
Abstract
Background:
Mood disturbances are implicated in the pathogenesis of fibromyalgia. The aim of this study was to assess the effect of different doses of melatonin on quality of life, mood status, pain, anxiety, and urinary cortisol levels in patients with fibromyalgia.
Methods:
After a 10-day baseline period for the collection of data about participants’ initial status, participants took different doses of melatonin for 10 consecutive days each, with placebo given during the 10 days either before or between melatonin doses. Participants’ moods, quality of life, and pain levels were assessed using the Fibromyalgia Impact Questionnaire (FIQ), a Numerical Pain Scale (NPS), the State-Trait Anxiety Test (STAI), a Visual Analog Scale (VAS), and the Short Form-36 Health Survey (SF-36). Urinary cortisol levels were measured using enzyme-linked immunoassay.
Results:
Doses of 9, 12, and 15 mg of melatonin were associated with decreases in the total score of the FIQ, NPS scores, and urinary cortisol levels. The State-Anxiety subscale of the STAI improved after the 12 mg dose. The scores on the VAS improved after the 9 mg dose. The dimensions evaluated in the SF-36 questionnaire improved after the 9 mg dose.
Conclusion:
Melatonin improved mood, anxiety levels, and quality of life while decreasing cortisol levels in patients with fibromyalgia.
Fibromyalgia (FM) is a chronic widespread pain syndrome that is accompanied by fatigue, sleep disturbances, anxiety, depression, lack of concentration, and neurocognitive impairment (Giacomelli et al., 2013). The worldwide prevalence of FM is 3–6% (Gonzalez, del Teso Rubio, Paniagua, Criado-Alvarez, & Holgado, 2015), with women making up the large majority (90%) of cases (Wilhelmsen, Amirian, Reiter, Rosenberg, & Gögenur, 2011), with a male-to-female ratio of 1:6–10 (Gonzalez et al., 2015).
Studies have shown both a blunted morning serum cortisol level and an elevated evening serum cortisol concentration in FM patients (Korszun, 2000; Mahdi, Fatima, Das, & Verma, 2011; McLean et al., 2005). Cortisol is considered one of the most important biomarkers of stress. Altered functioning of the hypothalamic–pituitary–adrenal (HPA) axis produces a change in the circadian rhythm of cortisol. Patients with FM also present low levels of circulatory tryptophan, serotonin, and melatonin (Cordero et al., 2010; Hussain, Al-Khalifa, Jasim, & Gorial, 2011; Mahdi et al., 2011). These molecules act as antioxidants, possess anti-inflammatory properties, and are linked to pain modulation and mood status, among other crucial physiological functions (Danilov & Kurganova, 2016). Some authors have proposed that the etiology of the chronic pain affecting patients with FM is more related to pain-processing mechanisms at the level of the central nervous system than to musculoskeletal disorders (Hussain et al., 2011).
Clinical and experimental studies have demonstrated the favorable anxiolytic and analgesic properties of melatonin in the treatment of diseases with pronounced chronic pain (Wilhelmsen et al., 2011), sleep (Castaño et al., 2018; Guerrero, Carrillo-Vico, & Lardone, 2007), and mood disturbances (Reiter, 2003). Accordingly, the use of melatonin in the treatment of FM is not a novel idea (Acuña-Castroviejo, Escames, & Reiter, 2006; Citera et al., 2000; Hussain et al., 2011). FM has been associated with psychological and psychiatric disorders, most often with anxiety and depression (Revuelta, Segura, & Tevar, 2010). There is a strong association, more generally, between chronic pain disturbances and alterations in mood status (Bair, Robinson, Katon, & Kroenke, 2003). Therefore, the aim of this study was to evaluate the effects of the administration of progressively increasing doses of melatonin (3, 6, 9, 12, and 15 mg) on quality of life, general mood status, pain, anxiety, and cortisol levels in patients with severe FM (Wolfe et al., 2010), that is, patients who scored greater than 70 on the Fibromyalgia Impact Questionnaire (FIQ).
Material and Methods
Participants
We initially recruited 97 patients with FM for the present study, 36 of whom met inclusion criteria and were finally enrolled in the study. Included as participants were women diagnosed with FM using the American College of Rheumatology guidelines (Wolfe et al., 2010), aged 40–60 years, who had a medium socioeconomic status and a total score on the FIQ < 70. Moreover, none of the participants were involved in physical/psychological therapies. A total of three participants dropped out during the course of the study due to family-related matters and lack of adherence to the protocol. All participants maintained their lifestyle habits related to medication, diet, sleep, and exercise throughout the study. We recruited participants from the pool of patients referred to the Internal Medicine Service (outpatient department) at Servicio Extremeño de Salud (Badajoz, Spain) and collected data from October to March across 3 consecutive years (2013–2015).
Both the Ethical Committee of the University of Extremadura (Badajoz, Spain) and the Ethical Committee of Servicio Extremeño de Salud approved the study, and the protocol adhered to the Declaration of Helsinki, the Council of Europe, and the Universal Declaration of United Nations Educational, Scientific, and Cultural Organization on human rights, biomedicine, and human genome. We obtained written informed consent from all participants.
Experimental Design
The study had a longitudinal placebo-controlled design with a 10-day baseline period, followed by an initial 10-day placebo period, and five melatonin-administration periods of 10 days each, separated by washout periods (10 days each) during which patients were treated with placebo, for a total duration of 110 days. All patients took the same doses of quick-release, plant-derived melatonin in a sequential pattern of increasing doses (Guinama, Puebla de Vallbona, Spain; 3, 6, 9, 12, 15 mg/day). Each dose was taken as a single pill (containing pure melatonin) at night, 30 min before going to bed, during 10 consecutive days. During the placebo and washout periods, participants took a placebo (a pill containing rice starch) at night (1 pill/day) for 10 consecutive days. Patients visited the Department of Physiology at the University of Extremadura in Badajoz, Spain, at baseline and every 10 days to complete study measures and pick up the next 10 days of treatment (either melatonin or placebo). The timing of collection of each of the outcome measures is shown in Table 1.
