
Abstract
Current medical technology permits the early detection of risk factors for coronary artery disease (CAD) in adults, and interventions are available to prevent CAD-related morbidity and mortality. The goal of this study was to determine the effectiveness of a Qigong exercise intervention in improving biomarker levels and mental and physical health outcomes in community-dwelling adults diagnosed with CAD risk factors, in a southern Taiwanese city. Participants were randomly assigned to an experimental (n = 84) group that participated in a 60-min Qigong group session 3 times per week for 3 months or a control (n = 61) group that did not receive the intervention. Self-perceived mental and physical health assessed with the Chinese Health Questionnaire-12, and body fat percentage were measured at baseline and 6, 12, and 16 weeks. Blood samples were collected at baseline and 12 weeks for analysis of lipid profiles, high-sensitivity C-reactive protein (hs-CRP), glycated hemoglobin (HbA1c), and fasting plasma sugar. Linear mixed model analyses revealed that experimental participants had significantly improved perceived mental and physical health and body fat percentage compared to the control group at 6 and 12 weeks but not 16 weeks. The lipid profiles were significantly more improved in the Qigong group than in the control group at 12 weeks. Qigong exercise, however, had no significant effects on hs-CRP, HbA1c, or fasting plasma sugar. Findings suggest that Qigong exercise improves a limited number of CAD risk factors in community-dwelling adults aged 40 years and over.
The prevalence and aggregated costs of cardiovascular diseases (CVDs) increase substantially as the average age of a population increases (Heidenreich et al., 2011). An estimated 17 million people died from CVD in 2008, representing 30% of all deaths globally. Of these deaths, an estimated 7.3 million were attributed to coronary artery disease (CAD; World Health Organization [WHO], 2014). CAD, also known as ischemic heart disease, is the leading killer of men and women worldwide and is responsible for approximately one third of all deaths in individuals older than 35 years (Bhatia, 2010; Hanson, Fareed, Argenio, Agunwamba, & Hanson, 2013). Recognized risk factors for the development of CAD include family history, high blood pressure, smoking, elevated low-density lipoprotein cholesterol (LDL-C), diabetes, physical inactivity, and obesity (Bhatia, 2010), with behavioral risk factors accounting for about 80% of cases. Primary care practitioners are able to identify people at higher risk of CAD early in the process, and proactive interventions are available that reduce the risk of heart attacks (WHO, 2014).
Physical activity (PA), exercise training, and cardiorespiratory fitness provide benefits in primary and secondary CAD prevention (Lavie, Thomas, Squires, Allison, & Milani, 2009). Meditative movement categories of PA such as Tai Chi and Qigong, which encompasses Tai Chi movements, are holistic in nature and have increased in popularity over the past few decades (McCaffrey & Fowler, 2003; Rogers, Larkey, & Keller, 2009). Qigong, which is based on a holistic system of healing that integrates gentle movement exercise, meditation, breathing techniques, and self-massage, is considered to be the ancient root of traditional Chinese medicine practice. It is simpler and more repetitive than Tai Chi, easy to learn, and may be practiced while standing, walking, sitting, or lying down (Rogers et al., 2009; Ross, 2009). Many branches and hundreds of forms of Qigong exercise have developed in different regions, with some designed for specific health-enhancement purposes. These branches and forms have developed a theoretical basis, and investigators have conducted extensive research to assess their health effects in terms of balance, physical function, cardiopulmonary and immune system health, and psychological well-being (Jahnke, Larkey, Rogers, Etnier, & Lin, 2010; Rogers et al., 2009).
Results of previous studies have demonstrated that Qigong reduces the levels of known CAD risk factors apolipoprotein A1 (APO-A1), total cholesterol (TC), and triglycerides (TGs) and increases the level of high-density lipoprotein cholesterol (HDL-C) in both healthy individuals and hypertensive patients (Cheung et al., 2005; Lee, Lee, Kim, & Choi, 2004; Vera et al., 2007). Impaired glycemic control is another known risk factor for CAD (Heijden, Ortegon, Niessen, Nijpels, & Dekker, 2009). Liu, Miller, Burton, and Brown (2010) conducted a single-group pre-posttrial on 11 participants (3 men and 8 women, aged 42–65 years) with elevated blood glucose levels to verify the efficacy of Qigong exercise in controlling glycemic levels. Their results demonstrated significant improvements in glycated hemoglobin (HbA1c) and insulin resistance after a 12-week regimen of Tai Chi and Qigong exercise training. The authors further verified that this 12-week regimen decreased HbA1c, fasting blood insulin, and insulin resistance in a randomized controlled trial (Liu, Miller, Burton, Chang, & Brown, 2011).
High-sensitivity C-reactive protein (hs-CRP) levels and certain affective dispositions have also been identified as risk factors for CAD. The U.S. Preventive Services Task Force (2009) recommends including hs-CRP, which plays a key role in the pathophysiology of atherosclerosis, as a novel risk factor for assessing asymptomatic persons with CAD. Aerobic exercise may lower the risk of CAD by decreasing hs-CRP levels (Goldhammer et al., 2005; Kondo, Kobayashi, & Murakami, 2006). Suls and Bunde (2005) identified particular affective dispositions (such as anger, anxiety, and depression) as risk factors for CVD. Their conclusions, however, grew out of a study that used older data from the National Health Insurance Database that are now outdated due to the worsening overall CVD risk profile of the general population in Taiwan over the past 3 decades (Y. Cheng et al., 2005). This worsening risk profile makes identifying effective prevention strategies to reduce CAD morbidity more vital than ever.
There are very few studies addressing the effects of Qigong exercise on CAD risk factors. Therefore, we designed this study to investigate the effects of a particular widely practiced Qigong exercise regimen on biomarkers associated with increased risk for CAD (hs-CRP, glycemia, and lipid profile) and mental and physical health in participants with at least one identified CAD risk factor.
Method and Material
Study Design and Setting
This study was a multisite (communities), single-blind, and cluster randomized controlled trial in southern Taiwan. We applied permuted block randomization, with a community health center as a unit, using two lots, one of which was marked E for experimental group and the other C for control group. A total of 13 communities that had not had Qigong programs in the previous year and did not have a program planned for the next 16 weeks were recruited to participate, with each community assigned randomly to either the Qigong group (12 weeks of regular Qigong exercise training [7 communities]) or the control group (regular life maintenance: maintaining usual daily activities and exercise habits [6 communities]). This cluster randomization was used to reduce the possibility of contamination between the two groups. All assessment staff members were blinded to the group assignment of participants. To ensure participant compliance with the protocol and to help verify the data, the same group of assessment staff and instructor remained in charge of a particular center for the duration of the study. The institutional review board of National Cheng Kung University approved the study protocol, and all participants provided written informed consent. We conducted the study between December 2011 and August 2012.
