
Abstract
Objectives:
To explore whether newborns born via Cesarean section have a weaker intraoral vacuum compared with those born vaginally and to determine whether a weaker intraoral vacuum is related to a delayed onset of lactation.
Methods:
For this prospective cohort study, 71 mother–infant dyads were enrolled and divided into birthing groups, vaginal or Cesarean. The newborn intraoral vacuum was measured via a tube placed alongside the nipple and connected to a pressure sensor during a breast-feeding session within the first 24 hr after birth. Onset of lactation was confirmed by maternal perception of breast fullness. The intraoral vacuum and its relationship with the onset of lactation were analyzed.
Conclusion:
Cesarean section may weaken newborns’ intraoral vacuum within the first 24 hr after birth. Stronger intraoral vacuum was related to earlier onset of lactation. Early intervention aimed at the weaker intraoral vacuum should be provided to promote the onset of lactation.
In China, the 6-month exclusive breast-feeding rate is less than 30% (Guo et al., 2013; Zheng et al., 2014). Research has shown Cesarean delivery to be an independent risk factor for not breast-feeding (Zanardo et al., 2010), and the early breast-feeding rate among mothers who delivered by Cesarean was only 0.57 times that of mothers giving birth vaginally (Prior et al., 2012). Currently, the global Cesarean section rate is 26.3–28.9% of births (Chalmers et al., 2010; Mittal, Pardeshi, Mayadeo, & Mane, 2014), while it has reached 60% in some areas of China (Bogg, Huang, Long, Shen, &Hemminki, 2010).
Birth by Cesarean section is a risk factor for delayed onset of lactation (Dewey, Nommsen-Rivers, Heinig, & Cohen, 2003). The onset of lactation, characterized by the start of copious milk production, is key to early successful breast-feeding (Brownell, Howard, Lawrence, & Dozier, 2012; Liu et al., 2013), and the risk of early cessation of breast-feeding increases with delayed onset of lactation (Hruschka, Sellen, Stein, & Martorell, 2003; Liu et al., 2013). Nevertheless, the mechanism by which Cesarean section affects the onset of lactation is still unclear.
Newborns’ continuous sucking is the major stimulus to promote milk generation. Early and frequent sucking (Moore, Anderson, Bergman, & Dowswell, 2012) and correct positioning and attachment (Cadwell, 2007) have been recommended as significant measures to promote the onset of lactation and establish breast-feeding. However, two randomized clinical trials (Gouchon et al., 2010; Nolan & Lawrence, 2009) verified that even when newborns delivered by Cesarean section began sucking within 2 hr of birth or when they were in the anesthesia recovery room, the breast-feeding rate at discharge and 1 month was not improved. The primary characteristics of infant sucking are strength, duration, and frequency. The World Health Organization (2009) suggests that 8–12 breast-feeding sessions per day are needed within the first several days after birth to promote the onset of lactation. However, few studies have explored whether the effectiveness of sucking originates from its duration, frequency, strength or some combination of these characteristics.
The strength of sucking helps to establish lactation. As the tongue lowers during a suck cycle, milk flows freely into the intraoral space (Sakalidis, Williams, Garbin, et al., 2013). Furthermore, as the tongue continues lowering, a negative pressure is generated, which researchers report as the main driving force for removing the milk from the breast (Geddes, Kent, Mitoulas, & Hartmann, 2008). The newborns’ continuous sucking is the main stimulus for lactation (Kent, 2007).
Researchers have observed that newborns delivered via Cesarean section have a different sucking dynamic compared to those delivered vaginally (Sakalidis, Williams, Hepworth, et al., 2013). We hypothesized that delivery via Cesarean section detrimentally affects the sucking strength of newborns during breast-feeding, resulting in a delayed onset of lactation. Therefore, in the present study, we explored whether newborns delivered via Cesarean section have a weaker intraoral vacuum compared to those born vaginally.
Method
Design
We used a prospective cohort study design and convenience sample in this research, with groups defined by delivery mode. The ethics committee of Nantong University approved the study protocol (No. 2014-069), and the study was registered in the Chinese Clinical Trial Registration (No. ChiCTR-OOC-14005294).
Participants
We carried out the study in the Affiliated Hospital of Nantong University, a comprehensive university teaching hospital with 2,002 beds. The number of newborns delivered in the hospital accounts for 21% of the total delivered in Nantong City. We recruited healthy single-birth primipara aged 20–35 years. Study participants included those who delivered healthy full-term newborns with Apgar scores higher than 7 and were willing to breast-feed their babies. We excluded women with breast-feeding contraindications, dyads who experienced mother–infant separation, mothers who were using artificial feeding, those who had a history of breast surgery/injury, women with mammary dysplasia, women with a flat or inverted nipple, women with complications related to pregnancy/labor, those who smoked during pregnancy, and women with a pregestational body mass index (BMI) > 27 kg/m2 (obesity). Before enrollment, we provided both verbal and written information regarding the aim and procedures of the study to all potential participants, informed them of their right to withdraw from the study at any time without citing any reason, and obtained written informed consent from each participant.
Mothers in the vaginal group had a normal vaginal delivery without dystocia, the use of analgesia, or midwifery forceps during labor. Those in the Cesarean group had a Cesarean delivery without postoperative patient-controlled analgesia (PCA). We excluded women who had PCA because of the possible confounding effect of anesthesia on the newborns’ intraoral vacuum.
Mothers who delivered via Cesarean section received epidural anesthesia comprising 15–20 ml of 2% lidocaine and 5 ml of 0.75% ropivacaine. If necessary, an additional 5-ml dose of ropivacaine was given to secure analgesia. The hospital is baby friendly with obstetric rooming-in wards. In the cases of vaginal delivery, newborns received umbilical care and a physical assessment and were wiped dry and dressed after birth. Immediately after wiping and dressing, a skin-to-skin contact with mother and first breast-feeding happened. In contrast, after Cesarean delivery, newborns had a short period of skin-to-skin contact with the mother in the operating room before being sent to the delivery room for the same routine care that vaginally delivered newborns received. Newborns delivered via Cesarean section received the first breast-feeding, on average, just 1 hr later compared to vaginally delivered infants, when the mother was transferred to the ward. For all mothers and infants, the nurse assisted with positioning, attachment, and breast-feeding on demand.