Experimental Design.
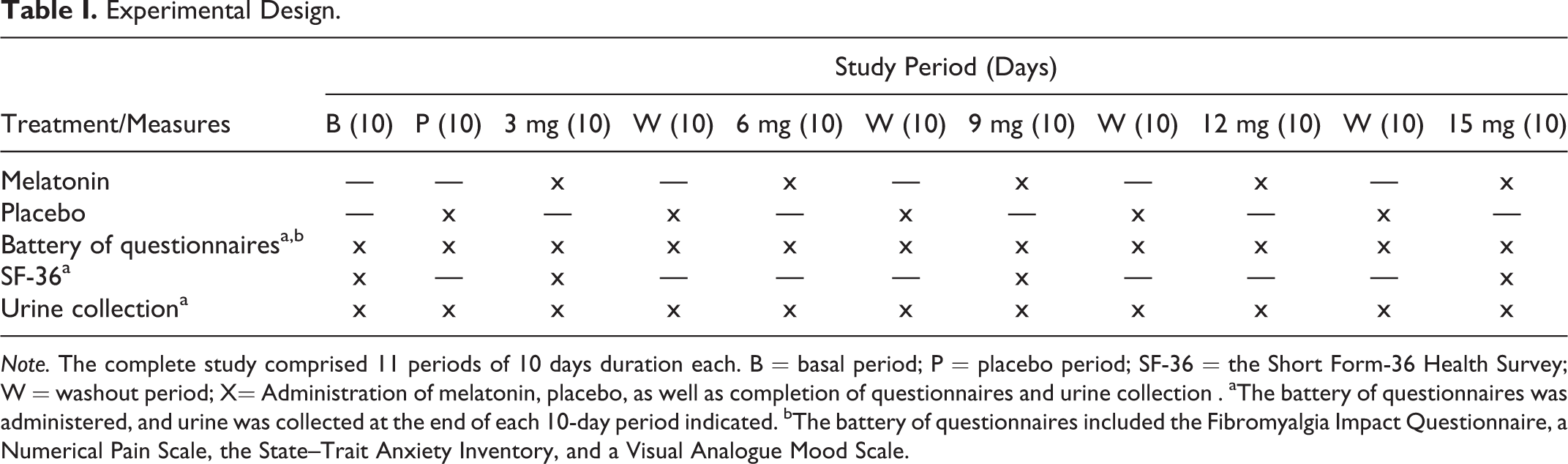
Note. The complete study comprised 11 periods of 10 days duration each. B = basal period; P = placebo period; SF-36 = the Short Form-36 Health Survey; W = washout period; X= Administration of melatonin, placebo, as well as completion of questionnaires and urine collection . aThe battery of questionnaires was administered, and urine was collected at the end of each 10-day period indicated. bThe battery of questionnaires included the Fibromyalgia Impact Questionnaire, a Numerical Pain Scale, the State–Trait Anxiety Inventory, and a Visual Analogue Mood Scale.
Measures
At the end of each 10-day study period, we had patients complete a battery of self-report questionnaires to evaluate physical and psychological symptoms, pain levels, and mood state. These questionnaires included validated Spanish-language versions of the FIQ, a Numerical Pain Scale (NPS), the State–Trait Anxiety Inventory (STAI), and a Visual Analogue Mood Scale (VAS). We also had participants provide a urine sample for cortisol measurement at the end of each period. At baseline and at the end of the treatment periods for 3 mg, 9 mg, and 15 mg of melatonin, we had participants complete the Short Form-36 Health Survey (SF-36) to evaluate the effect of a low, medium, and high doses, respectively, on health-related quality of life.
FIQ
The FIQ is a disease-specific instrument (Burckhardt, Clark, & Bennett, 1991) that comprises 10 subscales of disabilities and symptoms. The first item contains 10 subitems related to the ability to perform large-muscle tasks, with each subitem rated on a 4-point Likert-type scale. Items 2 and 3 ask the patient to mark the number of days they felt well and the number of days they were unable to work (including housework) because of FM symptoms. Items 4 through 10 are horizontal linear scales marked with 10 increments on which the patient rates work difficulty, pain, fatigue, morning tiredness, stiffness, anxiety, and depression. The global score has a range from 0 to 100, with higher scores representing a poorer quality of life. Patients with scores below 50 are considered to have mild FM, those with scores between 50 and 70 have moderate FM, and those with scores greater than 70 have severe FM (Burckhardt et al., 1991; Monterde, Salvat, Montull, & Fernández-Ballart, 2004).
NPS
The NPS is a segmented numeric version of a Visual Analogue Scale in which the patient selects a number (from 0 to 10) that best reflects the intensity of their pain. This scale has only 1 item, in the form of 10-cm horizontal line with equal segments numbered from 1 to 10, where 0 is the absence of pain and 10 represents the worst pain imaginable. Patients select the number that best represents the intensity of their pain (Hawker, Mian, Kendzerska, & French, 2011).
STAI
The STAI assesses state and trait anxiety through 20 items on each of the two scales, with a Likert-type response including four options. In the case of state anxiety, the scale ranges from 0 (none) to 3 (a lot), while the Trait-Anxiety Scale ranges from 0 (almost never) to 3 (almost always). In both the state and Trait-Anxiety Scales, some of the items are inverted and assess well-being or the absence of anxiety, while the rest of the items refer to the presence of anxiety. The total score is obtained by summing the items after the inversion of those that are drafted positively. Total scores range between 0 and 60, with higher scores indicating more anxiety (Guillén-Riquelme & Buela-Casal, 2015).
