
Abstract
Introduction and Objectives:
Methicillin-resistant Staphylococcus aureus (MRSA) is the most prevalent pathogen causing nosocomial infections in hospitals and health centers. This work is an effort to understand the epidemiology of MRSA and other multidrug-resistant pathogens in an intensive care unit (ICU) and to analyze characteristics that might determine the risk of MRSA colonization/infection in this unit.
Method:
An observational, 1-year prospective longitudinal study was conducted to obtain information about MRSA and other multidrug-resistant colonizations/infections. The study was conducted with ICU patients with an artificial airway. Data were obtained from the National Study of the Control of Nosocomial Infections in Intensive Care Units database.
Results:
MRSA colonization was highly prevalent (33%); however, other pathogens like gram(−) Bacillus showed a higher infectious potency. Acute Physiology and Chronic Health Evaluation (APACHE-II) score >15 and hospital stay of >4 days were the main variables that significantly predicted the risk of developing MRSA colonization (p < .001 in both cases). Moreover, the presence of MRSA increased the risk of developing a second multidrug-resistant colonization/infection, especially with methicillin-resistant Pseudomona.
Discussion:
The high prevalence of MRSA emphasizes the need to continue studying risk factors for MRSA colonization/infection, which may allow early identification of this pathogen. Therefore, we propose the use of the APACHE-II score and length of hospital stay to predict increased risk of MRSA colonization. Awareness of the heightened risk in particular patients could lead to early detection and prevention.
Staphylococcus aureus is one of the main pathogens that cause nosocomial infections in the intensive care unit (ICU); however, it is also part of the primary endogenous bacterial flora of hospitalized patients. Since the detection of the first methicillin-resistant S. aureus (MRSA) strain in 1961 (Jevons, 1961), the relevance of this pathogen has increased considerably, as it has become part of the bacterial ecosystem of many hospitals (Lee et al., 2013, 2016). More importantly, the incidence of MRSA colonization/infection, especially in the ICU, has been increasing over the past decades, with several epidemic outbreaks and endemic situations (Stock et al., 2016). Therefore, it has become necessary to develop epidemiological controls that can allow us to predict a possible MRSA colonization/infection at the time of admission to prevent cross-transmission, which is the responsibility of both the medical and nursing staff. Early detection is also needed to avoid unnecessary isolation procedures along with the consequent impacts on patient safety (Callejo-Torre et al., 2016).
In general, nosocomial infections are some of the most important public health problems encountered today (Chacko et al., 2017); therefore, it is necessary to understand the epidemiology and impact of these infections, especially in those patients with a poor health status (i.e., critical patients). MRSA is of great clinical and epidemiological relevance because it is associated with high morbidity and mortality rates and increases the number of hospitalization days and health-care costs (Olaechea et al., 2016). To reduce the impact of nosocomial infections, a multicenter project called the National Study of the Control of Nosocomial Infections in Intensive Care Units (ENVIN-UCI) was developed to determine the infection incidence in critically ill patients. This collaborative multicenter study, which covered 24.8% of the ICUs in Spain, revealed the relevance of all pathogens, not just MRSA. Moreover, this study identified several clinical factors associated with the risk of infection (Olaechea et al., 2003).
In the present study, we further analyzed the data collected for one ICU as part of the ENVIN-UCI to evaluate the influence of several colonization/infection risk factors on the prevalence of the most common multidrug-resistant pathogens. Our hope is that this analysis will serve as a starting point for improving identification and preventive management of patients at increased risk of infection.
Method
Study Design and Participants
We performed an observational, longitudinal prospective study in the ICU of the University Hospital of Torrevieja (Alicante, Spain) from January 1 to December 31, 2017. During this period, 1,291 patients were admitted to the unit. Of these, we evaluated 348 patients who required orotracheal intubation in order to determine the prevalence of MRSA and other nosocomial agents. All admitted patients were included in the analysis, and we established no exclusion criteria.
The Catholic University of Murcia Ethics Committee and the Clinical Commission of the University Hospital of Torrevieja provided written authorization for this study. We guaranteed confidentiality and anonymity of the data and carried out all procedures in accord with the Helsinki Declaration Agreement.
Data Collection
We obtained anthropometric (weight and height) and other clinical parameters such as lymphocytes, neutrophils, leukocytes, and plasma urea levels. To determine the severity of the patients’ health conditions, we used the Acute Physiology and Chronic Health Evaluation (APACHE) Version II Scale (Wong, Crofts, Gomez, McGuire, & Byrick, 1995). This scale was applied within the first 24 hr after the patient’s admission to the ICU. The values of APACHE-II range from 0 to 71, with higher scores indicating more severe disease and an increased risk of death. We also calculated a Barthel index score to evaluate patients’ degree of dependence for completing activities of daily life. We collected all of these data from the patients’ medical records in the hospital database.