Measurement
Intraoral vacuum
We measured the strength of each infant’s intraoral vacuum right at the start of breast-feeding, when the sucking was stable and continuous, using Geddes’s method (Geddes et al., 2008), as depicted in Figure 1. A tube (450 mm, 1.3 mm inside diameter × 2.7 mm outside diameter) was placed alongside the nipple and connected to a pressure transducer (TCT-1202; Lenosensor Co., Ltd., Beijing, China). The transducer was connected via an interconnect cable to an amplifier bridge (Lenosensor Co., Ltd., Beijing, China), and the output was recorded using an analog-to-digital converter (XSTC09; Lenosensor Co., Ltd.), Power Lab signal collection and data analysis system (T900; Lenosensor Co., Ltd.), and software package (M400 data collection management software, version M4600D(#0100); Lenosensor Co., Ltd.). The tube was removed immediately after the measurement. This method allowed for the direct measurement of the vacuum. Repeatability error of the pressure sensor was 0.02%, and the comprehensive precision was 0.5% full scale.
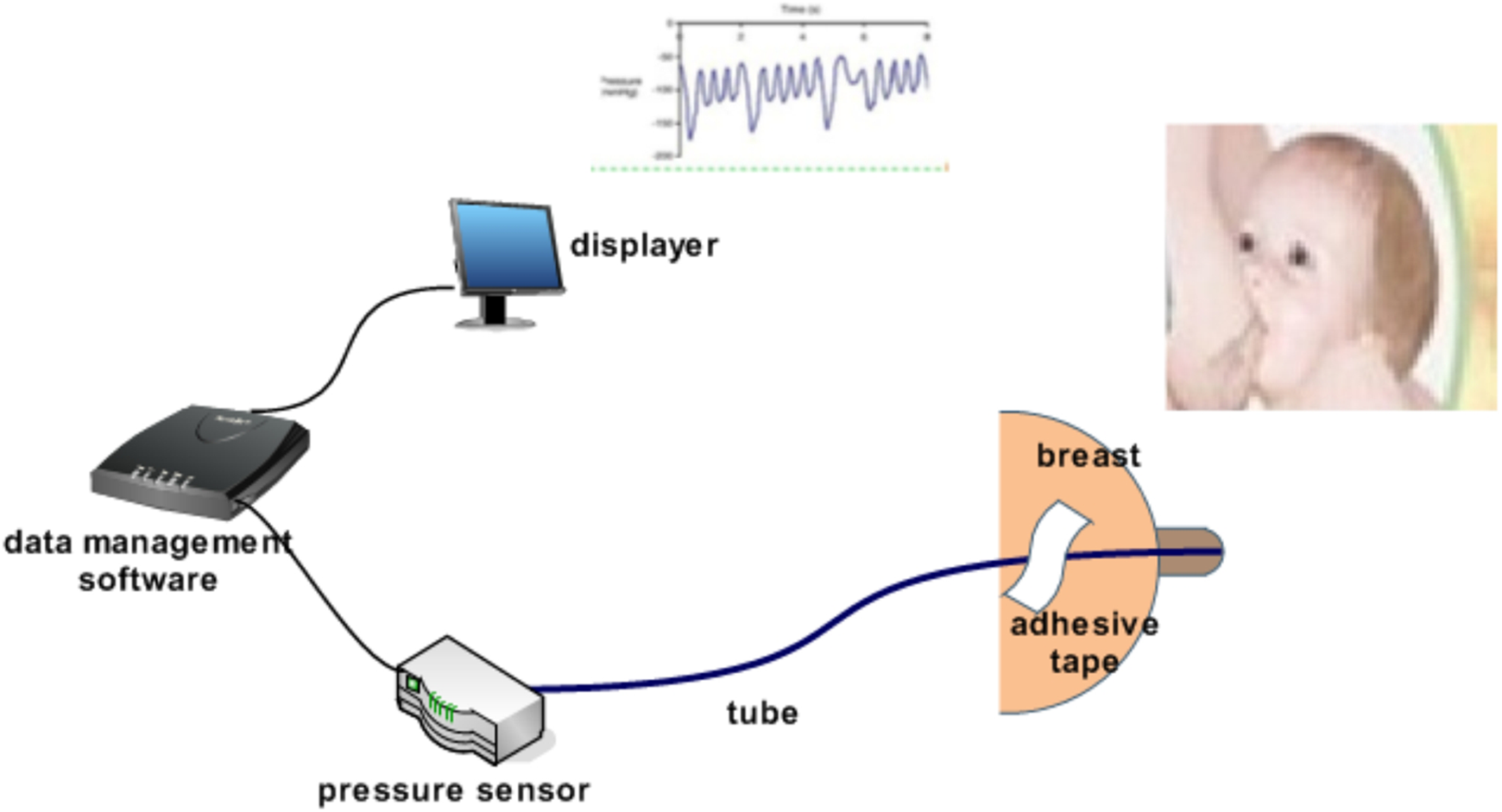
Measurement of the newborn’s intraoral vacuum.
We measured the intraoral vacuum within the first 24 hr after birth in order to capture the effects of Cesarean delivery. The half-life clearance is 1.8–4.2 hr for ropivacaine (Kitayama et al., 2014) and 1.5–2.0 hr for lidocaine (Shiroma et al., 2014). Usually five half-lives are required for plasma clearance (Rosenberg, Veering, & Urmey, 2004). Therefore, much of the first 24 hr after birth was influenced by the surgery.
