
Abstract
Background:
Neonates born small for gestational age (SGA) face increased risk of neonatal mortality, childhood developmental problems, and adult disease. The placenta is a key factor in SGA development because of its multiple biological processes that underlie fetal growth. However, valid and reliable placental biomarkers of SGA have not been determined.
Objectives:
The objective of this article was to systematically identify and review studies examining associations between placental biomarkers and SGA and assess those biomarkers’ predictive value.
Methods:
Use of the matrix method and the PRISMA guidelines ensured systematic identification of relevant articles based on selection criteria. PubMed, CINAHL, and EMBASE were searched for English articles published in 2005–2016 that addressed relationships between placental biomarkers and SGA.
Results:
The search captured 466 articles; 13 met selection criteria. The review identified 14 potential placental biomarkers for SGA, with placental growth factor and soluble fms-like tyrosine kinase 1 being the most commonly studied. However, findings for these and other biomarkers have often been contradictory. Thus, no placental biomarkers have been confirmed as reliable for predicting SGA.
Conclusion:
The inconsistent findings suggest low placental biomarker reliability, perhaps due to the multifactorial nature of SGA. This review is novel in its focus on identifying potential placental biomarkers for SGA, producing a better understanding of how placental function underlies fetal growth. Nevertheless, use of placental biomarkers alone may not be adequate for predicting SGA. Therefore, combinations of biomarkers and other predictive tests should be evaluated for their ability to predict risk of SGA.
Small for gestational age (SGA) is defined as a weight (either in utero estimated fetal weight or birth weight) less than the 10th percentile for a specific gestational age (Vayssiere et al., 2015) and is now the term recommended for describing small fetuses or neonates (Ego, 2013). This definition encompasses the entire spectrum of fetuses, including those who are constitutionally small and those with intrauterine growth restriction (IUGR) who have failed to achieve their growth potential (Wilcox, 2001; Wollmann, 2009). Being born SGA confers risk of increased perinatal, childhood, and adulthood complications (Saleem et al., 2011) such as stunted growth and undernutrition in childhood (Blake et al., 2016) and cardiovascular risk (Lenfant, 2008), metabolic problems (Barker et al., 1993), and poor neurodevelopmental outcomes in adulthood (Savchev et al., 2013). In low- and middle-income countries, an estimated 32.4 million babies were born SGA in 2010, constituting 27% of all live births (Lee et al., 2013), compared to 9–10% in the United States (Talge, Mudd, Sikorskii, & Basso, 2014). Thus, SGA is a greater public health problem in low- and middle-income countries than in developed countries; however, most SGA-prevention studies have been conducted in developed countries (Lee et al., 2013). Given the prevalence and adverse effects of SGA, it is critical that effective screening and treatment procedures be developed for SGA in pregnancy to avoid the adverse health outcomes faced by neonates born SGA.
Several studies have demonstrated that maternal factors are associated with SGA. These factors include age, marital status, education, income, and parity (Ota et al., 2014); body mass index (Frederick, Williams, Sales, Martin, & Killien, 2008); gestational weight gain (Boriboonhirunsarn, 2015); preeclampsia, chronic hypertension, and anemia (Jariyapitaksakul & Tannirandorn, 2013; Ota et al., 2014); alcohol and illicit substance use (Ota et al., 2014); and psychosocial factors such as stressful life events and lack of social support (Sanguanklin et al., 2014). Fetal factors are also associated with SGA, including fetal sex, malformation, and infections (Wollmann, 2009). In addition, placental factors are strongly associated with impaired fetal growth, particularly an abnormal placental vascular system that leads to poor maternal–fetal blood transfusion (Wollmann, 2009).
According to the developmental origins of health and disease (DOHaD) theoretical framework, the normal pattern of fetal development is disrupted by abnormal stimuli that occur at a critical point of in utero development and that influence changes in cell allocation differentiation, tissue and organ growth, and birth weight (Barker, 2007; Gluckman & Hanson, 2006; Rutherford, 2013). Placental adaptation occurs in response to the abnormal stimuli and produces changes in both placental structure and function, resulting in disrupted fetal development that leads to adverse health effects such as diabetes or hypertension in adulthood (Gillman et al., 2007; Myatt, 2006). Disruption of normal placental development also leads to functional alterations in the placenta (Myatt, 2006). Study findings have shown that abnormal placental function was accompanied by alterations in placental vasculogenesis and angiogenesis of the vascular system (Mayhew, Charnock-Jones, & Kaufmann, 2004), in the activity of amino acid transporters (Jansson, Ekstrand, Bjorn, Wennergren, & Powell, 2002), and in hormone and enzyme activities (McMullen et al., 2004). Because the placenta regulates fetal growth and development, playing an active role in programming the fetal experience in utero, placental dysfunction can lead to disease in adult life (Myatt, 2006).
The placenta is the conduit for transferring maternal nutrients to the developing fetus, and research has implicated placental insufficiency in impaired fetal growth and reduced birth weight (Parra-Saavedra et al., 2013). This organ produces many substances that are associated with its function and related to birth outcomes (Ilekis et al., 2016; Myatt, 2006). Placental growth factor and vascular endothelial growth factor are among the substances produced specifically by the placenta (Charnock-Jones, Kaufmann, & Mayhew, 2004), while others are produced by both the placenta (which is primarily of embryonic origin) and the maternal tissue (Haig, 1996). For example, leptin, a polypeptide hormone that regulates body weight and homeostasis, is produced by both the mother and the placenta. Although maternal serum leptin levels during pregnancy are higher than those in nonpregnant women, this hormone is considered a good placental biomarker because leptin levels drop precipitously after the placenta is delivered, suggesting that the rise in leptin during pregnancy is largely due to the placenta (Henson & Castracane, 2000; Yura et al., 1998).