Presence of MRSA and Other Multidrug-Resistant Pathogens
Once the patients were admitted to the ICU and after we had evaluated whether they met the study selection criteria, we collected pharyngeal, rectal, and bronchial aspirate (BAS). The procedure to obtain the samples is detailed in Olaechea et al. (2003). In addition, we took samples from any surgical wounds or pressure ulcers that were present. We sent these samples to the microbiology service for the detection of MRSA, vancomicin-resistant Enterococcus, methicillin-resistant Pseudomona, imipenem-resistant Acinetobacter, Enterobacter producing extended-spectrum β-lactamase (ESBL-Enterobacter), and multidrug-resistant gram(−) Bacillus following the ENVIN-UCI protocols (Olaechea et al., 2003). Samples were obtained at the time of admission to the ICU and, for postadmission surveillance, every 7 days after that for the duration of the patient’s stay in the ICU.
Statistical Analysis
For the statistical analysis, we first calculated basic descriptive statistics, analyzing frequencies and/or percentages for categorical variables and using the means and standard deviations for continuous variables.
To analyze the possible relationships between the presence of MRSA and/or other pathogens and several categorical characteristics of the study population, such as sex and degree of dependence (Barthel index), we used the χ2 test. For the APACHE-II score, the days of hospital stay, and the values of the clinical parameters, we compared data using the Student’s t test, depending on the presence of MRSA colonization/infection or not.
To determine the predictive capacity of the different variables regarding the presence of MRSA colonization/infection, we performed a multivariable logistic regression analysis exclusively with those variables that showed a significant association in the bivariate analysis. We used a backward stepwise method of analysis to determine the best predictive model. Finally, once we identified the variables with greater predictive capacity, we carried out a “classification tree” analysis, based on decision-making theory, to calculate the cutoff points that might offer greater sensitivity and specificity to identify those patients at highest risk of MRSA colonization/infection. We used the Chi-squared automatic interaction detector (CHAID) algorithm to detect the best predictors. All tests were performed with the statistical software SPSS, Version 23.0. The level of significance for all statistical tests was set at p < .05.
Results
Clinical Characteristics of the Patients
Participating patients (N = 348) had a mean age of 68 ± 13 years, and 61% (n = 213) were men. Their mean APACHE-II score was 22 ± 9 points, which predicted a mortality percentage of 44–55%. Most participants came to the ICU directly from home (66%), followed by other hospital services (28.2%). The remaining patients came from other hospitals (4.6%), and 1.2% were transferred from nursing homes. Average ICU stay was 8 ± 9 days.
Of all the patients evaluated, 85.8% suffered from chronic diseases. Most of them had diabetes (25.3%), followed by cancer (24.1%) and, at lower percentages, nephropathy (11.5%), immunosuppression (10.9%), and liver disease (5.8%). Barthel’s index scores indicated that a large majority of participants (84.2%) had a high level of independence, although there was variation in degrees of dependence across patients. Finally, 30.8% of the patients were within the normal range for body mass index (BMI = 18.5–24.9 kg/m2), while 57.3% of the patients were above the healthy cutoff value (BMI > 25 kg/m2). Table 1 presents data for key anthropometric and clinical variables.
Comparative Analysis of Selected Demographic and Clinical Characteristics of Patients in the Intensive Care Unit With or Without MRSA Colonization/Infection at Admission or Postadmission.
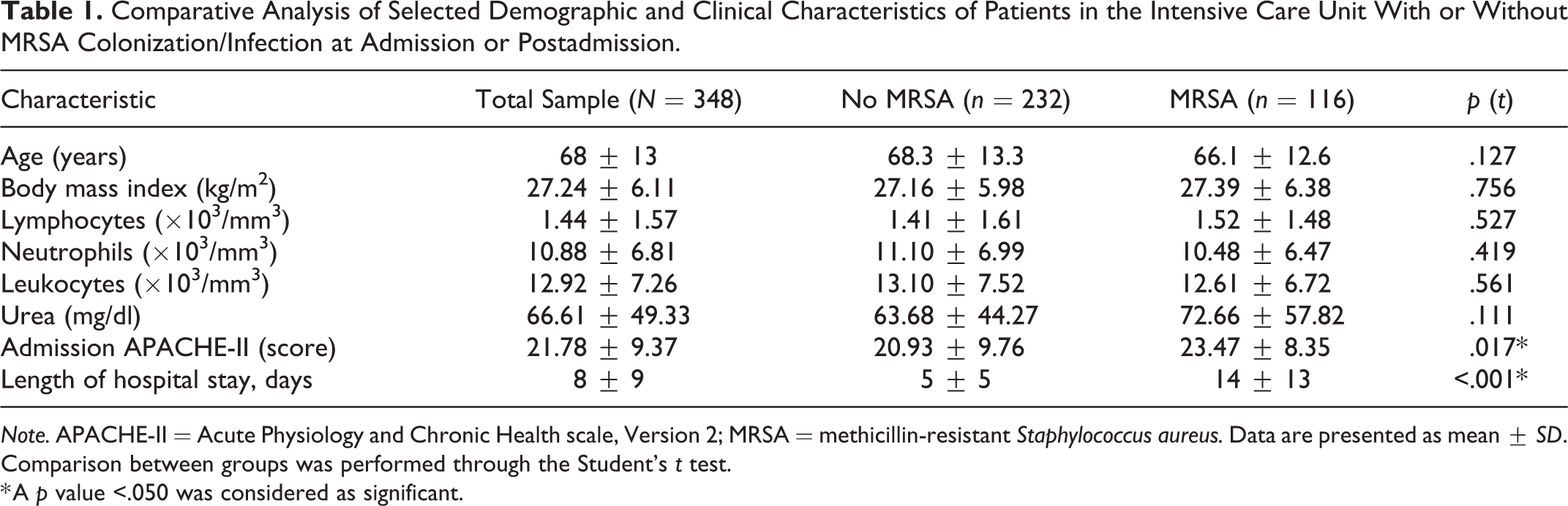
Note. APACHE-II = Acute Physiology and Chronic Health scale, Version 2; MRSA = methicillin-resistant Staphylococcus aureus. Data are presented as mean ± SD. Comparison between groups was performed through the Student’s t test.
