IA being significantly lower than those of PWD without IA (p < .001). In addition, IA occurred significantly more frequently among participants in the severe stage of dementia than in those in other stages (p < .001).
Comparison of Demographic Characteristics and Cognitive Function Between People With Dementia (PWD) by Presence (n = 98) or Absence (n = 98) of Ideational Apraxia (IA).
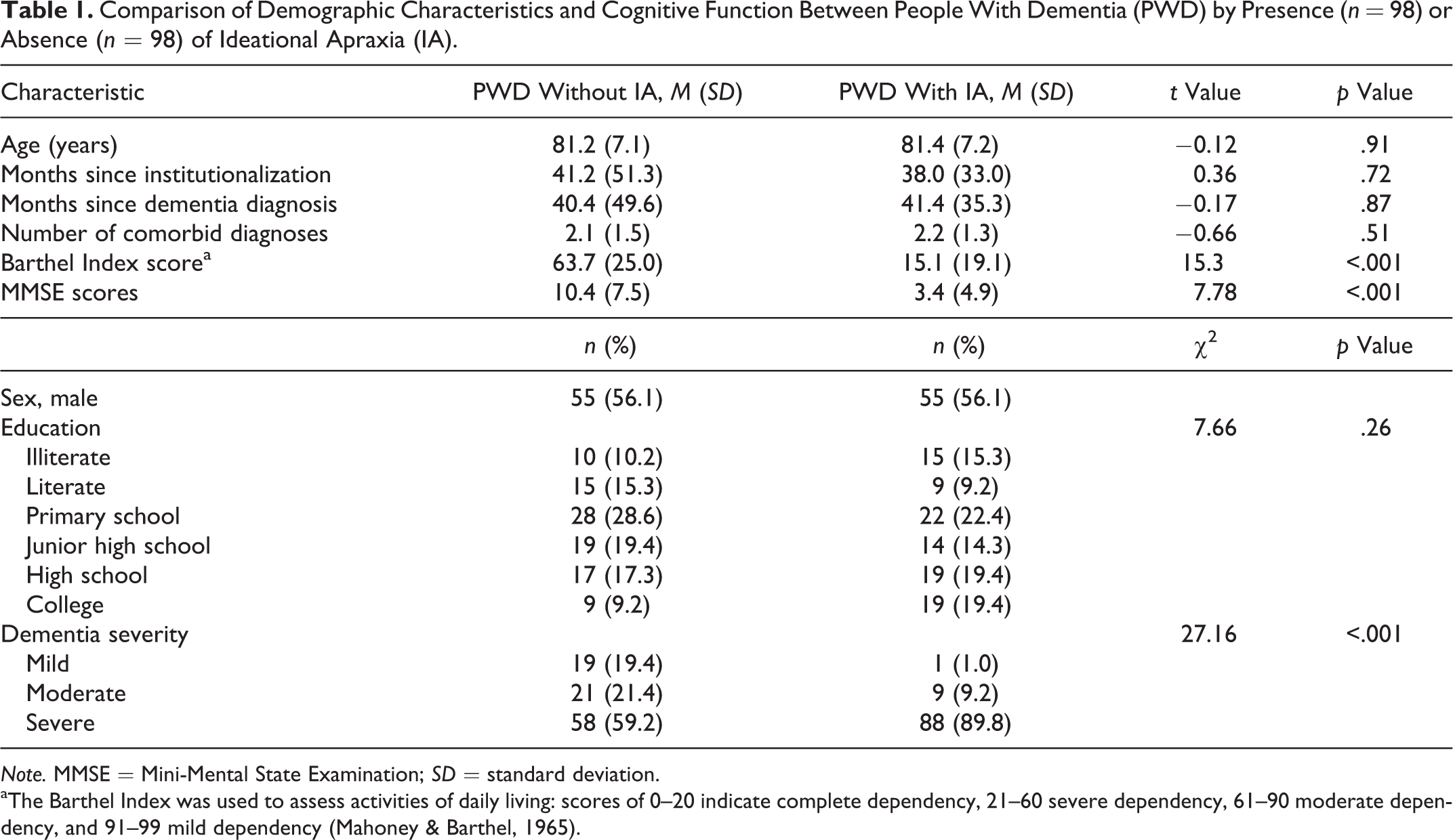
Note. MMSE = Mini-Mental State Examination; SD = standard deviation.
aThe Barthel Index was used to assess activities of daily living: scores of 0–20 indicate complete dependency, 21–60 severe dependency, 61–90 moderate dependency, and 91–99 mild dependency (Mahoney & Barthel, 1965).