Placental biomarkers reflect placental functions that link placental physiology and fetal growth (Heazell, Whitworth, Duley, & Thornton, 2015). For instance, placental growth hormone (PGH) is predominantly expressed in the syncytiotrophoblast layer of the placenta. PGH can also be detected in maternal circulation from 12 to 20 weeks of gestation up to term, as it gradually replaces pituitary growth hormone. Researchers have observed lower maternal levels of PGH in pregnancies with fetal growth restriction (Evain-Brion & Malassine, 2003). Measurement of placental biomarkers in maternal blood is one common method of evaluating placental functions related to pregnancy outcomes (Zhong, Zhu, & Ding, 2015). However, these placental chemical products can be identified in various locations such as placental tissue, amniochorionic membranes, amniotic fluid, fetal blood, and cord blood as well as maternal blood and urine (Heazell et al., 2015).
Previous systematic reviews have shown that many biomarkers are associated with adverse pregnancy outcomes such as SGA, IUGR, stillbirth, preterm birth, and preeclampsia. These biomarkers include pregnancy-associated plasma protein A, free β-human chorionic gonadotrophin, placental growth factor, placental protein 13, α-fetoprotein, thyroid-stimulating hormone, urinary albumin, and vitamin D (Conde-Agudelo, Papageorghiou, Kennedy, & Villar, 2013; Zhong et al., 2015). However, these systematic reviews did not focus specifically on SGA as an outcome. Moreover, no valid and reliable placental biomarkers related to SGA have been determined. Thus, the purpose of the present article was to systematically identify and review studies examining associations between placental biomarkers and SGA and those biomarkers’ predictive value. By focusing only on potential placenta-specific biomarkers and SGA, we intended to provide a better understanding of how placental function regulates fetal growth as well as information that might help to improve pregnancy outcomes and reduce risks of SGA.
Method
In conducting this systematic review, we were guided by the matrix method of identifying, organizing, and critically evaluating previous research on a topic of interest (Garrard, 2017). The steps of this method, which we applied in the present review, are (1) establishing the purpose of the review, (2) organizing and conducting a search for studies that meet specific criteria, (3) abstracting relevant study components, (4) analyzing and summarizing information across studies, and (5) drawing conclusions based on review results. We also followed the PRISMA flow diagram to ensure systematic identification of relevant articles (Moher, Liberati, Tetzlaff, Altman, & the PRISMA Group, 2009).
Search Strategy
We conducted comprehensive searches in PubMed, CINAHL, and EMBASE, databases that index health science literature, for relevant articles using medical subject headings (MeSH) and the key words biomarkers and biological markers, placenta, small for gestational age, and intrauterine growth restriction. We also reviewed references and bibliographies of relevant articles to identify additional studies. The inclusion criteria for studies were articles (1) published in peer-reviewed journals from 2005 to 2016, (2) in English, (3) with full-text availability online, and (4) that addressed the relationship between placental biomarkers and SGA. Included studies could employ any type of design, experimental, or nonexperimental design. We excluded studies that (1) were case series, reports, editorials, comments, reviews, or unpublished manuscripts; (2) reported placental biomarkers in women with multiple pregnancies or who were diagnosed with preeclampsia or diabetes; or (3) used uterine artery Doppler, as this method is not employed to measure biomarkers.
Selection Process
The initial search of electronic databases produced 466 potentially relevant articles: 163 in PubMed, 126 in CINAHL, and 177 in EMBASE. After a review of all titles, we removed 311 duplicates and irrelevant titles and screened the remaining 155 studies by reading each abstract. Based on the screening, 23 studies warranted full-text retrieval. Also, two studies we identified in article reference lists and bibliographies warranted full-text retrieval. In the end, 13 studies met the inclusion criteria and were included in the systematic review. Figure 1 presents the PRISMA flow diagram depicting the study selection process (Moher et al., 2009).