* A p value <.050 was considered as significant.
Prevalence of Colonization/Infection by MRSA and Other Multidrug-Resistant Organisms
Our data showed a high prevalence of MRSA-positive colonizations/infections among the 348 participants. Specifically, we detected MRSA in 116 participants at admission or postadmission (Figure 1), or 33% of the patients admitted in 2017, though only two patients went on to develop MRSA infections. Most of the positive samples were obtained from rectal swabs (72.4%), followed by pharyngeal samples (26.7%) and blood samples (1%). In addition, our data showed a high prevalence of methicillin-resistant Pseudomonas (MRP) colonizations/infections that was similar to that of ESBL-Enterobacter. Overall, we detected 20 cases of colonization by ESBL-Enterobacter, and 9 developed infections, for an infection rate of 45% for this pathogen. Data regarding these and the other pathogens are shown in Figure 1.
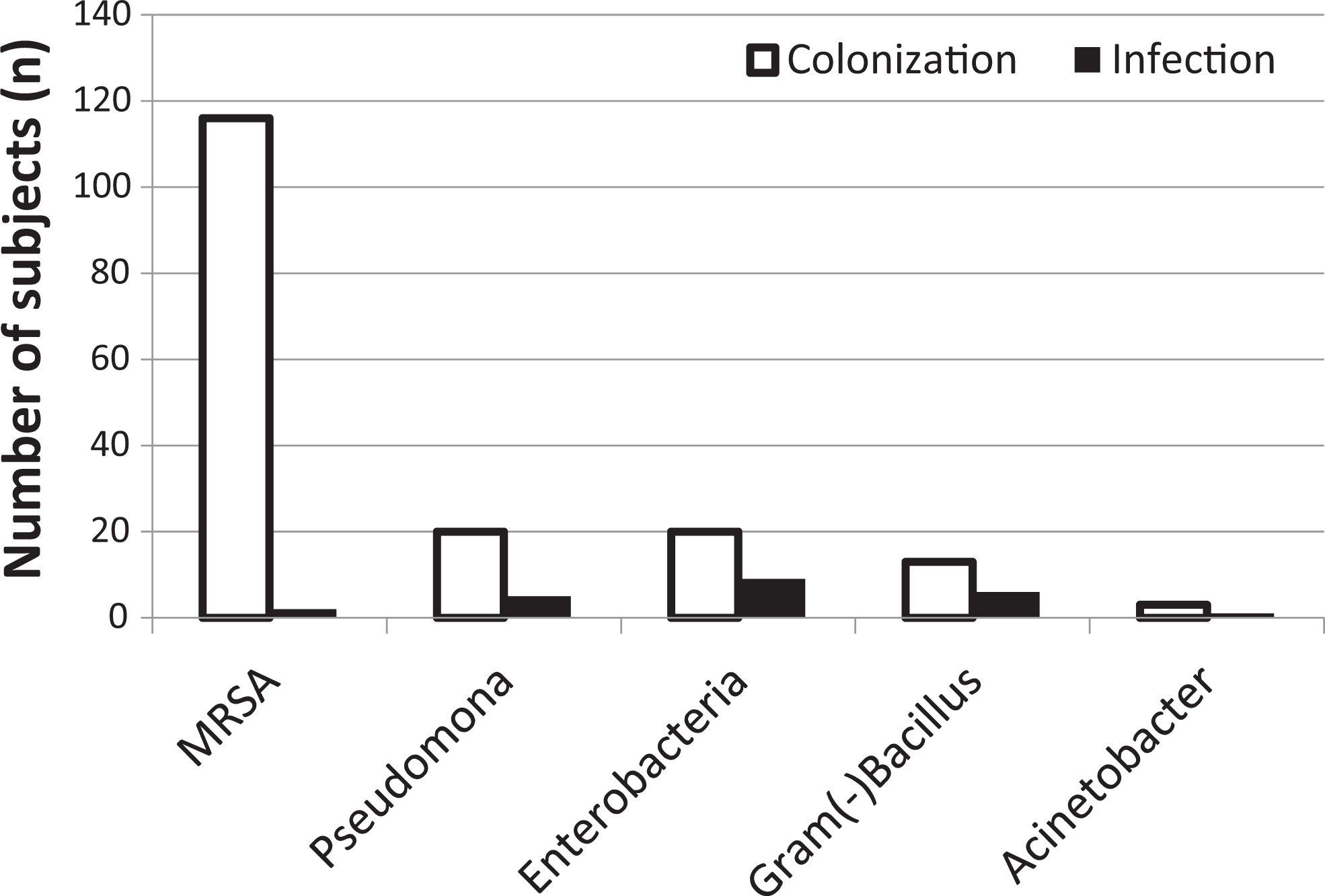
Prevalence of colonization and infection by multidrug-resistant pathogens at admission to the intensive care unit (N = 348). MRSA = methicillin-resistant Staphylococcus aureus.
