
Abstract
The purpose of this cross-sectional study was to explore the determinants of hemoglobin A1c (HbA1c) levels in insulin-treated patients with Type 2 diabetes mellitus (T2DM) based on demographic and disease characteristics, self-reported regimen adherence factors (adherence in insulin regimen and self-monitoring of blood glucose), and psychosocial factors (decisional balance for insulin injection, health literacy, self-efficacy for insulin injection, diabetes distress, and empowerment perceptions). Via convenience sampling, 255 insulin-treated patients with T2DM were recruited from two endocrinology clinics in Taiwan. A self-report questionnaire was used to collect demographic and disease characteristics, regimen adherence factors, and psychosocial factors. The first HbA1c level measured after completion of the questionnaire was the dependent variable. The last HbA1c level measured before patients started insulin therapy as well as body mass index (BMI) was collected from medical records. Results indicated that adherence in insulin regimen was relatively good. Regimen adherence factors did not significantly correlate with HbA1c levels, but empowerment perception, decisional balance for insulin injection, health literacy, and diabetes distress did. The hierarchical multiple regression models indicated that BMI, the last HbA1c levels before starting insulin therapy, empowerment perception, and diabetes distress were important determinants of HbA1c levels. Nurses could periodically assess the diabetes distress of insulin-treated patients with T2DM and refer to mental health professionals when needed. Furthermore, applying empowerment approaches such as enhancing self-awareness of improved glycemic control and sharing more decision-making power with insulin-treated patients with T2DM might have benefits for their glycemic control.
Keywords
Approximately 425 million individuals have been diagnosed with diabetes worldwide (International Diabetes Federation [IDF], 2017). Furthermore, according to the IDF, it is predicted that 642 million individuals will suffer from Type 2 diabetes mellitus (T2DM) by the year 2040. In Taiwan, the prevalence of T2DM has reached 9.2%, and diabetes was the fifth leading cause of death in 2016 (Ministry of Health and Welfare, 2016). Controlling T2DM is a national health issue in many countries, including Taiwan.
Poor glycemic control increases the risk of developing a range of complications in patients with T2DM, such as cardiovascular disease and diabetic retinopathy (American Diabetes Association [ADA], 2018). Hemoglobin A1c (HbA1c) levels are a vital health indicator for patients with T2DM, and the ADA recommends <7% as a reasonable goal for optimal control. Initiation of the use of insulin early in the disease course has been shown to improve glycemic control, reduce hypoglycemic episodes, and potentially slow down disease progression (Aschner et al., 2012; Hanefeld, 2014). Insulin injection is frequently recommended for patients with T2DM who were originally treated with oral drugs but who demonstrate poor glycemic control (Rodbard et al., 2009). Nevertheless, even many patients prescribed insulin do not achieve optimal glycemic control. In fact, only 35–54% of insulin-treated patients with T2DM have HbA1c levels <7% (Giugliano, Maiorino, Bellastella, Chiodini, & Esposito, 2011a, 2011b). Furthermore, researchers have reported that HbA1c levels of insulin-treated patients with T2DM were higher than those of patients receiving oral drug therapy (Bahrmann et al., 2014; DiBonaventura, Wintfeld, Huang, & Goren, 2014). Exploring determinants of HbA1c levels, specifically in insulin-treated patients with T2DM, should help in the design specific interventions to improve glycemic control.
Research has shown that demographic and disease characteristics such as sex, age, diabetes duration, and body mass index (BMI) are associated with HbA1c levels in insulin-treated patients (Angamo, Melese, & Ayen, 2013; Linetzky, Jiang, Funnell, Curtis, & Polonsky, 2017). Furthermore, for these patients, the ADA (2018) emphasizes adherence to insulin regimens suggested by health-care providers regarding frequency and dosage of injections as well as self-monitoring of blood glucose (SMBG) for achieving optimal glycemic control. A number of studies have shown that adherence to the recommended insulin regimen and SMBG are associated with more optimal HbA1c levels (DiBonaventura et al., 2014; Linetzky et al., 2017). Insulin-regimen adherence factors should therefore be considered when exploring determinants of HbA1c levels in insulin-treated patients with T2DM.