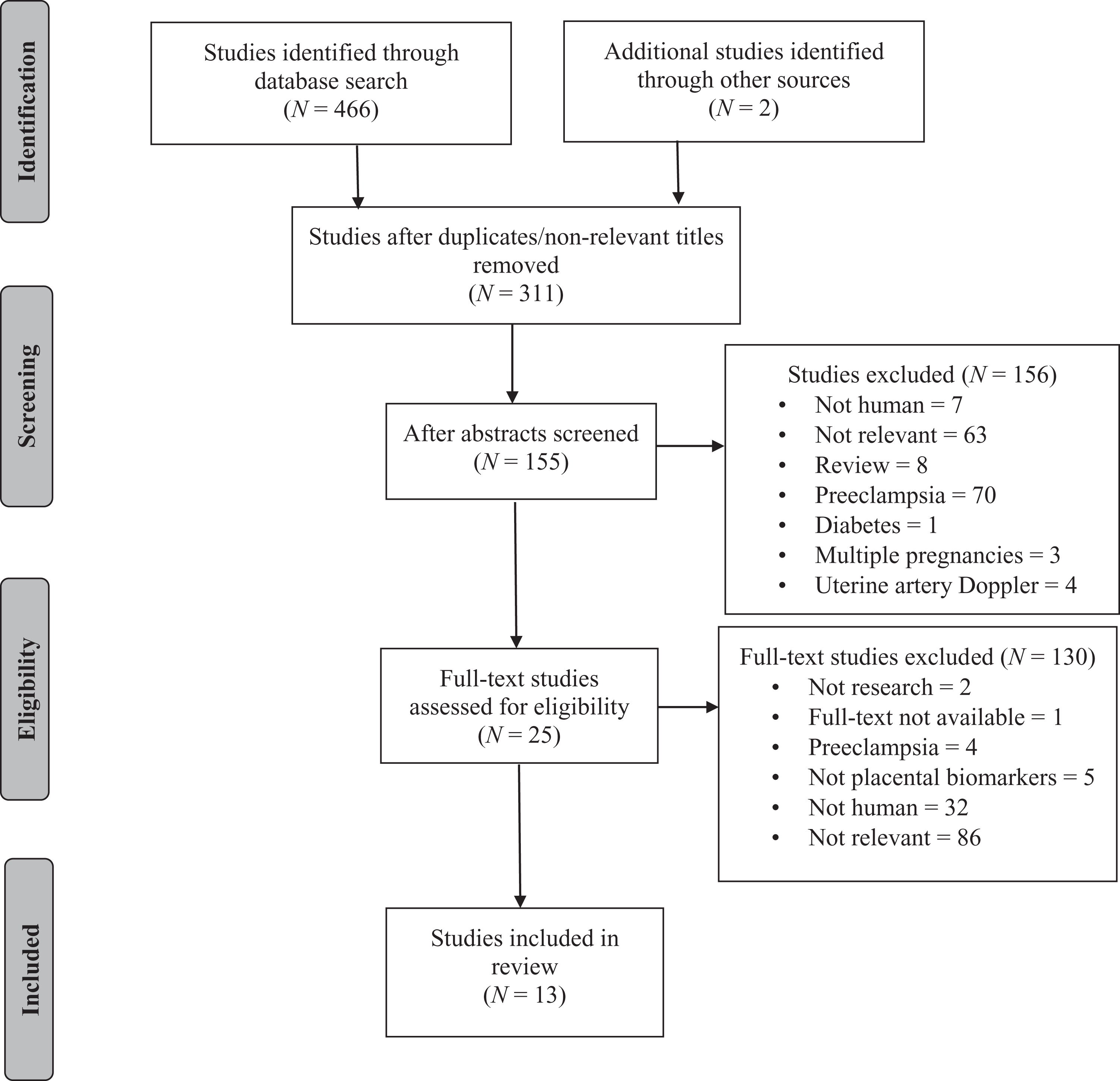
PRISMA flow diagram illustrating the selection process (Moher et al., 2009).
Quality Appraisal
Quality assessment is an integral part of any systematic review because it decreases the risk of bias in review results (Whiting, Rutjes, Reitsma, Bossuyt, & Kleijnen, 2003). In the present review, we used a modified version of the QUADAS tool for the quality assessment of diagnostic accuracy studies (Whiting et al., 2003) based on the approach of Conde-Agudelo, Papageorghiou, Kennedy, and Villar (2013). Evaluation criteria included 5 items important to study quality, each of which we scored as yes, no, or unclear (see Table 1).
Quality Evaluation Criteria for the Studies.
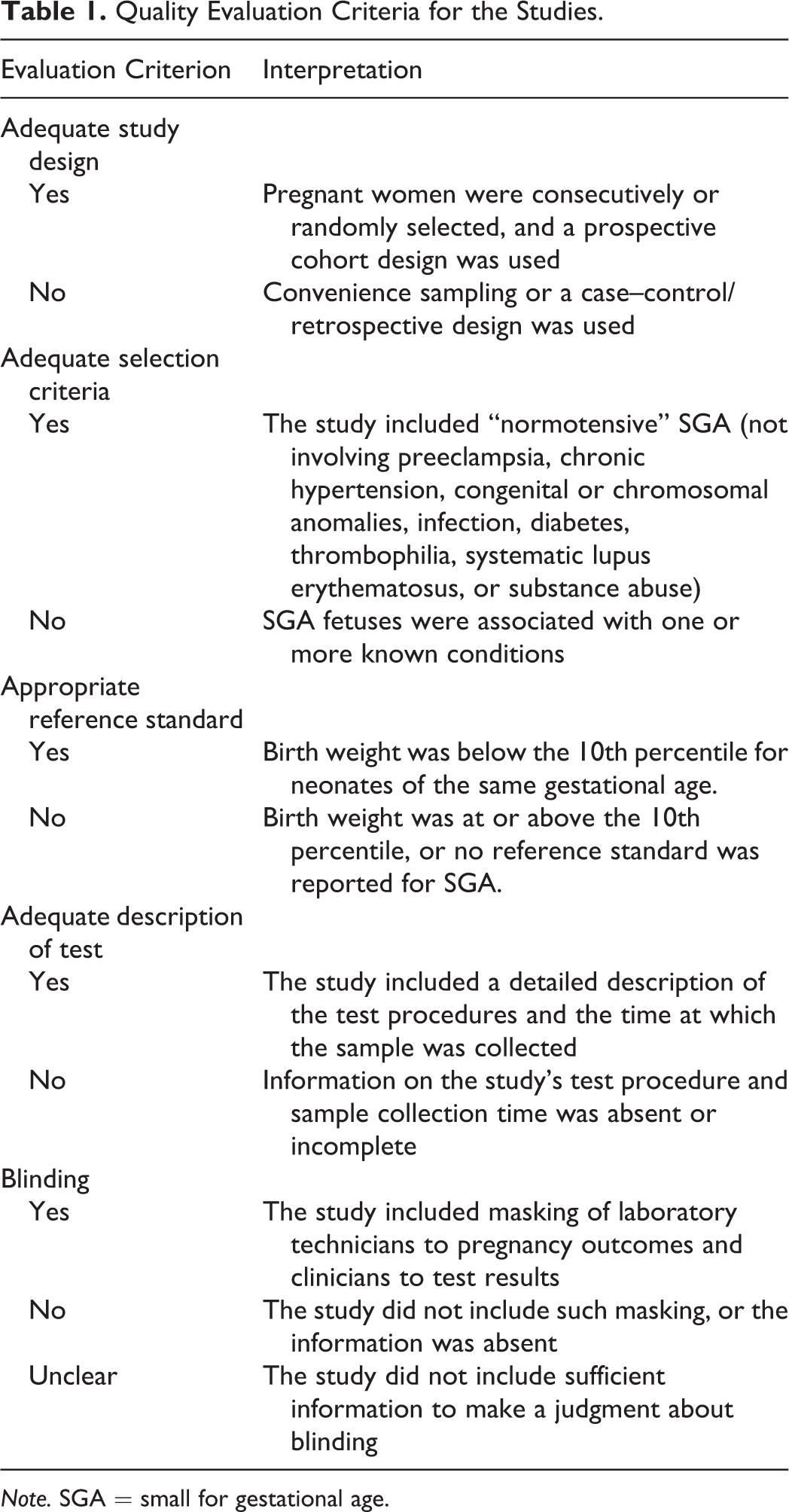
Note. SGA = small for gestational age.
Data Extraction and Analysis
After examining all eligible studies, we developed a review matrix using Garrard’s matrix method as a guide (Garrard, 2017). Some studies reported multiple outcomes; however, we only include findings related to SGA in the discussion below.
