
Abstract
Background:
Atypical antipsychotic medications increase the risk of developing metabolic syndrome (MetS) and cardiovascular diseases in people with schizophrenia.
Aim:
To explore the prevalence of MetS and the predictors associated with the number of MetS components in people with chronic schizophrenia.
Methods:
We recruited 357 participants from 10 rehabilitation wards in northern Taiwan. The Beck Anxiety Inventory, Beck Depression Inventory-II, Health-Promoting Lifestyle Profile (HPLP), and modified Baecke physical activity questionnaire were used to evaluate the participants. MetS prevalence was calculated using the modified Adult Treatment Panel III criteria for Asians.
Results:
The prevalence of MetS in this sample was 37.8%. Multinomial logistic regression revealed that the HPLP-exercise score (odds ratio [OR] = 0.411, p = .002) and depressive symptoms (OR = 0.949, p = .040) were protective factors for ≥4 MetS components. The leisure physical activity level (OR = .536, p = .024) was a protective factor for three MetS components. Body mass index ≥24 kg/m2 was the strongest risk factor for two MetS components (OR = 8.057, p < .001), three MetS components (OR = 11.287, p < .001), and ≥four MetS components (OR = 15.621, p < .001). Additionally, participants’ age >40 (OR = 3.638, p = .012) was a risk factor for ≥four MetS components.
Conclusion:
In this study, the prevalence of MetS was higher than that reported for patients utilizing community-based services in Taiwan. The important risk factors for MetS were being overweight and older than 40. The protective factors for MetS were a high HPLP-exercise score and leisure-based physical activities.
Second-generation antipsychotic drugs increase the risks of developing metabolic syndrome (MetS) and cardiovascular diseases. Previous studies have shown that treatment with antipsychotic drugs is correlated with weight gain (Newcomer & Haupt, 2006), dyslipidemia, and diabetes (Henderson et al., 2005) and that the incidence of sudden cardiac death is nearly 2 times greater for patients who take antipsychotic drugs than for individuals who do not (Ray, Chung, Murray, Hall, & Stein, 2009).
The prevalence of MetS in the general population in Taiwan is 15.7% (Hwang, Bai, & Chen, 2006). This figure increases to 34.9% for people with schizophrenia spectrum disorder who live in community-based rehabilitation facilities (Huang et al., 2009). Researchers have reported the prevalence of MetS in people with schizophrenia to be 2–3 times higher than it is in the general population (De Hert, Schreurs, Vancampfort, & van Winkel, 2009).
In Taiwan, studies of MetS in people with schizophrenia spectrum disorders (Huang et al., 2009) have primarily investigated individuals who live in communities rather than those who are hospitalized with the disorder. However, compared to individuals living in communities, hospitalized patients may exhibit greater symptom severity and may be administered a higher drug dose, which increases their risks of developing heart disease and MetS (Ray et al., 2009). Moreover, patients in acute wards can be examined during routine check-ups performed in the hospital, whereas patients in chronic and rehabilitation wards are frequently neglected. Thus, these hospitalized patients with schizophrenia warrant further attention.
Previous studies have verified that the use of atypical psychotropic medication increases the risk of developing MetS (Bai et al., 2009; De Hert et al., 2008). However, psychiatrists still use atypical psychotropics because these medications can improve both the positive and the negative symptoms of people with schizophrenia (Burton, 2006). In addition, atypical psychotropic drugs can increase patient compliance (Cortesi et al., 2013) and enhance their quality of life (Chue, 2006). Thus, psychiatric professionals must monitor patients with chronic schizophrenia for MetS.
The risk factors for MetS generally include unhealthy dietary behaviors, lack of exercise, and smoking. The likelihood that people with schizophrenia will follow a healthy lifestyle (e.g., no smoking, regular exercise, and a healthy diet) is substantially lower than it is for the general population (Levander, Eberhard, & Lindström, 2007; Roick et al., 2007; Vancampfort, Probst, et al., 2011). Furthermore, among people with schizophrenia, the number of cigarettes those who have MetS smoke is markedly higher compared to those who do not have this syndrome (Vancampfort, Probst, et al., 2011). Since the Tobacco Hazards Prevention Act, which prohibits people from smoking in hospital spaces, was implemented several years ago in Taiwan, the risk factor of smoking has been effectively reduced for patients treated in chronic rehabilitation wards. In addition, because these patients consume their meals in the hospital, problems concerning the intake of fatty foods are effectively controlled. Therefore, the prevalence of and risk factors for MetS in people with chronic schizophrenia who live in rehabilitation facilities, where diet and smoking are controlled, is a topic that warrants further investigation. The purpose of the present study was to explore the prevalence of MetS and the predictors associated with the number of MetS components in people with chronic schizophrenia who live in rehabilitation wards.
Methods
Participant recruitment
We recruited participants from 10 inpatient psychiatric rehabilitation units in New Taipei City, Taiwan, from April 2013 to April 2014. The inclusion criteria included a Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV), diagnosis of schizophrenia and an age of between 20 and 65 years, hospitalization in a rehabilitation unit, and a stable condition at the time of data collection. Participants were able to provide written informed consent and comprehend the instruments. We excluded patients who had an intellectual disturbance or substance abuse issues, as determined by chart review.