Of the 116 patients who tested positive for MRSA, 76.7% had it previously (i.e., they tested positive for MRSA at the ICU admission data collection time point), while 23.3% acquired the colonization in the ICU. The prevalence of ESBL-Enterobacter pathogens was also high at the time of admission. However, the other pathogens studied, especially the gram-negative Bacillus spp., were mainly acquired in the ICU (Figure 2).
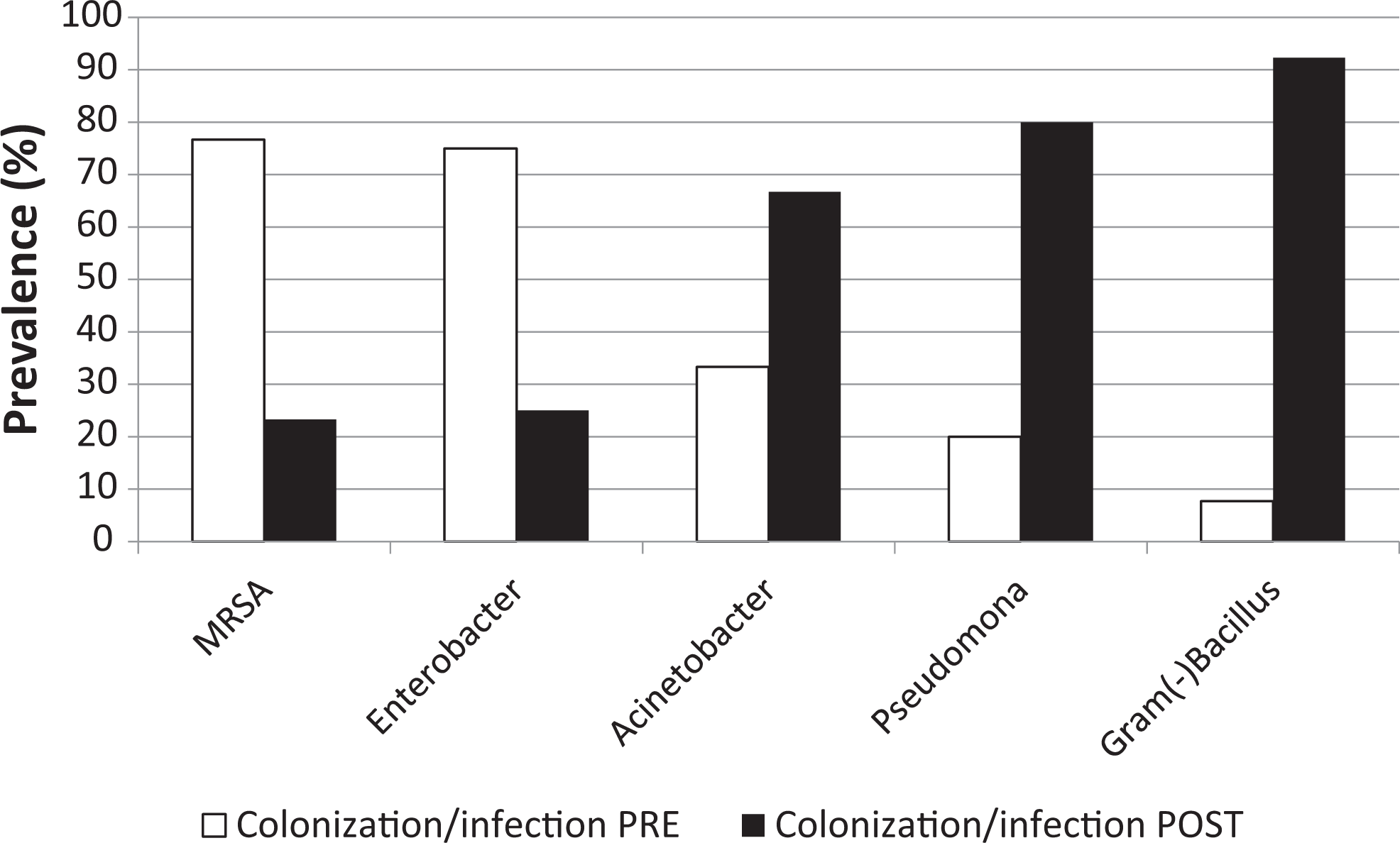
Prevalence of colonization/infection of multidrug-resistant pathogens that started before admission to the intensive care unit (ICU; pre) and that developed during the ICU stay (post). MRSA = methicillin-resistant Staphylococcus aureus.
Relationships Between the Clinical Characteristics and the Presence of MRSA
Of all of the clinical characteristics of the participants, the APACHE-II score showed a statistically significant association with the presence of a pathogen. Specifically, patients with MRSA colonizations/infections showed significantly higher APACHE-II scores than those without. The variable with the highest t value was the number of days in the ICU. Patients who had MRSA colonization/infection had an average stay that was 3 times longer than those without MRSA. No other anthropometric or clinical variables had significant relationships to MRSA colonization/infection (Table 1). Similarly, there seemed to be no significant relationship between the degree of dependence in the performance of activities of daily living and colonization/infection with MRSA (χ2 = 2.146, p = .709).
