
Abstract
Oxytocin (OT), a neuropeptide produced primarily in the hypothalamus, is associated with both critical physiological and psychological processes, particularly stress and feelings of affiliation. Increasingly, researchers are seeking ways to reliably incorporate OT as an outcome biomarker in clinical research. Previously, OT levels were measured in plasma or urine. Recently, researchers have measured this biomarker in saliva, particularly when conducting research in clinical and community settings. In spite of increased interest in the use of salivary OT in clinical research, procedures for handling, transport, and analysis of specimens vary. It is not known if significant OT protein degradation occurs if samples are initially transported on wet ice before being frozen. The aim of this study is to evaluate the effect of transport media (wet vs. dry ice) on OT levels derived from saliva collected from 12 postpartum women residing in the community. Saliva collected from each participant was divided between two microcentrifuge tubes (MIDSCI, Valley Park, MO), one placed on wet ice and one on dry ice for transport from the participant’s home to the laboratory freezer. Time from collection to storage freezer was recorded. Laboratory personnel, blinded to method of transport, batch processed the samples. No significant differences in OT levels were found by transport method. Despite large interperson variations in OT levels, there were negligible intraperson variations. Although further research is required to identify factors (including transport time) related to interperson variation, this study supports the use of wet ice as a means of transporting salivary OT specimens in community-based research.
Oxytocin (OT), a neuropeptide produced primarily in the hypothalamus, has been widely studied in relationship to pregnancy, birth, and lactation. Accumulating biobehavioral research now links OT with a variety of behavioral responses such as building of social bonds and response to stress (Carter et al., 2007). This important biomarker provides an opportunity to further explore the relationship of human physiological responses to a variety of behavioral situations including behavioral disorders (Hoffman, Brownley, Hamer, & Bulik, 2012), sleep stage (Blagrove et al., 2012), lactation (White-Traut et al., 2009), and parental caregiving (Feldman, Gordon, Influs, Gutbir, & Ebstein, 2013). Earlier research used primarily plasma-derived OT. More recently, investigators have sought reliable procedural approaches for collecting and handling saliva-derived OT. Salivary OT may be easier to obtain from participants, but it poses greater challenges in analysis due to differences in the peripheral environments of plasma and saliva. Identifying procedures to reliably collect salivary-derived OT in a community setting is of value to clinical researchers seeking to use this biomarker.
Previous research involving measurement of OT occurred in laboratory settings with handling of the saliva samples taking place under very controlled conditions. Unlike plasma, saliva contains proteolytic enzymes and fosters bacterial growth that can accelerate degradation of the OT protein (McCullough, Churchland, & Mendez, 2013). Early freezing of samples is thought to reduce degradation risk (Wilde, Out, Johnson, & Granger, 2013). Unfortunately, the use of dry ice, which flash freezes the saliva sample at the time of collection, requires an additional level of procedural complexity and contains some physical risk should participants or study personnel come in direct contact with the dry ice. The latter is of particular concern for studies in which there may be young children in the homes where samples are collected.
It is not known how much OT proteins may be degraded if the sample is not immediately frozen. Some researchers have collected samples in the home and had the samples refrigerated or kept on wet ice until they could be transferred to a laboratory freezer. For example, White-Traut et al. (2009) used salivary OT samples from lactating women who self-collected saliva samples by passive drool at repeated times over 2 days in a home setting. Participants stored samples in their refrigerators until research assistants retrieved them at the end of each 24-hr period. Samples were transported on wet ice and then centrifuged at −4°C when they arrived in the lab, after which they were stored at −80°C until being assayed. Results from that study provided evidence that reliable OT levels could be obtained from community-collected samples. Other researchers had participants immediately place saliva samples in their home freezers (Holt-Lunstad, Birmingham, & Light, 2011) before transporting the samples to the laboratory typically on wet ice.
At present, there is no evidence supporting the superiority of the effects of transportation using either dry or wet ice on the quality of the final samples. The primary aim of the present study was to compare salivary OT levels in two saliva samples simultaneously collected in participants’ homes, with one transported on wet ice and the other transported on dry ice to the laboratory. A secondary aim was to explore any effects on OT levels associated with time of transport of the saliva samples from collection to placement of samples in the laboratory freezer.
Method
Study Procedures
The appropriate institutional review boards and administrators approved all study procedures, including protocols for recruiting participants and obtaining written informed consent. We recruited 12 postpartum women from two community-based obstetrical clinics. Saliva was collected from each participant in her home during a single study visit. We encouraged participants to drink plenty of fluids and avoid caffeine-containing drinks beginning 6 hr before the designated collection time. During the study visit, we asked each participant to rinse her mouth thoroughly to remove any food residue. We did not attempt to control for timing of the last infant feeding, but during the saliva collection, we encouraged the participant to envision feeding her infant in order to promote increased OT release (Uvnäs-Moberg, 1998). Prior to and during saliva collection, we kept saliva collection tubes (UltraSal-2 tubes; Salimetrics, Carlsbad, CA) chilled on wet ice.