Results
Study Quality
We have summarized the quality assessments of the 13 reviewed studies in Figure 2. Most studies (85%) used a prospective design with consecutive recruitment. All 13 studies employed appropriate selection criteria that included normotensive SGA neonates with a birth weight lower than the 10th percentile. Moreover, most studies (85%) provided detailed descriptions of test procedures and sample collection times. However, only 15% of the studies masked laboratory technicians and clinicians to test results.
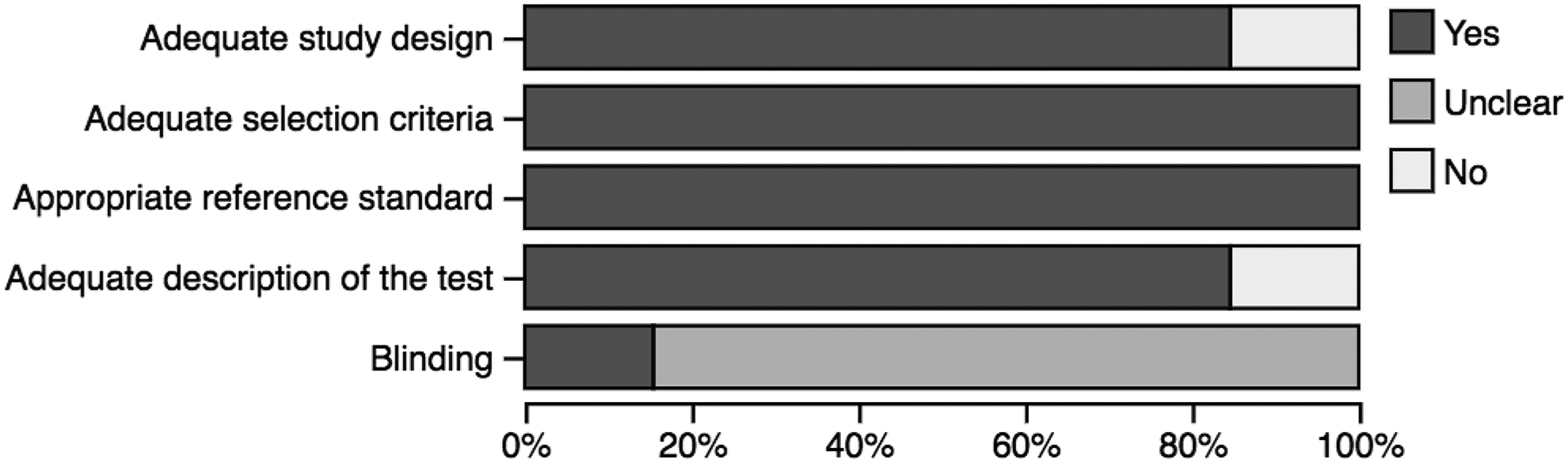
Summary of the quality assessment of the 13 studies reviewed.
Study Characteristics
A total of 13 studies, which comprised a combined sample of 56,041 women and evaluated a total of 14 placental biomarkers, met the inclusion criteria. We list placental biomarkers evaluated in these studies for their ability to predict SGA in Table 2 and summarize the characteristics of the included studies in Table 3.
Placental Biomarkers Predicting SGA in Reviewed Studies.