Our findings were somewhat contradictory in regard to clinical history. There was no relationship between the presence of diabetes, liver disease, nephropathy, or immunosuppression and the risk of MRSA colonization/infection. However, contrary to what might be expected, those patients with cancer histories had a significantly lower risk of MRSA colonization than those without such a history (χ2 = 4.270, p = .039).
We performed a multivariable logistic regression analysis to determine the degree of influence clinical variables had on the risk of MRSA colonization/infection. Both the APACHE-II score and the days of the hospital stay significantly influenced the risk of colonization/infection by MRSA (Table 2). Although the odds ratios (OR) seem low, it’s important to remember that both of the predictor variables (APACHE-II and days of stay) are continuous variables, meaning that for each additional point in value, the risk of colonization/infection was multiplied. So, for example, for every additional day in the ICU, the MRSA risk increased by a factor of 1.148.
Multivariate Logistic Regression Analysis Considering Methicillin-Resistant Staphylococcus Aureus (MRSA) Colonization as the Dependent Variable and APACHE-II Score and Days of Stay in the Intensive Care Unit as Independent Variables.
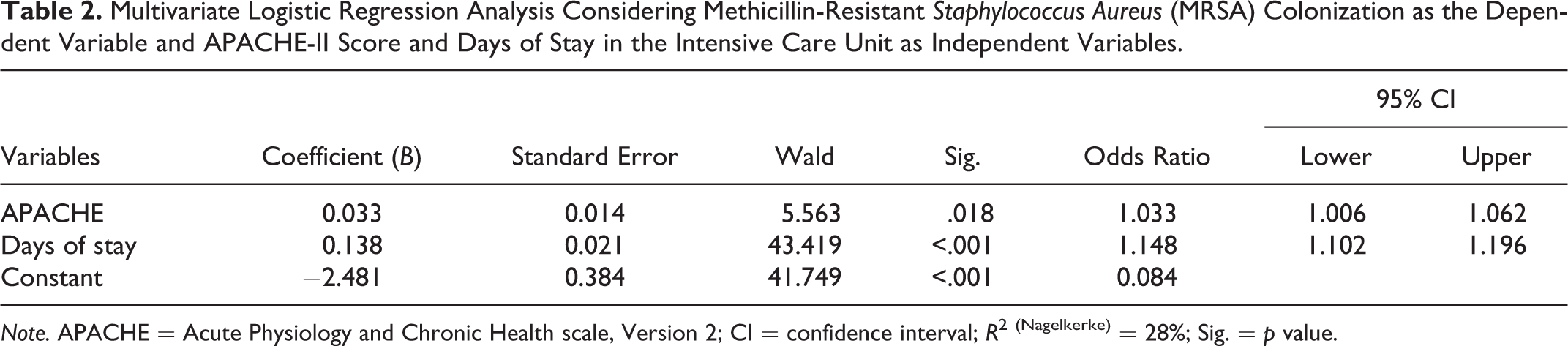
Note. APACHE = Acute Physiology and Chronic Health scale, Version 2; CI = confidence interval; R 2 (Nagelkerke) = 28%; Sig. = p value.
Finally, we carried out a decision-making analysis of these two variables (APACHE-II score and days of stay in the ICU) using a classification tree to determine the most precise diagnostic criteria to predict MRSA colonization (Figure 3). For the APACHE-II Scale, our analysis established a cutoff point of 15 points, with scores higher than 15 predicting a significant increase in the risk of MRSA colonization/infection. Likewise, more than 4 days in the ICU predicted a significant increase in the risk of MRSA colonization/infection (Figure 3).