Passive drool saliva samples were collected from each participant in the following manner. After 1 min of saliva saving, the participant was instructed to release the saliva by passively drooling into the collection tube. Saliva was repeatedly collected in 1-min increments and until the level in the collection tube reached 2 ml. We recorded the participant identification code, date, and time and then used a micropipette to draw up and transfer two aliquots (0.6 ml each) of the sample into chilled microcentrifuge tubes (MIDSCI, Valley Park, MO). One aliquot was placed in dry ice covering the sample. The other aliquot was placed on wet ice covering the sample. The order in which samples were placed on dry and wet ice was randomly assigned by participant and recorded. Research assistants recorded the time the saliva sample was collected from the participant and the time the sample was placed in the study freezer. We designated the elapsed time as transport time. Samples were transported to the specimen freezer where they were held at −80 °C until all samples were batch shipped overnight on dry ice the Ohio State University College of Nursing Biomedical Research Laboratories. Laboratory personnel were blinded to type of transport medium.
Laboratory Procedures
In humans, researchers have quantitatively measured OT levels in plasma, saliva, urine, and other biological fluids by radio immunoassay (RIA) and enzyme-linked immunosorbent assay (Boyd, Jackson, Hollingsworth, Forsling, & Chard, 1972; Chard, Boyd, Forsling, McNeilly, & Landon, 1970). Since 2004, commercially available immunoassays have been used successfully in biomedical and behavioral research efforts (Prakash, Metten, Schams, & Wuttke, 1998). The OT neuropeptide is extremely labile, making sample collection and storage difficult. Under most physiologic conditions, OT levels in peripheral tissues fall below most biomedical assay detection limits. Additionally, a number of related compounds, mesotocin and vasotocin in particular, have significant cross-reactivity to OT (Robinson, 1980). Some assay protocols recommend sample concentration to increase OT levels to measurable detection thresholds. Other protocols include high-performance liquid chromatography (HPLC) extraction to isolate OT peptides (Bello, White-Traut, Schwertz, Pournajafi-Nazarloo, & Carter, 2008; Sarkar & Prakash, 2006). Since the purpose of the present study was to evaluate procedures for transporting saliva samples and not tissue-specific measurements, we chose to concentrate the samples instead of using HPLC extraction. This decision was supported by the work of Kramer, Cushing, Carter, Wu, and Ottinger (2004) and Zak, Kurzban, and Matzner (2004), who successfully measured OT levels using commercially available immunoassays without HPLC extraction.
We also chose an immunoassay to measure OT levels after reviewing the considerable time and technical requirements for RIA. The commercially available Enzo immunoassay (ADI-900-15A; Farmingdale, NY) uses a competitive binding polyclonal antibody to quantitatively measure OT in biological samples. Optical density is measured at 405 nm for an alkaline phosphatase enzyme reaction that is used to quantitatively determine OT concentration. The intensity of the detected optical density is inversely proportional to the concentration of OT in the standards provided by the manufacturer and the experimental samples.
Samples arrived at the Ohio State University College of Nursing Biomedical Research Laboratories in plastic microcentrifuge tubes frozen on dry ice. The samples were stored at −80°C until being placed directly in a Millrock BenchTop lyophilizer (Kingston, NY) for concentration. After lyophilization, the samples were reconstituted with 200 μl of assay sample diluent, resulting in a 2.5× experimental sample. The manufacturer’s instructions were followed without modification except the samples were concentrated as described above prior to analysis instead of using C18 HPLC column for extraction.
Briefly, 100 μl samples, standards, and control buffers were added to a 96-well plate in duplicate. A standard curve was created using known OT solution provided by the manufacturer. Assay diluent was added to nonspecific binding and blank wells to determine background optical density. Antibody conjugate was added to the experimental sample wells and the total activity well to determine assay efficiency. The manufacturer reports that the calculated efficiency of saliva samples is approximately 100% as compared to human plasma (118%) and breast milk (74%). The samples were incubated with the antibody conjugate overnight at 4°C with gentle agitation. All wells were extensively washed to remove unbound proteins, and the alkaline phosphatase enzyme reaction was stopped with an acid solution provided by the manufacturer. The 96-well plate was immediately measured at 405 nm on a BioTek microplate reader (Winooski, VT) to determine optical density. The 96-well plate was then measured at 590 nm to determine optical density in the nonspecific binding and blank wells to determine background.