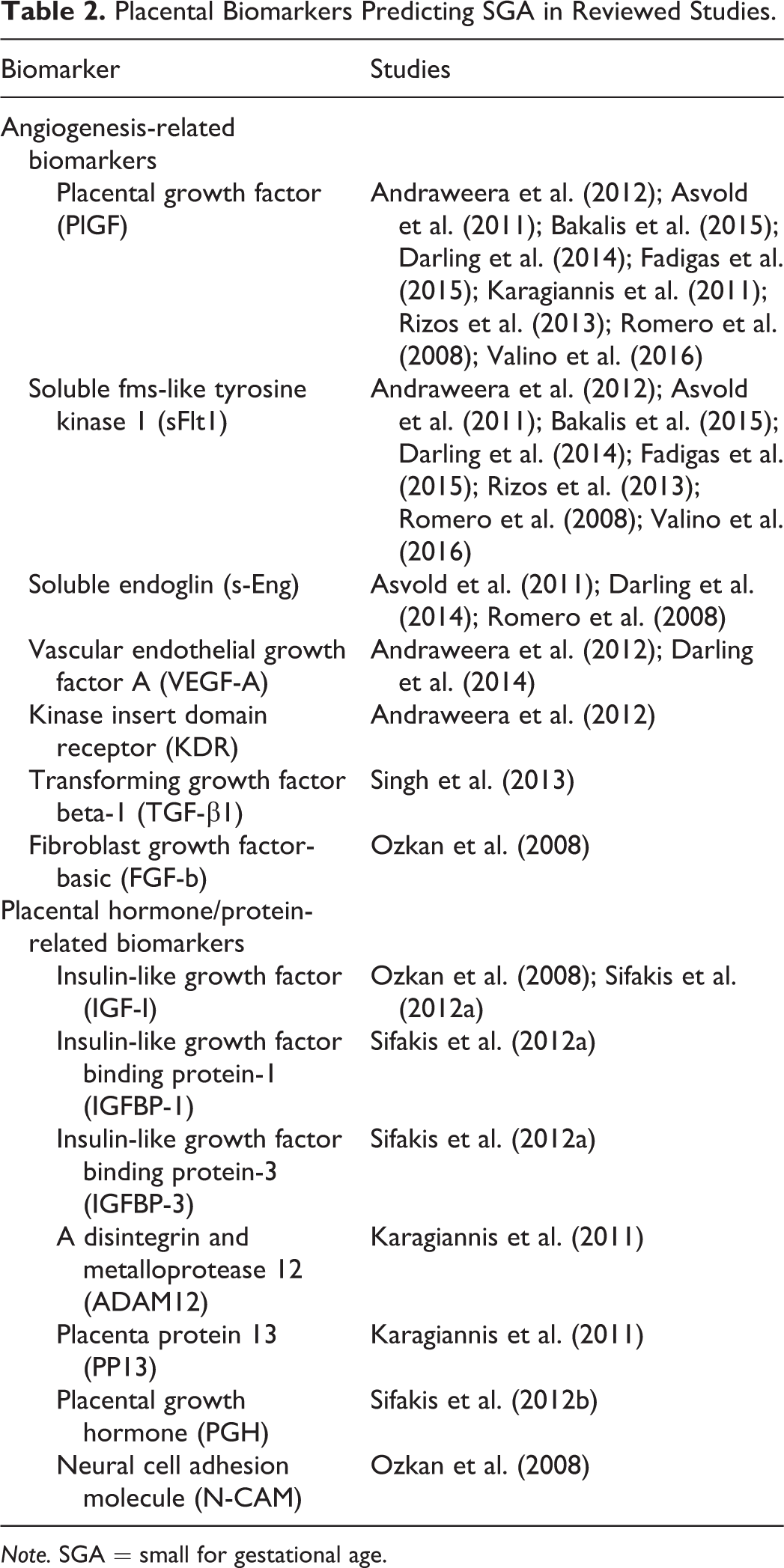
Note. SGA = small for gestational age.
Summary of Reviewed Studies on Placental Biomarkers Predicting SGA.
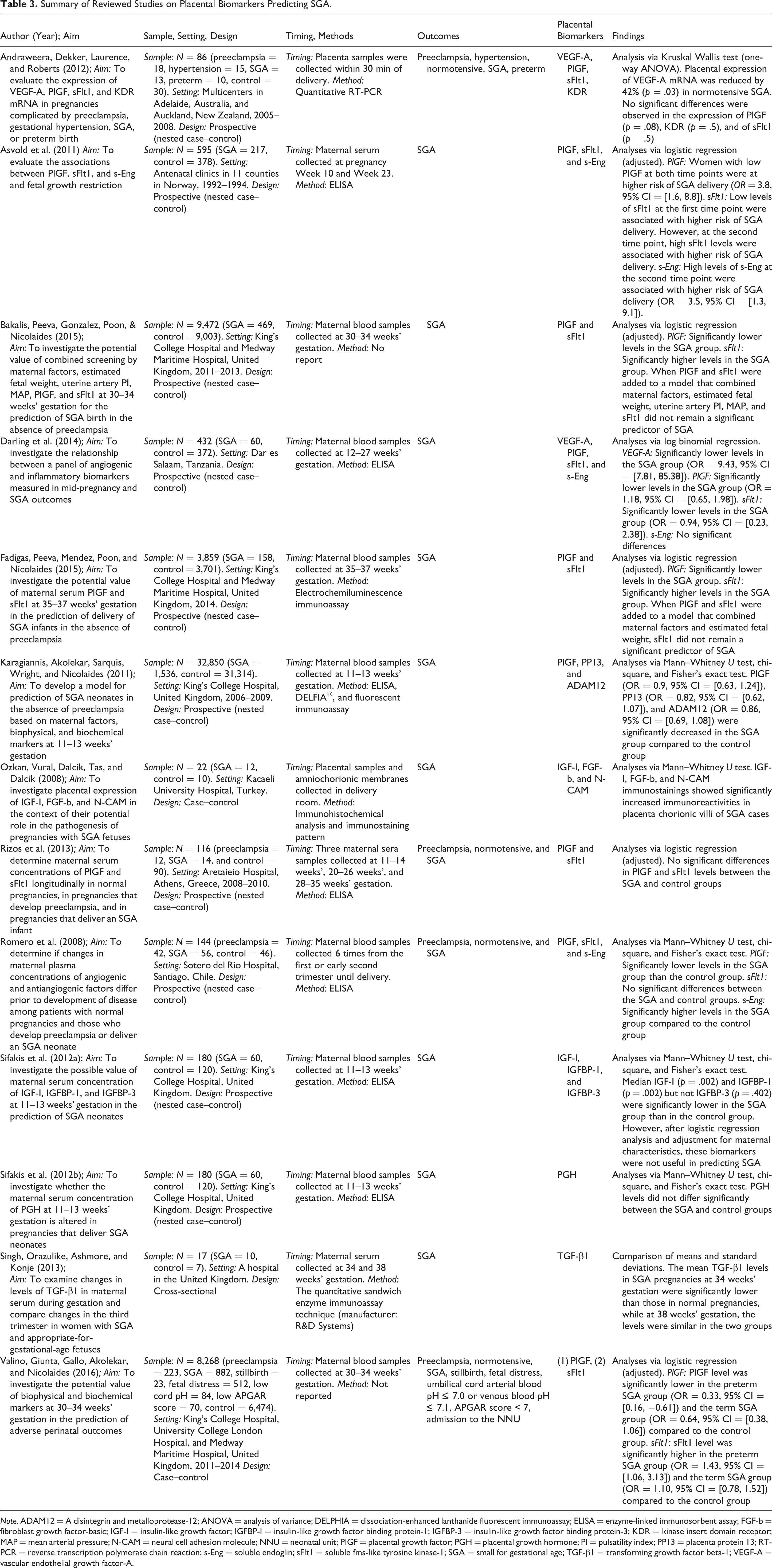
Note. ADAM12 = A disintegrin and metalloprotease-12; ANOVA = analysis of variance; DELPHIA = dissociation-enhanced lanthanide fluorescent immunoassay; ELISA = enzyme-linked immunosorbent assay; FGF-b = fibroblast growth factor-basic; IGF-I = insulin-like growth factor; IGFBP-I = insulin-like growth factor binding protein-1; IGFBP-3 = insulin-like growth factor binding protein-3; KDR = kinase insert domain receptor; MAP = mean arterial pressure; N-CAM = neural cell adhesion molecule; NNU = neonatal unit; PIGF = placental growth factor; PGH = placental growth hormone; PI = pulsatility index; PP13 = placenta protein 13; RT-PCR = reverse transcription polymerase chain reaction; s-Eng = soluble endoglin; sFlt1 = soluble fms-like tyrosine kinase-1; SGA = small for gestational age; TGF-β1 = transforming growth factor beta-1; VEGF-A = vascular endothelial growth factor-A.
Placental Biomarkers
In the reviewed studies, researchers measured biomarkers in maternal serum (11 studies), placental tissues (2 studies), and amniochorionic membranes (1 study; see Table 3). Placental biomarkers that these studies found to be associated with SGA can be divided into angiogenesis-related biomarkers and placental hormone/protein-related biomarkers.
Angiogenesis-related biomarkers