We made the recordings when the newborns were willing to suck. The nurse first evaluated the readiness of the infant to suck using the Chinese version of the Infant Breastfeeding Assessment Tool (Huang, Lee, Huang, & Gau, 2009). The measurement began only if the baby was sucking with no stimulation or mild stimulation such as unbundling, patting, or burping. If the infant did not indicate a readiness to suck, we tried again during the next feeding. In order to capture the intraoral vacuum when the baby was hungry, we attempted to measure 2 hr after the preceding breast-feeding session. Assisted by nurses to ensure correct positioning and attachment for the breast-feeding infant, the puerperae lay on the bed in a lateral position for measurement. Measurement began when the baby had a regular and stable sucking rhythm. In consideration of the potential risk that prolonged measurement on the first day after birth might pose to sucking behavior, the detection lasted for only 30 s. Given that the sucking rate of newborns is typically 1.7 ± 0.2 sucks/s (Lindner, 1991), 30 s was sufficient to allow for adequate data collection. Prieto et al. (1996) reported that the intraoral vacuum peaked at −199 mmHg for the first breast then weakened to −187 mmHg on the other breast based on continuous measurement of an entire breast-feeding session (7 min on average). Therefore, our measurement protocol satisfied a 10% detection error, meeting the requirements of the ethics committee.
Using data collection management and analysis software, we calculated the minimum (peak intraoral vacuum), maximum (baseline intraoral vacuum), and mean pressures (mean intraoral vacuum; average of all the peak and baseline intraoral vacuums) within the 30-s measurement interval for each infant.
Onset of lactation
Beginning at 24 hr after delivery and continuing every 4 hr until the onset of lactation, we questioned mothers regarding if and when they noticed a sudden feeling of fullness in their breasts to confirm the onset of lactation (Parker, Sullivan, Krueger, Kelechi, & Mueller, 2012; Perez-Escamilla & Chapman, 2001). This approach, based on maternal report of when her breasts felt “noticeably fuller” on a scale of 1–5 (where 1 = no change since giving birth, 3 = noticeably fuller, and 5 = uncomfortably full), has been validated (Perez-Escamilla & Chapman, 2001).
Prenatal, delivery, and postpartum data
We investigated a wide range of variables as potential confounders of intraoral vacuum or onset of lactation, including maternal education, household income, marital status, maternal age, and other demographic factors, which we collected via a face-to-face interview. We also assessed pregnancy-related information, including prepregnancy maternal BMI, gestational BMI gain, health problems during pregnancy, attendance at antenatal care appointments, and delivery-related factors, including delivery mode, anesthesia with Cesarean delivery, and newborn birth weight, gender, and gestational age, which we collected via medical records. Finally, we examined postpartum variables such as time to first breast-feeding, duration of first breast-feeding, breast-feeding frequency within 24 hr, breast-feeding duration within 24 hr, supplementation with formula within 24 hr, baby’s admission to the neonatal department, and onset of lactation and maternal psychological factors. We gathered the feeding data from nursing records kept by nurses we had trained for data collection before the start of the study. During their routine checks on the newborns (every 30 min to 1 hr on the first day after delivery and at least every 2 hr thereafter), the nurses asked the parents or caregiver about the time and duration of each breast-feeding session and the time and volume of each formula feeding.
Breast-feeding frequency refers to the number of breast-feeding sessions in a 24-hr period. If the infant’s sucking was off and on, we only recorded the sucking duration and counted the sum as one sucking episode, even if the newborn’s mouth left the breast temporarily. We measured the mother’s stress level using the Chinese version of the Edinburgh Postnatal Scale (Lee et al., 1998), a self-evaluation tool, 3 days after delivery.
Statistical Analysis
The sample size was calculated in the following way based on preliminary experiments. A two-sided level of significance of .05 and power of 0.9 was defined. According to data from 21 newborns in preliminary experiments, the peak intraoral vacuum was −19 kPa for the vaginal group and −15 kPa for the Cesarean group; the standard deviation (SD) in the Cesarean group was 7.1 kPa. Factoring in a 20% increase in sample size to account for dropouts, 33 subjects were needed for each group.
The data were imported into Epidata 3.1 and analyzed with Stata 10.0. Continuous variables with normal distribution were expressed with mean and standard deviation and analyzed with two independent samples t-test. Rank sum test was adopted for data with abnormal distribution and results were expressed using median and interquartile range. χ2 test was used for grouped data and rank sum test for ranked data.
Allowing for the imbalanced baseline and confounding effect of formula intake, we conducted covariance analysis for the adjusted intraoral vacuum comparison. We controlled the variables of maternal age, gestational BMI gain, antenatal care interviews, time to first breast-feeding, formula volume, and formula frequency. Multivariate regression was adopted for analysis of the relationship between the intraoral vacuum and the onset of lactation. In the multivariate regression model, variables such as maternal age, gestational BMI gain, antenatal care interview, time to first breast-feeding, formula volume, formula frequency, and delivery mode were controlled as confounding factors.
Results
The flow of participants from eligibility to data analysis is shown in Figure 2. Of 476 potential dyads evaluated, 124 were eligible. Of these, 53 (42.7%) mothers refused to participate, 17 (33.3%) who delivered vaginally and 36 (49.3%) who delivered via Cesarean section. There was no difference in the response rate between the two groups (χ2 = 3.133, p = .077). Similarly, there was no difference in the baseline information between the mothers who participated and those who refused (age t = −1.42, p = .16; nationality χ2 = 1.78, p = .18; education χ2 = 0.66, p = .42; employment χ2 = 1.46, p = .23). Among the 71 dyads who enrolled, 2 newborns were transferred to the neonatal department because of bilirubinemia before the maternal onset of lactation. The mother–infant separation may have skewed the results for onset of lactation. We included the data of these 71 dyads in the statistical analyses.