Instruments
The dependent variable for this study was the presence or absence of three or more criteria for MetS. We employed the modified Third Report of the National Cholesterol Education Program’s Adult Treatment Panel III criteria, with waist circumference (WC) for Asians, to diagnose MetS in the adult population (Tan, Ma, Wai, Chew, & Tai, 2004). We classified participants meeting three or more of the following five widely used criteria as having MetS: (a) WC: male ≥90 cm, female ≥80 cm; (b) systolic blood pressure (SBP) ≥ 130 mmHg and/or diastolic blood pressure (DBP) ≥85 mmHg or current treatment for hypertension; (c) high-density lipoprotein (HDL) cholesterol: male <40 mg/dl, female <50 mg/dl, or known treatment for low HDL cholesterol; (d) fasting serum glucose levels ≥100 mg/dl or known treatment for diabetes; and (e) triglyceride (TG) level ≥150 mg/dl or known treatment for high TGs. Predictor variables included information about demographics, health-promoting lifestyles, physical activity, depression, and anxiety.
Demographic data, disease, and treatment information
We collected data on demographic, disease, and treatment variables for all participants, including age, sex, body mass index (BMI), education, marital status, disease duration, pharmacotherapy (antipsychotics, lipid-lowering drugs, antidiabetic drugs, and antihypertensive drugs), anxiolytic drugs, hypnotics, and chlorpromazine at 100-mg equivalent doses (Gardner, Murphy, O’Donnell, Centorrino, & Baldessarini, 2010).
Health-Promoting Lifestyle Profile questionnaire
We employed the Chinese version of Walker’s Health-Promoting Lifestyle Profile (HPLP) questionnaire (Walker, Sechrist, & Pender, 1987), which had been translated from the original English by M. Y. Chen et al. (1997). The HPLP includes 40 items related to nutrition, health responsibility, spiritual growth, interpersonal support, exercise, and stress management. It uses a 4-point Likert-type response format to obtain data regarding frequency of reported behaviors, with responses ranging from 0 (never) to 3 (always). A higher score on the instrument indicates a higher level of health-promoting behaviors. M. Y. Chen et al. (1997) found good internal consistency reliability for the Chinese version of the questionnaire (Cronbach’s α > .80). In the present study, the Cronbach’s α coefficient of the chronic schizophrenia sample was .959.
Physical activity
The physical activity assessment included two parts: a 6-min walking test (6MWT) and the Baecke habitual physical activity questionnaire (Baecke, Burema, & Frijters, 1982). The questionnaire consists of a scale with one section each on work (8 items), leisure (4 items), and sports activities (4 items). Belgian researchers have employed this scale to measure the physical activity of people with schizophrenia (Vancampfort, Sweers, et al., 2011). Ho, Yu, and Chan (2015) subsequently translated it into Chinese, producing the modified Chinese Baecke questionnaire. This questionnaire uses self-report to assess physical activity over the 12 months. The Chinese version of the questionnaire consists of the following 4 indices: work, sports, leisure time, and housework. Because the research participants in the current study were patients who lived in rehabilitation facilities and did not perform housework, we excluded the housework index. Questions in each index are scored on a 5-point Likert-type scale, ranging from never to always. Higher scores indicate higher levels of physical activity. In the present study, the Cronbach’s α coefficient of the chronic schizophrenia sample was .875.
Depressive symptoms
We assessed depressive symptoms with the Beck Depression Inventory, 2nd edition (BDI-II; Beck, Steer, & Brown, 1996). The BDI-II includes 21 items that ask respondents to assess their condition over the previous 2 weeks. Each item is scored as follows: 0 = symptom absent, 1 = symptom present, 2 = moderate symptom, or 3 = severe symptom. Total score ranges from 0 to 63. Respondents are classified into one of the following four categories according to the total score: minimal depression (0–13), mild depression (14–19), moderate depression (20–28), and severe depression (29–63). Beck, Steer, and Brown (1996) used the Hamilton Rating Scale for Depression to evaluate criterion validity, which reached .71. Chemerinski, Bowie, Anderson, and Harvey (2008) examined the dimensional structure of the BDI-II in a large sample of elderly medicated schizophrenia outpatients. Lu, Che, Chang, and Shen (2002) assessed the reliability and validity of the Chinese version of the BDI-II in Taiwan. The cutoff scores for patients with mild, moderate, and severe depression were 16 of 17, 22 of 23, and 30 of 31, respectively. This scale demonstrated good internal consistency (Cronbach’s α) of .94 and a split-half reliability of .91. Further, Dutch (van Oosterhout, Krabbendam, Smeets, & van der Gaag, 2013) and Taiwanese (Yang, Lee, Lo, & Beckstead, 2015) research teams employed this instrument to measure depressive symptoms in people with schizophrenia. In the present study, the Cronbach’s α coefficient of the chronic schizophrenia sample was .908.