Participants
We recruited potential participants from communities in one city in southern Taiwan. Inclusion criteria were (1) 40 years of age or more; (2) able to communicate in Chinese or Taiwanese (interview or self-administration); (3) exhibiting at least one of seven indicators of increased risk for CAD, including family history (myocardial infarction, coronary revascularization, or sudden death of an immediate relative, either male <55 years or female < 65years of age), cigarette smoking (current smoker or past smoker who quit within the past 6 months), hypertension, dyslipidemia (TC > 200 mg/dl, HDL < 45 mg/dl, or LDL > 130 mg/dl or on lipid-lowering medication), impaired fasting glucose (fasting blood glucose ≥100 mg/dl confirmed on two separate occasions), obesity (body mass index [BMI] > 27 kg/m2 or waist girth >90 cm/35.5 in for men and >80 cm/31 in for women, or waist to hip ratio ≥0.95 for men and ≥0.86 for women), and sedentary lifestyle (not participating in a regular exercise program or accumulating 30 min or more of moderate PA on most days of the week); (4) able to move freely without aids; (5) free of chest pain or shortness of breath; and (6) having little or no experience at practicing Qigong. Participants with the following characteristics were excluded: (1) a serious medical condition that precluded safe participation in an exercise program such as unstable chest pain, myocardial infarction, severe hypertension, peripheral vascular disease, stroke, congestive heart failure, chronic obstructive pulmonary disease, psychiatric disease, and active cancer; (2) inability to complete the 16-week study or unlikely to be compliant (i.e., planning to join other exercise programs within 16 weeks); (3) inability to walk without a cane or other assistive device and with a recent history of postural hypotension or syncope. We recruited a total of 145 eligible adult residents from the communities and, via cluster randomization, assigned them to either the Qigong (n = 84) or the control group (n = 61; Figure 1).
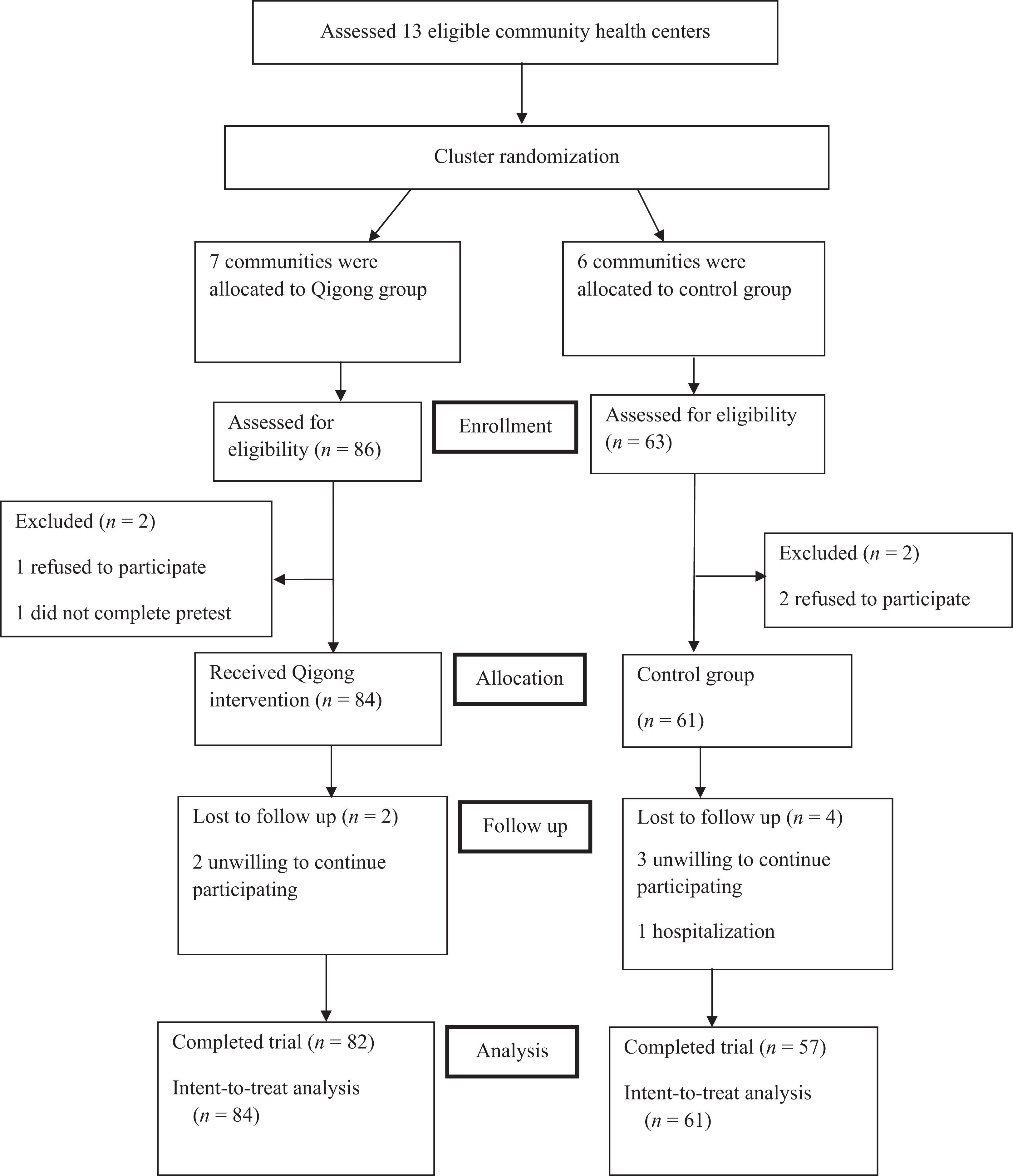
Flowchart of participants.