Mealtime Performance and Nutritional Status
Table 2 presents the differences in mealtime performance and nutritional status between PWD with and without IA. In PWD without IA, the six observed eating behaviors were rated between 2.2 and 3.0 points, indicating that participants could complete each eating task almost independently. By contrast, in PWD with IA, five of the six eating tasks were rated between 0.5 and 0.8 points, indicating that participants were almost completely dependent on caregivers for these behaviors. PWD with IA needed verbal cues or physical assistance during mealtimes, especially for biting, chewing, and swallowing without choking. The scores on all six eating tasks differed significantly between PWD with and without IA (p < .001). Although the eating abilities of PWD with IA were significantly worse than those of PWD without IA, the total time required for eating was significantly less for PWD with IA than for PWD without IA (p = .003). The time spent being fed by caregivers in PWD with IA was significantly greater than in PWD without IA (p < .001). PWD with IA also required more verbal assistance during mealtime than PWD without IA (p = .04) and were fed by caregivers during more meals (p < .001) than PWD without IA. In addition, PWD with IA consumed approximately 90% of their food, while PWD without IA consumed only 78.9%. The percentage of participants who consumed a full meal was significantly higher in the PWD with IA group than in the PWD without IA group (p = .001).
Comparison of Mealtime Performance and Nutritional Status Between People With Dementia (PWD) With (n = 98) and Without (n = 98) Ideational Apraxia (IA).
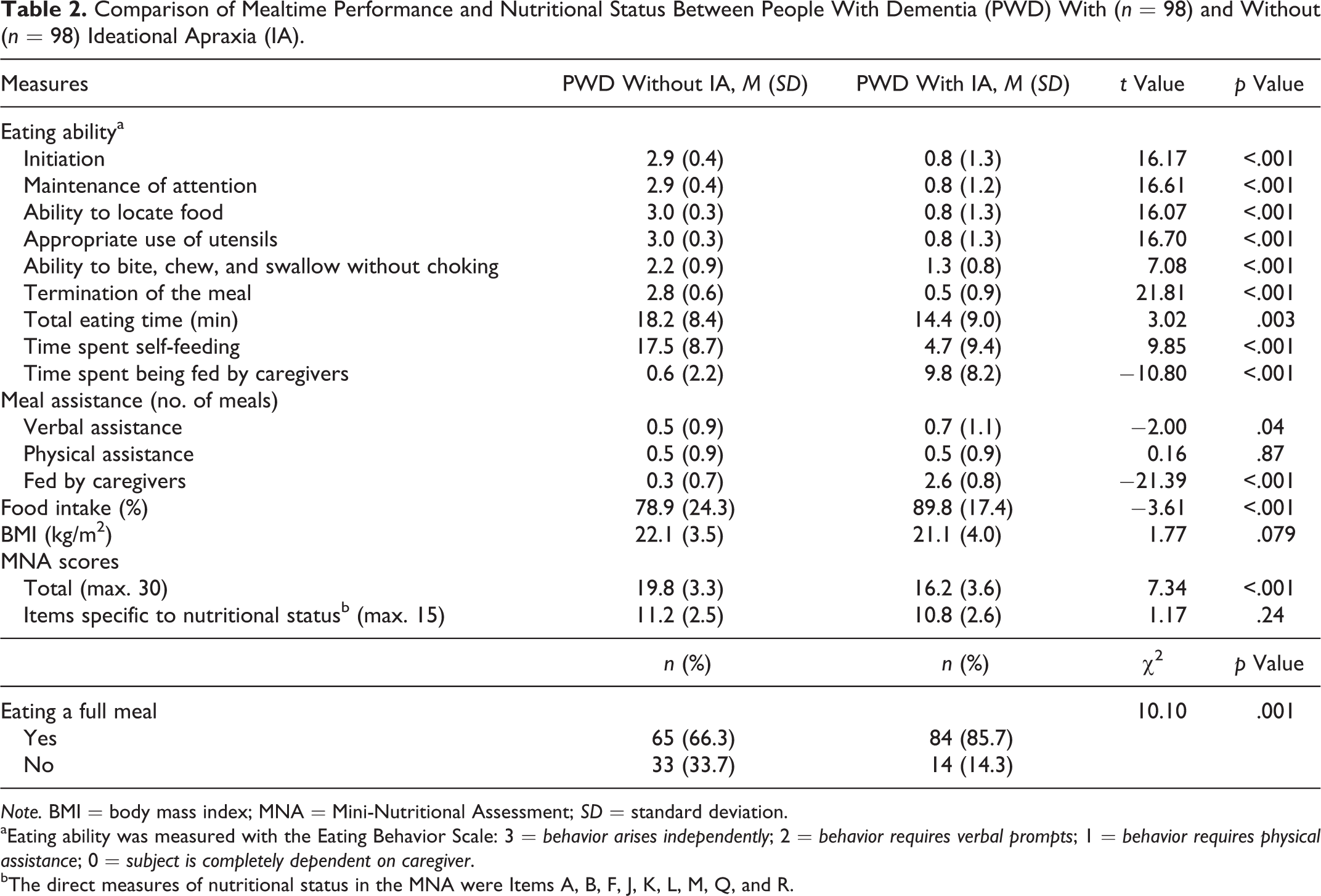
Note. BMI = body mass index; MNA = Mini-Nutritional Assessment; SD = standard deviation.