Research has also identified several modifiable psychosocial factors that are associated with HbA1c levels in patients with T2DM, regardless of insulin treatment status (Brown et al., 2016), that could be explored as potential determinants of HbA1c levels specifically in insulin-treated patients with T2DM. Among these factors, investigators have frequently identified attitude toward behaviors as an important determinant of behaviors and, subsequently, of health outcomes. The transtheoretical model posits that individuals simultaneously weigh the pros and cons of a behavior before adopting it (Prochaska, Redding, & Evers, 2008). The concept of decisional balance was found to be associated with many health behaviors and outcomes. Although insulin-treated patients might have more positive than negative attitudes toward insulin injection, they might hold negative attitudes toward it related to side effects such as hypoglycemia and weight gain (Tong, Vethakkan, & Ng, 2015). Decisional balance for insulin injection might thus be an important psychosocial determinant of HbA1c levels in insulin-treated patients. This hypothesis has not been thoroughly explored in insulin-treated patients with T2DM and merits further study.
Patients need to clearly understand and effectively apply health information in order to make appropriate health decisions for the management of their illness (Nutbeam, 2000). Health literacy, or the cognitive and social ability to access, comprehend, judge, and use health information in health decisions, requires functional literacy, communicative literacy, and critical literacy (Nutbeam, 2000). In order to have an appropriate insulin treatment plan, insulin-treated patients need to not only be able to adjust their insulin regimen according to the daily fluctuation of blood glucose levels but also critically appraise different sources of information and negotiate with health-care providers. Possession of adequate health literacy might be crucial for the achievement of optimal glycemic control in insulin-treated patients with T2DM.
Self-efficacy, which is considered an important determinant of health outcomes, refers to the confidence an individual has that she or he is able to successfully perform activities that will lead to the achievement of desired outcomes (Prochaska et al., 2008). A strong body of evidence supports the association between high levels of self-efficacy and low levels of HbA1c in patients with T2DM (Gonzalez, Shreck, Psaros, & Safren, 2015; Lee et al., 2016). It follows, then, that high levels of self-efficacy for insulin injections should be associated with low HbA1c levels in insulin-treated patients with T2DM.
Performing daily self-care activities is demanding, which might lead patients with T2DM to experience stress. Diabetes distress, which refers to significantly negative emotional reactions to the stress of managing diabetes (Fisher, Gonzalez, & Polonsky, 2014), has become a major issue for patients with T2DM (ADA, 2018). Researchers found that the level of diabetes distress in insulin-treated patients was higher than that in patients with T2DM receiving oral drug treatment (Snoek, Skovlund, & Pouwer, 2007). Furthermore, additional research found that high diabetes distress levels were associated with high HbA1c levels in insulin-treated patients (Linetzky et al., 2017).
In addition to the intrapersonal psychosocial factors mentioned above, patient–provider communication style affects health outcomes of patients with T2DM (ADA, 2018). Linetzky et al. (2017) found that the quality of the interaction between patient and physician directly affected HbA1c levels in insulin-treated patients. Patient empowerment, which is one type of patient–provider interaction, refers to a process in which health-care providers encourage patients to think critically and act autonomously rather than to merely follow assigned regimens (Anderson & Funnell, 2010). Through patient empowerment, patients make their own health decisions and take control of their disease(s). Patient empowerment has been positively associated with maintenance of optimal HbA1c levels in patients with T2DM regardless of insulin treatment status (Rossi et al., 2015); thus, it is worth exploring whether it is associated specifically with HbA1c levels in insulin-treated patients with T2DM.
The aim of the present study was to explore the determinants of HbA1c levels in insulin-treated patients with T2DM among demographic and disease characteristics, self-reported regimen-adherence factors, and psychosocial factors.