Intervention
The Qigong exercise program was developed using a consensus process that involved six experts (one Qigong master with more than 20 years of Qigong practice, two gerontology nursing scholars, one cardiovascular clinic physician, one health promotion educator, and one occupational therapist). The Qigong intervention protocol was designed following the recommendations for cardiovascular safety for exercise for reducing the risks of CVD in middle-aged and elderly people: at least 150 min/week of moderate-intensity aerobic activity, with no more than 60 min of continuous exercise per session, and intermediate rest (Ajisaka, 2006; Centers for Disease Control and Prevention [CDC], 2015). One session in the Qigong intervention took approximately 60 min, which included a warm-up (10 min), Qigong movements (30 min) and intermediate rest (5 min), cooldown (5 min), and meditation (10 min). The warm-up included 10 exercises designed to relax the body from the neck to the ankles. The Qigong movements were modified and set by Master Ce Hang Truong (Compassionate Service Society, 2014) to be easy to learn and master in a short period. These movements encompassed 14 gentle stretching and body movements in standing postures for which all participants were required to coordinate their breathing. The cooldown encompassed three movements to smooth the heart rate: slowly raising both hands over the head followed by fully opening hands on the chest and then holding hands flat at shoulder height. The 10-min meditation component required that participants sit and keep their bodies aligned along a center line (head in line with the spine), focus on abdominal breathing (concentrate on the single thought), and visualize for relaxation (from head to toes). The Qigong exercise was implemented as a group class and practiced 3 times per week for 12 weeks at either 9:00–10:00 a.m. or 2:30–3:30 p.m., with an instructor at quiet venues that were similar across communities. Participants were asked to exhale when their muscles were contracted and inhale when their muscles were relaxed through the entire 60 min Qigong exercise. To ensure safety, elderly participants practiced at the closest proximity to the instructor to facilitate close monitoring during the intervention. The average adherence rate for the intervention was 81.4%, with 8 participants having a rate of adherence less than 60% (range 17.2–57.4%).
Exercise Intensity
For this study, the target exercise intensity was 3 = moderate, in accordance with the Borg scale for rating perceived exertion (from 0 = nothing at all to 10 = very very hard; Borg CR-10 scale; Borg, 1998). The scale incorporated simplified numerical and verbal descriptors of perceived exertion. After the 6-week intervention, when participants were familiar with how to perform the Qigong exercise regimen, we had them perform a 30-min practice session and used the Borg CR-10 scale to measure the perceived intensity of the exercise for each participant. The average self-perceived intensity score was 2.98 (SD = .77, range 1–6).
Outcome Measures
We administered a demographic and health habits questionnaire at baseline to all participants. We administered the Chinese Health Questionnaire-12 (CHQ-12), which assesses self-perceived mental and physical health, and measured body fat percentage at baseline and at 6-, 12-, and 16-week posttests. We collected blood samples for analysis of biomarkers at baseline and the 12-week posttest only. These measures were administered at the community health centers by appointment at times other than the Qigong exercise sessions.
T. A. Cheng and Williams (1986) developed the 12-item CHQ-12 to assess community psychiatric illness. The instrument was derived from the General Health Questionnaire (Goldberg, 1972), with the addition of items that are of special relevance to ethnically Chinese populations. CHQ-12 items assess the following dimensions: somatic symptoms, anxiety and worry, social dysfunction, family relationships, and depression. Respondents use a 4-point Likert-type scale to rate their overall health during the past 2-week period. Total possible scores range from 0 to 12, with higher scores associated with worse self-perceived mental and physical health (T. A. Cheng, Wu, Chong, & Williams, 1990). The CHQ-12 was validated in a sample of community residents in Taiwan (Chen, Tsang, Chong, & Tang, 2000). For the present study, the Cronbach’s α was .82.
We measured body fat percentage using a digital body fat scale (Tanita Monitor Scales, TBF521). We asked participants to empty their bladder prior to taking this measurement.
The biomarkers we analyzed from the blood sample included hs-CRP (Hitachi-7600 automatic biochemistry analyzer), HbA1c (ultra high-performance liquid chromatography), plasma fasting sugar (Olympus AU2700 plus analyzer; Olympus CO Ltd., Tokyo, Japan), and lipid profiles (TC, TG, HDL-C, LDL-C, and very [V]LDL-C; Hitachi-7600 automatic biochemistry analyzer; Hitachi High-Technologies Corporation, Hitachi Naka city Japan). All testing was conducted at the laboratory of a medical center in southern Taiwan. Prior to the intervention and at 12 weeks’ posttest, we collected 10 ml of blood from the antecubital vein at 7–8 a.m. We asked participants to refrain from consuming food, coffee, tea, and alcohol and from smoking for at least 12 hr prior to the blood draw. Participants were permitted to drink pure water during this period. After participants completed blood sampling, we asked them to sit quietly for a 15- to 20-min observation period, after which we served them breakfast. Prior to the 6-week posttest, we sent the results of the baseline blood tests to each participant.
Statistical Analysis
We used IBM SPSS Statistics 17.0 (SPSS/IBM Inc., Chicago, IL) for all analyses. Descriptive statistics (frequency, mean, and standard deviation) were used to describe and summarize baseline data. Tests for differences between groups in terms of baseline characteristics and pretest variables included χ2 for categorical variables and two-sample t-tests for continuous variables. An intent-to-treat (ITT) analysis of the results was applied to provide unbiased assessment of treatment efficacy. ITT analysis requires all randomized participants to be included even if they did not fully adhere to the protocol because the lack of adherence might be treatment related (Son, Friedmann, & Thomas, 2012). This approach allowed the use of the entire ITT group while optimally estimating treatment effects in the presence of missing data in a statistically unbiased manner (Polit & Gillespie, 2010). To confirm that the statistical approach and missing data did not misrepresent the results, we also analyzed each outcome measure using a linear mixed model (LMM) of covariates in the longitudinal data. A mixed model with both fixed and random effects was used to investigate the treatment differences (fixed effects), while the correlated effects (random effects including the effect of clustering) were adjusted from the repeated measures. The level of significance accepted for all analyses was p < .05.
We used power analysis to determine the sample size. Extrapolating for a medium effect of 0.50 based on prior research (Tsang, Fung, Chan, Lee, & Chan, 2006), a minimum sample of 63 per group was needed to achieve a power of 0.80 with an alpha of .05 (Polit & Hungler, 2003). Therefore, we randomly selected and approached 84 experimental subjects and 61 control subjects for the study and ITT analyses.