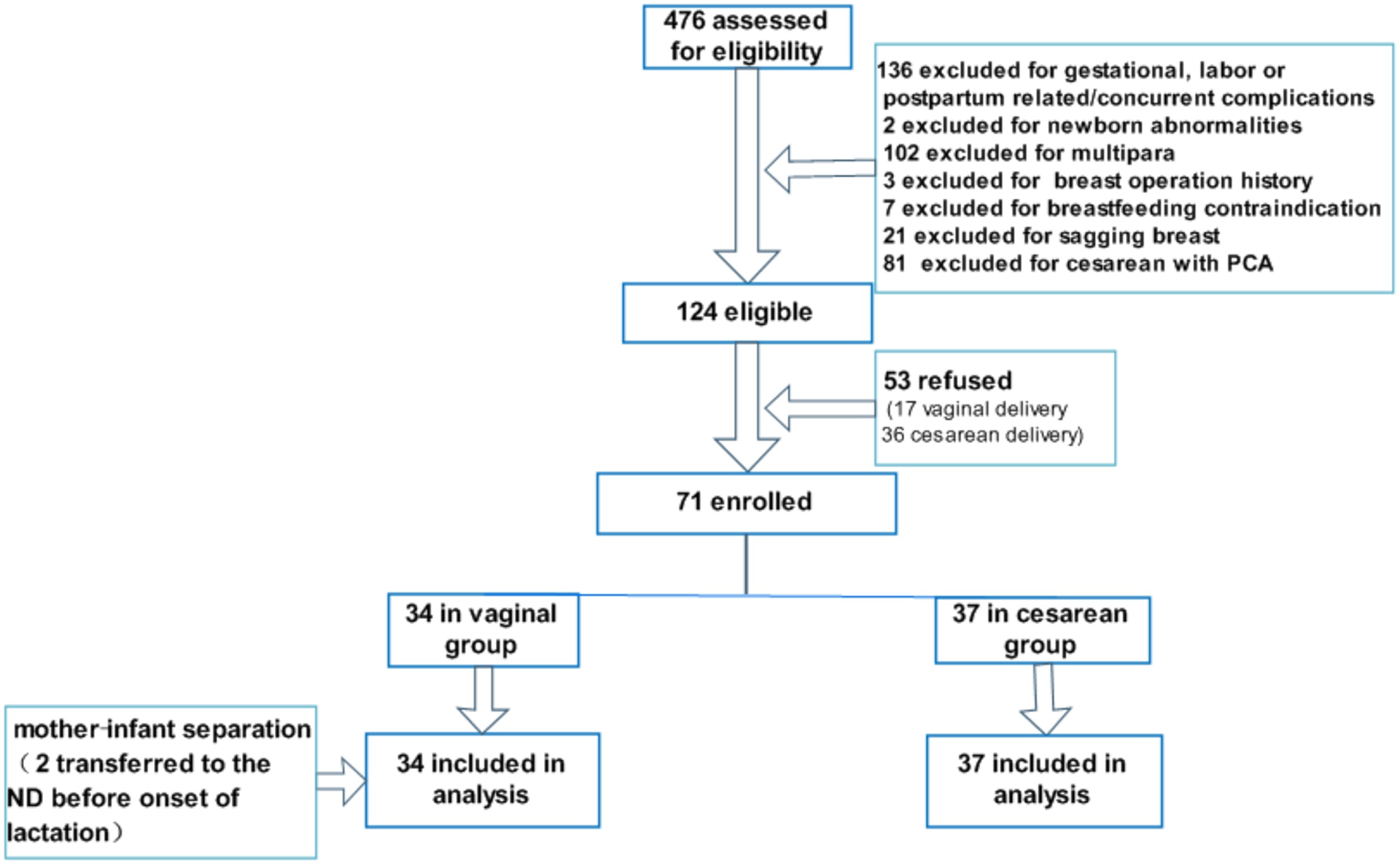
Flow of mother–infant dyads through study. ND = neonatal department; PCA = patient-controlled analgesia.
Mothers in the vaginal group were younger (p = .001), more were unemployed (p = .040), their BMI increased less over the gestational period (p = .005), and they had more antenatal care interviews (p = .021) than those in the Cesarean group (Table 1). As shown in Table 2, both the time to first breast-feeding (t = −11.484, p = .000) and the onset of lactation (52.94 ± 16.80 hr vs. 61.78 ± 10.90 hr, respectively; p = .010) were earlier in the vaginal group than that in the Cesarean group.