Anxiety symptoms
We assessed the subjective severity of participants’ anxiety with the Beck Anxiety Inventory (BAI; Beck, Epstein, Brown, & Steer, 1988). Beck et al. developed this 21-item inventory using the DSM (Third Edition) or DSM (Third Edition Revised) diagnostic standards. Each item has four possible responses ranging from 0 (not at all) to 3 (severely). Total score ranges from 0 to 63, with respondents classified into one of the following four categories according to this score: minimal anxiety (0–7), mild anxiety (8–15), moderate anxiety (16–25), and severe anxiety (26–63). The BAI is widely employed for clinical assessment and research of acute (W. C. Chen et al., 2009) and chronic schizophrenia (Yang et al., 2015). Che, Lu, Chen, Chang, and Lee (2006) tested the reliability and validity of the Chinese version of the BAI in Taiwan and found that the optimal cutoff point for discriminating between anxious and nonanxious patients was 13 of 14. The criterion validity of the Chinese BAI was tested using the Hamilton Anxiety Rating Scale (HAM-A) and reached .72 (Che et al., 2006). This scale demonstrated good internal consistency (Cronbach’s α) of .95 and a split-half reliability of .91. Further, Dutch researchers employed this instrument to measure anxiety symptoms in people with schizophrenia (van Oosterhout et al., 2013). In the present study, the Cronbach’s α of the chronic schizophrenia sample was .946.
Procedure
The Joint Institutional Review Board (12-S-019) and Bali Psychiatric Center, Ministry of Health and Welfare (IRB1020206-01) approved the study procedures. We invited all of the people with schizophrenia in the 10 rehabilitation units from which we recruited to participate in this study. A total of 383 patients were initially recruited to participate. After we provided an explanation of the research procedure, 93.21% of those patients agreed to participate and signed their own consent forms, for a total of 357 participants. After they provided informed consent, we asked study participants to provide demographic data and complete a structured questionnaire, which included the HPLP, Baecke questionnaire, BDI-II, and BAI and took about 30 min to complete.
We evaluated the 6MWT according to the American Thoracic Society (2002) guidelines. We performed the test in an indoor corridor of the rehabilitation units and attempted to minimize external stimuli. Two cones placed 25-m apart indicated the length of the walkway. We instructed participants to walk back and forth around the cones for 6 min, without running or jogging. Resting was allowed if necessary, but participants were to resume walking as soon as they were able to do so.
We obtained the fasting blood sugar, TG, and HDL levels; WC; BP; body height; and body weight of the participants from their medical records. For patients whose medical records did not contain their fasting blood sugar, TG, or HDL level from the previous 3 months, we administered blood tests to acquire these data.
Data Analysis
We analyzed the data using IBM SPSS for Windows (version 20.0) and performed descriptive statistical analyses of the participants’ demographic data. We used independent t-tests and χ2 tests to examine the relationships between MetS and demographic data, health promotion lifestyle, physical activity, and depressive and anxiety symptoms. Candidate predictors for inclusion in the simple logistic regression were selected from the significant results of the t-test or χ2 tests. The multinomial logistic regression model revealed significant predictors of the number of MetS components. Based on the finding of a significant bivariate association with MetS, we selected the following six factors to enter into the model: BMI ≥24 kg/m2, age ≥ 40 years, HPLP-exercise subscale score, Baecke physical activity leisure subscale score, depressive symptoms, and anxiety symptoms. We considered p < .05 to be statistically significant.
Results
Demographic Characteristics and Medications
We recruited 357 participants for this study. Ages ranged from 23 to 65 years, with a mean age of 47.96 years (SD = 9.12). A total of 70 (19.6%) participants used both typical and atypical psychotropic medications, while 219 (61.3%) used only atypical psychotropic medication. Of the latter, 140 (39.2%) used clozapine and 79 (22.1%) used risperidone. Table 1 shows the demographic characteristics and types of medication used for the participants with and without MetS. BMI and age were the only demographic or medication-related variables that differed between groups, with participants with a BMI ≥24 kg/m2 and an age ≥40 years having a significantly higher prevalence of MetS.
Comparison of Demographic Characteristics and Medications Prescribed in Patients With and Without Metabolic Syndrome (MetS).