Results
Of the 145 eligible participants, 139 completed the trial, including 82 in the Qigong group and 57 in the control group. The attrition rate was 2.04% in the Qigong group (2 individuals unwilling to participate after completing the 6-week posttest due to lack of interest) and 6.6% in the control group (3 individuals refused further contact and 1 was hospitalized for herniation of the intervertebral disc after completing the 12-week posttest). There were no reports of injuries from the Qigong exercise program. The attrition rate of 4.1% for the entire group may thus be considered low. We used an ITT analysis to provide an unbiased assessment of treatment efficacy. The majority of participants were women (73.8%), married (77.2%), living with their family (91.7%), and graduates of junior high school or less (44.8%). The mean age of participants was 62.05 (SD = 10.54) years (range 40–80 years). Participants’ average number of CAD risk factors and chronic diseases was 2.18 (SD = 1.06) and 1.15 (SD =1.22), respectively. The three most prevalent CAD risk factors in descending order were obesity (n = 84, 57.9%; mean waist to hip ratio = 0.91 for men and = 0.88 for women), sedentary lifestyle (n = 67, 46.2%), and hypertension (n = 54, 37.2%). The three most prevalent chronic diseases in descending order were hypertension (n = 46, 31.7%), degenerative arthritis (n = 27, 18.6%), and diabetes mellitus (n = 25, 17.2%). Most participants had a healthy lifestyle with no smoking (97.9%) or drinking habits (95.9%) and were regular exercisers (53.1%) who averaged 2.24 (SD = 2.46) exercise sessions per week. The most prevalent forms of exercise in descending order were walking (n = 36, 24.8%), folk dancing (n = 23, 15.9%), and stretching (n = 19, 13.1%). As shown in Table 1, we found no significant differences between the two groups in terms of demographic profile.
Comparison of Demographic Characteristics Between Groups.
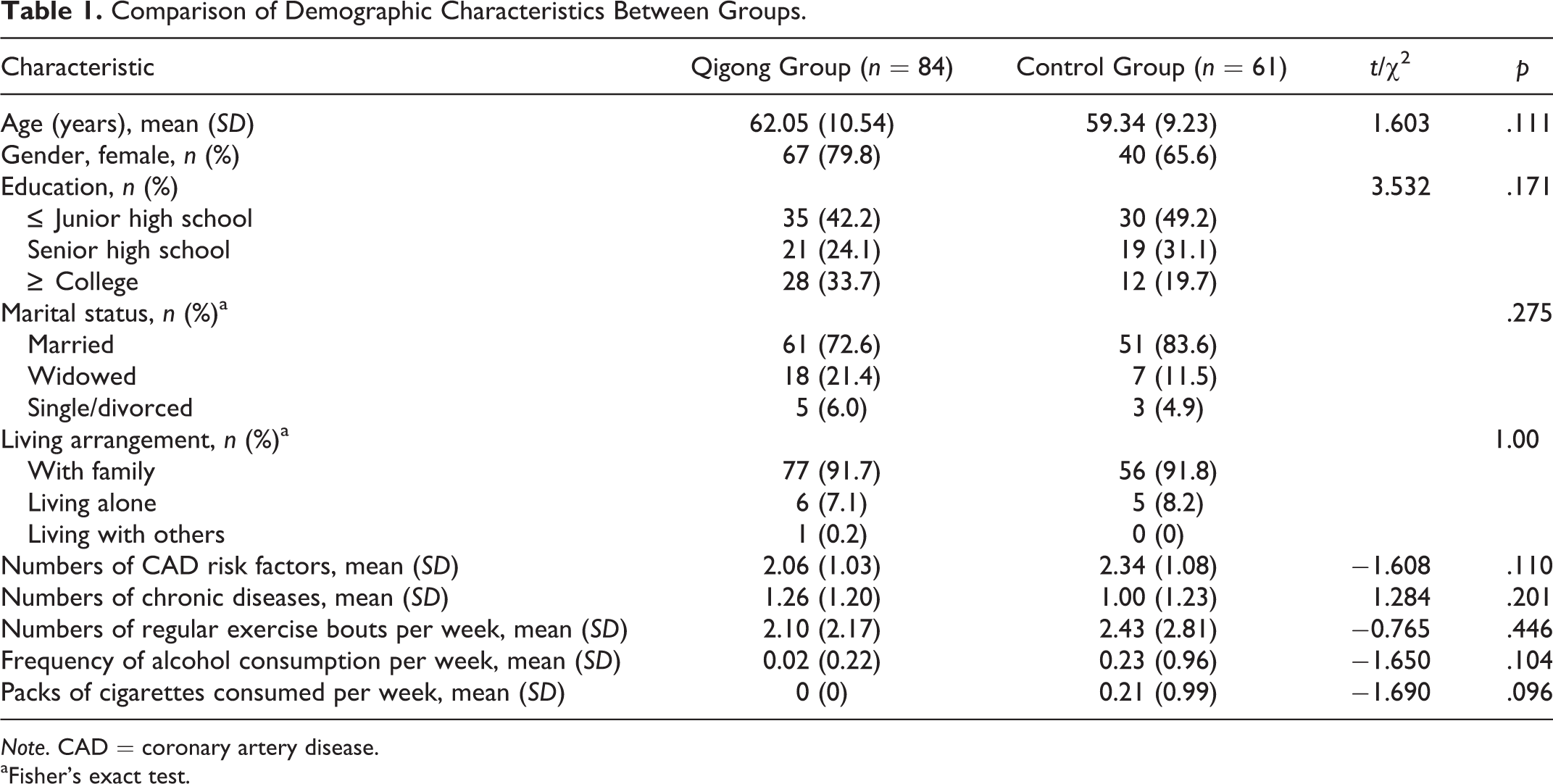
Note. CAD = coronary artery disease.
aFisher’s exact test.
Table 2 presents a comparison of the means and standard deviations for the outcome measures at baseline. There were significant differences in the CHQ-12 (p = .016) and LDL-C (p = .039) baseline values between the two groups. Participants in the Qigong group rated their mental and physical health more poorly on the 4-point scale and thus had higher scores on the CHQ-12 than their control group peers. Further, participants in the Qigong group had significantly lower pretest LDL-C levels than their control group peers. We used mixed model analysis to adjust for these potential confounders (i.e., baseline values of CHQ-12 and LDL-C). We found no significant differences between the two groups in the remaining outcome variables at baseline.