Demographic Information for Mother–Infant Dyads.a
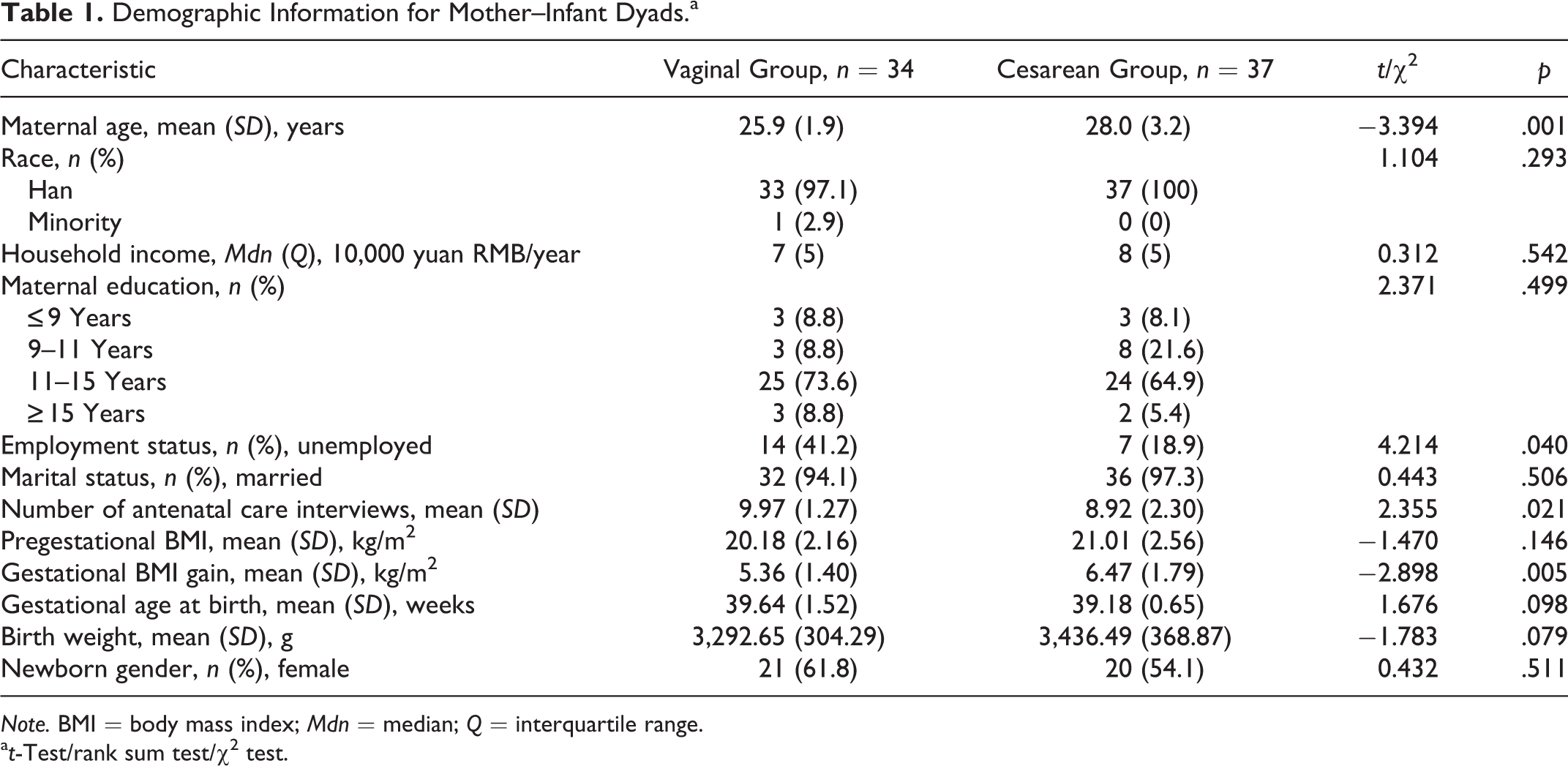
Note. BMI = body mass index; Mdn = median; Q = interquartile range.
at-Test/rank sum test/χ2 test.
Breast-Feeding Characteristics Within 24 Hr After Birth.a
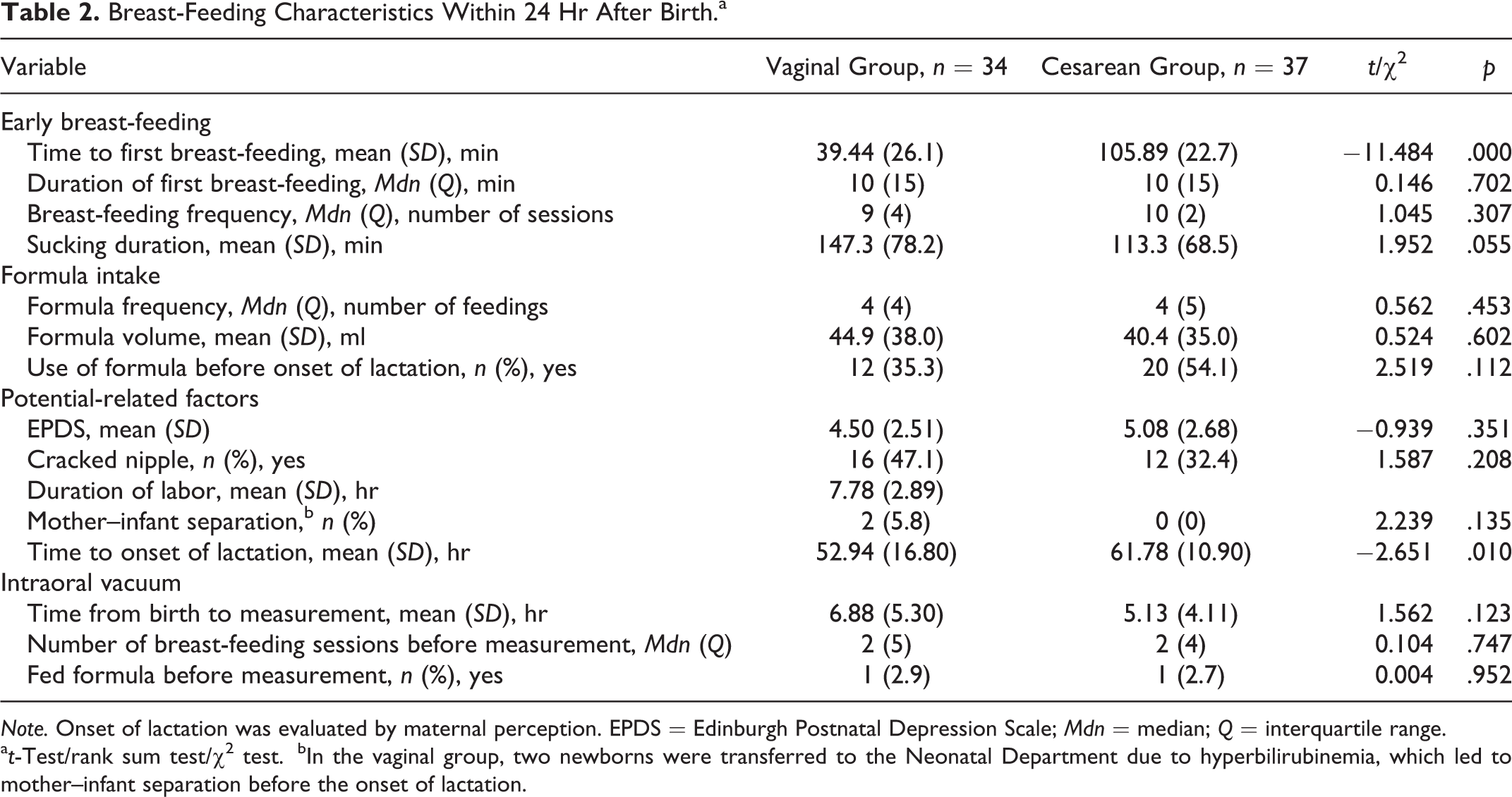
Note. Onset of lactation was evaluated by maternal perception. EPDS = Edinburgh Postnatal Depression Scale; Mdn = median; Q = interquartile range.
