
Abstract
Objectives:
The aim of the study was to assess the concentrations of tissue factor (TF) and tissue factor pathway inhibitor (TFPI) in the blood of patients with a postoperative wound after neurosurgery.
Method:
Participants included 20 adult patients who underwent neurosurgery because of degenerative spine changes. The concentration of TF and TFPI in the patients’ blood serum was measured 3 times: before surgery, during the first 24 hr after surgery, and between the 5th and 7th days after surgery. The control group comprised 20 healthy volunteers similar to the patient group with respect to gender and age.
Results:
A statistically significant difference was observed between TF concentration at all three measurement time points in the research group and TF concentration in the control group (p = .018, p = .010, p = .001). A statistically significant difference was found between TFPI concentration at the second time point in the research group and TFPI concentration in the control group (p = .041). No statistically significant within-subject difference was found between TF concentrations before and after surgery. A statistically significant within-subject difference was found between TFPI concentrations within 24 hr after surgery and 5–7 days after surgery (p = .004).
Conclusion:
High perioperative concentrations of TF indicate not only the presence of thrombophilia but also the importance of TF in the wound-healing process. Perioperative changes in TFPI concentrations are related to its compensatory influence on hemostasis in thrombophilic conditions.
Clinical observations and laboratory tests indicate thrombophilia in the postoperative period independent of the extent of the operation (i.e., after small local procedures as well as extensive orthopedic or abdominal surgeries). The risk of thrombotic complications increases in the postoperative period, and test results have shown an elevated platelet count, increased fibrinogen level, and a higher than normal concentration of thrombophilia markers (i.e., thrombin–antithrombin complex and blood level of fibrinopeptides; Kijowski et al., 1994; Parolari at al., 2005).
Activation of the blood clotting process is an organism’s natural physiological reaction to blood vessel injury and prevents excessive blood loss. Hemostasis activation is thus the first phase in the postoperative wound-healing process. Other phases include inflammation; mesenchymal cell differentiation, proliferation, and migration to the wound site; angiogenesis; reepithelialization; and collagen synthesis to ensure that the growing tissue is strong (Li, Chen, & Kirsner, 2007). The first phase of hemostasis begins immediately after injury when the vessels contract and platelets releasing platelet-derived growth factor (PDGF) aggregate at the wound site. PDGF stimulates cellular division and angiogenesis and contributes to activation of plasmatic coagulation, which results in fibrin production (Guo & DiPietro, 2010).
Tissue factor (TF), released in the circulation after the continuity of a blood vessel is disrupted, plays a key role in activating the plasma coagulation system. Large amounts of TF are present in the brain, heart, kidneys, lungs, uterus, and placenta. Blood vessels are surrounded by cells constitutively expressing TF, including those of the abovementioned organs. Breakage in the continuity of a blood vessel results in exposure of the TF contained in fibroblasts and pericytes, which in turn initiates coagulation. TF is a 47-kDa transmembrane glycoprotein that was first cloned in 1987. The TF extracellular domain contains binding sites for coagulation Factor VII/VIIa, while transmembrane domain plays a role in binding the TF/VIIa complex to the cell surface and in the full expression of procoagulant activity (Hoffman & Monroe, 2012). The TF cytoplasmic domain is related to the angiogenesis process and conveys cellular signals (Bluff, Brown, Reed, & Staton, 2008). The binding of plasma FVII/FVIIa with TF leads to the formation of thrombin, activation of platelets, and cleavage of fibrinopeptides from fibrinogen (Zwicker, Trenor, Furie, & Furie, 2011). Cleavage of fibrinopeptides A and B from fibrinogen is the first step in the formation of fibrin monomers. Polymerization of fibrin monomers leads to the formation of unstable fibrin strings, which become a stable fibrin network as an effect of plasma coagulation Factor XIII activity. This fibrin network gives a clot mechanical and chemical resistance. The clot not only seals the wound and prevents infection but also provides a framework for fibrous tissue proteins (collagen, elastin, and reticulin) and fibronectin, which bridge the wound edges. Inflammatory cells—monocytes, which differentiate into macrophages—are attracted into the fibrinous–fibrous bridge. The inflammatory phase is followed by the fibroblastic phase, which involves synthesis of collagen and elastic fibers and reticulum. Oxygen is essential in this phase; therefore, new blood vessels are formed via the process of angiogenesis.