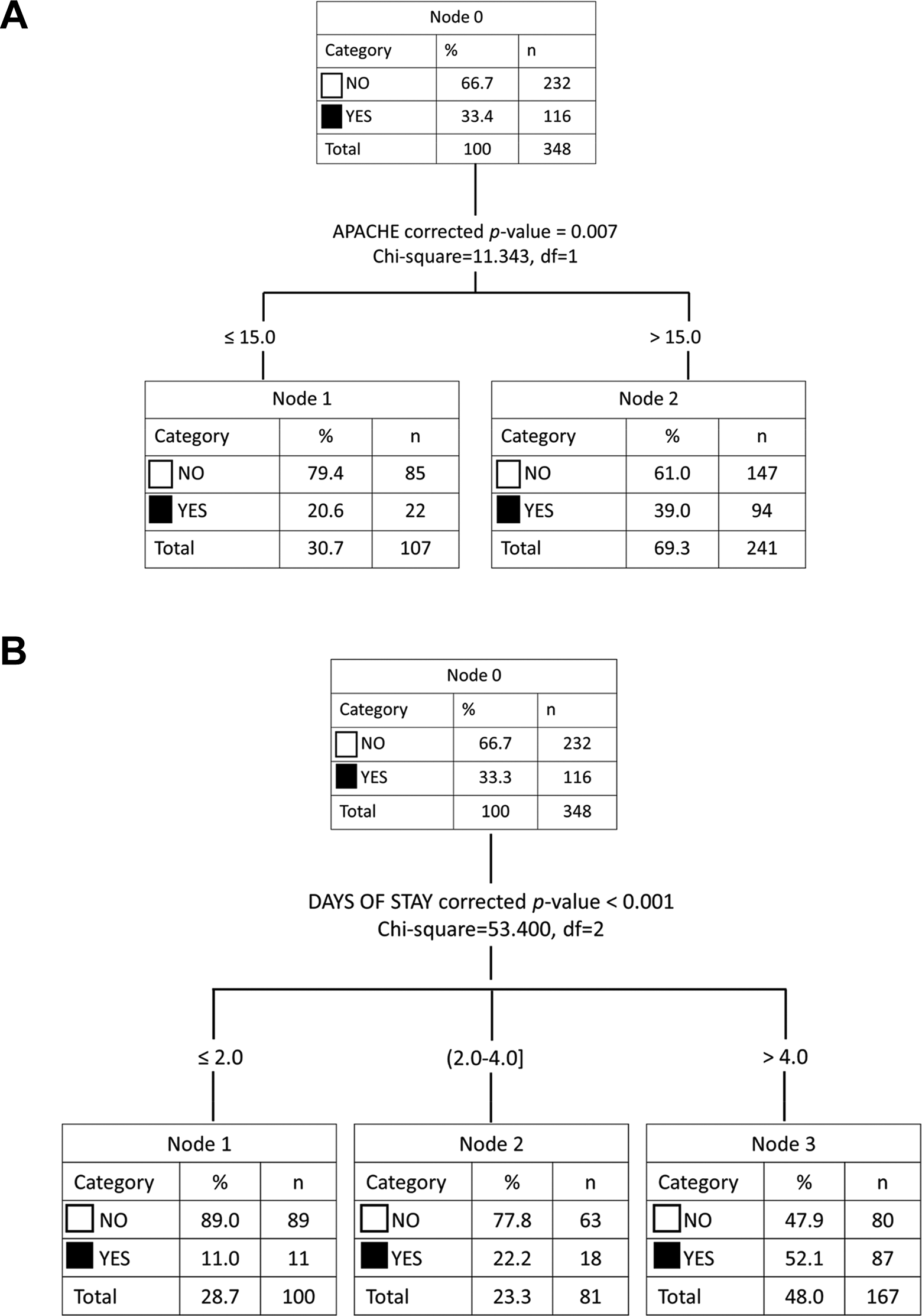
Decision-making analysis using the Chi-squared automatic interaction detector (CHAID) ) algorithm to determine the best predictive criteria for methicillin-resistant Staphylococcus aureus (MRSA) colonization/infection using the significant variables of (A) Acute Physiology and Chronic Health Evaluation (APACHE-II) score and (B) days of stay in the intensive care unit (ICU). MRSA colonization/infection was the dependent variable, with the study population being divided into categories depending presence (Yes) or absence (No) of colonization. Cut off for the APACHE-II score was 15 and for days of stay was 4, with higher values predicting significantly increased risk. MRSA = methicillin-resistant Staphylococcus aureus.
Relationships Between MRSA Colonization/Infection and Colonization/Infection With Other Multidrug-Resistant Pathogens
We found that 1.4% of participants had three simultaneous infections, while another 9.85% had two simultaneous infections, which might indicate possible interactions among the pathogens. Therefore, we evaluated the possible relationships between colonization/infection with MRSA and with the other multidrug-resistant agents. Our results showed that an MRSA colonization significantly increased the risk of other colonizations/infections, as shown in Figure 4. Of great interest was the relationship between MRSA and MRP. In those patients with MRSA colonization/infection, the relative risk of also having an MRP colonization/infection was 13-fold higher than in patients without an MRSA colonization/infection.