at-Test/rank sum test/χ2 test.
bIn the vaginal group, two newborns were transferred to the Neonatal Department due to hyperbilirubinemia, which led to mother–infant separation before the onset of lactation.
Intraoral Vacuum
The peak, mean, and baseline intraoral vacuums in the vaginal group (peak = −19.89 ± 7.69 kPa; mean = −10.60 ± 4.79 kPa; and baseline = −2.30 ± 2.61 kPa) were significantly stronger than those in the Cesarean group (peak = −13.42 ± 6.26 kPa; mean = −7.68 ± 2.80 kPa; and baseline = −1.22 ± 0.66 kPa), as shown in Table 3. After adjusting for potential confounding factors, the peak and baseline intraoral vacuums in the vaginal group were still significantly stronger than those in the Cesarean group, but there was no statistical difference in the mean intraoral vacuum (Table 4). Using covariate analysis, we found that the frequency of formula feeding in the first 24 hr after birth was related to peak and mean intraoral vacuum; the volume of formula fed was related to the mean intraoral vacuum; and the gestational BMI gain was related to the baseline intraoral vacuum. Maternal age, the number of antenatal care interviews, and time to first breast-feeding session had no relationship with the peak, mean, and baseline intraoral vacuum, as shown in Table 4 note.
Strength of Newborns’ Intraoral Vacuum Within 24 Hr of Birth.

Adjusted Strength of Newborns’ Intraoral Vacuum After Controlling for Confounders.a
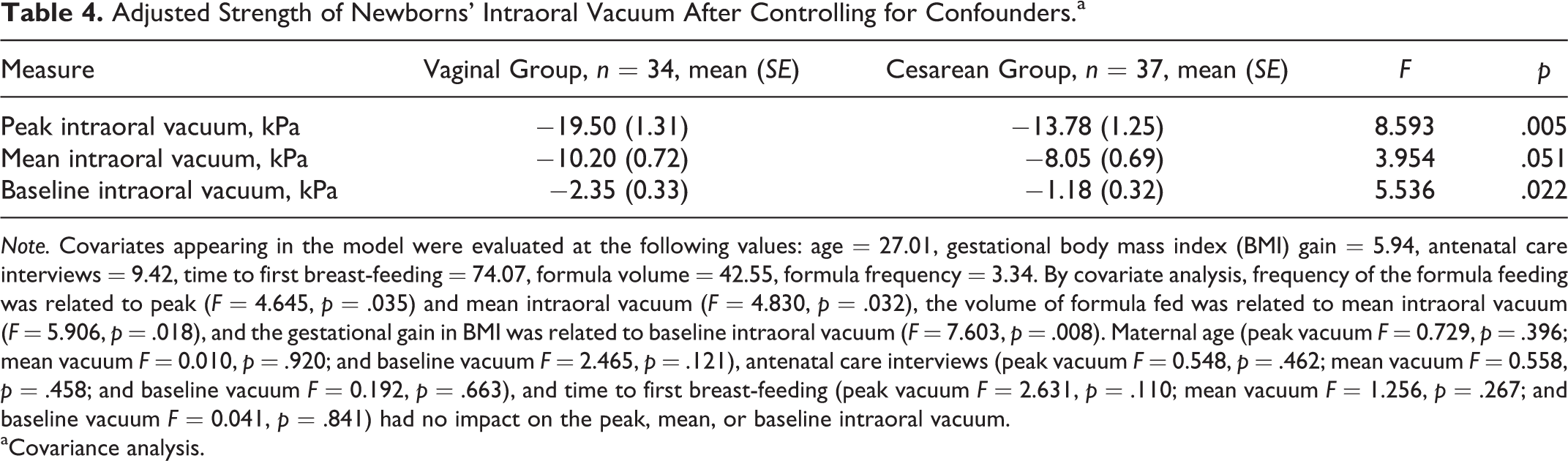
Note. Covariates appearing in the model were evaluated at the following values: age = 27.01, gestational body mass index (BMI) gain = 5.94, antenatal care interviews = 9.42, time to first breast-feeding = 74.07, formula volume = 42.55, formula frequency = 3.34. By covariate analysis, frequency of the formula feeding was related to peak (F = 4.645, p = .035) and mean intraoral vacuum (F = 4.830, p = .032), the volume of formula fed was related to mean intraoral vacuum (F = 5.906, p = .018), and the gestational gain in BMI was related to baseline intraoral vacuum (F = 7.603, p = .008). Maternal age (peak vacuum F = 0.729, p = .396; mean vacuum F = 0.010, p = .920; and baseline vacuum F = 2.465, p = .121), antenatal care interviews (peak vacuum F = 0.548, p = .462; mean vacuum F = 0.558, p = .458; and baseline vacuum F = 0.192, p = .663), and time to first breast-feeding (peak vacuum F = 2.631, p = .110; mean vacuum F = 1.256, p = .267; and baseline vacuum F = 0.041, p = .841) had no impact on the peak, mean, or baseline intraoral vacuum.
aCovariance analysis.
