
Abstract
Background:
Roux-en-Y gastric bypass (RYGB) is considered the gold standard for gastric bypass, displaying better results for metabolic disorders than other surgical procedures over the long term. The aim of this study was to determine the effects of bariatric surgery, in particular the RYGB technique, on metabolic syndrome (MS) and other biochemical parameters implicit in the comorbid conditions associated with obesity, as well as to explore the influence of this surgical procedure on psychiatric comorbidity in the study population.
Method:
An observational retrospective cohort study based on 146 clinical records of patients having undergone RYGB between January 1, 2011, and January 1, 2014, was performed. Data related to metabolic and psychiatric comorbidity were gathered at three stages: prior to surgery and at 3 and 9 months following surgery.
Results:
There was a progressive and statistically significant reduction of all biochemical parameters analyzed at 3 and 9 months following surgery except high-density lipoprotein cholesterol, which significantly increased (beneficial) in value. These changes imply a remission of >90% for all metabolic disorders and the consequent tendency toward a reduction in prescribed pharmacological treatments, with MS found in only one subject at 9 months. There was, however, no significant reduction in pharmacological treatments for psychiatric comorbidities.
Conclusion:
Findings suggest that RYGB is an effective treatment for MS and other metabolic disorders but not for psychiatric comorbidities accompanying MS.
Keywords
The inexorable global increase in obesity has become a worldwide concern of the highest magnitude (Nepal, Bhattarai, & Agustin, 2015; Ortiz, Vidal-Melo, & Walsh, 2014). Obesity produces cardiometabolic complications, known collectively as metabolic syndrome (MS; Lin, Liang, Liao, & Tsay, 2014). Despite the fact that obesity is one of the most highly researched of the nutritional disorders, the World Health Organization (WHO, 2012) reports that its prevalence doubled worldwide from 1998 to 2008, with recent European levels ranging between 6% and 20% (Rabin, Boehmer, & Brownson, 2007). The latest report on prevalence in Spain states that 17% of the population is obese (Instituto Nacional de Estadística, 2013). Narrowing the focus down to the Murcia region of Spain, the location of the present study, a recent population study revealed that more than one third of the study sample suffered from obesity; of these, researchers categorized 6.4% as morbidly obese (Fernández-Ruiz, Paniagua-Urbano, Sole-Agusti, Ruiz-Sanchez, & Gomez-Marin, 2014), a prevalence level similar to that found in the United States (Sturm & Hattori, 2013).
A range of metabolic disorders are associated with obesity, such as diabetes mellitus (DM), arterial hypertension (AHT), dyslipidemia (DLP), hyperuricemia, and nonalcoholic fatty liver disease (NAFLD; Boban et al., 2014; Mulero et al., 2012); the co-occurrence of several of these disorders denominates MS. The impact of MS in recent decades on morbidity, mortality, and health-care expenditures justifies identification of the syndrome as one of the 21st century’s epidemics (Nepal et al., 2015).
A number of studies have suggested an association between obesity and psychiatric comorbidity (Garimella, Sears, & Gehi, 2016; Gibson-Smith et al., 2016; Jokela et al., 2016) as well as other unhealthy lifestyles and behaviors (Strine et al., 2008). The prevalence of psychiatric comorbidities worldwide, in particular depression and anxiety, is high and manifests in the form of persistent disabling illnesses (Greenberg et al., 2003; Young, Klap, Shoai, & Wells, 2008). The economic cost of mental health disorders associated with obesity is also a significant concern (Rudisill, Charlton, Booth, & Gulliford, 2016).
Conservative therapies (diet, physical exercise, and cognitive–behavioral therapy) used to treat clinically severe obesity or obesity associated with comorbidity (MS) have proven insufficient over the medium term, with reports of only a 5% weight loss, and over the longer term results are even more discouraging (Nepal et al., 2015; Trueman et al., 2010). Bariatric surgery (BS) has emerged as a far-reaching therapeutic option with beneficial side effects beyond the mere loss of weight, including the remission of comorbid conditions (Mohos, Nagy, Schmaldienst, & Prager, 2011). Among the alternative forms of BS, the Roux-en-Y gastric bypass (RYGB) is considered the gold standard, displaying better results for metabolic disorders than other surgical procedures over the long term (Bays et al., 2009; Yang, Wang, & Yang, 2015). RYGB is a mixed BS technique that involves the creation of a 6-cm long gastric chamber with a volume of 5–50 ml either partitioned or completely isolated from the remaining stomach, typically via staples, with a 75- to 150-cm length of small intestine connected in a “Y” configuration to form an enteroenterostomy to the jejunum some 30–50 cm from the Treitz ligament (Raj, Kumaravel, Chandramaliteeswaran, Vaithiswaran, & Palanivelu, 2012).