VAS
VASs have been found to be an effective tool for measuring changes over time in response to treatment for symptoms of mood disturbance, and their reliability and validity have been well-documented (McCormack, David, & Sheather, 1988). In the present study, the VAS was a 100-mm horizontal line with anchors placed at both poles that indicated antithetic conditions (the descriptors ranged from very bad at 0 mm to very good at 100 mm; Burckhardt & Jones, 2003). We used four such scales to measure the participants’ general mood status in terms of family relationships, social relations, frame of mind, and fitness.
The SF-36
The SF-36 is a generic instrument for assessing health-related quality of life. It includes 36 items that capture an 8-scale profile of scores: physical functioning, social functioning, role physical, role emotional, vitality, bodily pain, mental health, and general health. The scores for the individual domains are derived from the SF-36 Health Survey Manual and Interpretation Guide and are summed to give an overall score ranging from 0 to 100, such that the higher this score, the better the patient’s function (Alonso et al., 1998; Vilagut et al., 2005).
Determination of urinary cortisol levels
We collected first-voided morning urine samples at the end of each period and stored them at −80°C until biochemical assay. We quantified cortisol levels using a commercial enzyme-linked immunosorbent assay kit (DRG® Urinary Cortisol [EIA-2989], Springfield, Illinois) according to the manufacturer’s instructions. Samples were run in duplicate. The intra- and interassay coefficients of variation (CV) of this assay were 6.4% and 4.37%, respectively. To adjust for variation in the dilution of urine, we expressed cortisol levels as urinary cortisol/urine creatinine ratio. Creatinine concentration was determined by means of the Jaffe test, a colorimetric method used to determine creatinine levels in blood and urine. By means of Jaffe’s reaction, creatinine produces an orange color with picric acid in alkaline medium. The quantified color change that occurs is directly proportional to the concentration of creatinine in blood in urine (Klante, Brinschwitz, Secci, Wollnik, & Steinlechner, 1997; Toora &Rajagopal, 2002).
Statistical Analysis
We used the Kruskal–Wallis (nonparametric) test for analysis of independent groups. Values are presented as mean ± standard error of the mean of the number of determinations. The degree of significance was set at p < .05, and all analyses were performed using the statistical package GraphPad Prism (version 5.0, 2007; GraphPad Software, Inc., San Diego, CA).
Results
In general, the administration of melatonin improved mood and quality of life and reduced anxiety levels in patients with FM. The intake of melatonin produced a significant decrease (p < .05) in the FIQ total score relative to both the baseline and initial placebo periods (Figure 1).
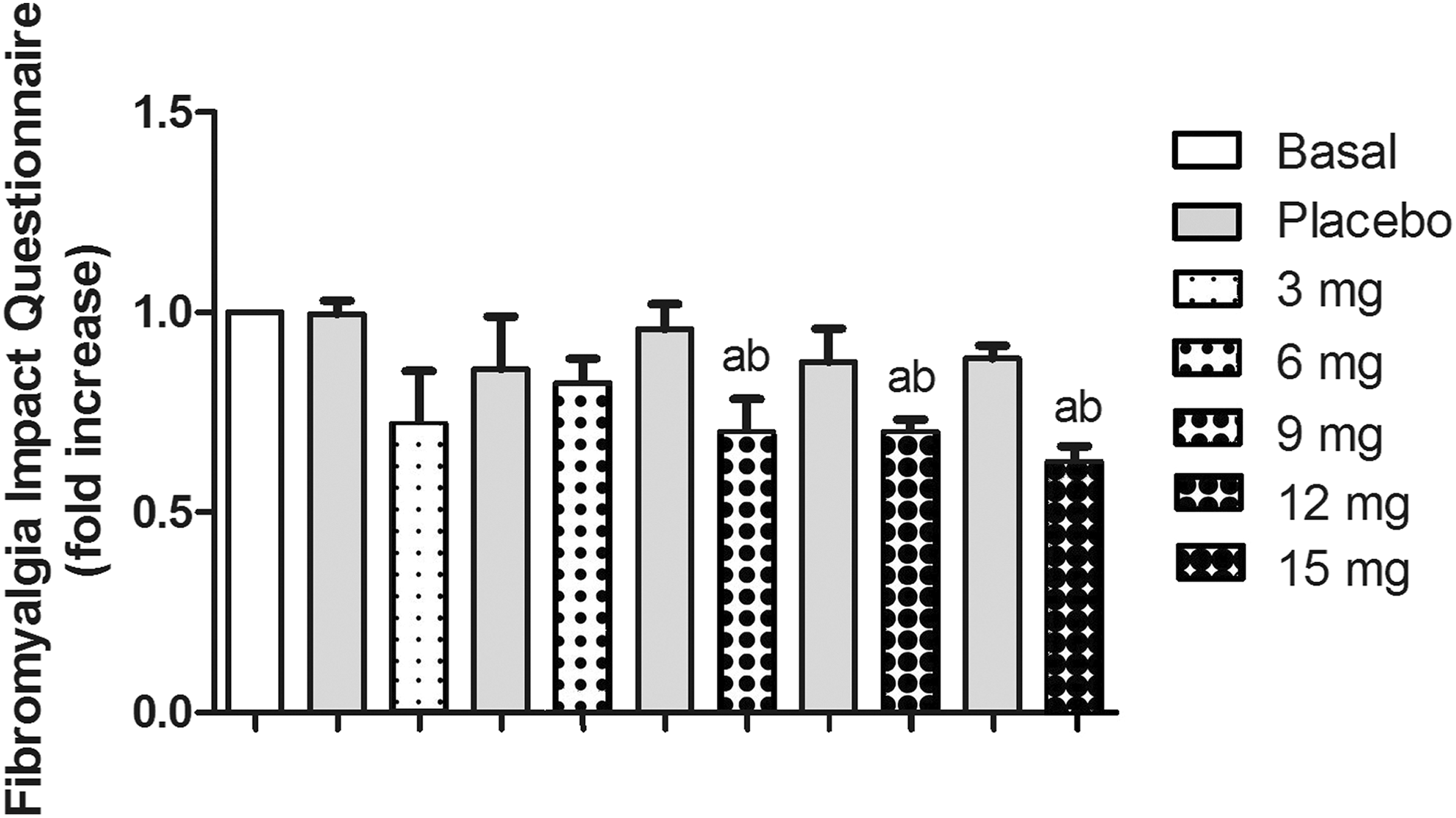
Effect of the administration of different doses of melatonin (3, 6, 9, 12, 15 mg/day for periods of 10 days each) on Fibromyalgia Impact Questionnaire total score. Bars indicate mean fold change in scores from baseline ± standard error of the mean from 33 participants. a p < .05 with respect to the baseline value; b p < .05 with respect to the initial placebo condition.