Relationship Between Intraoral Vacuum and Onset of Lactation
Multivariate regression analysis showed that strength of intraoral vacuum was strongly correlated with the onset of lactation when other variables were controlled: maternal age, gestational BMI gain, antenatal care interviews, time to first breast-feeding, formula volume, formula frequency, and delivery mode (Table 5). That is, stronger intraoral vacuum was related to earlier onset of lactation.
Relationship Between Strength of Intraoral Vacuum and Onset of Lactation.a
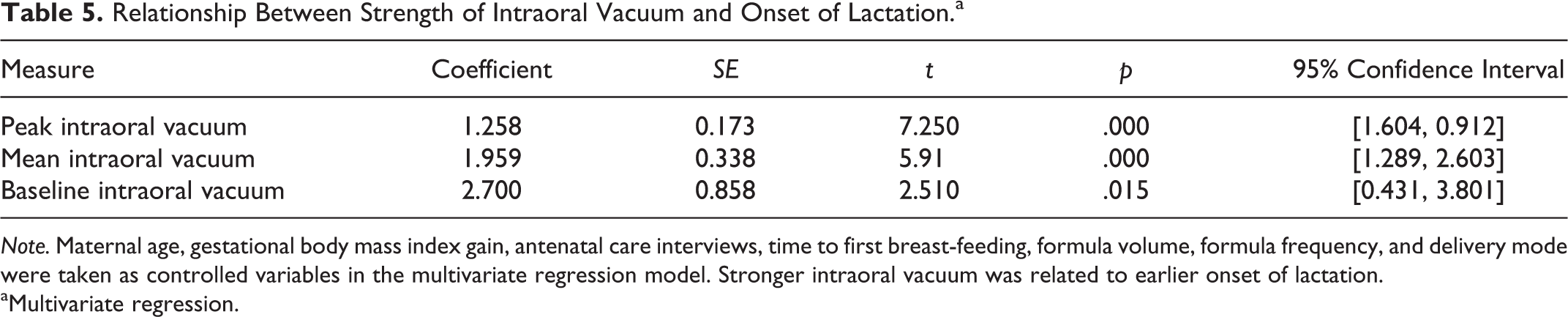
Note. Maternal age, gestational body mass index gain, antenatal care interviews, time to first breast-feeding, formula volume, formula frequency, and delivery mode were taken as controlled variables in the multivariate regression model. Stronger intraoral vacuum was related to earlier onset of lactation.
aMultivariate regression.
Discussion
Cesarean Section Weakened Newborns’ Intraoral Vacuums
In the present study, newborns had a weaker peak intraoral vacuum after Cesarean section than after vaginal birth when confounding variables were controlled. Sakalidis et al. (2013) discovered that infants delivered by Cesarean section showed a broader range of tongue movement, faster suck rates, and fewer central nervous system responses than those delivered vaginally. Geddes, Kent, Mitoulas, and Hartmann (2008) found that newborns’ posterior tongue moves downward during sucking, generating instantaneous negative oral pressure. When the posterior tongue reaches the lowest point, the negative pressure sensor detects the peak intraoral vacuum and milk flows into the oral cavity. Given these findings, we propose that the increased rate of tongue movement demonstrated by infants born via Cesarean section would result in the tongue not moving as far downward, leading to a weaker intraoral vacuum and correspondingly less effective sucking compared to infants delivered via vaginal delivery.
Additionally, experts believe that injuries from a Cesarean surgical procedure that cannot be distinguished by the naked eye may make the newborn fail in its attempt at positioning, attachment, and sucking (Smith, 2007). Among 12 pairs of cranial nerves, 6 participate in sucking and swallowing. The cranial nerves pass through the cranial pores. When the obstetric forceps or obstetrician’s hands assist the fetal head out of the uterine incision, the trigeminal or hypoglossal nerve may become constricted. Intubation and sucking amniotic fluid will stimulate the glossopharyngeal nerve and detrimentally affect the newborn’s ability to attach to the nipple. Central analgesics administered during a Cesarean delivery could also reduce the endogenous maternal endorphin level, thus decreasing the endogenous endorphin level the newborn gains through breast milk, aggravating the newborn’s pain, and disrupting the sucking behavior. In another study, Kron, Stein, and Goddard (1966) found that analgesics used during vaginal delivery were still having a detrimental effect on infants 4 days after birth, with infants showing uncoordinated tongue movements and weakened intraoral vacuums. The reduced effectiveness of the sucking led to a decreased volume of breast milk during lactation. Thus, both the Cesarean operation and anesthesia can adversely impair an infant’s tongue movement, providing further explanation for the weakened intraoral vacuum we found in the Cesarean group.
Relationship Between Strength of Intraoral Vacuum and Onset of Lactation
Our findings show that the strength of the intraoral vacuum within the first 24 hr after birth was strongly correlated with onset of lactation. Previous researchers have reported many factors to be predictors of the onset of lactation, including frequency of breast-feeding within the first 24 hr after birth (Nommsen-Rivers, Chantry, Peerson, Cohen, & Dewey, 2010), formula intake within 48 hr of birth (Hruschka et al., 2003), maternal age (Nommsen-Rivers, Dolan, & Huang, 2012), parity (Nommsen-Rivers et al., 2012), and maternal BMI (Dewey et al., 2003; Nommsen-Rivers et al., 2012). However, few of them have discussed the relationship between the strength of infant sucking and the onset of lactation. Goyal, Banginwar, Ziyo, and Toweir (2011) pointed out that correct positioning, attachment, and sucking are necessary components for the onset of lactation, as they guaranteed an airtight cavity and maximum possible negative pressure. Other authors have confirmed that sucking stimulus within the first day after birth is especially important for the onset of lactation (Edmond et al., 2006; Renfrew, Lang, & Woolridge, 2000). These findings are consistent with our finding in the present study that early sucking strength was related to the onset of lactation.