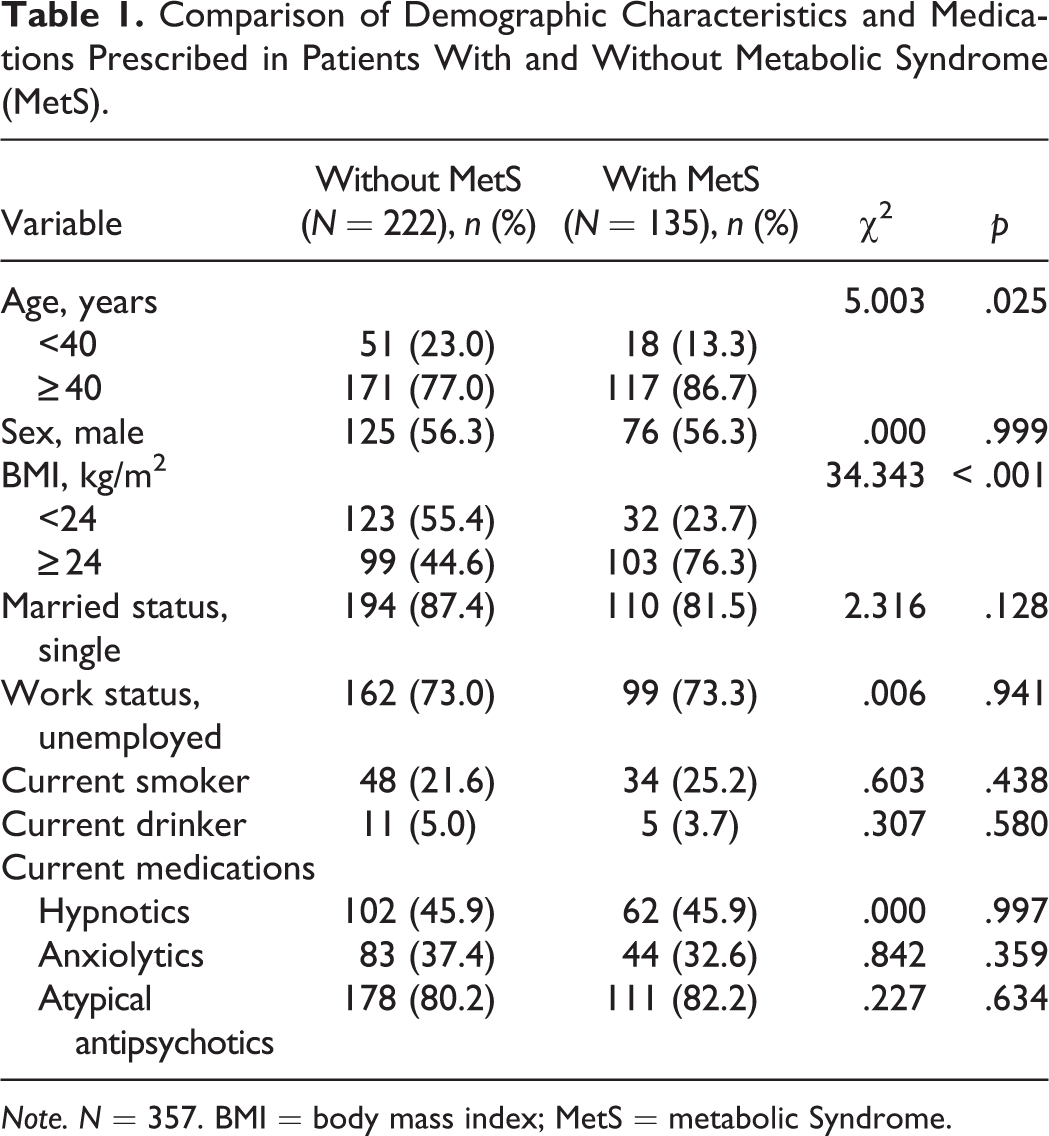
Note. N = 357. BMI = body mass index; MetS = metabolic Syndrome.
Prevalence of Abnormal Metabolic Parameters and MetS
The numbers of participants with abnormalities in the five metabolic parameters we assessed were as follows: (a) elevated fasting plasma glucose (including a blood sugar level ≥100 mg/dl or the use of hypoglycemic agents), n = 101 (28.3%); (b) hypertriglyceridemia (including a TG level ≥150 mg/dl or the use of antilipemic agents), n = 120 (33.6%); (c) low HDL cholesterol (including an HDL <40 mg/dl for men, an HDL <50 mg/dl for women, or the use of lipid drugs), n = 170 (47.6%); (d) elevated BP (SBP ≥130 mmHg, DBP ≥85 mmHg, or the use of antihypertensive drugs), n = 144 (40.3%); and (e) central obesity (WC ≥90 cm for men and ≥80 cm for women), n = 222 (62.2%). The number of participants with abnormal values for three or more of the five parameters and, therefore, identified as having MetS was 135 (37.8%). The numbers of participants with abnormal values for one to five of the parameters were as follows: one component, n = 75 (21%); two, n = 96 (26.9%); three, n = 69 (19.3%); four, n = 47 (13.2%); and five, n = 19 (5.3%).
Associations of MetS With Demographic Characteristics, Physical Activity, Symptoms of Depression and Anxiety, and Health-Promoting Lifestyle
As shown in Tables 1 and 2, the following variables were related to MetS: age (χ2 = 5.003, p = .025), BMI (χ2 = 34.343, p < .001), HPLP-exercise subscale (t = 3.278, p = .001), depressive symptoms (BDI score; t = 2.800, p = .005), anxiety symptoms (BAI score; t = 2.664, p = .008), and Baecke habitual physical activity questionnaire leisure index (t = 2.343, p = .020).
Associations of Demographic Characteristics and Key Variables With Metabolic Syndrome (MetS).