Specifically, doses of 9, 12, and 15 mg/day of melatonin produced a significant decrease (p < .05) in pain levels measured by the NPS with respect to baseline and the initial placebo period (Figure 2). Doses of 12 and 15 mg of melatonin/day caused a significant decrease (p < .05) in state anxiety on the STAI with respect to baseline and placebo periods (Figure 3A) in a dose-dependent manner. Although we observed slight decreases in the Trait-Anxiety subscale score (Figure 3B) after 12 and 15 mg of melatonin/day, these decreases did not reach statistical significance. Figure 4 shows change in scores on VAS for mood status for the dimensions of family relationship (Figure 4A), social relations (Figure 4B), frame of mind (Figure 4C), and fitness (Figure 4D) domains. The mean score for the family relations dimension improved significantly (p < .05) with the 9 mg of melatonin/day, with respect to baseline, placebo periods, and 3 mg of melatonin/day. We observed a slight dose-dependent increase in the mean score for the social relations dimension, but these values did not reach significance. For the dimension of frame of mind, we observed a dose-dependent effect that became significant with respect to baseline and placebo values only after the administration of 12 and 15 mg/day. Regarding the fitness dimension, doses of 9 mg, 12 mg, and 15 mg of melatonin produced significant changes (p < .05) with respect to both baseline and placebo periods.
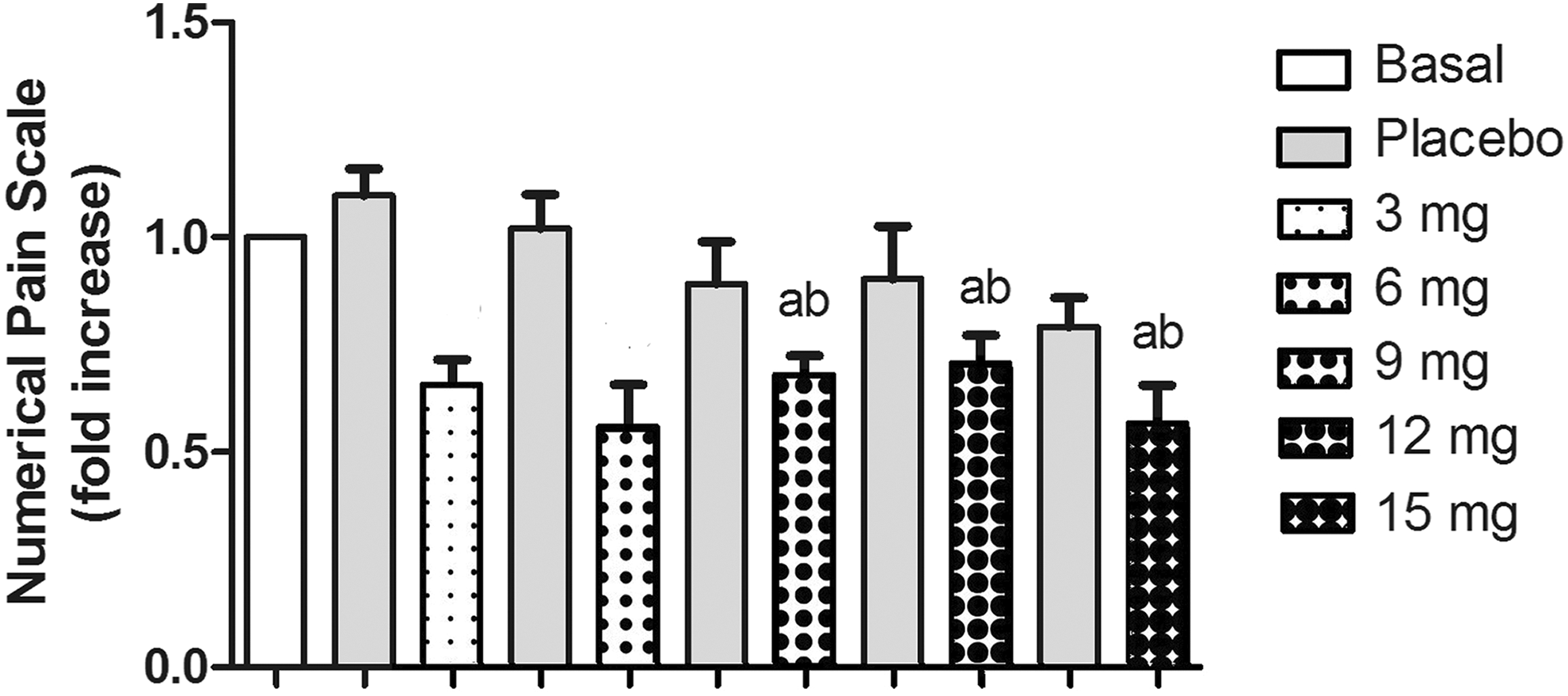
Effect of the administration of different doses of melatonin (3, 6, 9, 12, 15 mg/day for periods of 10 days each) on the Numerical Pain Scale. Bars indicate mean fold change in scores from baseline ± standard error of the mean from 33 participants. a p < .05 with respect to the baseline value; b p < .05 with respect to the initial placebo condition.