Functional alterations in the placenta are often caused by abnormal development of the placental vascular system, which is the product of vasculogenesis and angiogenesis (Salafia, Charles, & Maas, 2006; Triunfo et al., 2014). Vasculogenesis is responsible for creation of the primary vascular plexus in the placenta, whereas angiogenesis is responsible for creation of blood vessels and their development into a mature placental vascular system (Charnock-Jones et al., 2004). Vasculogenesis occurs in placental villi between Days 21 and 31 of pregnancy, whereas angiogenesis occurs in placental villi from Day 32 until term. Vasculogenesis is a complex process, and investigators have identified few of the factors involved. It is, therefore, less difficult to detect factors involved in angiogenesis.
Investigators have identified the vascular endothelial growth factor (VEGF) family as a regulator of both vasculogenesis and angiogenesis (Arroyo & Winn, 2008; Vrachnis et al., 2013). The VEGF family includes seven proteins: VEGF-A (commonly referred to as VEGF), VEGF-B, VEGF-C, VEGF-D, VEGF-E, VEGF-F, and placental growth factor (PlGF; Vrachnis et al., 2013). The various VEGF proteins bind to two tyrosine kinase receptors, VEGF-1 (flt1) and VEGF-2 (kinase insert domain receptor [KDR]; Neufeld, Cohen, Gengrinovitch, & Poltorak, 1999). In addition to the VEGF family, investigators have identified other placental products as angiogenesis-related factors, including angiopoietins (Ang-1 and Ang-2), transforming growth factor beta-1 (TGF-β1), fibroblast growth factor-basic (FGF-b), and soluble endoglin (s-Eng; Charnock-Jones et al., 2004; Levine et al., 2006; Mayhew et al., 2004).