Recent studies show that TF may play a role in numerous wound-healing mechanisms. Chen and colleagues (2005) claim that TF is an important link between the early inflammatory response to wounding and reparative processes. There are numerous articles on TF in relation to surgical operations in patients with metabolic disorders (diabetes or obesity) or diseases that might disrupt the wound-healing process (neoplastic diseases; Guo & DiPietro, 2010). However, we could find no description in the literature of TF action in patients with no coexisting disorders, where wound healing involves healing by first intention, and no postoperative complications that could interfere with the activity of wound-healing factors are expected. The aim of the present study was to assess the concentrations of TF and tissue factor pathway inhibitor (TFPI) in the blood of patients with postoperative wounds before and after the operation. TFPI is a serine protease, a major TF-dependent coagulation pathway inhibitor that inhibits FXa/TF/FVIIa complex. It is produced mainly by vascular endothelial cells, and its increased concentration in blood serves as evidence of stimulation or damage of the endothelium (DelGiudice & White, 2009). Subjects were patients undergoing surgery for cervical or lumbar discopathy, with no coexisting disorders. We posed three specific research questions:
Method and Materials
Participants
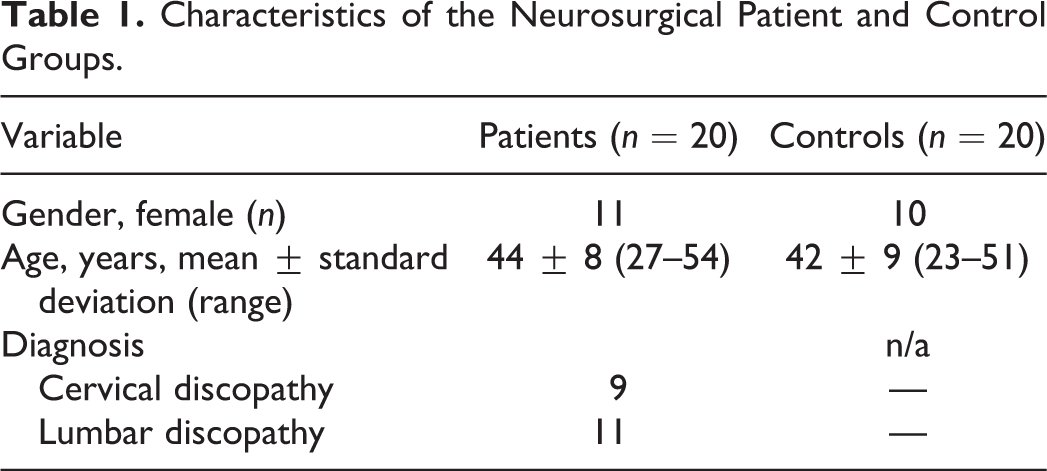
We conducted the study in the Neurosurgery and Neurotraumatology Clinic, Nicolaus Copernicus University (NCU), Collegium Medicum (CM) in Bydgoszcz, Poland. Participants included 20 adult patients (9 men and 11 women) aged 27–54 years (mean age 44 ± 8 years) who underwent surgery for degenerative spine changes (see Table 1 for demographic and medical characteristics of the patient and control groups). The diagnosis of degenerative spine change was made on the basis of the patient’s case history, neurological examination, and neuroimaging tests (using computed tomography or magnetic resonance imaging). We excluded patients who, apart from the degenerative spine change, were also diagnosed with coexisting diseases of the central nervous system (e.g., proliferative process or vascular malformation) or disorders that interfere with the wound-healing process (concomitant atherosclerosis and its complications, diabetes in pregnant women, neoplastic disease, and AIDS). Also patients who had undergone another surgery within 30 days preceding their admission to the Neurosurgery and Neurotraumatology Clinic were excluded from the study. The control group comprised 20 healthy volunteers, similar to the research group with respect to gender and age, who were not receiving treatment.