Based on studies showing that the early sucking of infants born via Cesarean section failed to promote breast-feeding (Gouchon et al., 2010; Nolan & Lawrence, 2009), we propose that interventions to address the weaker sucking strength of the Cesarean newborn might improve breast-feeding outcomes. Interestingly, Chapman, Young, Ferris, and Perez-Escamilla (2001) applied a breast pump set at 100 mmHg sucking pressure to puerperae within the first 3 days after Cesarean delivery to promote the onset of lactation, but milk transfer to the newborn did not show a significant improvement compared to mothers who did not use a breast pump. However, 100 mmHg is approximately equivalent to the strength of the intraoral vacuum we measured in the infants born via Cesarean in the present study (peak intraoral vacuum of 13.78 kPa = 103.35 mmHg). We thus speculate that the relatively weak vacuum of the breast pump, as compared to the peak intraoral vacuum of 19.89 kPa (149.18 mmHg) of the infants born via vaginal delivery, created an insufficient stimulus to improve breast-feeding outcomes in the Cesarean population.
Formula Feeding Was Negatively Related to the Strength of Intraoral Vacuum
We found that the frequency and volume of formula intake were negatively related to the strength of the intraoral vacuum. Previous studies have explored the relationship between formula intake and breast-feeding outcomes. Flaherman et al. (2013) verified the effectiveness of early limited formula use on improving the duration and exclusivity of breast-feeding. Geddes et al. (2012) found that the baseline and peak intraoral vacuum infants applied to the breast were significantly stronger than the vacuum they applied to the pacifier and that the nipple expanded more in response to sucking than did the pacifier. These findings imply that infants’ sucking behavior may be changed when they are given a pacifier.
Other Factors
Dyads in the Cesarean group experienced a postponed first breast-feeding compared to those in the vaginal birth group. However, time to first breast-feeding did not influence the strength of intraoral vacuum after controlling for other confounders. In the present study, gestational BMI gain was related to baseline intraoral vacuum. Further study is needed to determine the mechanism for this relationship.
Strength of Intraoral Vacuum in the Literature
In the present study, the peak intraoral vacuum for newborns delivered via vaginal birth was −19.89 ± 7.69 kPa (−149.18 ± 57.67 mmHg) within 24 hr after delivery. In previous studies, Geddes et al. (2008) reported a peak intraoral vacuum of −145 ± 58 mmHg and Prieto et al. (1996) a strength of −197 ± 10 mmHg. The infants in Geddes et al.’s study were aged 3–24 weeks, and investigators used a 650-mm-long sucking tube with an outside diameter of 4 mm to measure the strength of the intraoral vacuum. Prieto et al. studied 7-month-old infants using a 1,000-mm-long tube with an outside diameter of 2.4 mm. By contrast, the infants in the present study were less than 1 day old, and we used a 450-mm-long tube with an outside diameter of 2.7 mm to measure the strength of the intraoral vacuum. These differences were likely responsible for the differences in the findings.
Implications for Nursing Practice
Our findings in the present study that birth by Cesarean section weakened the intraoral vacuum and that the strength of the intraoral vacuum was related to the onset of lactation expand our existing knowledge about the causes of delayed onset of lactation. These results provide evidence of the physiological mechanisms that contribute to the delayed onset of lactation among mother–infant dyads who experience Cesarean birth in addition to the emotional and sociopsychological mechanisms favored by current thinking.
Our findings imply that, in addition to providing emotional and social support, nurses could provide interventions targeting the weakened intraoral vacuum of newborns delivered via Cesarean section in order to facilitate the successful onset of lactation and start of breast-feeding. Not only could caregivers provide professional support regarding breast-feeding protocols for first-time mothers in terms of correct positioning and attachment for breast-feeding, but for newborns with a weak intraoral vacuum they could consider providing additional stimulus as a supplement, such as an electric breast pump. The negative pressure of the pump, however, should be set within the normal range of the peak intraoral vacuum of healthy newborns born via uncomplicated vaginal delivery.
Limitations
Due to ethical concerns and maternal attitudes, we monitored only 30 s of a breast-feeding session rather than the entire session, which may have affected the results. In addition, some of the infants in the present study received a large amount of formula via bottle. As frequency and amount of formula feeding was a confounder for the strength of the intraoral vacuum and the onset of lactation, our results may differ from results among a sample in which no formula was used. Additionally, we did not measure the strength of the intraoral vacuum over the longer term in the present study and, consequently, cannot draw any conclusions about the long-term effects of type of birth on the strength of the intraoral vacuum.
Footnotes
Acknowledgements
We would like to thank the English teachers Richard Riggio and Zhengzheng Dai for their language assistance and professor Yan Ding for her technological support.
Author's Contribution
Feng Zhang contributed to conception, design, acquisition, analysis, and interpretation; drafted and critically revised the manuscript; gave final approval; and agreed to be accountable for all aspects of work ensuring integrity and accuracy. Haiou Xia contributed to conception, design, acquisition, and interpretation; drafted and critically revised the manuscript; gave final approval; and agreed to be accountable for all aspects of work ensuring integrity and accuracy. Xia Li contributed to conception, design, and interpretation; drafted and critically revised the manuscript; gave final approval; and agreed to be accountable for all aspects of work ensuring integrity and accuracy. Ling Qin contributed to design and interpretation, drafted and critically revised the manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy. Hongmei Gu contributed to design and interpretation, drafted and critically revised the manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy. Xujuan Xu contributed to conception and interpretation, drafted and critically revised manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy. Meiyun Shen contributed to conception and interpretation, drafted and critically revised the manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Funding of Nursing Scientific Research at Fudan University (Program no. FNF201422).