Of the 13 studies in this review, 9 reported data on PlGF, 8 on soluble fms-like tyrosine kinase-1 (sFlt1), 3 on s-Eng, 2 on VEGF-A, and 1 each on KDR, TGF-β1, and FGF-b (see Table 2). Of the nine studies reporting on PIGF, seven reported that levels were significantly lower in the SGA group than in the appropriate-for-gestational-age (AGA) group, whereas two reported no significant differences. Likewise, three studies reported that sFlt1 levels were significantly higher in the SGA group than in the AGA group, while three others reported no significant differences. In contrast, Darling et al. (2014) reported that sFlt1 levels were significantly lower in the SGA group. Furthermore, Asvold et al. (2011) found that sFlt1 levels were significantly lower in the SGA group than in the AGA group at the first blood sampling (Week 10) but significantly higher in the second sampling (Week 23). For s-Eng, two studies showed higher levels in the SGA group than in the AGA group, and one study showed no significant difference in levels between the groups. In addition, two studies reported that low levels of VEGF-A were associated with higher risk of SGA delivery. Andraweera, Dekker, Laurence, and Roberts (2012) observed no significant differences in the expression of KDR between the SGA and the AGA groups. Moreover, Singh, Orazulike, Ashmore, and Konje (2013) found that the mean TGF-β1 levels in the SGA group were significantly lower than in the AGA group. Finally, Ozkan, Vural, Dalcik, Tas, and Dalcik (2008) found that FGF-b levels were increased in SGA cases (see Table 3).
Placental hormone/protein-related biomarkers
The placenta is an organ that secretes many different hormones and metabolites into maternal blood (Evain-Brion & Malassine, 2003). Placental hormone activities are important in maintaining pregnancy and inducing metabolic adaptations between mother and fetus, whereas placental proteins regulate adaptive maternal–fetal immune response (Blackburn, 2007; Than et al., 2014). The placenta synthesizes various peptide growth factors, which are usually proteins or steroid hormones such as insulin-like growth factor (IGF-I) and PGH (Evain-Brion & Malassine, 2003). These factors regulate cell growth and differentiation, healing, hormone release at the local level, and uterine contractility (Blackburn, 2007).
Of the studies in the present review reporting on the relationship between SGA birth and placental hormones or proteins, two reported data on IGF-I and one each reported on insulin-like growth factor binding protein-1 and -3 (IGFBP-1 and -3), A disintegrin and metalloprotease-12 (ADAM12), placenta protein 13 (PP13), PGH, and neural cell adhesion molecule (N-CAM; see Table 2). Ozkan et al. (2008) reported significantly lower IGF-I levels in an SGA group versus an AGA group. In addition, Sifakis, Akolekar, Kappou, Mantas, and Nicolaides (2012a) found significantly lower IGF-I and IGFBP-1 levels in an SGA group than in an AGA group but no difference in levels of IGFBP-3 between the groups. Karagiannis, Akolekar, Sarquis, Wright, and Nicolaides (2011) found that ADAM12 and PP13 levels were significantly lower in the SGA group. Furthermore, Sifakis, Akolekar, Kappou, Mantas, and Nicolaides (2012b) found that PGH was not significantly associated with SGA delivery. Finally, Ozkan et al. (2008) found that N-CAM levels were increased in SGA cases (see Table 3).
Discussion
Main Findings
In the present systematic review, we found that research has not yet determined a single placental biomarker that reliably predicts SGA, a result similar to the findings of other recent reviews of SGA, IUGR, preeclampsia, stillbirth, and preterm birth (Conde-Agudelo et al., 2013; Heazell et al., 2015; Hui et al., 2012). However, the present review is unique in targeting SGA (apart from preeclampsia, stillbirth, and preterm birth) and placental biomarkers, thus enhancing understanding of how placental function regulates fetal growth.
The generally accepted definition for SGA is a fetus or neonate whose weight is less than the 10th percentile for a specific gestational age (Vayssiere et al., 2015). This definition is not linked to pathology because it includes both constitutionally small and IUGR fetuses/neonates (Wilcox, 2001; Wollmann, 2009). Therefore, when using percentile as a reference standard for categorizing SGA births, it is important that researchers differentiate between constitutionally normal SGA and pathological SGA groups. However, IUGR usually corresponds with SGA that is associated with evidence of abnormal fetal growth confirmed by repeated ultrasound and/or a specific cause can be identified, such as abnormal placental function, toxic effects, or fetal infections (Vayssiere et al., 2015; Wollmann, 2009). Thus, placental biomarkers appear to be more clearly associated with pathological SGA (IUGR) than constitutionally normal SGA.
Moreover, the inconsistent results we evaluated in the present review suggest low reliability of placental biomarkers, which could be attributable to the multifactorial nature of SGA. SGA has many causes, including maternal, fetal, and placental factors (Wollmann, 2009). The limited clinical ability to identify reliable placental biomarkers is thus understandable. Moreover, some of the placental biomarkers covered in this review appeared only in a single study, including KDR, IGFBP-1, IGFBP-3, ADAM12, PP13, PGH, TGF-β1, FGF-b, and N-CAM (see Table 2). Therefore, the studies of the ability of placental biomarkers to predict SGA infants are still too small in scope and number to draw conclusions, and further research on these biomarkers is warranted.