Comparison of Outcome Variables at Baseline Between Groups.
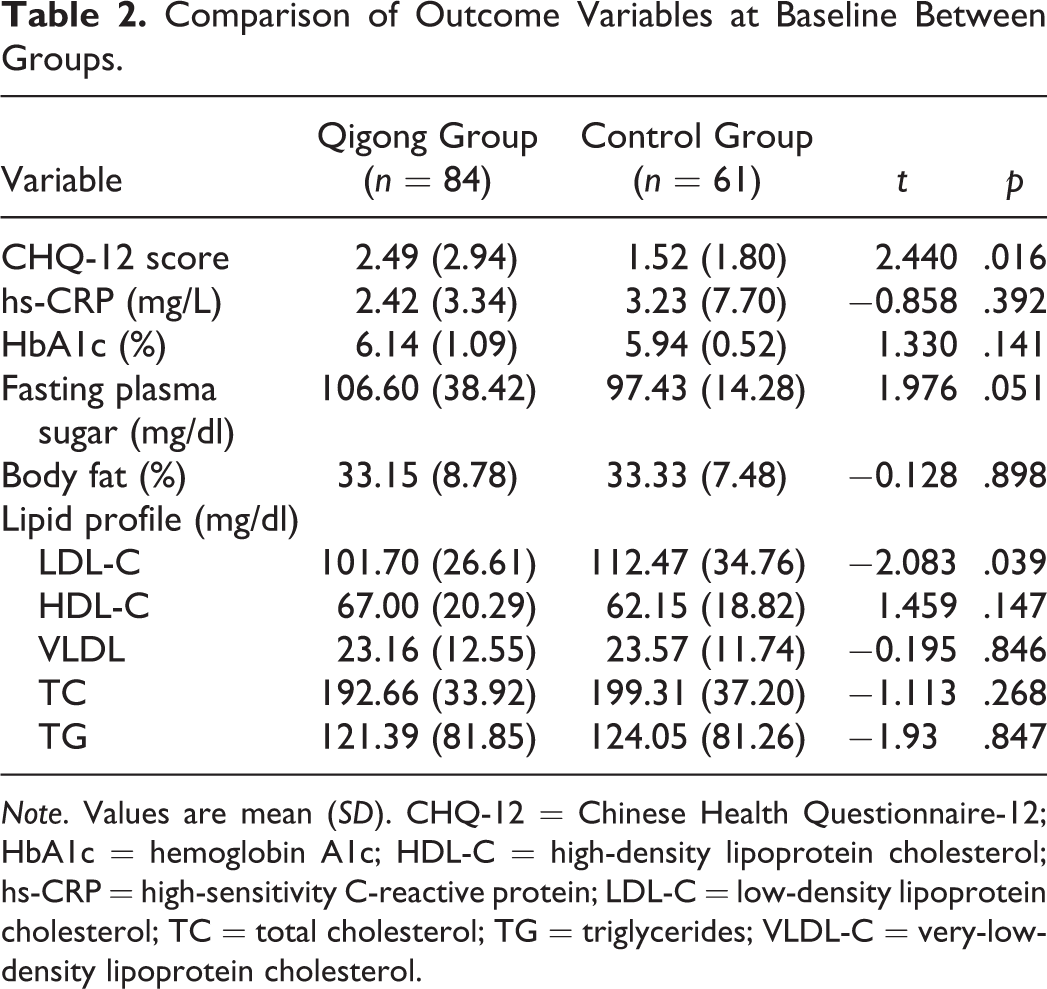
Note. Values are mean (SD). CHQ-12 = Chinese Health Questionnaire-12; HbA1c = hemoglobin A1c; HDL-C = high-density lipoprotein cholesterol; hs-CRP = high-sensitivity C-reactive protein; LDL-C = low-density lipoprotein cholesterol; TC = total cholesterol; TG = triglycerides; VLDL-C = very-low-density lipoprotein cholesterol.
Figure 2 depicts mean scores on the CHQ-12 for the Qigong and control groups from baseline through the 16-week follow-up. There were significant differences between the two groups at 6 and 12 weeks (p < .001), but not at the 16-week follow-up (p = .054), demonstrating that, while Qigong group participants improved significantly over the control group in terms of perceived mental and physical health at the midpoint and end of the intervention period (6 and 12 weeks), these improvements did not hold through the 16-week posttest. Figure 3 depicts mean body fat percentages for the Qigong and control groups from baseline through the 16-week follow-up period. Body fat percentage decreased by 2.0% in the Qigong group and increased by 0.3% in the control group from baseline to the 12-week posttest, with significant differences between groups at both time points (<.001). However, as with CHQ-12 score, by the 16-week posttest, the difference in mean body fat percentage between groups was no longer significant. Of note, we found a trend toward decreasing body fat percentages over time in both groups over the 16-week study period.
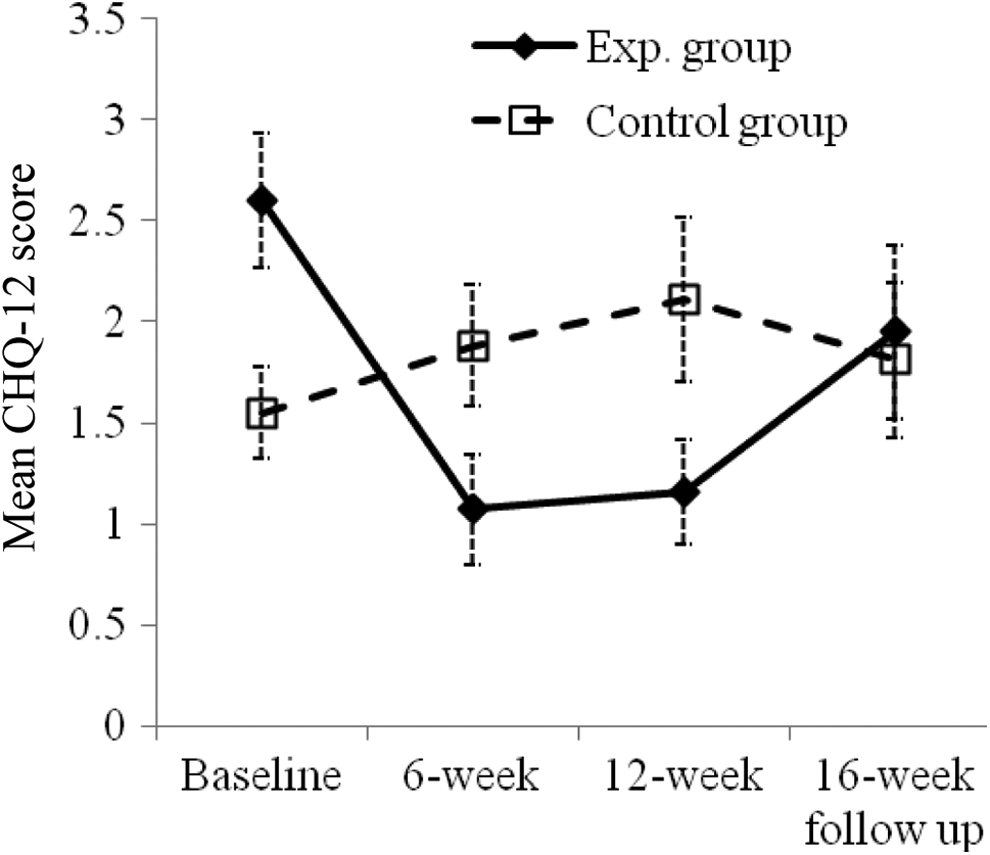
Mean scores on the Chinese Health Questionnaire-12 (CHQ-12) from baseline to 16-week posttest, with 95% confidence interval, for the Qigong (Exp.) and control groups.