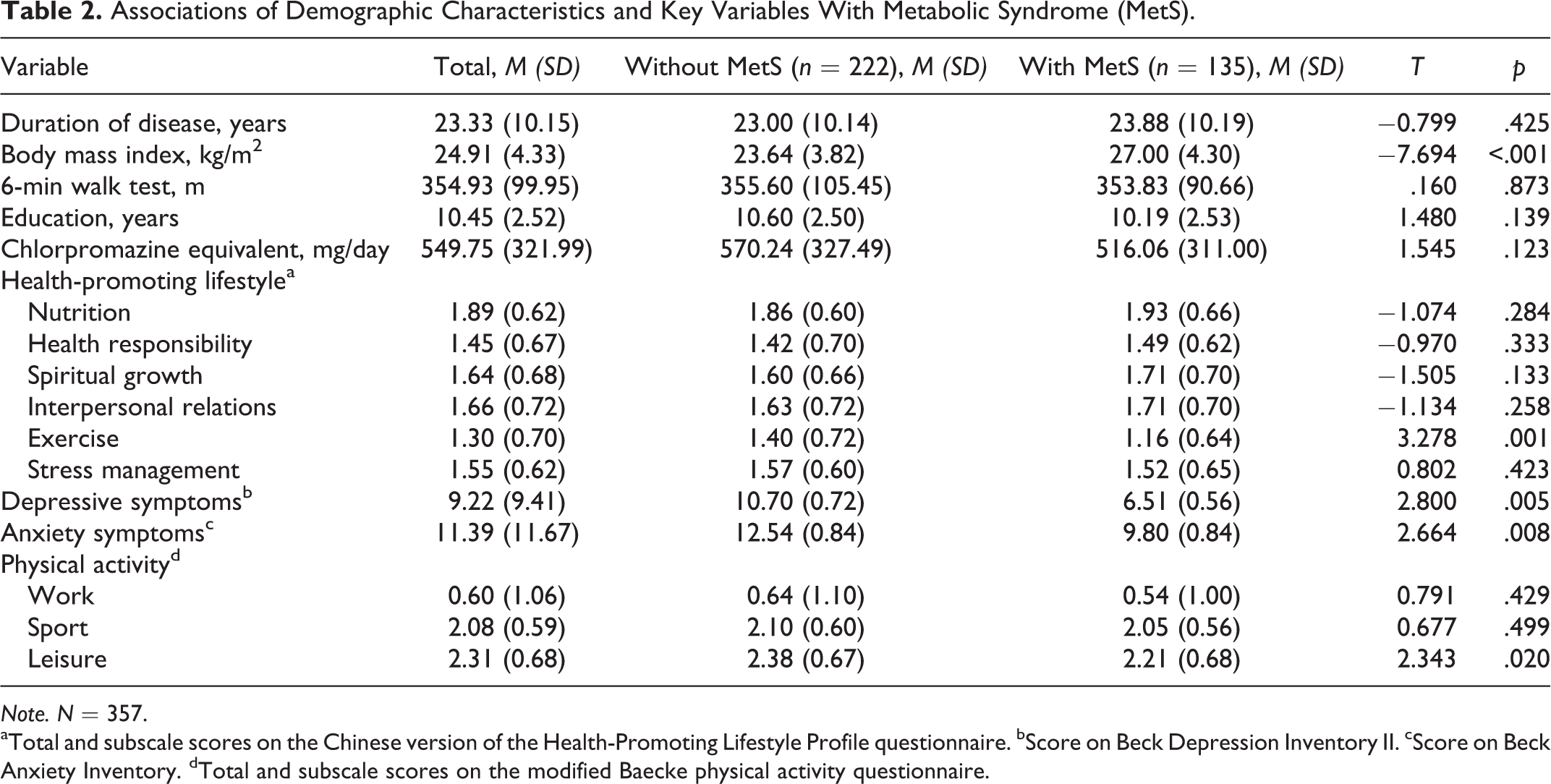
Note. N = 357.
aTotal and subscale scores on the Chinese version of the Health-Promoting Lifestyle Profile questionnaire. bScore on Beck Depression Inventory II. cScore on Beck Anxiety Inventory. dTotal and subscale scores on the modified Baecke physical activity questionnaire.
Predictors of MetS
Table 3 shows the simple logistic regression analysis results assessing the effects of individual predictors on MetS. The results indicate that a BMI ≥24 kg/m2 and an age of over 40 years were risk factors for MetS. By contrast, higher scores on the leisure-based physical activity subscale of the Baecke inventory and the HPLP exercise subscale were protective factors for MetS. In addition, higher scores for depressive and anxiety symptoms were associated with lower risk of MetS.
Simple Logistic Regression for Individual Predictors of Metabolic Syndrome in Patients With Chronic Schizophrenia.