Method
Study Design and Participants
For this study, we adopted a cross-sectional design. Because participants aged >80 years might have difficulty in reading and completing a self-report questionnaire and those aged <20 years might have low prevalence of T2DM, we limited participants to those aged 20–85 years. We recruited patients who had been diagnosed with T2DM for more than 6 months and on insulin treatment for at least 6 months from two outpatient endocrinology clinics in Taiwan by convenience sampling. Patients who were unable to communicate verbally or finish questionnaires due to physical or mental problems were excluded. Physicians at the clinics referred eligible patients to a research assistant, who explained the purposes of the study to them. After eligible patients signed the informed consent forms, they were administered the questionnaires. We provided a gift of soap to patients who completed the questionnaire.
We recruited 255 patients as participants. Based on an α level of .05, a small effect size for multiple linear regression (f 2 = .15), and 15 independent variables in the multiple linear regression model, we calculated that a sample size of 255 would be adequate to reach a power of .95. Data were collected from September 2016 to March 2017.
Data Collection
The first HbA1c level measured after administration of the questionnaire (current HbA1c level) was a dependent variable. We also collected the last HbA1c level measured before the patient started insulin therapy and BMI (weight in kilogram/height in m2) from the medical record of each participant. We used an anonymous self-report questionnaire to collect the following data.
Demographic and disease characteristics
Demographic and disease characteristics collected via the self-report questionnaire included sex, age, duration of diabetes, duration of treatment with insulin injection, and whether or not participants were taking oral medication to treat their diabetes in addition to insulin (no/yes).
Self-reported regimen adherence factors
The questionnaire also had items measuring recommended and actual weekly performance in maintaining an insulin-administration regimen (frequency and dosage) and SMBG. We calculated adherence rate using actual performance divided by recommended performance and multiplying by 100. An adherence rate <100% was categorized as incomplete adherence, while ≥100% was categorized as complete adherence.
Decisional balance for insulin injection
We developed the 13-item Decisional Balance for Insulin Injection Scale to assess participants’ attitude toward insulin injection. The scale comprised subscales of Pros (5 items) and Cons (8 items). Respondents rated each item from 1 point (strongly disagree) to 5 points (strongly agree). We calculated mean item scores for the Pros and Cons subscales separately and then calculated the score for decisional balance for insulin injection by deducting the mean item score of the Cons subscale from that of the Pros subscale. The total possible score ranged from −4 to 4. A positive score indicated that perceptions of Pros outweighed those of Cons, and the higher the score, the more positive the decisional balance for insulin injection. We created this scale after conducting exploratory factor analysis (EFA). Its construct validity was preliminarily supported. The Cronbach’s α of Pros and Cons subscales were .79 and .88, respectively, and the content validity index (CVI) was .9 in the present study.
Health literacy
We used the Chinese-language version of the Health Literacy Scale for Diabetes to assess the health literacy of participants (Lee et al., 2016). Previous research supported the construct validity of this scale as evaluated by EFA and its reliability (Lee et al., 2016). The scale includes 14 items, of which 5 measure functional literacy, 4 measure communicative literacy, and 5 measure critical literacy. Respondents rate each item on a 4-point scale, ranging from 0 (never) to 3 (usually), with functional literacy reverse-scored. The total possible score ranges from 0 to 42. The higher the total score, the better the health literacy. In the present study, Cronbach’s α was .85, and the CVI was 1.0.
Self-efficacy for insulin injection
We developed a 4-item scale measuring self-efficacy for insulin injection to assess the confidence participants had in their ability to preserve insulin and inject it according to recommended dosage, time, and injecting position. Respondents rated each item on a 5-point scale ranging from 0 (no confidence) to 4 (over 80% confidence). The total possible score ranged from 0 to 16, with higher scores indicating better self-efficacy for insulin injection. In the present study, one factor was produced by EFA, which lent preliminary support to the construct validity of this scale. Cronbach’s α was .89, and the CVI was 1.0 in the present study.