Background measurements for the Enzo assay were negligible; nonetheless, mean optical density background was subtracted. The intra-assay precision for the experimental wells was determined to be 3.53%. The coefficient of variation was calculated automatically by the BioTek microplate reader based on replicates within the assay. The average standard deviation for the experimental well duplicates was 0.0158.
Statistical Analysis
We used descriptive statistics to evaluate continuous study variables for measures of central tendency and to summarize categorical variables. Due to skewed distributions, we used a Spearman rank-order coefficient correlation to evaluate the relationship between OT concentration and transport time for each of the transport methods. To examine the mean differences in OT concentration by transport method, we used the Wilcoxon signed-rank test.
Results
We recruited 12 postpartum women to participate in the study, of whom 67% were Latinas and 42% reported Spanish as their primary language. Their ages ranged between 28 and 38 years (M = 32.42, SD = 3.37), and 50% had a BA or BS degree. The participants’ infants’ age ranged from 2 to 16 weeks; all participants reported breastfeeding exclusively at the time of the saliva collection. Table 1 shows the salivary OT concentration level (picograms per milliliter) by transport method and transport time in minutes. The mean concentration of OT in saliva samples transported on dry ice was 53.4 (SD = 32.7); the mean concentration of OT for samples transported on wet ice was 48.3 (SD = 31.8).
Salivary Oxytocin Level by Transport Method and Transport Time.
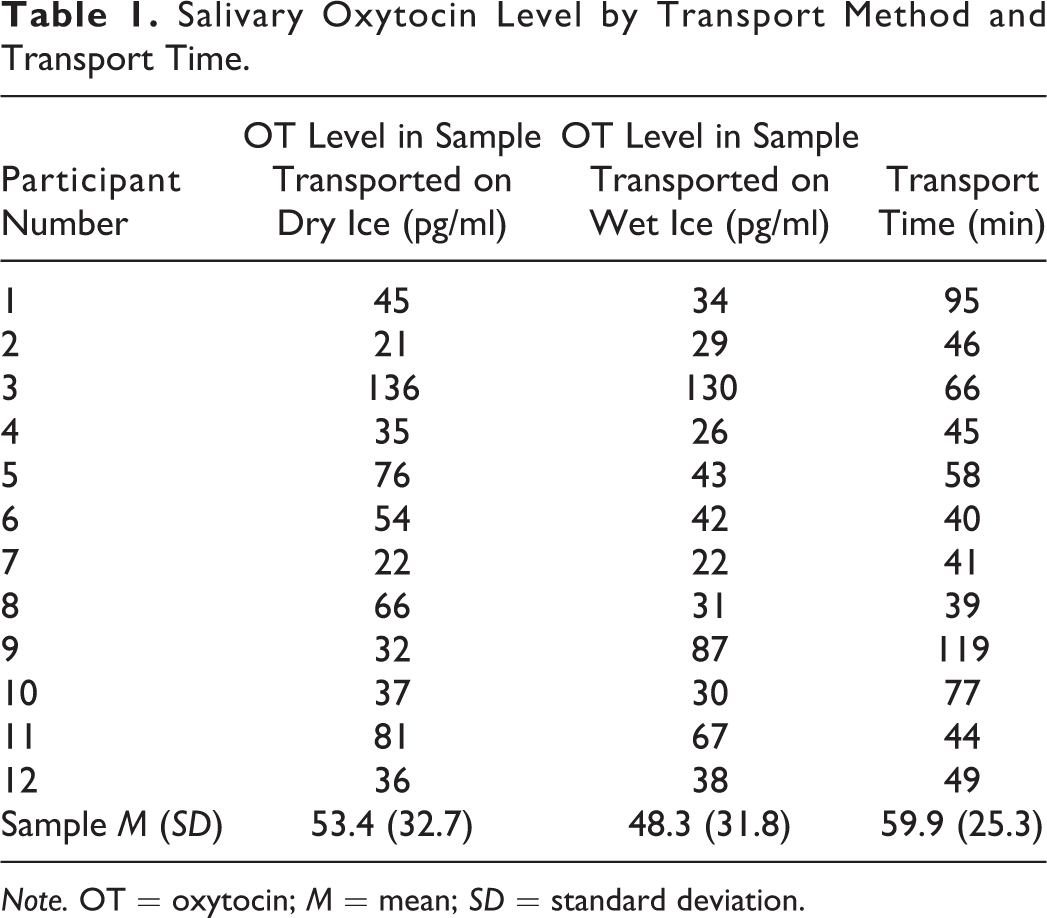
Note. OT = oxytocin; M = mean; SD = standard deviation.