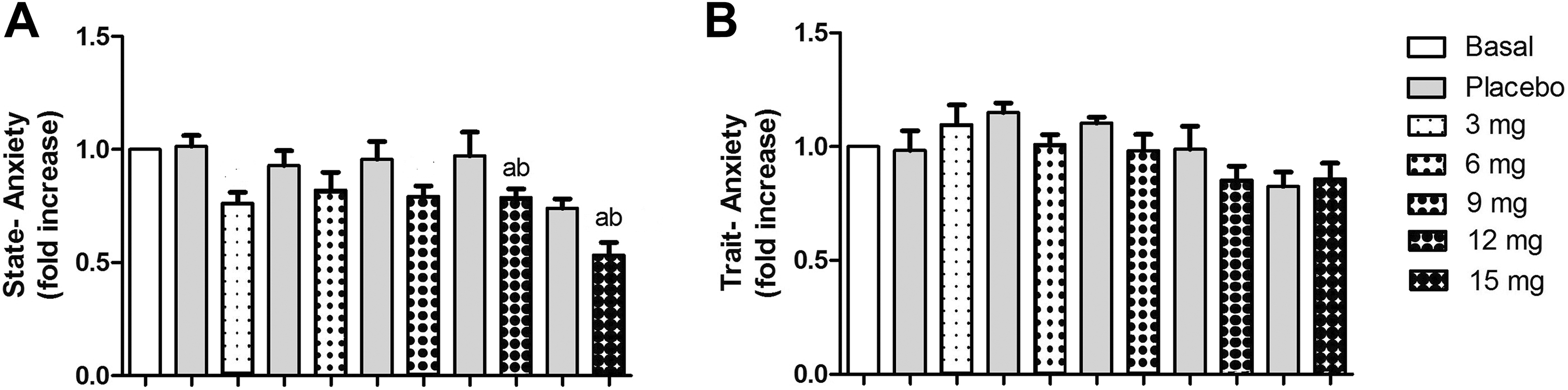
Effect of the administration of different doses of melatonin (3, 6, 9, 12, 15 mg/day for periods of 10 days each) on state–trait Anxiety Inventory (STAI) scores. (A) State–anxiety subscale, (B) Trait–Anxiety subscale. Bars indicate mean fold change in scores from baseline ± standard error of the mean from 33 participants. a p < .05 with respect to the baseline value, b p < .05 with respect to the initial placebo condition.
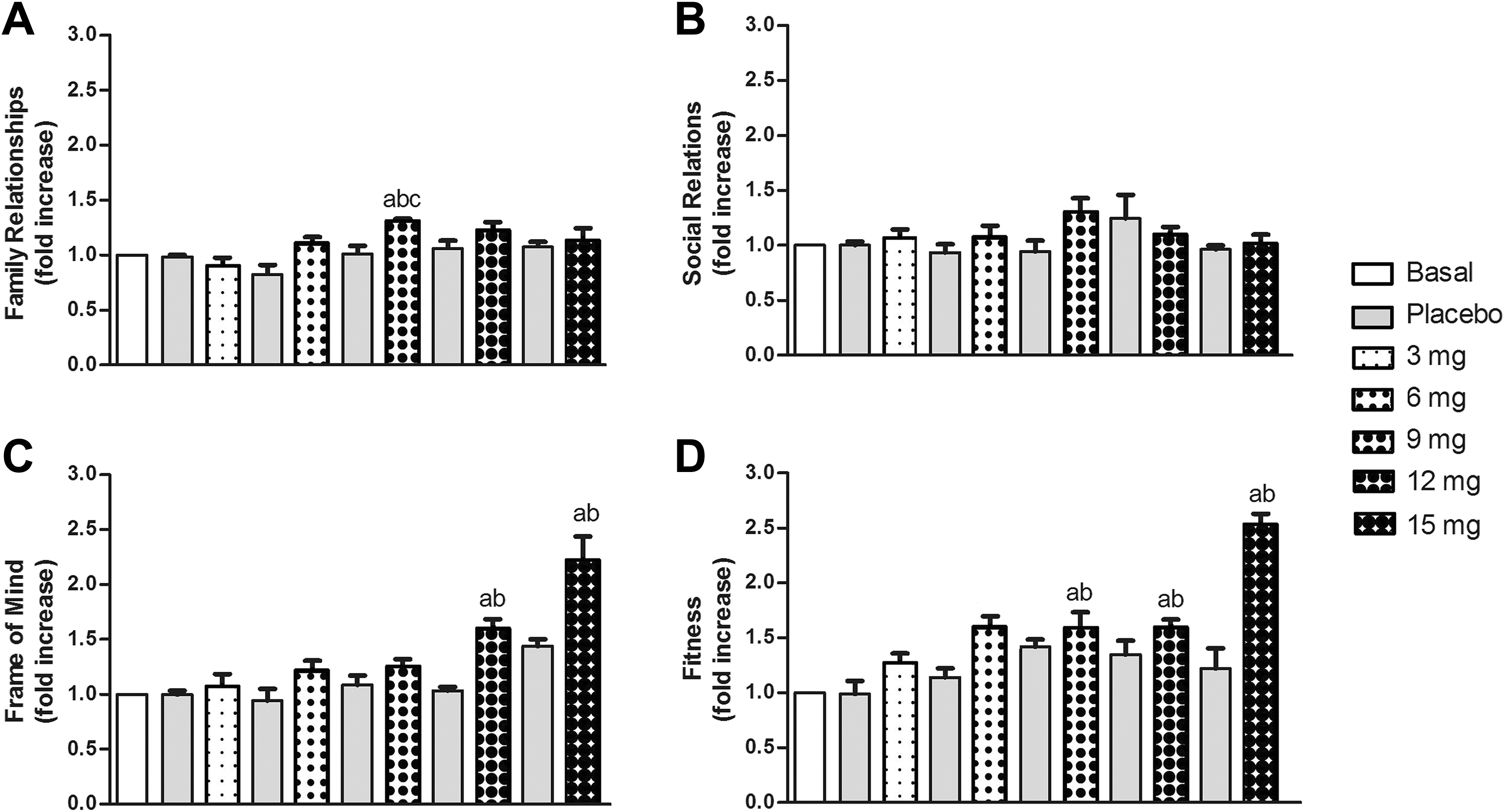
Effect of the administration of different doses of melatonin (3, 6, 9, 12, 15 mg/day for periods of 10 days each) on the visual analogue mood scale for (A) family relationships, (B) social relations, (C) frame of mind, and (D) fitness. Bars indicate mean fold change in scores from baseline ± standard error of the mean from 33 participants. a p < .05 with respect to the baseline value, b p < .05 with respect to the initial placebo condition, c p < 0.05 with respect to 3 mg dose.