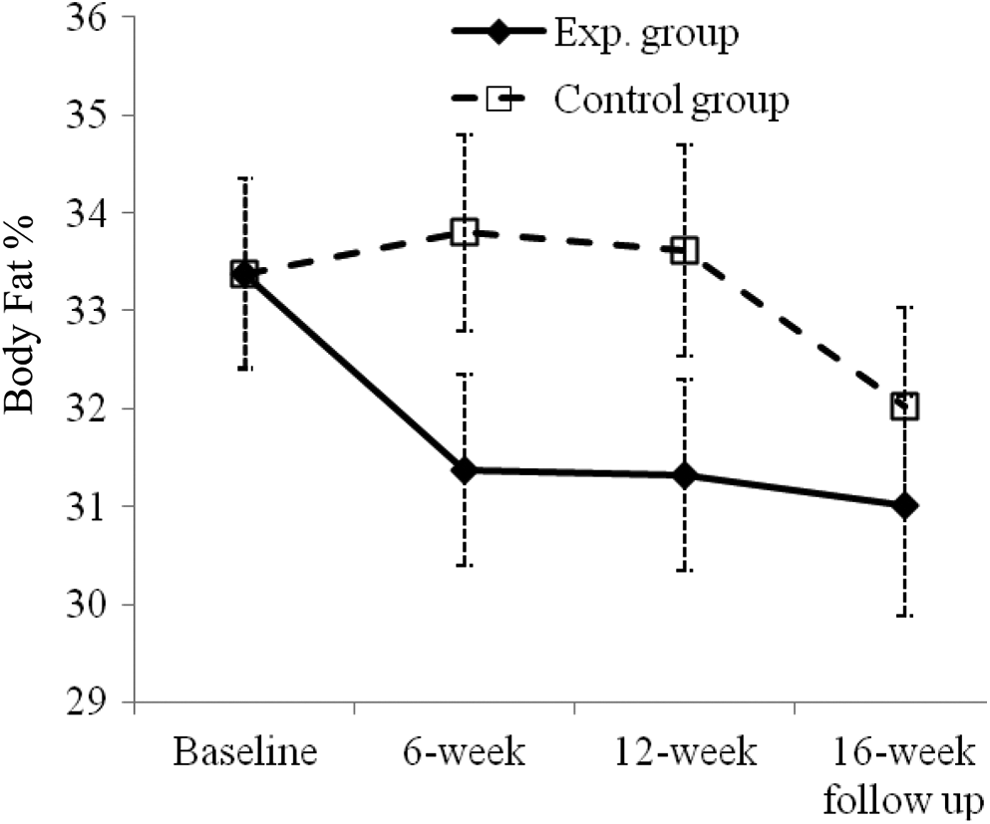
Mean body fat percentage from baseline to 16-week posttest, with 95% confidence interval, for the Qigong (Exp.) and control groups.
Table 3 shows the effects of the 12-week Qigong exercise intervention on selected biomarkers using mixed models analysis. We found significant differences in the mean changes in LDL-C, VLDL-C, TC, and TGs between the groups. There were, however, no significant differences in the mean changes in the other biomarker outcome measures between groups. The Qigong group had significantly lower mean levels of blood lipid profile measures than the control group at the 12-week posttest, with the exception of HDL-C level, which did not differ significantly between groups.
Between-Group Comparison of the Effects of Qigong Exercise on Biomarker Outcome Measures Using Linear Mixed-Model Analysis.