The aim of the present study was to determine whether BS, in particular the RYGB technique, is effective in treating psychiatric comorbidity as well as MS (as defined using the international criteria established by the WHO; Alberti & Zimmet, 1998), and other biochemical parameters implicit in the comorbid conditions associated with obesity as well as on psychiatric comorbidity. The study population from Murcia (Spain) exhibits a prevalence of MS well above that reported for other regions of Spain, albeit one that is within the range reported for the rest of Europe (Fernández-Ruiz et al., 2014).
Method
Study Setting and Subjects
We performed a retrospective observational study at the endocrinology and nutrition unit of the Virgen de la Arrixaca Clinical University Hospital (HCUVA), which is the reference hospital for the Murcia region (Spain). We selected the study population from the database of patients registered in Area 1 of the public health system of Murcia who were over 18 years of age and had been treated via the RYGB surgical procedure between January 1, 2011, and January 1, 2014. Exclusion criteria were as follows: (1) medical records in which presurgical assessment or postsurgical follow-up of patients had been performed at health-care facilities other than the endocrinology and nutrition unit of the HCUVA and (2) those records that were missing study variables, either due to alterations in treatment or data collection prior to or following surgery or the death of a patient (Figure 1). The final sample included a total of 146 medical histories. Since all eligible subjects were included, we applied no sampling technique. One researcher gathered all the data.
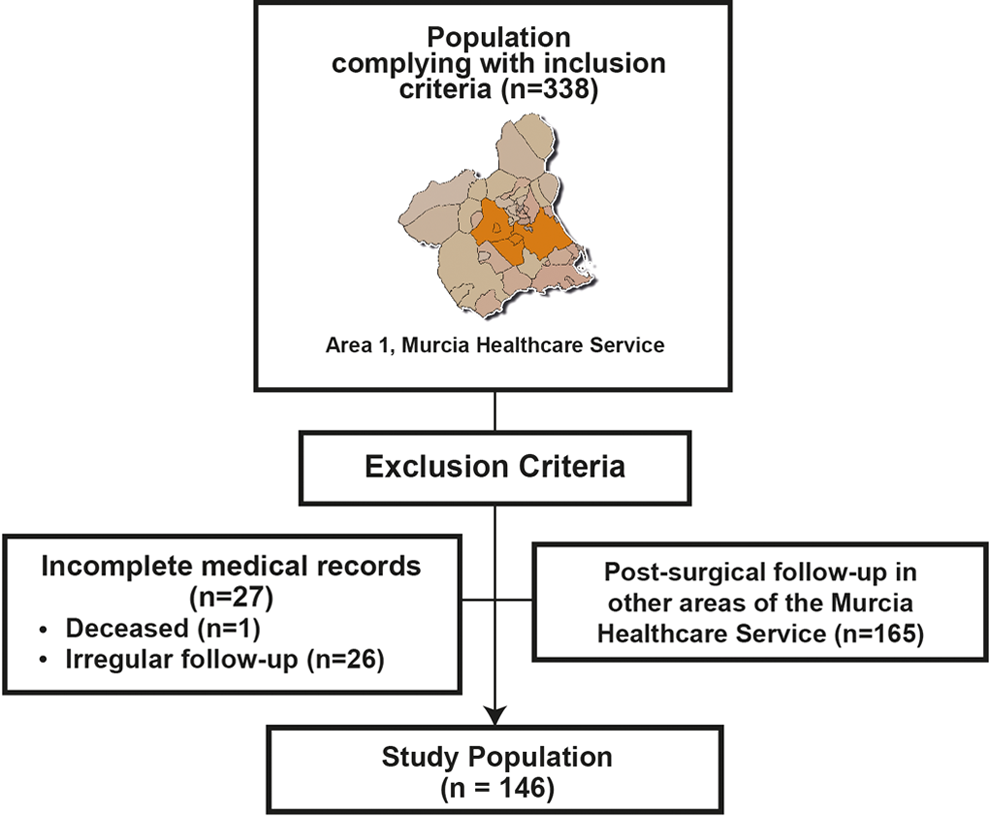
Subject selection process.