Characteristics of the Neurosurgical Patient and Control Groups.
Measurements
We drew blood for the measurement of TF and TFPI once from each control participant and 3 times from each patient. The first time point for patient blood sampling was 24–1 hr before surgery (Measurement 1), the second was within the first 24 hr after surgery (Measurement 2), and the third was between the 5th and 7th days after surgery (Measurement 3). All blood draws in both groups were performed in the morning with participants having rested for 30 min and refrained from eating for at least 8 hr. Using a vacuum system, we drew 5 cm3 of blood via venipuncture from a vein in the cubital fossa free of venous stasis into polyethylene test tubes with 3.2% sodium citrate in a 9:1 ratio. We sent all samples to the Laboratory of Hemostasis Disorders in the Faculty of Pathophysiology at NCU, CM to measure the concentrations of TF and TFPI using enzyme-linked immunosorbent assays. The blood samples were taken according to the blood draw procedures of the Neurosurgery and Neurotraumatology Clinic. All blood draws performed on patients were also used for obtaining samples for use in laboratory tests essential for diagnostic and therapeutic processes connected with their surgical procedure.
Ethical Considerations
The Bioethics Committee of NCU , CM in Bydgoszcz, Poland, approved this study (Permit no. KB/126/2007). Each participant was informed about the aim of the research and provided written informed consent.
Statistical Analysis
We performed statistical analyses using Microsoft Excel and STATISTICA, version 9.1. We used descriptive statistics (arithmetic mean, standard deviation [SD], median [Me], minimum [Min], and maximum [Max]) to describe participant characteristics and initial measures. Because the distribution of the analyzed parameters differed from a normal distribution, we used the nonparametric Friedman test to analyze the changes in TF and TFPI within the patient group across consecutive measurements. We used the Mann–Whitney test (Z) to compare mean values between groups. The correlation between the individual factors (concentrations) was assessed using Pearson’s correlation coefficient (r p). Statistical hypotheses were verified at the level of relevance p < .05.
Results
Comparison of TF and TFPI Concentrations Between the Patient and Control Groups
Table 2 shows the mean TF and TFPI concentrations for the patient group at each time point and for the control group. Mean TF concentration in the patient group at Measurement 1 was significantly higher than that in the control group (Z = 2.36, p = .018; see Table 2). We found no statistically significant difference in TFPI concentration between the patient group at Measurement 1 and the control group (Z = −0.85, p = .39). At Measurement 2, mean TF concentration in the patient group was again significantly higher than that in the control group (Z = 2.56, p = .010), and mean TFPI concentration was significantly lower than that in the control group (Z = −2.05, p = .041). Mean TF concentration in the patient group at Measurement 3 remained significantly higher than that in the control group (Z = 3.25, p = .001), but there was no statistically significant difference in TFPI between groups at this time point (Z = 0.56, p = .57).
Tissue Factor (TF) and Tissue Factor Pathway Inhibitor (TFPI) Concentrations (mean ± SD) in Blood of Patients and Controls.

Note. P 1, P 2, and P 3 relate to the comparisons between controls and patients at Measurements 1, 2, and 3, respectively. Measurement 1 = 24–1 hr before surgery; Measurement 2 = within 24 hr after surgery; Measurement 3 = between the 5th and 7th days after surgery.
Change in TF and TFPI Concentrations in the Patient Group Across Consecutive Measurements
Table 3 presents TF and TFPI concentrations in the patient group across the three measurements. We found no statistically significant difference in TF concentrations between measurements taken before and after the operation, χ2(n = 20, df = 2) = 1.37, p = .50. We did, however, find a statistically significant difference in TFPI concentrations across measurements taken before and after the operation, χ2(n = 20, df = 2) = 11.10, p = .004. The difference between median TFPI concentrations in Measurements 2 and 3 was statistically significant (p = .004).