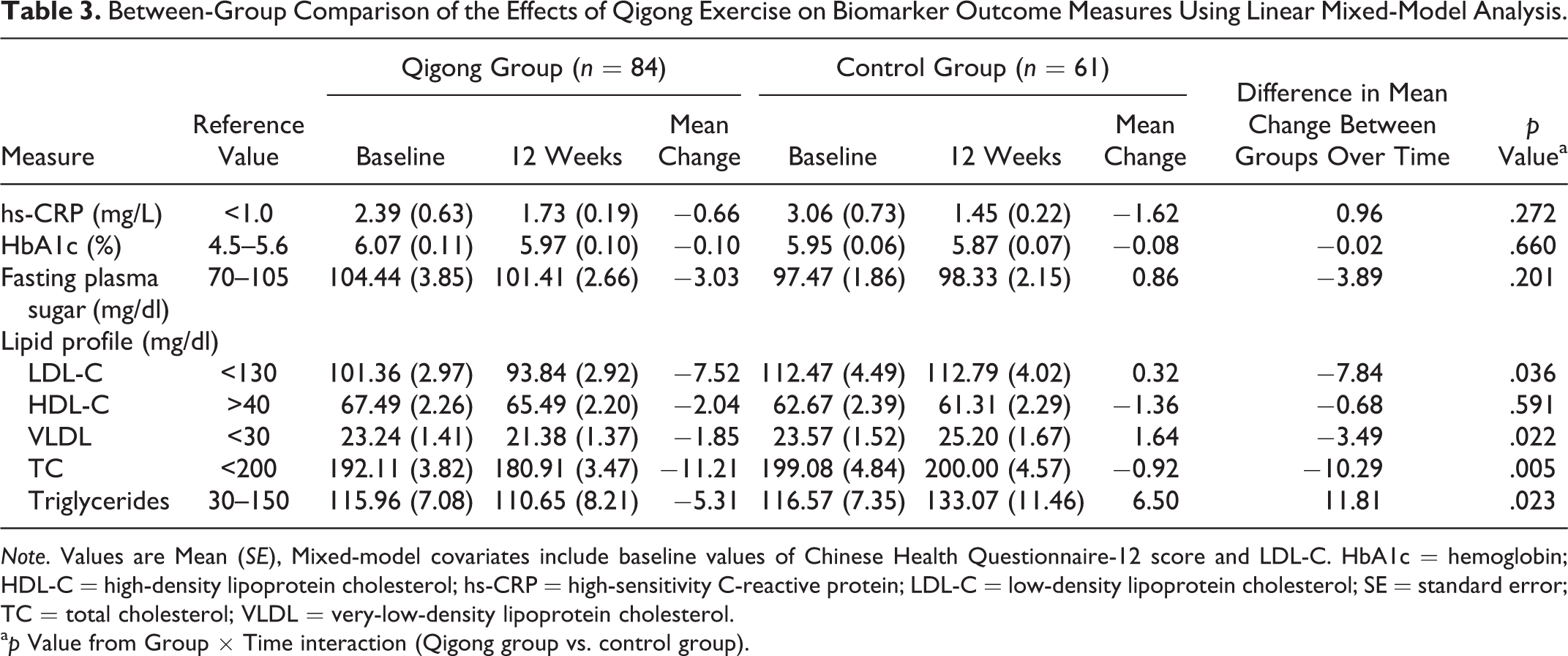
Note. Values are Mean (SE), Mixed-model covariates include baseline values of Chinese Health Questionnaire-12 score and LDL-C. HbA1c = hemoglobin; HDL-C = high-density lipoprotein cholesterol; hs-CRP = high-sensitivity C-reactive protein; LDL-C = low-density lipoprotein cholesterol; SE = standard error; TC = total cholesterol; VLDL = very-low-density lipoprotein cholesterol.
a p Value from Group × Time interaction (Qigong group vs. control group).
Discussion
Our findings in the present study suggest that a 12-week Qigong exercise program had positive effects on self-perceived mental and physical health, body fat percentage, and lipid profile in community-dwelling adults over 40 years of age who had at least one risk factor for CAD. We observed significant positive effects on self-perceived mental and physical health and body fat percentage after 6 weeks of practice, with the most significant effects realized at the 12-week posttest, while the lipid profile improved significantly after 12 weeks.
We used a clustered and randomized controlled trial design for this study because it was impossible to blind participants to their group allocation due to the nature of the intervention. We enhanced study rigor in the following ways: (1) the lead researcher (H.-M. H.) uniformly trained and carefully monitored the volunteer coteachers of the exercise program to guarantee the exercise quality and safety of individual elderly participants in this study. Further, a single investigator collected data for each group throughout the study in order to build a relationship of trust with participants. This arrangement likely contributed to the lower attrition rate (4.1%) in our study compared to similar studies (9.8% attrition rate in Liu et al., 2011; 8.3% attrition rate in Kuan, Chen, & Wang, 2012). (2) Research assistants involved in collecting and analyzing data were blinded to group allocation in order to minimize investigator bias. (3) We analyzed the entire ITT sample to maintain the integrity of the randomization process. (4) We used LMM analysis to reduce the impact of missing data. Finally, (5) we examined novel and multiple biochemical indicators of CAD risk, including hs-CRP, HbA1c, plasma fasting sugar, TC, TG, HDL-C, LDL-C, and VLDL-C.
The most prevalent CAD risk factor among our participants was obesity (57.9%). Our results suggest that Qigong exercise may be an effective and proactive intervention among this population because it reduced the percentage of body fat and improved self-perceived mental and physical health and well-being within 6 weeks of starting the intervention and improved dyslipidemia within 12 weeks of starting the intervention. These findings are supported by those of previous studies. For example, Lee, Lee, Kim, and Choi (2004) tested an 8-week Qigong intervention with hypertensive patients (N = 36) and found that the posttest levels of TC, HDL, and APO-A1 were significantly improved over pretest levels. In a single-group pre-posttrial, Liu et al. (2010) reported that a 12-week Tai Chi/ Qigong exercise training intervention (1–1.5 hr/session, 3 times per week for 12 weeks) significantly improved the perceived general health and depressive state of participants. Several possible mechanisms could explain the results of the present study. First, the natural release of stress hormones such as adrenaline, noradrenaline, and cortisol after physical exercise has been shown to decrease anxiety, fear, and depression (Lee, Lee, & Kim, 2003; Tsang et al., 2013). Second, self-hypnotic suggestion during meditation has been shown to enhance positive thoughts (Chow & Tsang, 2007). Third, taking part in group exercise has been shown to promote interpersonal relationships (Chan, Lee, Suen, & Tam, 2010). Any of these effects could lead to the improvement in self-perceived mental and physical health and well-being that we found in our Qigong participants. In addition, deep abdominal breathing and body movements have been shown to increase fuel metabolism and reduce body fat mass (Dumortier et al., 2003; Tsai, Chen, Lin, & Yeh, 2008). Also, regular aerobic exercise training can increase triacylglycerol oxidation and facilitate the release of fatty acid from adipose tissue and skeletal muscle (Gordon et al., 2008; Horowitz & Klein, 2000).
In following up on the longer term effects of a Qigong exercise program 4 weeks after the 12-week intervention had ended (i.e., 16 weeks posttest), we detected no significant differences between 16-week posttest values and baseline values of percentage of body fat or the self-perceived mental and physical health of Qigong group participants. Most participants had exercised regularly, usually in the form of regular walking, as part of their exercise regimen prior to participating in the present study. Thus, Qigong group participants may have discontinued their regular exercise (e.g., walking) in order to attend the Qigong exercise program, which is group oriented and instructor led and is a more complex activity than walking. Once the program was discontinued, participants in the Qigong group may have stopped practicing Qigong, which may explain the nonsignificant findings in the Qigong group for both variables at the 16-week follow-up. Guo and colleagues (2008) suggested that Qigong interventions be maintained for a period of more than 2 months in order to enhance the familiarity and proficiency of practitioners with the exercise movements. However, our findings support continuing Qigong exercise practice interventions for longer than 12 weeks in order to improve long-term benefits. Tsang, Fung, Chan, Lee, and Chan (2006) reported similar results, finding that an 8-week Qigong practice did not have a maintenance effect on depression evaluation at postintervention Weeks 4 and 8.