The same surgical team operated on 338 patients during the data collection period (Figure 1). Of these, we excluded 165 from the study because their postsurgical follow-up took place elsewhere in the health-care system within Murcia. Our reasoning for excluding these patients is that these alternative hospitals are not provisioned with specialized nutritional, bariatric, or metabolic surgery nurses for the monitoring, either prior to or following surgery, of patients undergoing RYGB. This is paramount since nurses are responsible for coordinating the entire patient treatment team during both stages. In the presurgical stage, the team aims for the patient include a drop in weight of 10–15% in order to avoid possible complications during laparoscopy and to help the patient develop a commitment to acquire and maintain healthy habits. In order to achieve these aims, the nurse specialist has periodic meetings with patients, with no more than 15–20 days between appointments, prescribes and supervises low-calorie diets (1,000–1,500 kcal per day), including very low-calorie diets, thus avoiding deficiencies in micronutrients, and advises patients to incorporate physical exercise adapted to their physical limitations into their routines. During the postsurgical stage, the gradual loss of weight and dietetic adjustments remain priorities, and these aims are reinforced as per the presurgical stage. The nurse specialist advises patients on the reintroduction of different foods in a stepwise fashion, from multiple intakes of liquids to solids over the course of 6–12 weeks, depending on patient tolerance. Over the first 15 days, a liquid diet is indicated to ensure the supply of macronutrients, which normally requires a supplementary protein supply. Subsequently, a semiliquid stage begins with the addition of adding pureed carbohydrates (potatoes, vegetables, and legumes) together with a gradual increase in white meats, fish, and eggs. At approximately 2 months, the intake of solids commences, with patients progressively increasing quality and quantity as tolerated. Such progressive diets require monitoring, particularly in the immediate postsurgical stage, with revisions occurring every 7–10 days for which consultation with a nurse is essential because any dietary transgressions may have harmful consequences. Once again, the nurse also emphasizes the importance of progressive physical exercise adapted to the patient’s condition.
Data Collection
We collected data from medical records for a range of metabolic disorders as well as other related variables at three stages: prior to surgery and at 3 and 9 months following surgery. We categorized the data as sociodemographic variables (age and gender), clinical background (psychiatric and cardiovascular history), body mass index (BMI), biochemical parameters (baseline blood glucose level [BGBL], glycated hemoglobin [HbA1c], total cholesterol [TC], triglycerides [TG], low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol [HDL-C], uric acid, gamma-glutamyl transpeptidase [GGT > 61 U/L], glutamic–pyruvic transaminase [GPT > 40 U/L], and glutamate-oxaloacetate transaminase [GOT > 38 U/L]), clinical parameters (arterial blood pressure [BP], systolic blood pressure [SBP], and diastolic blood pressure [DBP]), diagnosed metabolic diseases (DM, AHT, DLP, and hyperuricemia), and the pharmacological treatment for each one. We classified participants by BMI according to the American Society for Metabolic and Bariatric Surgery (Aills, Blankenship, Buffington, Furtado, & Parrott, 2008): normal weight (18.5–24.9 kg/m2), Grade 1 overweight (25–26.9 kg/m2), Grade 2 overweight or preobesity (27–29.9 kg/m2), Type 1 obesity (30–34.9 kg/m2), Type 2 obesity (35–39.9 kg/m2), Type 3 or morbid obesity (40–49.9 kg/m2), Type 4 or extreme obesity (50–50.9 kg/m2), or Type 5 obesity (≥60 kg/m2).
We diagnosed MS using the international criteria established by the WHO (Alberti & Zimmer, 1998). According to the WHO, the main criteria are alterations to baseline blood sugar levels (baseline fasting blood glucose > 110 mg/dl and/or blood glucose ≥ 140 mg/dl following a 2-hr glucose tolerance test), glucose intolerance (baseline fasting blood glucose > 126 mg/dl or blood glucose > 140 mg/dl and <200 mg/dl following a 2-hr glucose tolerance test), or DM (baseline fasting blood glucose > 126 mg/dl or blood glucose > 200 mg/dl following a 2-hr glucose tolerance test) and two or more of the following: BP ≥ 140/90 mmHg, TG ≥ 150 mg/dl, HDL-C < 35 mg/dl in men or <39 mg/dl in women, abdominal obesity (waist–hip ratio > 0.90 in men or >0.85 in women), and/or BMI > 30 kg/m2.
We defined improvement in metabolic or psychiatric comorbidity as a reduction in pharmacological treatment and changes in biochemical parameters as well as a change in medical diagnosis recorded by a clinical specialist in the patient’s medical history. For example, if at the 3- and 9-month time points, we noted a reduction in blood glucose levels and a reduction or suppression of insulin or antidiabetic treatment and there was no diagnosis of DM recorded, we considered that the patient no longer presented this pathology. Likewise, if we did not note a reduction in anxiolytic and/or antidepressant treatments and the psychiatric illness persisted in a patient’s postsurgical reports, we considered that there had been no positive progress regarding this diagnosis.