The placental biomarkers most commonly reported in the 13 studies were PlGF and sFlt1. This prevalence is likely due to their major roles in the establishment and maturation of the vascular system of the human placenta (Vrachnis et al., 2013), which is the product of two processes, vasculogenesis and angiogenesis. Researchers have hypothesized that low concentrations of PlGF and high concentrations of sFlt1 are associated with impaired angiogenesis and placental development, leading to pregnancy complications such as preeclampsia and SGA (Arroyo & Winn, 2008). Most of the studies in the present review support this hypothesis (see Table 3). However, some studies reported contradictory findings. For example, Andraweera et al. (2012) and Rizos et al. (2013) found no significant differences in PlGF levels between SGA and AGA groups. Moreover, Andraweera et al. (2012), Rizos et al. (2013), and Romero et al. (2008) found no significant differences in the sFlt1 levels between SGA and AGA groups. These contradictory findings may be the result of differences in sampling times or frequencies, laboratory methods, or statistical analyses; Table 3 shows the variety of approaches used in the studies. The predictive accuracy of PlGF and sFlt1 thus remains unclear, and further research is required to confirm their value in predicting SGA.
Strengths and Limitations
This systematic review involved a comprehensive examination of the literature on SGA currently available, rigorous assessment of the quality of the studies, and reporting on a wide range of placental biomarkers. Nevertheless, the review has some limitations, which are similar to those of other systematic reviews on maternal serum biomarkers and biomarkers of IUGR (Conde-Agudelo et al., 2013; Hui et al., 2012). First, the heterogeneity of the placental biomarkers and procedures used to examine them made the comparison of studies challenging. Second, not all studies reported the procedures and techniques researchers used to examine biomarkers, and most studies did not report whether they masked laboratory technicians to pregnancy outcomes and clinicians to test results. Therefore, the predictive accuracy reported for a given placental biomarkers may be biased. Third, we included only studies published in English, and there may well be studies published in other languages that could shed further light on placental biomarkers. Fourth, there are many causes of SGA, including maternal, fetal, and placental factors (Zabransky, 2013); thus, studies that examine only placental biomarkers, excluding maternal and fetal factors, may be too limited in identifying reliable predictors of SGA infants. Finally, the adverse pregnancy outcomes of some studies included in this review were not independent of one another. For example, authors reported coexisting adverse outcomes such as preeclampsia and SGA. It is possible that these were competitive outcomes that decreased the apparent predictive ability and accuracy of placental biomarkers for SGA alone.
Implications for Future Research
Several placental biomarkers for predicting SGA (see Table 2) have been too little investigated to draw meaningful conclusions about their value. We found that PlGF and sFlt1 were the most commonly examined placental biomarkers, but their predictive accuracy and reliability for SGA remain unclear. Additional research is warranted to further explore and confirm the relationships between these placental biomarkers and SGA.
Further research should also be performed to determine the best combinations of tests for predicting SGA (e.g., placental biomarkers plus uterine artery Doppler and associated maternal, fetal, and placental factors). Some investigators have, in fact, recently reported on the accuracy of combined tests for predicting SGA (Bakalis, Peeva, Gonzalez, Poon, & Nicolaides, 2015; Karagiannis et al., 2011; Valino, Giunta, Gallo, Akolekar, & Nicolaides, 2016). For example, Bakalis, Peeva, Gonzalez, Poon, and Nicolaides (2015) developed a screening instrument combining maternal factors, estimated fetal weight, uterine pulsatility index, mean arterial pressure, PlGF, and sFlt1 at 30–34 weeks of gestation for prediction of SGA. They reported that combined screening at a 10% false-positive rate predicted 89%, 94%, and 96% of SGA deliveries at 32–36 weeks of gestation with birth weights of <10th, <5th, and <3rd percentiles, respectively; moreover, the combined screening predicted 57%, 65%, and 72% of SGA deliveries at ≥37 weeks at the respective percentiles. Combined screening for maternal, biophysical, and biochemical factors could thus potentially identify a high proportion of pregnancies that will deliver SGA neonates. Further screening intervention studies are needed to determine whether these combined screenings produce results that can be used to improve pregnancy outcomes.
At the same time, the current revolution in genetic knowledge has markedly challenged and altered our understanding of health and disease. Therefore, researchers should also give more attention to studying associations between genetic markers and SGA in order to better understand the molecular mechanisms underlying fetal growth and development. Research findings in this area will be critical for developing screening and treatment procedures to prevent adverse pregnancy outcomes such as SGA (Ilekis et al., 2016).
Finally, there is an opportunity to link placental biomarkers and associated birth outcomes to long-term developmental processes and adult health (Rutherford, 2013). Future research should evaluate the predictive value of placental biomarkers related to neonatal outcomes such as stillbirth, neonatal death, preterm birth, neonatal intensive care unit admission, fetal abnormality, and serious neonatal health outcomes (e.g., necrotizing enterocolitis, chronic lung disease, intraventricular hemorrhage, sepsis, and seizure) as well as long-term health outcomes in childhood and adulthood (Heazell et al., 2015). In particular, researchers should give greater attention to studying these relationships in developing countries where SGA is a major public health problem. Improved understanding of the potential relationship between placental biomarkers and adverse neonatal health outcomes may help to decrease risks of neonatal mortality and morbidity as well as risks of adverse health outcomes throughout the life span.
Conclusion
It is vital that researchers continue to seek to increase our understanding of the relationship of placental biological processes to SGA and fetal growth. Such research will deepen our understanding of the normal physiology of fetal development, give clinicians the opportunity to screen pregnant women with valid placental biomarkers, and expand our arsenal of safe and effective treatments for SGA fetuses during pregnancy.
Footnotes
Authors’ Note
Ruchob, Rutherford, and Bell contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy.
This article was completed while Rungnapa Ruchob was a doctoral student at the University of Illinois at Chicago.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.