We found no significant correlations between OT level and transport time using dry ice (r = −.070, p > .05) or wet ice (r = .364, p > .05). Moreover, preliminary analysis by visual inspection of scatter plots did not provide reliable evidence of a monotonic relationship between OT levels and either transport method or transport time.
A Wilcoxon signed-rank test indicated the median OT concentration level (picograms per milliliter) increased from the wet ice (Mdn = 36) to the dry ice (Mdn = 41) transport method; 8 of the 12 paired samples showed higher concentrations of OT when dry ice was used, 3 paired samples showed lower concentrations when dry ice was used, and 1 showed no difference. The difference scores were symmetrically distributed as assessed by a histogram. Despite the increase in median OT concentration level in the dry transport samples, the observed differences between paired samples were not statistically significant (z = −1.511, p > .05).
Discussion
For more than 40 years, efforts to accurately measure OT levels in humans by biomedical assay techniques have been met with a variety of collection, transport, storage, and technical difficulties. In order to use OT as a reliable research measure, it is essential that investigators identify procedures to overcome these difficulties. One important procedural aspect of handling salivary OT samples is using a cold transport medium to reduce degradation of the neuropeptide. In the present study, we evaluated differences in recovered OT related to transport time and medium (wet or dry ice).
We observed large between-subject variation in concentration levels of OT and little within-subject variation between transport methods. Previous studies citing measurement of salivary OT have identified factors perturbing the level of OT found in the saliva of various population samples such as enzymatic activity of salivary proteases, viscosity of saliva samples, and concentration of OT in saliva (Carter et al., 2007).
The within-subject variation in this study generally showed slightly higher levels of OT in samples transported on dry ice as compared to wet ice. However, a few samples revealed higher OT levels in samples transported on wet ice compared to dry ice. This inconsistent finding may be explained by the presence of varying levels of OT in the saliva itself, particularly if the saliva was more viscous at the time of sample collection. The viscosity of saliva is quite variable due to a number of factors including age, level of hydration, medications, and chronic diseases (Preoteassa et al., 2014). In the present study, a single saliva sample collected by passive drool was aliquoted by micropipette into two chilled CryoTubes before being placed on ice for transport. There may have been slightly higher concentrations of OT in one or the other of the sample aliquots even though we attempted to control for this by randomly assigning order of samples placed on dry or wet ice for each participant.
In this pilot study, we did not demonstrate any consistent differences in OT levels between the two transport media. The study was limited by the small sample size and varying home conditions under which the saliva was collected. However, we followed a consistent protocol of sample collection, transport, storage, and assay. A larger sample size with more homogenous inclusion criteria might help identify more consistent differences in measurable OT in saliva transported using differing methods. Further, we did not detect differences in OT level by transport time, which averaged 60 min (range = 39–119 min). However, it is reasonable to assume that longer transport time from collection to placement in a laboratory freezer might result in significant degradation of OT level in saliva. Future research is needed to explore this factor in order to develop optimal protocols for collecting salivary OT in a community setting.
Conclusion
Reliable and accurate measurement of OT in saliva has the potential to provide an important measure of effectiveness of interventions aimed at improving mood and well-being in individuals. While laboratory measurement of OT has allowed for an increase in understanding of the relationship of this neuropeptide to human mood and emotional states, the complexity of the sample collection procedures for this biomarker has limited its use as an outcome measure in clinical research. Our findings in the present study suggest that OT concentration may be feasibly and reliably measured from saliva samples obtained in the field and transported on wet ice to clinical research facilities. Replication of this study with a larger sample size is recommended.
Footnotes
Authors’ Note
This article describes original work and has not been published elsewhere, nor is it under consideration for publication by any other journal. Intellectual property, data, and materials generated under this project will be administered in accordance with university and participating institutional policies. Depending on such policies, materials may be transferred to others under the terms of a material transfer agreement.
Author Contribution
Lois C. Howland contributed to conception, design, acquisition, analysis, and interpretation; drafted the manuscript; critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Rita H. Pickler contributed to conception, design, analysis, and interpretation; drafted the manuscript; critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Brent A. Sullenbarger contributed to conception, design, analysis, and interpretation; drafted the manuscript; critically revised the manuscript; and gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy. Cynthia D. Connelly contributed to conception, design, analysis, and interpretation; drafted the manuscript; critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by the National Institute of Mental Health Grant R01-MH075788 to Cynthia D. Connelly and by the University of San Diego Hahn School of Nursing and Health Science Faculty Research Incentive Grant to Lois C. Howland.