aEating ability was measured with the Eating Behavior Scale: 3 = behavior arises independently; 2 = behavior requires verbal prompts; 1 = behavior requires physical assistance; 0 = subject is completely dependent on caregiver.
bThe direct measures of nutritional status in the MNA were Items A, B, F, J, K, L, M, Q, and R.
There was no significant difference in BMI between PWD with and without IA (p = .079). The total MNA scores of PWD with IA were significantly lower than those of PWD without IA (p < .001). The mean total score for PWD with IA was 16.2, which would indicate malnourishment. However, further analysis of the items directly related to nutritional status (Items A, B, F, J, K, L, M, Q, and R, with a total of 15 points) revealed no significant difference in the mean scores on these items between PWD with and without IA (p = .24).
Discussion
In the present study, we found that the self-feeding ability of 24.8% of the PWD was affected by IA. This prevalence rate was lower than the 51% LeClerc et al. reported (2004). A number of study characteristics might explain this difference in prevalence rate. First, we assessed 2.5 times the number of PWD (395 vs. 156) in the present study compared to LeClerc et al.’s study. Second, in LeClerc et al.’s study, a research assistant observed only one meal to identify PWD who were unable to self-feed using a utensil, while in the present study we classified PWD as having IA only when they displayed an inability to initiate, follow through and sequence eating actions in at least two of three observed meals.
The cognitive function of PWD with IA was worse than that in PWD without IA in the present study, as determined by MMSE scores. The inability to self-feed due to IA generally occurred among participants in the severe stage of dementia. This finding is identical to that of Rapcsak, Croswell, and Rubens (1989), who found that IA occurred relatively late in the course of dementia, and supports Pilgrim and Humphreys’ (1991) proposition that there is more than one cognitive route for eliciting an action. In the early to middle stages of dementia, individuals with semantic deficits might access their intact procedural memory (a direct route) in order to self-feed using a utensil. However, when the disease progresses to the late stage, PWD may be unable to self-feed continuously and sequentially due to procedural memory impairment. Our results also indicate that there may be a close relationship between the progression of the disease and the appearance of IA.
In the present study, the PWD who did not exhibit IA could independently complete almost all eating tasks at mealtimes. However, PWD with IA needed to be fed or given verbal assistance in executing each eating action. Thus, the overall organization of eating was impaired in PWD with IA. This result is similar to the finding of de Renzi and Lucchelli (1988) that patients with left brain damage were less efficient in using objects and completed fewer actions correctly than those without such damage. Furthermore, the PWD with IA in the present study had more successfully retained the ability to bite, chew, and swallow than other eating abilities. This finding is not surprising given Gahagan’s (2012) observation that the ability to coordinate swallowing, which occurs at 34–37 weeks’ gestational age, is the first eating behavior to be acquired and the last to disappear in PWD.
Given that the self-feeding ability of PWD with IA was obviously impaired in the present study, they required caregiver assistance at mealtime to achieve optimal food intake. Accordingly, the frequency of mealtime assistance was significantly higher in PWD with IA than in PWD without IA, with caregivers providing more verbal assistance and more often feeding PWD with IA. This finding might be associated with the inability of PWD with IA to sequence motor actions (LeClerc & Wells, 1998). In previous studies, researchers found that PWD with IA had difficulty performing a multiple-step eating task, especially in beginning a meal (Edahiro et al., 2010; Zadikoff & Lang, 2005). Caregivers would tell them what the next step was, and these verbal instructions (or cues) helped most of them start eating, continue eating without interruption, and maintain complete eating behaviors (Edahiro et al., 2010). However, providing physical guidance (e.g., assisting a resident in holding utensils) or partial physical assistance (e.g., caregiver physically feeding a mouthful of food), alone, might not be sufficient to encourage PWD with IA to initiate the next eating step. Therefore, when participants could not complete eating cycles when provided with verbal instructions (or cues), caregivers in the present study commonly undertook spoon-feeding to ensure sufficient food intake.