Although we found larger reductions in both HbA1c and fasting plasma sugar in the Qigong group than in the control group from baseline to the end of the 12-week intervention (−0.10 vs. −0.08 and −3.03 vs. 0.86, respectively), the differences in these reductions were not significant. This result partially echoes those of the study by Liu et al. (2010) in which they followed a 3-month Qigong training program in subjects with raised blood glucose levels and found no effects on fasting sugar levels, defined as blood sugar level measured after subjects not having had anything to eat or drink (except water) for at least 8 hr prior to testing (American Diabetes Association [ADA], 2014). Although in the present study we tested the fasting plasma sugar levels of participants after a short (8-hr) period of fasting, these levels were still subject to the influence of the quantity and types of foods participants had consumed prior to the start of the fasting period. We informed all participants of their baseline plasma sugar levels prior to the 6-week posttest, and it may be that this prior knowledge encouraged participants to self-regulate their food intake prior to blood sampling at the 12-week posttest, which may be a contributing factor in the nonsignificant change found in blood glucose levels.
The HbA1c test measures the average blood glucose for the past 2–3 months, with values between 5.7% and 6.4% indicative of prediabetes (ADA, 2014). This test is considered more stable in terms of accuracy of results than the fasting plasma sugar test. In general, the participants in the present study were classified as prediabetic based on their baseline values: mean = 6.14% in the Qigong group and mean = 5.94% in the control group. The HbA1c profile of participants was similar to that in Liu, Miller, Burton, Chang, and Brown’s (2011) study (mean = 6.05% in the Qigong group, mean = 5.85% in the control group). However, in Liu et al.’s study, the authors reported statistically significant changes (p = .042) in HbA1c after 12 weeks of Qigong practice, while we found no significant between- or within-group differences. This discrepancy in findings between the two studies may be related to normal exercise habits and/or medication use. Participants in Liu et al.’s study participated in a 12-week Qigong training program and used a supplemental video/DVD for home practice for 1–1.5 hr each day. Furthermore, the researchers recruited subjects with raised glucose level who were not currently using diabetes medication. Conversely, in the present study we used an instructor-led group exercise that was held 3 times per week with no home practice. Furthermore, we did not exclude from participation otherwise-qualified individuals who were taking diabetes medicine.
CRP levels vary seasonally, with higher values during the winter and spring and lower values during the summer (Sung, 2006). Although hs-CRP is more sensitive than CRP to inflammation, there have been few studies that have examined the effects of Qigong interventions on hs-CRP that we can compare to ours. In our study, we ran the intervention from winter to spring (December 2011 to March 2012), while we collected data from the control group from winter to summer (January 2012 to August 2012). While the control group exhibited a greater reduction in hs-CRP than the Qigong group (−1.62 vs. −0.66, respectively), the difference between the changes in mean in the groups was not significant (p = .272), a finding that is consistent with that of the study by Chang, Koo, Chen, Lu, and Lin (2013) on the effects of a Tai Chi exercise intervention on hs-CRP. In contrast, Oh et al. (2012) used a 10-week medical Qigong exercise intervention with cancer patients and reported significant reductions in CRP levels. The difference in the results may be related to exercise dosage, sample population, or Qigong intervention format. Oh and colleagues asked the intervention group participants to attend at least 90 min of exercise sessions per week and encouraged them to do home practice for at least 30 min each day. They excluded participants who withdrew from the study from analyses in the final sample and had adopted a medical Qigong intervention that was specially designed for cancer patients. In contrast, the exercise program we used in the present study was a 60-min session that we conducted 3 times per week, we analyzed the entire ITT sample, and the exercise program was designed for a middle-aged and older aged population. Previous reports have shown that younger populations, longer intervention periods (over 6 months), and higher BMI values (≥ 25 kg/m2) are more likely to generate lower hs-CRP values (Kondo et al., 2006; Michigan, Johnson, & Master, 2011). Future studies should adopt long-term (> 6-month) interventions, evaluate the impact of Qigong exercise on hs-CRP in different age-groups and during different seasons, and use repeated measures.
The main limitations of the present study were that individuals were not randomly assigned to the two groups and that we did not limit the control group to sedentary subjects. The Qigong intervention used in our study should be further optimized to maximize community participation. Also, while the program of Qigong exercise integrates body movements, deep abdominal breathing, and meditation, the component(s) responsible for changes in the outcome measures remains unclear. Rogers, Larkey, and Keller (2009) indicated that uncertainty regarding mechanisms is a fundamental problem in trying to interpret the results of Qigong interventions. In addition, while our results may be more relevant to females than males due to the higher proportion of female participants, males with CAD have a higher rate of mortality than their female peers (Cheng et al., 2005). Further studies should enroll more male participants and longitudinally trace the efficacy of the Qigong intervention in decreasing the incidence of CAD events.
In summary, this study supports Qigong exercise as an accessible and effective intervention for community-dwelling adults aged 40 and over. Thus, we recommend the use of 12-week Qigong exercise programs to reduce the risk of CAD for male and female adults as they age. Furthermore, the results of this study enhance scientific knowledge regarding the positive influence of Qigong exercise on the biomarkers of CAD risk. Because CAD is the primary clinical outcome of metabolic syndrome (i.e., obesity, dyslipidemia, and hypertension), Qigong exercise may serve as an effective and noninvasive intervention, not only for managing asymptomatic individuals with CAD risk factors but also for reducing risk in those with metabolic syndrome. These findings have significant implications for nurses and other health-care professionals who wish to incorporate this safe, nonpharmacological intervention into clinical practice related to risk factors of CAD. This intervention program is sustainable and could be promoted in community settings to enhance peoples’ health quality.
Footnotes
Author Contribution
Hsuan-Man Hung contributed to conception and design, acquisition, analysis, and interpretation; drafted the manuscript; critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Shu-Hui Yeh contributed to design and acquisition, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Chung-Hey Chen contributed to conception and design and analysis and interpretation, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.