Ethical Considerations
The present study complied with all prerequisites as established by the HCUVA Ethical Committee, whose approval we obtained prior to carrying out the research. Likewise, we guaranteed complete anonymity and confidentiality for all data and information relative to patients in accordance with the Spanish law “Ley Orgánica 15,” passed on December 13, 1999, regarding the protection of personal data. The researcher responsible for gathering the data from the medical records compiled these in both electronic and paper format. The researcher then generated a database devoid of any personal information that might allow the identification of the patients, wherein medical record numbers were replaced with an alternative numbering system. Access to this file was controlled via a password.
Data Analyses
We performed statistical analyses using SPSS software version 22.0, with statistical significance set at p < .05. We analyzed variables using basic descriptive statistical calculations, frequencies, arithmetical average, and standard deviation, all with a confidence interval of 95%. We tested the assumption of normality prior to contrast testing the hypothesis. For the bivariate analysis of two qualitative variables, we used the χ2 test. We used McNemar’s nonparametric test for the analysis of two paired proportions and the nonparametric Cochran’s Q test for more than two correlated proportions. To study the efficacy of RYGB surgery at the different time points, we performed a partially repeated measures analysis of variance as a multivariate analysis.
Results
The final study population comprised 146 patients with an average age at the time of surgery of 42.2 ± 11.9 years, and the majority was female (69.2%). Of these patients, 10 (6.8%) had suffered a cardiovascular event prior to RYGB and, at the time of surgery, 27 (18.5%) had been diagnosed with mixed anxiety-depressive disorder and had received pharmacological treatment.
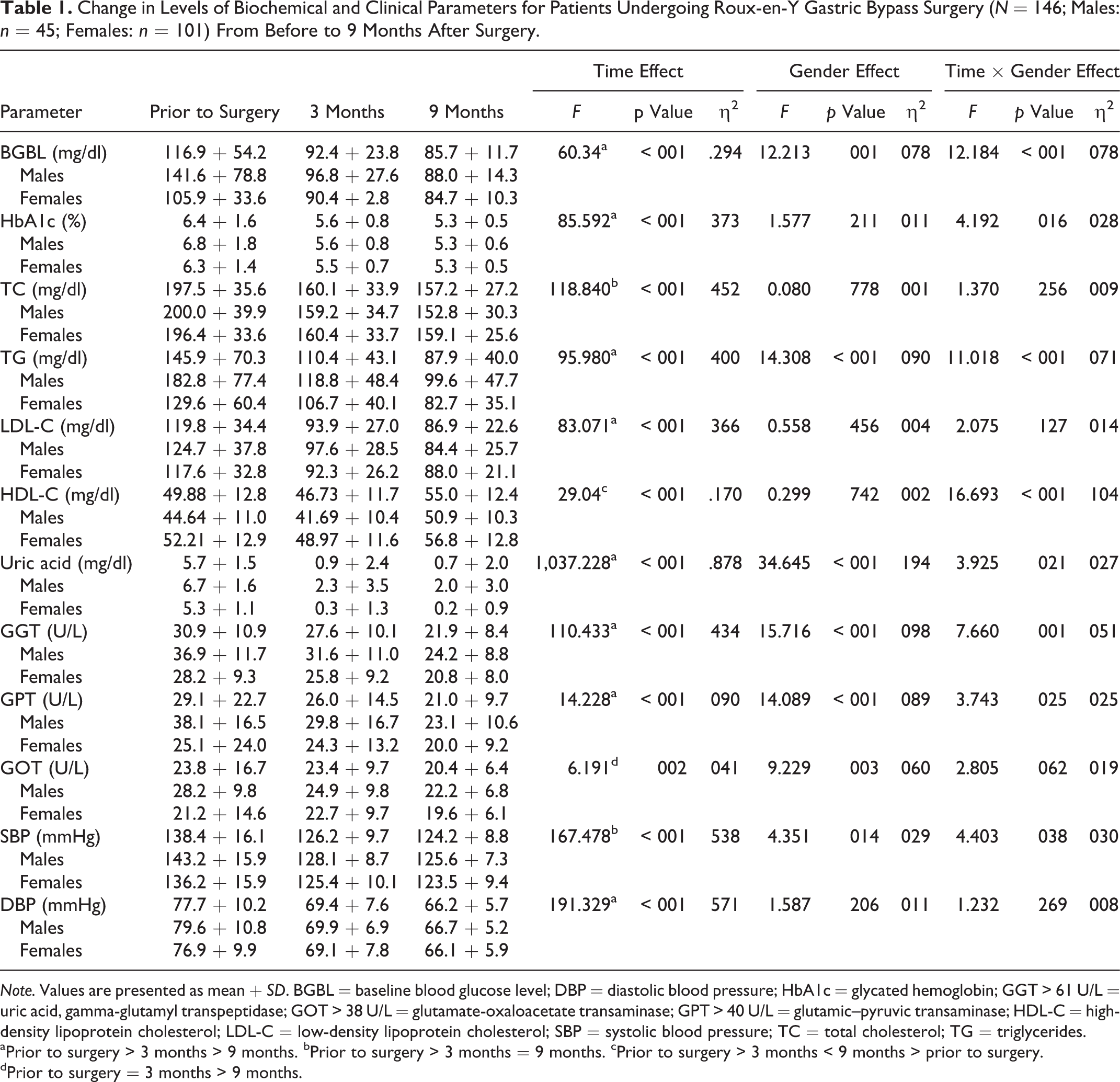