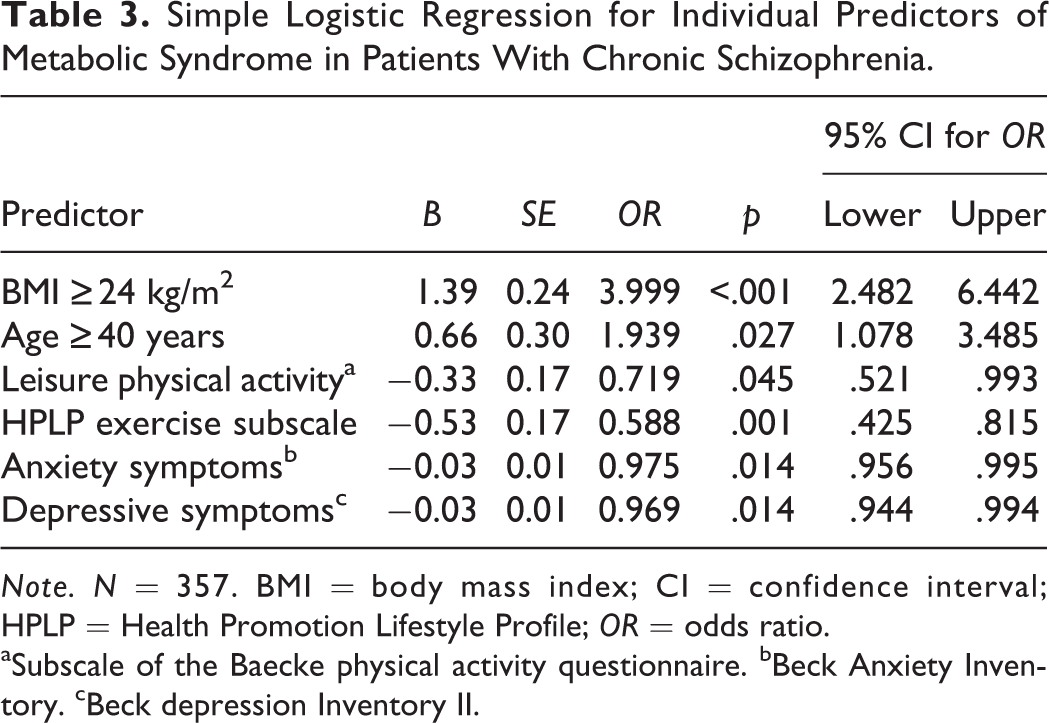
Note. N = 357. BMI = body mass index; CI = confidence interval; HPLP = Health Promotion Lifestyle Profile; OR = odds ratio.
aSubscale of the Baecke physical activity questionnaire. bBeck Anxiety Inventory. cBeck depression Inventory II.
For our multinomial logistic regression analysis, we used the classification method that Sekita et al. (2013) introduced, grouping participants with zero or one MetS component (i.e., abnormal metabolic parameter) into one group (126 participants, 35.3%) and those with four or five MetS components into another group (66 participants, 18.5%). We established the group of participants with zero or one MetS component as the reference group and compared it with participants with two, three, and four or five MetS components to facilitate prediction analysis.
Multinomial logistic regression analysis (Table 4) revealed that BMI ≥24 kg/m2 significantly increased the odds ratio (OR) for all participants with more than one MetS component, indicating that BMI ≥24 kg/m2 was a risk factor for MetS. Thus, for example, the risk of developing MetS increased by 8.057 even for participants exhibiting only two MetS components. For the predictor age ≥40 years, we observed no significant increase in the OR for participants with ≤3 MetS components; however, we did detect a significant increase in OR for those with four or five components such that the risk of developing MetS for participants aged 40 years or older was 3.638 times the risk for those younger than 40. Thus, we identified an age ≥40 years as a risk factor for MetS. For leisure-based physical activity, we observed a significant OR for the participants exhibiting three MetS components when compared to the reference group such that an increase of 1 point in leisure-based physical activity would reduce the probability of developing MetS by 46.4%, indicating that leisure-based physical activity was protective for MetS. We observed no significant effects of leisure-based physical activity on reducing the risk of MetS for participants with ≥four abnormal MetS components. We further found that a higher score on the HPLP exercise subscale score was a protective factor for MetS for those with ≥4 MetS components such that a 1-point increase in the HPLP-exercise subscale score decreased the probability of developing MetS by 58.9%. We also observed a significant change in the OR associated with depressive symptoms for participants with ≥four MetS components. For participants in this group, a 1-point increase in depressive symptoms reduced the probability of developing MetS by 5.1%. In these analyses, anxiety symptoms had no significant effect on the OR for any of the groups.
Multinomial Logistic Regression of the Association of Predictors With the Number of Metabolic Syndrome (MetS) Components in Patients With Chronic Schizophrenia.