Tissue Factor (TF) and Tissue Factor Pathway Inhibitor (TFPI) Concentrations in Blood of Patient Group Across Consecutive Measurements.

Note. Measurement 1 = 24–1 hr before surgery; Measurement 2 = within 24 hr after surgery; Measurement 3 = between the 5th and 7th days after surgery.
Correlation Between Consecutive Measurements of Individual Parameters
There was a statistically significant correlation between TF concentration before (Measurement 1) and directly after surgery (Measurement 2) in the patient group (r p = .50, p = .03). Patients with higher TF concentration before surgery also had higher TF concentration after surgery. We observed no statistically significant correlation between TF concentration before surgery (Measurement 1) and TF concentration 5–7 days postsurgery (Measurement 3; r p = .23, p = .34). Nor did we observe a statistically significant correlation between TF concentration directly after surgery (Measurement 2) and 5–7 days after surgery (Measurement 3; r p = .32, p = .19).
We found no statistically significant correlation between TFPI concentration before (Measurement 1) and directly after surgery (Measurement 2; r p = .44, p = .05) in the patient group. However, there was a statistically significant correlation between TFPI concentration before surgery (Measurement 1) and TFPI concentration 5–7 days after surgery (Measurement 3; r p = .48, p = .03). Patients with a higher TFPI concentration before surgery also had a higher TFPI concentration 5–7 days after surgery. We found no statistically significant correlation between TFPI concentration directly after surgery (Measurement 2) and TFPI concentration 5–7 days after surgery (Measurement 3; r p = .04, p = .86).
Discussion
Recent studies have provided new data related to the importance of TF in different phases of the wound-healing process. In the present study, we found that patients with discopathy had a significantly higher concentration of total TF before surgery than did healthy controls. It remained similarly higher in the patient group in consecutive measurements after the operation (on the 1st and between the 5th and 7th days after surgery).
We find this high TF concentration before surgery in patients with discopathy surprising because these patients did not suffer from other disorders. The main symptom in patients suffering from discopathy is pain resulting from herniated discs pressing on nerve roots associated with numbness and tingling in the affected part of the spine. The pressure on the nerves leads to the constriction of blood vessels, resulting in an insufficient blood supply to tissues and a local inflammatory response. Van der Putten et al. (2005), who studied patients with chest pain due to coronary disease, reported an increased concentration of plasma TF antigen in the form of inactive particles, which once activated could initiate the coagulation process. The authors suggested that TF inactivity resulted from the lack of procoagulant phospholipids in the blood. Another explanation of our finding might be related to TF expression in monocytes, which are cells involved in the inflammatory process (Osterud, 1998). Discopathy involves a local inflammatory process in which inflammatory cells, such as monocytes, migrate to the inflammatory site and transform into macrophages. Histological and immunohistochemical examinations of intervertebral discs from patients with lumbar pain have revealed the presence of macrophages and mast cells (Peng et al., 2006).
On the 1st day after surgery in the present study, TF concentration in the patients’ blood was slightly, and nonsignificantly, lower than it was before surgery. Nevertheless, it remained significantly higher than the concentration in the control group. During the operation, numerous blood vessels were cut, thus triggering the release of large amounts of TF and activating the coagulation process and fibrin production. Hattori, Khan, Dolman, and Edmunds (2005) found damaged monocytes in patients undergoing cardiac surgery involving cardiopulmonary bypass. According to the authors, soluble plasma TF in blood and monocytes activates Factors VII and X, which results in thrombin production. The clot that forms at the wound site seals the wound and forms a fibrin framework, which leads to the next phase of the healing process, the inflammatory response. Slightly lowered TF concentration in the early postoperative period (1st day after surgery) likely resulted from its consumption during the hemostasis phase of the wound-healing process.