The biochemical parameters we assessed underwent progressive and statistically significant improvements from presurgery to both 3 and 9 months following RYGB except for GOT, which showed no change from presurgery to 3 months but had decreased significantly by 9 months. HDL-C values, meanwhile, decreased from presurgery to 3 months but then increased from 46.7 ± 11.7 mg/dl at 3 months to 55.0 ± 12.4 mg/dl at 9 months (p < .001), which represents an improvement. Males showed greater improvement in HDL-C, BGBL, HbA1c, TG, GGT, and GPT than females, but the decrease in uric acid was greater for females (Table 1). Regarding the clinical parameters, males showed greater improvement than females in SBP.
Change in Levels of Biochemical and Clinical Parameters for Patients Undergoing Roux-en-Y Gastric Bypass Surgery (N = 146; Males: n = 45; Females: n = 101) From Before to 9 Months After Surgery.
Note. Values are presented as mean
aPrior to surgery > 3 months > 9 months. bPrior to surgery > 3 months = 9 months. cPrior to surgery > 3 months < 9 months > prior to surgery.
dPrior to surgery = 3 months > 9 months.
At the presurgical consultation, 54.2% (79/146) of patients had AHT, 28.1% (41/146) had DLP, 33.6% (49/146) had DM, and 21.9% (15/146) had hyperuricemia. Obesity was the only metabolic alteration present in 100% of subjects. Furthermore, 49 patients (33.6%) met the WHO criteria for metabolic syndrome. Finally, depressive symptoms were present in 18.5% (27/146) of the patients. All metabolic conditions improved from prior to surgery to 9 months after, with a significant decrease in the number of patients having AHT, DLP, DM, obesity, hyperuricemia, and MS (Table 2; Figure 2). The number of patients diagnosed with depression, however, remained the same throughout the study period (Table 2). At the completion of the research period, only one patient still met the WHO criteria for MS.
Change in Metabolic and Psychiatric Comorbid Conditions From Prior to Roux-en-Y Gastric Bypass Surgery to 9 Months After.
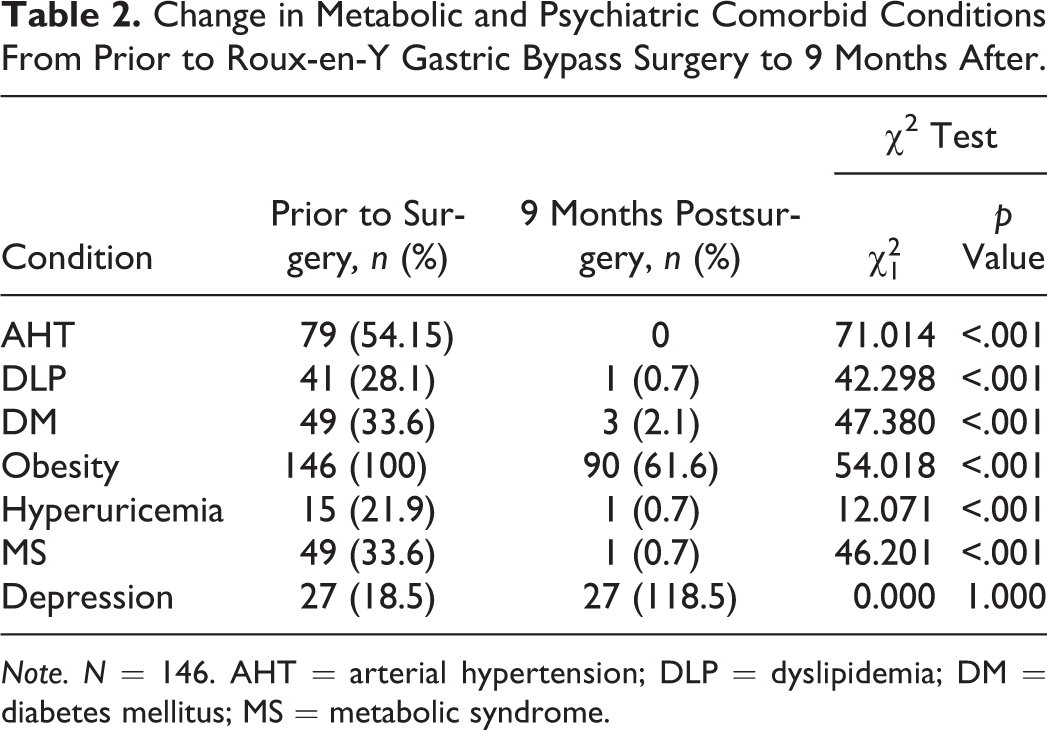
Note. N = 146. AHT = arterial hypertension; DLP = dyslipidemia; DM = diabetes mellitus; MS = metabolic syndrome.