Figure 5 shows the changes in the scores on the SF-36, which measures health-related quality of life via subscales for physical functioning (Figure 5A), social functioning (Figure 5B), role physical (Figure 5C), role emotional (Figure 5D), vitality (Figure 5E), bodily pain (Figure 5F), mental health (Figure 5G), and general health (Figure 5H). Scores for all subscales showed significant changes (p < .05). For physical functioning, there were significant changes from baseline with doses of 9 and 15 mg of melatonin/day (p < .05). For social functioning, role physical, and role emotional, scores differed significantly between doses of 15 mg of melatonin/day and both baseline and 3 mg/day of melatonin. For both social functioning and role emotional, scores at 15 mg/day also differed significantly from those at 9 mg of melatonin/day. Lower doses of melatonin were associated with significant changes in scores for the remainder of the domains. For vitality and general health, doses of 9 mg and 15 mg of melatonin/day were associated with significantly different scores (p < .05) with respect to baseline and 3 mg/day of melatonin. At a dose of 9 mg/day of melatonin, scores on the Mental Health subscale improved significantly (p < .05) with respect to baseline, and at a dose of 15 mg/day, scores on this subscale improved significantly (p < .05) with respect to both baseline and a 3 mg/day dose of melatonin. At doses of 9 and 15 mg melatonin/day, scores on the Bodily Pain subscale improved significantly with respect to baseline and 3 mg/day of melatonin, and furthermore, the score at a dose of 15 mg/day of melatonin also differed significantly with that at 9 mg/day of melatonin.
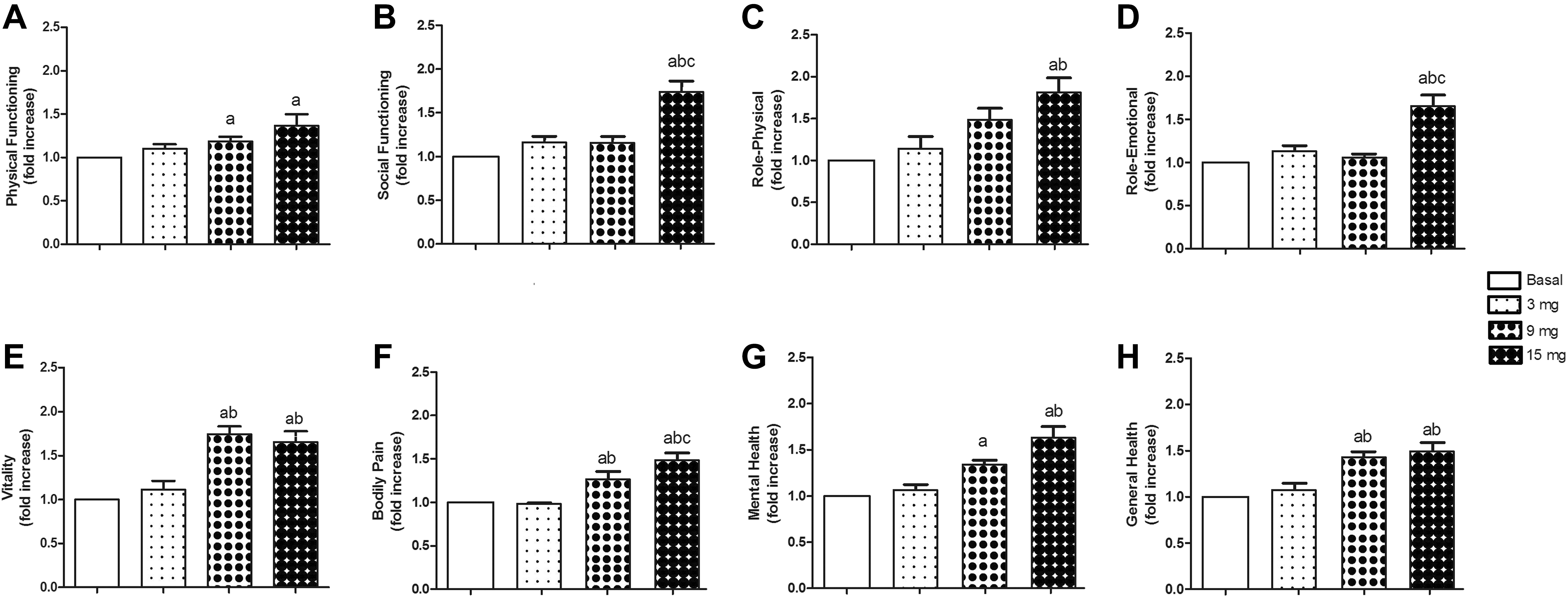
Effect of the administration of different doses of melatonin (3, 9, and 15 mg/day for periods of 10 days each) on the Short Form-36 Health Survey (SF-36) subscales of (A) Physical functioning, (B) social functioning, (C) role physical, (D) role emotional, (E) vitality, (F) bodily pain, (G) mental health, and (H) general health. Bars indicate mean fold change in scores from baseline ± standard error of the mean from 33 participants. a p < .05 with respect to the baseline value, b p < .05 with respect to 3 mg dose, c p < .05 with respect to 9 mg dose.