Monroe, Mackman, and Hoffman (2010), who examined hemophilia B mice, and McDonald, Yang, Roberts, Monroe, and Hoffman (2008) also indicated the importance of TF not only in the initial phase of the healing process but also in the next stages. When examining samples of animal tissues from wound sites, they observed the presence of TF around blood vessels on the 1st day after wounding, its disappearance within a day after injury and reappearance after 8 days. In a literature review, Chen et al. (2005) reported that TF not only initiates the coagulation process in the first phase of the wound healing process, which results in fibrin production, it also influences the production of strong angiogenic factors such as vascular endothelial growth factor (VEGF) and PDGF by its paracrine/hormonal action on Factor Xa, thrombin, and other coagulation proteins. The authors also noted that researchers have observed TF expression on keratinocytes. There is also evidence that TF cytoplasmic domain directly stimulates VEGF production by stimulating protease-activated receptor-2 (Bluff et al., 2008).
Our findings in the present study showed that total TFPI concentration decreased significantly on the 1st day after surgery, but 5–7 days later, it was higher than it was before surgery. Fedi et al. (1999) similarly observed a decrease in the TFPI level after an orthopedic operation. Dahm et al. (2003) and Harris, Stendt, Vollenhoven, Gan, and Tipping (1999) reported lowered TFPI levels in women taking combined oral contraceptives and found decreased TFPI concentration during intensified thrombotic processes. This decrease may result from TFPI consumption during the process of the inhibition of the TF-dependent coagulation pathway or indicate an increased risk of hypercoagulability. Soejima et al. (1999) reported increased TFPI concentration in patients with unstable coronary disease after administration of heparin. Because the increased TFPI level was associated with hypercoagulability through increased TF concentration, their findings demonstrate the significant role of TFPI in the inhibition of the coagulation process. Recent studies on TFPI in young women with myocardial infarction indicated that high TFPI concentrations in the women’s blood served as a compensatory mechanism in response to hypercoagulability as well as indicating stimulation of the endothelium (Winckers et al., 2011).
Conclusion
High perioperative concentrations of TF indicate not only blood hypercoagulability but also the significant role TF plays in the wound-healing process. It is a necessary factor in the hemostatic phase of wound healing and a mediator of signals that participate in the proliferative, inflammatory, and immune responses. Perioperative changes in TFPI concentrations are related to its compensatory regulation of hemostasis with hypercoagulability, where it serves as a major inhibitor of extrinsic tenase complex by controlling thrombin production.
Exploring knowledge related to wound healing is crucial in the practice of neurosurgical nursing. With each dressing change, nurses assess the process of wound healing. Biological processes of wound healing include many phases such as hemostasis (primary and secondary), inflammation, proliferation (epidermal regeneration, intercellular substance synthesis, and regeneration of blood vessels), connective tissue production, and the maturation phase (vasoconstriction, remodelling of extracellular matrix, and scar formation). Nursing teams should have a thorough knowledge of hemostasis and angiogenesis to better understand the mechanisms involved in the wound-healing process and, consequently, take proper care of postoperative wounds.
Footnotes
Acknowledgments
We would like to cordially thank the staff of the Laboratory of Hemostasis Disorders in the Faculty of Pathophysiology of NCU, CM, in Bydgoszcz for measuring the individual parameters.
Author Contribution
RS contributed to conception, design, and acquisition; drafted and critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy. MG contributed to conception, design, and acquisition; drafted and critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy. MB contributed to conception, design, and acquisition; drafted and critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy. EB contributed to conception, design, and acquisition; drafted and critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy. BH contributed to conception, design, and acquisition; drafted and critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy. DR contributed to conception, design, and acquisition; drafted and critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy. GG contributed to conception, design, and acquisition; drafted and critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was financed by the academic activity fund of Nicolaus Copernicus University (Research manager: Robert Ślusarz, PhD).