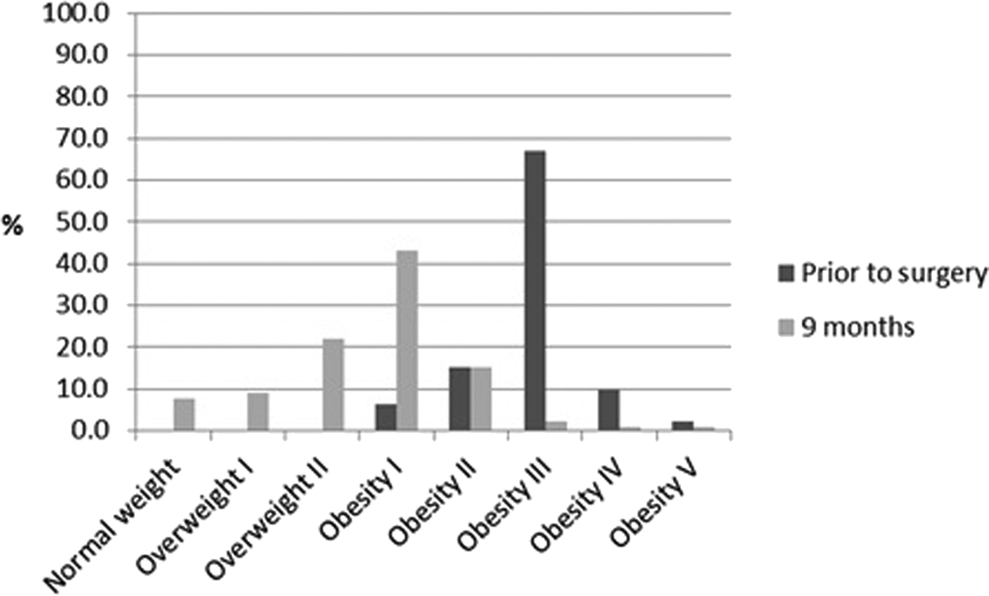
Change in the classification of subjects by weight from prior to Roux-en-Y Gastric Surgery to 9 months after (N = 146).
The improvement and/or resolution of the metabolic comorbidities were manifested in a reduction or elimination of the pharmacological treatments prescribed (Table 3). The prescription of antihypertensive medication dropped from 53.4% prior to surgery to 0.0% at 9 months, oral antidiabetic treatment dropped from 34.2% prior to surgery to 1.4% at 9 months, insulin therapy decreased by 100% by 9 months, and anti-DLP medication also showed a 100% reduction. We found no modifications in the pharmacological treatment of psychiatric comorbidities from prior to surgery to 9 months after, however.
Change in Pharmacological Treatment of Metabolic Comorbidities From Prior to Roux-en-Y Gastric Surgery to 9 Months After Surgery.