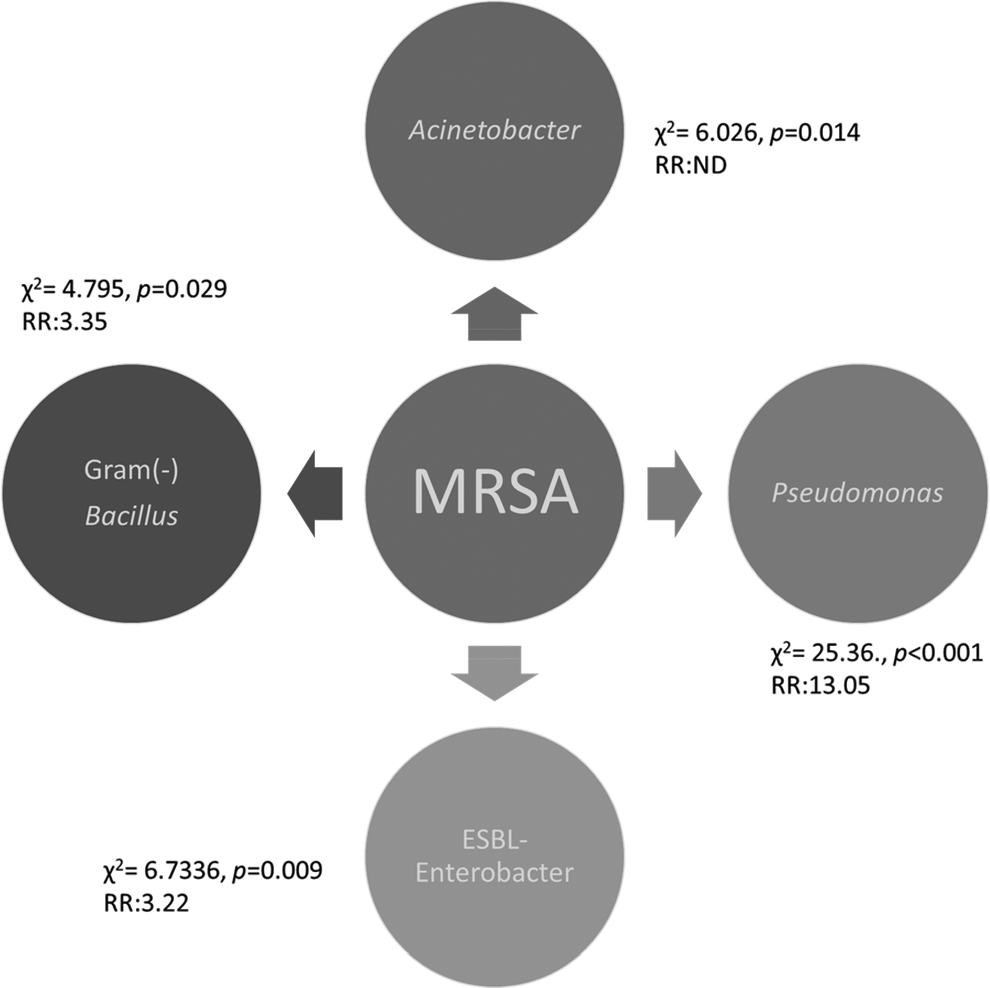
Relationships between MRSA colonization/infection and the risk of colonization/infection with the other multidrug-resistant pathogens. Pairwise associations were determined by the χ2 test. MRSA = methicillin-resistant Staphylococcus aureus; ND = not determinable; RR = relative risk.
Discussion
This research describes the incidence of colonization/infection by MRSA and other multidrug-resistant agents in an ICU. Of all the pathogens studied, the most prevalent was MRSA. These results are consistent with previous data obtained from the last ENVIN-UCI report (Palomar et al., 2015), although the MRSA prevalence in the present study was slightly higher than was reported in the European Antimicrobial Resistance Surveillance Network (EARS-Net) report (Kinoshita, Tokumasu, Tanaka, Kramer, & Kawakami, 2017). Based on the EARS-Net report, the prevalence of MRSA in Spain is slightly higher than that in many other countries in Europe, and much higher than some, like Iceland, where the prevalence is 0–2.8%. However, it is lower than that of other countries, such as Romania, which has an MRSA prevalence of 25–69%. Evidently, the characteristics of each region have significant influences on the prevalence of MRSA; therefore, it is important to carry out this type of epidemiological study at the local level in order to identify the local microbiological pathogens and detect these infectious agents early.
In 2014, the Spanish Society of Intensive and Critical Care Medicine and Coronary Units began a project called Zero Resistance (ZR), which had the aim of reducing the infection and/or dissemination of multidrug-resistant bacteria in ICUs (Garnacho Montero et al., 2015). The strategies proposed in the ZR project aimed to control cross-transmission through the health-care staff and eliminate the reservoirs. In the present study and in the ZR study, there was a significant increase in the number of patients identified with ESBL-Enterobacter and MRSA compared to previous data, especially upon admission to the ICU.
Only two patients in the present study developed MRSA infections. Although the results showed no relationship between being colonized by MRSA and developing an infection, other studies have found such a relationship. For example, Vigil et al. (2015) concluded that most of the patients with MRSA colonizations developed infections. Safdar and Bradley (2008) described a similar finding. Therefore, even though we did not observe a significant relationship in the present study, we cannot rule out the possibility that being colonized increases the risk of infection (Altınbas, Shorbagi, Ascıoglu, Zarakolu, & Cetinkaya-Sardan, 2013). Given the current evidence, it is recommended that each institution establishes appropriate hospital infection control policies according to the local epidemiological criteria. The present work may represent a starting point for that purpose.
The study of the risk factors associated with nosocomial infections in Spain was introduced in 2003 with the ENVIN-UCI project (Olaechea et al., 2003). This project identified a number of characteristics that might increase the risk of ICU infections. There seemed to be a greater probability of MRSA colonization in nursing home residents and patients transferred from other hospitals than in those patients admitted from their homes (Baldwin et al., 2009; O’Sullivan & Keane, 2000). However, we did not observe this kind of association in the present work.
Previous studies have indicated that suffering from a chronic disease is a risk factor for the presence of MRSA (Cadena, Thinwa, Walter, & Frei, 2016). In fact, several comorbidities, such as diabetes, liver disease, immunodeficiency, and cancer, are specific risk factors for MRSA infections (Ghanem, Abou-Alia, & Alsirafy, 2013; Lin et al., 2017; Popovich, Weinstein, Aroutcheva, Rice, & Hota, 2010). Contrary to what might have been expected based on these previous findings, however, though 85% of participants in the present study had at least one chronic disease, we found no relationship between clinical history and risk of MRSA colonization/infection except in patients with a history of cancer, which paradoxically was associated with a decreased risk of suffering from MRSA. Most likely this finding was not due to cancer being a protective factor but rather because the frailty of these patients encouraged the ICU staff to increase prevention measures. Prevention measures for patients with cancer are generally much more thorough than they are for patients with other pathologies. In fact, other studies have also observed that immunodeficiency exerts a protective effect, precisely because of the intense isolation measures used with these patients (Callejo-Torre et al., 2016).