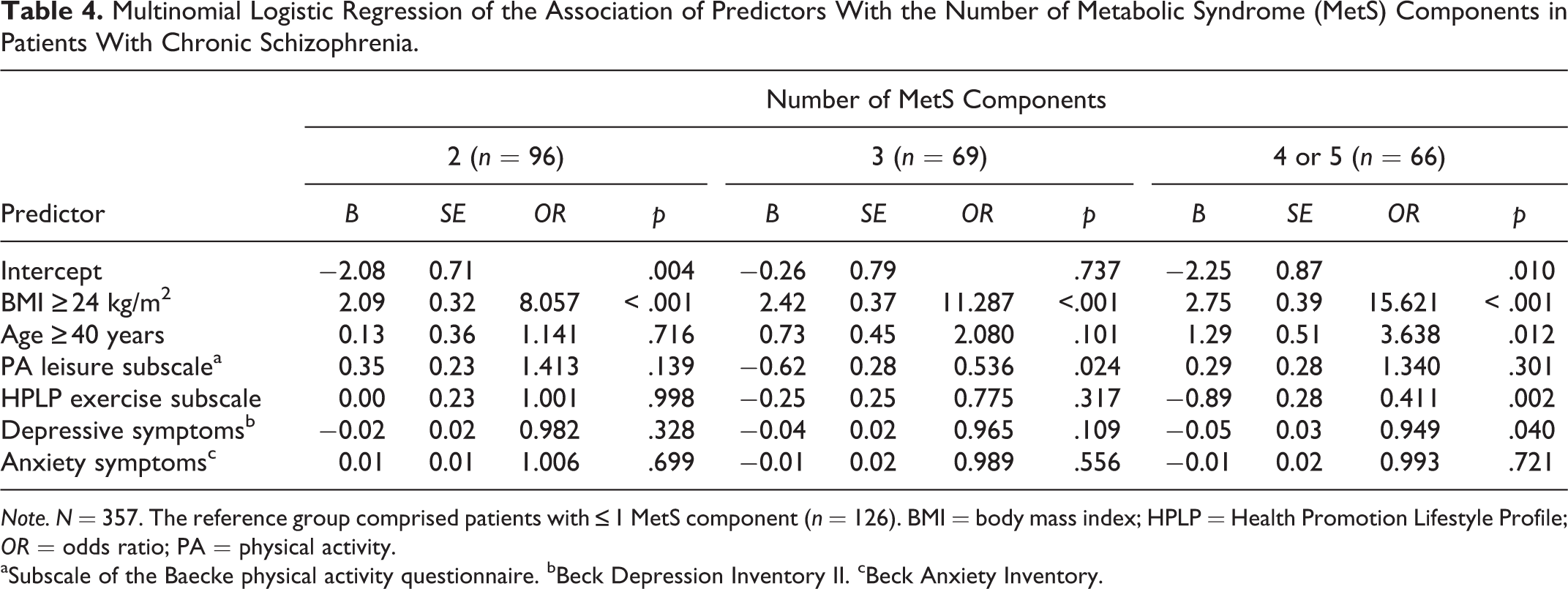
Note. N = 357. The reference group comprised patients with ≤1 MetS component (n = 126). BMI = body mass index; HPLP = Health Promotion Lifestyle Profile; OR = odds ratio; PA = physical activity.
aSubscale of the Baecke physical activity questionnaire. bBeck Depression Inventory II. cBeck Anxiety Inventory.
Discussion
In the present study, 37.8% of participants with schizophrenia being treated in inpatient psychiatric wards had MetS, a higher rate than the 15.7% researchers have reported for the general population (Hwang et al., 2006), and the 34.9% researchers have reported for people with schizophrenia who live in community-based rehabilitation facilities (Huang et al., 2009). In contrast with community-based rehabilitation facilities, inpatient rehabilitation facilities promote healthy dietary habits because the daily diets of patients are managed by nutritionists and supervised by nursing personnel. In addition, these facilities provide space for patients to engage in physical activities. Contrary to expectations, however, the higher prevalence of MetS among the patients living in the inpatient rehabilitation facilities demonstrates the severity of the problems associated with these patients.
Among our participants, 62.2% had a WC exceeding the normal range. In a previous study, Yazici et al. (2011) found that a greater percentage of patients with schizophrenia had an abnormal WC than any of the other four MetS components. These findings indicate the importance of obesity as a potential risk factor for MetS among patients treated in the facilities we examined in the current study. Staff in these facilities did encourage walking for exercise; however, this leisure-based physical activity is less demanding than the activities that Belgian medical facilities recommend for people with schizophrenia (Vancampfort, Sweers, et al., 2011). In addition, the duration of 6 min for the walking test in the present study was shorter than that in these Belgian studies. An investigation of the physical activity of people with schizophrenia spectrum disorder conducted in the United States showed that the amount patients with schizophrenia walked (measured via the number of steps taken per day) tended to be inversely related to body fat ratio and BMI (Beebe & Harris, 2013). This factor may have contributed to the rate of obesity we observed in the present study.
According to the recommendations from Gozdzik-Zelazny, Borecki, and Pokorski (2011), BDI-II scores ≥12 indicate depression in people with schizophrenia. In the present study, 122 patients (34.2% of participants) had BDI scores
Our study participants who did not have MetS exhibited significantly more symptoms of anxiety compared to those who had MetS. A French study of the relationship between symptoms of depression and anxiety and MetS in the general population showed that MetS was significantly related to depressive symptoms but not to symptoms of anxiety (Skilton, Moulin, Terra, & Bonnet, 2007). Using the HAM-A, Maslov et al. (2009) found no correlation between symptoms of anxiety and the prevalence of MetS for people with schizophrenia in Croatia. However, they did find a correlation between symptoms of anxiety and the prevalence of MetS for the general population such that severe symptoms of anxiety lead to an increased risk of developing MetS. In the present study, the BAI score was significantly lower in participants with MetS compared to those without. The difference between ours and previous findings may be due to the fact that 62.9% of people with schizophrenia in Taiwan use benzodiazepine (Wu, Lin, & Liu, 2011) to improve their sleep quality and symptoms of anxiety. Moreover, 54.62% of the participants in the present study used sleeping pills and anxiolytics, suggesting that the symptoms of anxiety we measured in this study were influenced by medication and were therefore not reflective of the patients’ true state.