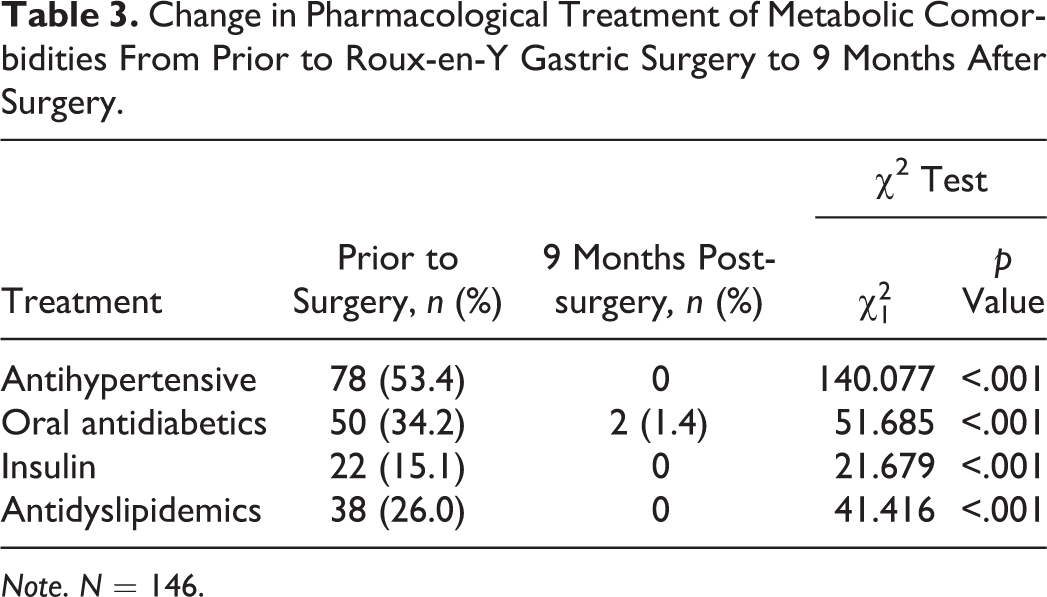
Note. N = 146.
Discussion
Therapeutic failure in the treatment of obesity has contributed to an alarming and insidious increase in this condition (Nepal et al., 2015). The association between obesity and certain metabolic disorders leads to deterioration in quality of life and an increased risk of cardiovascular morbidity and mortality, thus increasing health-care expenditures and constituting a serious challenge for modern society (Ortiz et al., 2014). Studies have also noted an association between obesity and psychiatric comorbidities, which adds to both the health risks and the economic costs of the condition. In the present study, we found that both weight and metabolic comorbidities improved significantly over 9 months after patients underwent RYGB surgery to treat obesity but that psychiatric comorbidities, specifically depression, remain unchanged.
Several authors have observed a beneficial response in obese patients to BS, reporting not only a lasting loss of weight but also an improvement with regard to MS (Bondugulapati, Eligar, & Rees, 2014; Mohos et al., 2011; Shuai, Tao, Mori, & Kanda, 2015). RYGB is considered the gold standard of metabolic surgery (Bays et al., 2009; Yang et al., 2015). A recent study demonstrated the cardioprotective effect of RYGB surgery due to its effect on the lipid profile independent of loss of weight (Osto et al., 2015), whereas the effects of other bariatric procedures are primarily attributable to weight loss (Aminian, Zelisko, Kirwan, Brethauer, & Schauer, 2015). The present study demonstrates the efficacy of RYGB for improving the lipid profile of the study population, showing a progressive and statistically significant reduction in TC, TG, and LDL-C until at least 9 months after surgery. Furthermore, our results confirm the cardioprotective effect found in previously published research through the increase in HDL-C levels in our sample. We also found that DLP improved most of all of the metabolic comorbidities as a result of this surgical procedure at 9 months postsurgery.
In the present study, we also observed a reduction of 93.9% in the number of patients diagnosed with DM from presurgery to 9 months after surgery along with a corresponding decrease in the prescription of oral antidiabetics and insulin. Findings of prior research support these results. Schauer et al. (2012) compared the efficacy of three different treatments over a 12-month period: RYGB, another bariatric procedure, and a conservative treatment (healthy lifestyle and pharmaceutical drugs). They found a reduction in HbA1c for all groups (6.4 ± 0.9%, 6.6 ± 1.0%, 7.5 ± 1.8%, respectively), with the RYGB group demonstrating the greatest change. In a more recent study, investigators found a reduction of 83% in HbA1c at 1 year following RYGB in diabetic patients with a BMI > 30 kg/m2 and of 80% in those with a BMI < 30 kg/m2 (Kaska, Proczko, Kobiela, Stefaniak, & Śledziński, 2014).