There was great homogeneity in clinical characteristics between the patients who had MRSA present and the noncarriers in the present study. Likewise, we found no previous studies that showed a predictive role for the clinical characteristics of the patients. Nevertheless, it is important to emphasize that, although we did not observe statistically significant relationships in the present study, we did observe a trend toward a higher probability of infection in subjects with lower BMI (<18.5 kg/m2). This finding may be probably due to the fact that these individuals have lower immunological activity, as reflected by the fact that they have presented a lower lymphocyte count (Haag-Weber, Dumann, & Hörl, 1992).
Although clinical characteristics didn’t differ much between patients with and without MRSA colonization, we did find that illness severity as measured by the APACHE-II score and days in the ICU were related to the risk of MRSA colonization/infection. According to our multivariate analysis, these two variables predicted the risk of carrying MRSA. Specifically, the greater the severity of the illness in the first 24 hr after admission to the ICU, the greater the probability of being infected with or colonized by MRSA, a finding that coincides with the results of Bouza et al. (2012), who also found through a multivariate analysis that higher APACHE II score was an independent risk factor for MRSA. Other authors, such as Callejo-Torre et al. (2016), have identified the APACHE-II score as the best predictor of risk of MRSA colonization/infection, with OR values very similar to those that we calculated. The duration of the ICU stay was also a very effective predictor of MRSA colonization/infection among our sample, with a longer stay significantly increasing the risk. Previous authors have described this phenomenon as well. Andreassen et al. (2017) found that patients with MRSA stayed on average 8 days longer in the hospital than controls. Therefore, though no studies have quantified the risk as we did in the present work, there does seem to be consensus that the longer the stay, the greater the probability of identifying colonization/infection with MRSA. In light of ours and prior findings, we recommend that patients with admission APACHE-II scores >15 and hospital stays longer than 4 days be monitored more closely for the development of MRSA colonization/infection.
According to the literature that we reviewed, the most useful type of sample for detecting MRSA is the nasal swab. It is important to point out that in the hospitals included in the ENVIN-UCI project, this type of sample is not collected, so the data we obtained in the present work cannot be compared with that of previous studies that have used nasal samples (Ho, Huang, & Lin, 2011). It may seem contradictory that the study did not analyze the samples in which most MRSA is detected; however, because many ICU patients are intubated and, therefore, sedated, it is possible to obtain a pharyngeal sample, which should be even more representative. In addition, studies have found that a very low number of positive samples were detected in the nasal swabs from patients with known infections, so this sample type has questionable usefulness based on its low sensitivity (Senn, Basset, Nahimana, Zanetti, & Blanc, 2012). The samples with the greatest number of positives in the present work were the rectal samples. Previous studies agree that the most frequent localization of MRSA after the nasal cavity is the rectal/perineal region (Aldeyab et al., 2009).
Finally, it is important to emphasize our finding that presenting with an MRSA colonization increases the risk of developing colonization/infection by other multidrug-resistant agents. Pereira, Oliviera, and Almeida (2016) recently described a similar finding, which reinforces the need to detect MRSA early in the ICU not only to prevent the development of an MRSA infection but also to prevent colonization/infection by other infectious agents.
In conclusion, the prevalence of MRSA colonization/infection in the present study was high, although the rate of infection was much lower than that of the other multidrug-resistant agents, especially gram-negative Bacillus spp. Moreover, the presence of MRSA was associated with an increased risk of colonization/infection by other multidrug-resistant pathogens, especially MRP, which reinforces the need to effectively prevent MRSA colonization.
Of all the risk factors we studied, the APACHE-II score and days of ICU stay showed significant predictive abilities regarding MRSA colonization. These findings lead us to recommend that ICU patients with admission APACHE-II scores >15 and who stay in the ICU for more than 4 days should be more closely monitored in order to prevent the development of colonization/infection. Nurses can play an important role in prevention efforts by conducting an early evaluation of illness severity using the APACHE-II scale and emphasizing controlling infections in patients with long hospital stays.
Footnotes
Author Contributions
J. J. Hernandez Morante contributed to conception and design, acquisition, analysis, and interpretation; drafted the manuscript; critically revised the manuscript; gave final approval. E. Ochotorena contributed to conception and design, acquisition, analysis, and interpretation; drafted the manuscript; critically revised the manuscript; gave final approval. R. Cañavate contributed to design, acquisition and interpretation; drafted the manuscript; critically revised the manuscript. R. A. Villegas contributed to conception, acquisition and analysis; drafted the manuscript; critically revised the manuscript; gave final approval. I. Viedma contributed to conception and design, acquisition, analysis, and interpretation; drafted the manuscript; critically revised the manuscript; gave final approval. All authors agree to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.