Urinary cortisol levels decreased with administration of 6, 9, 12, and 15 mg/day of melatonin (Figure 6), but these changes were only significant with respect to baseline and placebo conditions at doses of 9, 12, and 15 mg of melatonin.
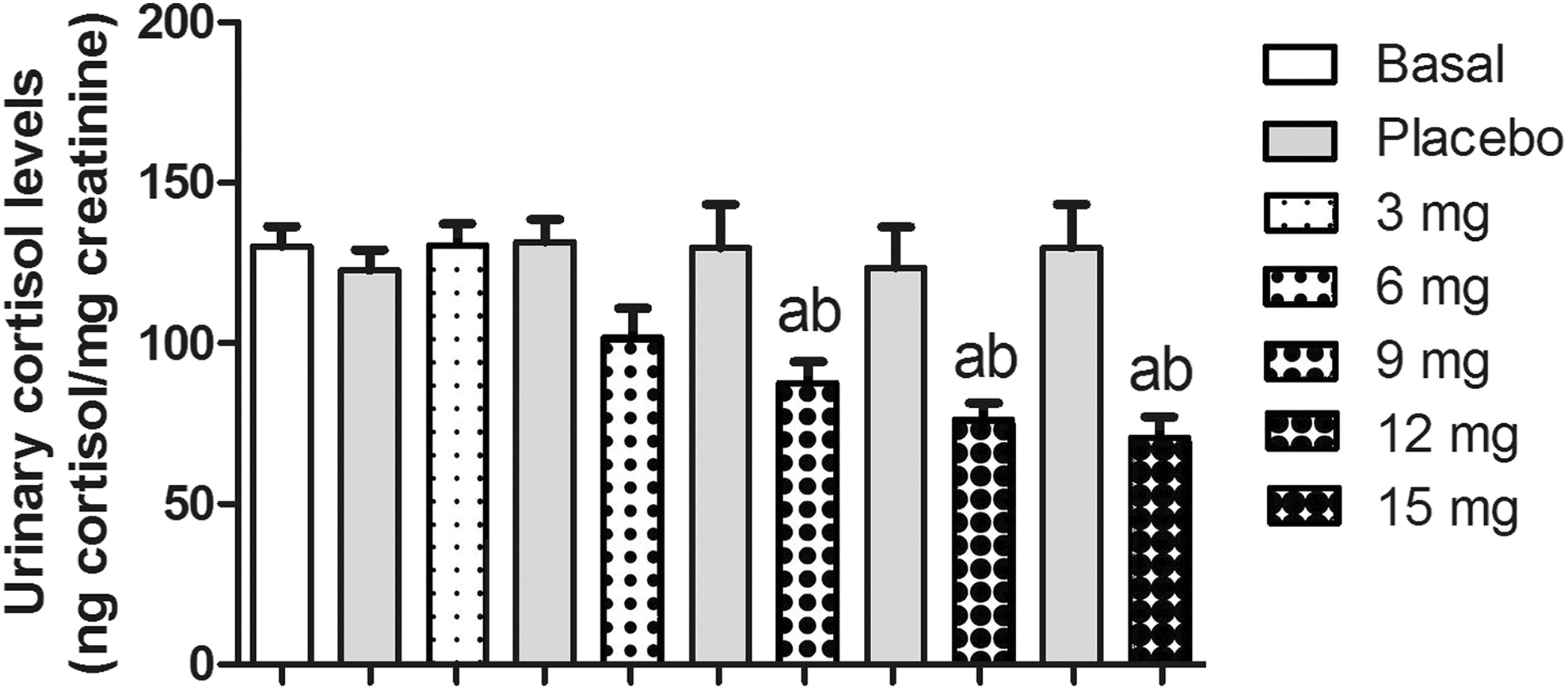
Effect of the administration of different doses of melatonin (3, 6, 9, 12, 15 mg/day for periods of 10 days each) on urinary cortisol levels. Bars indicate mean levels ± standard error of the mean from 33 participants. a p < .05 with respect to the baseline value, b p < .05 with respect to the initial placebo condition.
Discussion
The complexity of FM syndrome hampers the efficacy of treatment. In fact, there are no specific treatments for alleviating/combating this syndrome, and the main drugs prescribed are analgesics, sleep inducers, and anxiolytics, which are primarily used to address the most characteristic symptoms of FM such as pain, sleep disturbances, and anxiety (Hussain et al., 2011).
Research has shown that there are disturbances in the normal secretion pattern of cortisol in patients with FM (Mahdi et al., 2011). Studies have also revealed alterations in the circadian rhythm of melatonin in these patients (Chen, Zhang, & Huang, 2016). Others have reported that the intake of melatonin improves pain, fatigue, and depressive symptoms in FM patients (De Zanette et al., 2014; Wilhelmsen et al., 2011).
Several pieces of evidence demonstrate the relationship between melatonin and cortisol. Research has shown that acute stress triggers a biological stress adaptation response whereby the availability of cerebral serotonin (a precursor of melatonin) is increased, which promotes a negative feedback mechanism in the HPA axis to control cortisol levels (Van Praag et al., 2004). However, chronic stress reduces serotonin levels in the synaptic cleft and stimulates neuronal reuptake of the same, which can cause HPA-axis hyperactivity and the onset of affective disorders related to stress. Finally, melatonin exerts an inhibitory effect on the secretion of cortisol (Torres-Farfan et al., 2003), indicating that there is an inverse relationship between circadian cortisol and melatonin rhythms (Reiter et al., 2008).