Hyperuricemia is another metabolic disorder that has shown improvement in response to BS and in particular to RYGB surgery (Oberbach et al., 2014). Previous authors have provided evidence of a positive effect of BS on levels of transaminases (Dumas, Kinross, & Nicholson, 2014; Ricci et al., 2008). Very few researchers, however, have examined the effects of RYGB on these enzymes. In one recent study, authors reported that RYGB attenuated NAFLD in mice (Verbeek et al., 2014). Results from the present study for GGT, GPT, and GOT were similar to those mentioned above. However, more experimental and clinical analyses are required in order to better understand the effects of RYGB on MS and fatty liver disease.
Regarding psychiatric comorbidity, the available scientific literature is unclear as to whether BS improves mental health in those diagnosed prior to surgery. In a study with follow-up over a 36-month period, researchers reported that, following BS, participants experienced a reduction in occasional bouts of depression, yet they found no positive effect on anxiety (De Zwaan et al., 2011). Furthermore, Herpertz et al. (2003) suggest in their systematic review of the effects of BS on psychosocial functioning that BS actually reinforced psychiatric symptoms among patients with severe psychiatric comorbidity prior to surgery, thus leading to a reduction in quality of life. The results of the present study shed little light on this issue because we found no improvement in the number of patients prescribed antidepressants 9 months after RYGB surgery. However, the number of patients with psychiatric issues in our sample was small, which may have limited our ability to detect a significant change.
Given the present findings and those reported in the literature, then, it would seem that BS, applied in isolation, is more effective in addressing the metabolic than the psychiatric comorbidities that accompany obesity. The search for strategies to overcome this limitation is hindered by the lack of research examining this issue. However, researchers in one innovative, randomized study that compared improvement in depressive symptoms in those who had participated in behavioral therapy following RYGB with those who had received standard follow-up measures reported that 24% of participants receiving integrated treatment experienced a decrease in depressive symptoms, while only 6% of those subject to standard follow-up reported improvements (p < .001; Petasne Nijamkin, Campa, Samiri Nijamkin, & Sosa, 2013). Our results in the present study as well as those of previous studies in which authors found no effect of BS on psychiatric comorbidity combined with the findings of Petasne Nijamkin et al. suggest a need to provide integrated educational programs based on motivational behavior following BS to reduce psychosocial comorbidity and thus achieve improved quality of life.
A limiting factor of the present study is the dependence on medical records and the resultant restriction of available variables. One of the initial aims that we proposed in the project application was to assess the eating habits of patients following BS. However, because such variables were not documented in the patients’ medical records, this aim was not achievable. Likewise, we were not able to control for other variables of interest such as marital status, number of offspring, level of education, and employment status as potential confounding factors in this research because they were also not available in the records.
Thus, while our study provides strong evidence supporting RYGB surgery as an effective alternative method for combating metabolic comorbidities related to obesity, our findings and those of previous studies suggest that the procedure is not equally effective in treating psychiatric comorbidities. It is important that nurses are aware of alternatives to unsuccessful conservative treatments for obesity and its associated comorbidities, as well as the limitations they entail, and that researchers continue to explore methods for improving both metabolic and psychiatric outcomes of obesity treatment and, thus, quality of life for patients undergoing such treatment.
Footnotes
Acknowledgments
We wish to express our deepest gratitude to the HCUVA Ethical Committee, Registry and Codification Departments. Thanks to their collaborative efforts, this manuscript is now available to readers.
Authors’ Contribution
V. E. Fernández-Ruiz contributed to conception, design, data acquisition, analysis and interpretation; drafted the manuscript; critically revised the manuscript; gave final approval; and agrees to be held accountable for all aspects of work ensuring integrity and accuracy. D. Armero-Barranco contributed to conception, design, data analysis, and interpretation; drafted the manuscript; critically revised the manuscript; gave final approval; and agrees to be held accountable for all aspects of work ensuring integrity and accuracy. J. M. Xandri-Graupera contributed to conception, design, data acquisition, analysis, and interpretation; drafted the manuscript; critically revised the manuscript; gave final approval; and agrees to be held accountable for all aspects of work ensuring integrity and accuracy. J. A. Paniagua-Urbano contributed to conception, design, data acquisition, analysis, and interpretation; drafted the manuscript; critically revised the manuscript; gave final approval; and agrees to be held accountable for all aspects of work ensuring integrity and accuracy. M. Solé-Agustí contributed to conception, design, data acquisition, analysis, and interpretation; drafted the manuscript; critically revised the manuscript; gave final approval; and agrees to be held accountable for all aspects of work ensuring integrity and accuracy. J. Mulero contributed to conception, design, data acquisition, analysis, and interpretation; drafted the manuscript; critically revised the manuscript; gave final approval; and agrees to be held accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was sponsored by the Public Healthcare Service of Murcia, Spain.