In terms of total eating time, in the present study caregivers fed PWD with IA for approximately 68% of the time spent eating (9.8 of 14.4 min). However, caregivers maintained efforts to encourage self-feeding by providing verbal assistance for approximately 5 min after the start of eating time. If the self-feeding time in a meal can be increased by providing verbal assistance with meals, it is possible that eating independence can be maintained. Once most of the time spent eating consists of being fed by caregivers rather than self-feeding, the total eating time will likely be shortened and eating independence might decline rapidly (Edahiro et al., 2010).
The caregiver assistance provided at meals appears to have allowed the BMI of PWD with IA to be maintained to the same degree as that of PWD without IA in the present study. This finding supports the previous work of Lin, Watson, and Wu (2010) and Steele, Greenwood, Ens, Robertson, and Seidman-Carlson (1997). Also, perhaps because their food intake was maintained with assistance, PWD with IA did not fall into a malnourished state. Although their mean total score on the MNA did fall into the category of malnourished, when we looked specifically at the subgroup of items directly related to nutritional status, mean scores in PWD with IA did not differ significantly from those of PWD without IA, who were classified as “at risk for malnutrition” according to their total MNA scores. This finding suggests that PWD with IA may have had low total scores on the MNA because of characteristics other than nutritional status, such as a high level of dependence on others for assistance, severe dementia, and needing to be fed. Thus, verbal assistance and being fed at mealtimes appear to have a substantial impact on dietary parameters and anthropometric measures, even in the severe stage of dementia. Caregivers should closely monitor the eating behaviors of PWD with IA and provide assistance in a timely manner.
The PWD without IA group had a lower mean food intake and ate fewer full meals than the PWD with IA in the present study. However, their mean BMI was in the normal range and did not differ significantly from that of the PWD with IA. We believe that this apparent contradiction might be explained by the demographic characteristics of the PWD without IA. The PWD without IA group had better functional status (moderate dependency) and cognitive function than the PWD with IA group. Lin et al. (2010) found that nursing home residents with dementia who had moderate dependency could feed themselves and self-control eating behaviors but were generally ignored by staff during mealtimes, resulting in low food intake at mealtimes. However, PWD without IA might supplement their food intake with extra food throughout the day, according to their physical and psychological needs, which would help to maintain their BMI. By contrast, PWD with IA, who had very severe cognitive impairment and were completely dependent, relied entirely on staff assistance to ensure sufficient food intake regardless of whether it was mealtime or not.
Our study had some limitations. First, at the start of the study, we tried to weigh the food before and after a meal. However, in some research facilities, staff provided buffet-style meal service. The act of weighing the food after it had all been placed on residents’ meal trays triggered residents’ agitated behaviors, as they believed that the research assistants were taking their meals away permanently. In order to maintain the study format of observing the PWD at mealtime in a natural environment, we decided to use the percentage of meal eaten to represent food intake. Second, variations in meals observed for data collection (observing 2 lunches + 1 dinner or 1 lunch + 2 dinners) could potentially bias the results. However, the frequencies of the two possible observed meal combinations did not differ significantly between the two groups. We can thus assume that the method adopted for observing three meals was homogeneous between the groups. Finally, because of the cross-sectional design, we could not observe changes in eating ability, mealtime performance, or nutritional status over time for the PWD in the present study. A future study using similar measures with a longitudinal design would be useful.
Conclusion
In dementia special care units, approximately one in four residents may be at risk of IA. Our findings demonstrated that IA generally occurs in the severe stage of dementia and affects both mealtime performance and nutritional status. Therefore, when dementia progresses to the late stage, staff should pay special attention to residents’ mealtime performance and nutritional status. Staff should be reassigned based on the eating ability of PWD with IA rather than on the number of PWD in general participating in mealtime. PWD with IA require more mealtime assistance to ensure sufficient food intake and maintain BMI. We did find that PWD with IA could sequence the eating steps at some meals when staff provided verbal instructions (cues). Therefore, it might be useful to provide memory training, such as spaced retrieval, to help PWD with IA remember each eating step and, consequently, increase eating independence. Future studies could explore these types of interventions among PWD with IA. As for PWD without IA, especially those with moderate dependency, our findings suggest that staff should also monitor the amount they consume at each meal in order to avoid the risk of malnutrition.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by the National Health Research Institute (NHRI-EX98-9621PI).