Several studies have demonstrated an interaction between the pineal gland and the HPA axis, and hence between the rhythms of cortisol and melatonin (Korszun, 2000). The decrease in urinary cortisol levels we observed in the present study could, therefore, be due to the intake of the different doses of melatonin. The concentration of cortisol in first-void morning urine reflects the circulating levels of the previous night. The intake of melatonin thus likely decreased circulating cortisol during the night, indicating that melatonin treatment was beneficial for these patients.
In addition, melatonin and cortisol are both involved in mood regulation, pain modulation, and reduction in anxiety (Danilov & Kurganova, 2016; Fischer et al., 2016; McLean et al., 2005). Serotonin (a precursor of melatonin, as mentioned above) is an important modulator of pain and mood perception. Lower levels of serotonin have been correlated with painful points and depression, as well as high scores on the FIQ, in patients with FM (Cordero et al., 2010). It is thus likely that the positive effects on mood we observed in the present study in patients with FM could be attributed, at least in part, to the intake of melatonin.
Indeed, our results are in accord with those of several authors who have also demonstrated the beneficial effects of melatonin administration on the quality of life of patients with FM, as ascertained by FIQ scores and the different subscales of the SF-36. In the present study, we used both the SF-36 and FIQ to measure the quality of life in our participants. The FIQ is a disease-specific instrument (Burckhardt et al., 1991), while the SF-36 is a generic instrument for assessing health-related quality of life in the general population. Previous researchers have also used the SF-36 in patients with FM to measure their health status and quality of life (Birtane, Uzunca, Taştekin, & Tuna, 2007; Hoffman & Dukes, 2008; Salaffi et al., 2009).
Several studies have shown improvement in FIQ scores after the administration of melatonin (Citera et al. 2000; Hussain et al., 2011). De Zannete and coauthors (2014) reported that 10 mg of melatonin/day during 6 weeks improved FIQ scores in patients with FM. Others (Hussain et al., 2011) found significant decreases in total FIQ score after the intake of lower doses of melatonin, for example, 5 mg of melatonin/day, but longer periods of administration (8 weeks) were needed to produce this change. In the present study, we observed beneficial effects of melatonin in a short period of time with the higher doses (10 days for each dose). However, we did observe slight dose-dependent improvements in some variables with lower doses, though these changes were not statistically significant. If we had been administered the daily doses for a longer period, we might have observed significant changes at the lower doses.
Chronic pain is one of the main symptoms of FM syndrome (De Zanette et al., 2014). Our results in the present study show a significant decrease in pain levels after the higher doses of melatonin for 10-day periods. With lower doses, there was a trend toward improvement in pain levels, but these changes did not reach statistical significance. The analgesic properties of melatonin are well-documented (Citera et al., 2000; Danilov & Kurganova, 2016; Hussain et al., 2011; Wilhelmsen et al., 2011). Prior studies have also demonstrated the analgesic effects of melatonin in FM patients, but these involved longer periods of treatment to achieve such effects. Specifically, studies reported pain reduction with 3 mg/day for 30 days (Citera et al., 2000), 5 mg/day for 8 weeks (Hussain et al., 2011), 6 mg/day for 30 days (Reiter, Acuna-Castroviejo, & Tan, 2007), and 10 mg/day for 6 weeks (De Zanette et al., 2014).
Patients with FM also frequently experience increased levels of anxiety (Hussain et al., 2011; Pagano, Matsutani, Ferreira, Marques, & Pereira, 2004; Wilhelmsen et al., 2011). Generally, FM patients show high levels of anxiety and depressive symptoms, which contribute to increased perception of pain and somatization of symptoms, thereby increasing the impact on their quality of life (Uçar et al., 2015). Pagano, Matsutani, Ferreira, Marques, and Pereira (2004) reported that FM patients presented with higher levels of both state and trait anxiety compared to healthy subjects. In the present study, our results showed decreases in anxiety levels with respect to baseline values after melatonin administration, but these changes did not reach statistical significance. It seems possible that melatonin-induced decreases in cortisol levels, which we also found in the present study, would lead to decreases in levels of anxiety. Perhaps with longer periods of administration, the effects of melatonin on anxiety would have been significant.
Conclusion
Taking everything into account, the use of melatonin as an adjuvant therapy for the management of FM symptoms may be recommended. In the present study, administration of melatonin appeared to decrease the severity of some important FM-related symptoms, such as low mood state, increased anxiety levels, high pain levels, and/or impaired quality of life. Further studies with larger samples that explore the impact of melatonin administration at different doses and for different periods of time on quality of life in patients with FM are necessary to corroborate our findings and determine the most effective dose of melatonin for treating FM-related symptoms.
Footnotes
Acknowledgments
The authors are indebted to the volunteers in this study for their outstanding commitment and cooperation.
Author Contributions
M. Y. Castaño contributed to conception, acquisition, analysis, and interpretation; drafted the manuscript; critically revised the manuscript; gave final approval. M. Garrido contributed to conception and design, contributed to analysis and interpretation, drafted the manuscript, critically revised the manuscript, gave final approval. A. B. Rodríguez contributed to design, contributed to interpretation, drafted the manuscript, critically revised the manuscript, gave final approval. M. A. Gómez contributed to design, contributed to interpretation, drafted the manuscript, critically revised the manuscript, gave final approval. All authors agree to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Junta de Extremadura—European Regional Development Funds (ERDF; Grant Number BBB021-GR15051) and a research postdoctoral fellowship held by M. Garrido from Gobierno de Extremadura, jointly financed by the European Regional Development Fund (ERDF; Grant Number PO14013).