Regarding leisure-based physical activity, participants who did not have MetS engaged in more of these activities than those who had MetS, which is consistent with the findings of prior studies conducted in Belgium (Vancampfort, Sweers, et al., 2011). Although participating in leisure-based physical activities is crucial for people with chronic schizophrenia, they may stop engaging in these activities because of psychiatric symptoms, weight gain, stigma, or fear of danger (McDevitt, Snyder, Miller, & Wilbur, 2006). Some studies have shown that participation in sports and leisure-based physical activity is significantly lower among patients with schizophrenia who have MetS compared to those who do not (Vancampfort, Sweers, et al., 2011). However, in this study, we observed no difference in terms of sports-based physical activity perhaps because the inpatient rehabilitation wards in which participants were living had limited space and the 6MWT that we used was less useful for revealing such a difference than the test that (Vancampfort, Sweers, et al., 2011; Beebe et al., 2005) proposed that schizophrenia patients would achieve activity-related health improvements if they were encouraged to participate in physical exercises, and our findings support this proposal.
Although risk factors for MetS among patients with schizophrenia include lack of physical activity, age, sex, the number of years with the disease, and atypical psychotropic medication use (Mitchell et al., 2013; Vancampfort, Sweers, et al., 2011; Yazici et al., 2011), our analysis in the current study revealed no differences in the duration of disease or atypical psychotropic medication use between patients with and without MetS. This lack of differences between the groups may be due to the fact that 80% of the participants used atypical psychotropic medication and participants in both groups had been diagnosed with schizophrenia more than 20 years prior. In addition, the risk of developing MetS increases for individuals with schizophrenia who are overweight and older than 40 (Huang et al., 2009). In the present study, as the number of MetS components increased in participants with a BMI
These findings highlight the increased physical health risks that patients with schizophrenia face as they age and as their BMIs increase. The current practices for monitoring the physical health conditions of people with schizophrenia do not follow the recommendations of professional organizations such as the American Diabetes Association and the American Psychiatric Association. De Hert, van Winkel, Silic, Van Eyck, and Peuskens (2010) recommended that patients aged 40 years and older who are taking antipsychotic medications should receive blood tests every 3 months during the first year of treatment followed by annual blood tests.
Our findings in the present study showed that leisure-based physical activity is a protective factor for MetS. Thus, an increase in leisure-based physical activity reduces the probability of developing MetS. However, the level of leisure-based physical activity had no effect on reducing the risk of MetS for the patients with ≥ four MetS components. These patients must follow regular exercise plans in order to reduce the risk of developing MetS.
Sumamo, Ha, Korownyk, Vandermeer, and Dryden (2011) suggested that exercise and dietary-intake interventions could decrease the risk of developing MetS components. We did not address dietary intake as a risk factor for MetS in the present study.
Limitations
The present study had a number of limitations. First, because it had a cross-sectional design, we were not able to evaluate the chronological factors of developing MetS. Second, we could not ensure that the participants accurately completed the instruments. Evaluation of the participants’ physical activities was based on their subjective descriptions without the support of objective assessments. Researchers in subsequent studies should include objective assessment tools and follow-up studies and use a longitudinal design to assess the risk of developing MetS over time and consider the consequences when patient conditions change. Although we found scores on the HPLP exercise subscale to be one of the critical factors influencing risk of MetS, we did not actually observe the participants as they participated in the exercises. In addition, the generalizability of our results to the inpatient rehabilitation population is limited because we used a convenience sample; further, the results cannot be directly extrapolated to settings outside of inpatient rehabilitation institutions.
Conclusions
In the present study, we determined that 37.8% of the participating inpatients with chronic schizophrenia had MetS. The predictors and risk factors for MetS were weight (i.e., overweight) and age (i.e., ≥40 years). The protective factors for MetS were exercise, as measured by the HPLP exercise subscale, and leisure-based physical activities, as measured by the Baecke habitual physical activity questionnaire. The results of this study should encourage psychiatric professionals to emphasize the importance of exercise and physical activity to patients with schizophrenia. These professionals should encourage patients in rehabilitation facilities to exercise regularly to reduce the risk of developing MetS.
Footnotes
Acknowledgments
We thank the patients who participated in this study and the three research assistants (J. C. Lee, C. Y. Lin, and C. P. Lin CP) who helped with the data collection.
Author Contribution
CY Yang contributed to conception and design; acquisition, analysis, and interpretation; drafted the manuscript; critically revised the manuscript; gave final approval; and agreed to be accountable for all aspects of work ensuring integrity and accuracy. SC Lo contributed to conception and acquisition, analysis, and interpretation; critically revised the manuscript; gave final approval; and agreed to be accountable for all aspects of work ensuring integrity and accuracy. YC Peng contributed to conception, acquisition, and interpretation; critically revised the manuscript; gave final approval; and agreed to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided, in part, by a grant from the National Science Council, Taiwan (NSC 101-2410-H-010-012).