Diabetes distress
We assessed diabetes distress with the Chinese version of the Short-Form Problem Areas in Diabetes scale (Hsu et al., 2013). Previous research established construct validity examined by EFA, criterion-related validity, and reliability of this scale (Hsu et al., 2013). The instrument comprises 8 items, each of which respondents rate on a 5-point scale ranging from 0 (not a problem) to 4 (serious problem). Total possible score ranges from 0 to 32. with higher scores representing more-severe diabetes distress. In the present study, Cronbach’s α was .92, and the CVI was 1.0.
Empowerment perception
We used a 13-item Chinese version of the Diabetes Empowerment Process Scale (Lee et al., 2016) to assess the degree to which participants felt empowered by health-care providers (physicians, nurses, nutritionists, diabetes educators). Previous research supports construct validity evaluated by EFA and reliability of this scale (Lee et al., 2016). Respondents rate each item on a 5-point scale, with scores ranging from 1 (strongly disagree) to 5 (strongly agree). The total possible score ranges from 13 to 65, with higher total scores indicating higher perceived patient empowerment. In the present study, Cronbach’s α was .95, and the CVI was 1.0.
Validity and Reliability
The scales we used in the present study to measure health literacy, diabetes distress, and empowerment perception had been previously used in patients with T2DM without regard for insulin-treatment status (Hsu et al., 2013; Lee et al., 2016); thus, it is possible that they are not appropriate for a sample comprising insulin-treated patients only. Furthermore, we developed the scales of self-efficacy for insulin injection and decisional balance for insulin injection specifically for this study. We invited two endocrinologists and five certified diabetes educators to examine these scales for content validity. These experts rated the relevance of each item on a scale from 1 (irrelevant) to 4 (highly relevant and succinct). We calculated the CVI of each scale by dividing the number of items rated three or four by the total number of items. To assess the preliminary construct validity of the scales for self-efficacy for insulin injection and decisional balance for insulin injection, we used EFA. Furthermore, we calculated the internal consistency reliability of each scale using Cronbach’s α based on the data of all participants. As we mentioned above in the descriptions of the scales, all scales possessed acceptable validity and reliability.
Ethical Considerations
The institutional review boards (IRBs) of two hospitals approved this study (NO. KMUHI-E(I)-20150262, TSGHIRB-1-105-05-163). Participants were informed of their right to refuse participation or withdraw from the study without any penalty. We obtained a signed informed consent form before administering the questionnaire to participants.
Data Analysis
We used SPSS, Version 14.0 for Windows (SPSS, Inc., Chicago, IL) for all statistical analyses. To examine the distribution of the study variables among the participants, we used descriptive statistics. To examine the associations of demographic and disease characteristics, regimen adherence factors, and psychosocial factors with HbA1c levels, we used the Pearson correlation test. For investigating the relative importance of demographic and disease characteristics, regimen adherence factors, and psychosocial factors to the determination of HbA1c levels, we conducted hierarchical multiple regression analysis, sequentially entering blocks of demographic and disease characteristics, regimen adherence factors, and psychosocial factors into the model and coding nominal variables such as sex, combining oral medication, and regimen adherence factors as dummy variables. Statistical significance was established at p value less than .05.
Results
Table 1 includes a summary of the distribution of demographic and disease characteristics as well as psychosocial factors of the 255 participants. The mean age of participants was 56.58 ± 10.91 years, 38% (n = 97) were female, and 72.9% (n = 186) were using a combination of insulin and oral medication for treatment. Mean current HbA1c levels was 8.33% ± 1.49, and only 16.5% (n = 42) of participants had levels that met the recommended goal of <7% (ADA, 2018). A large majority of participants self-reported completely adhering to frequency (89.8%) and dosage (84.7%) recommendations for insulin injection, while 50.2% reported complete adherence to SMBG.
Distribution of Demographic and Disease Characteristics, Regimen Adherence Factors, and Psychosocial Factors of Participants.
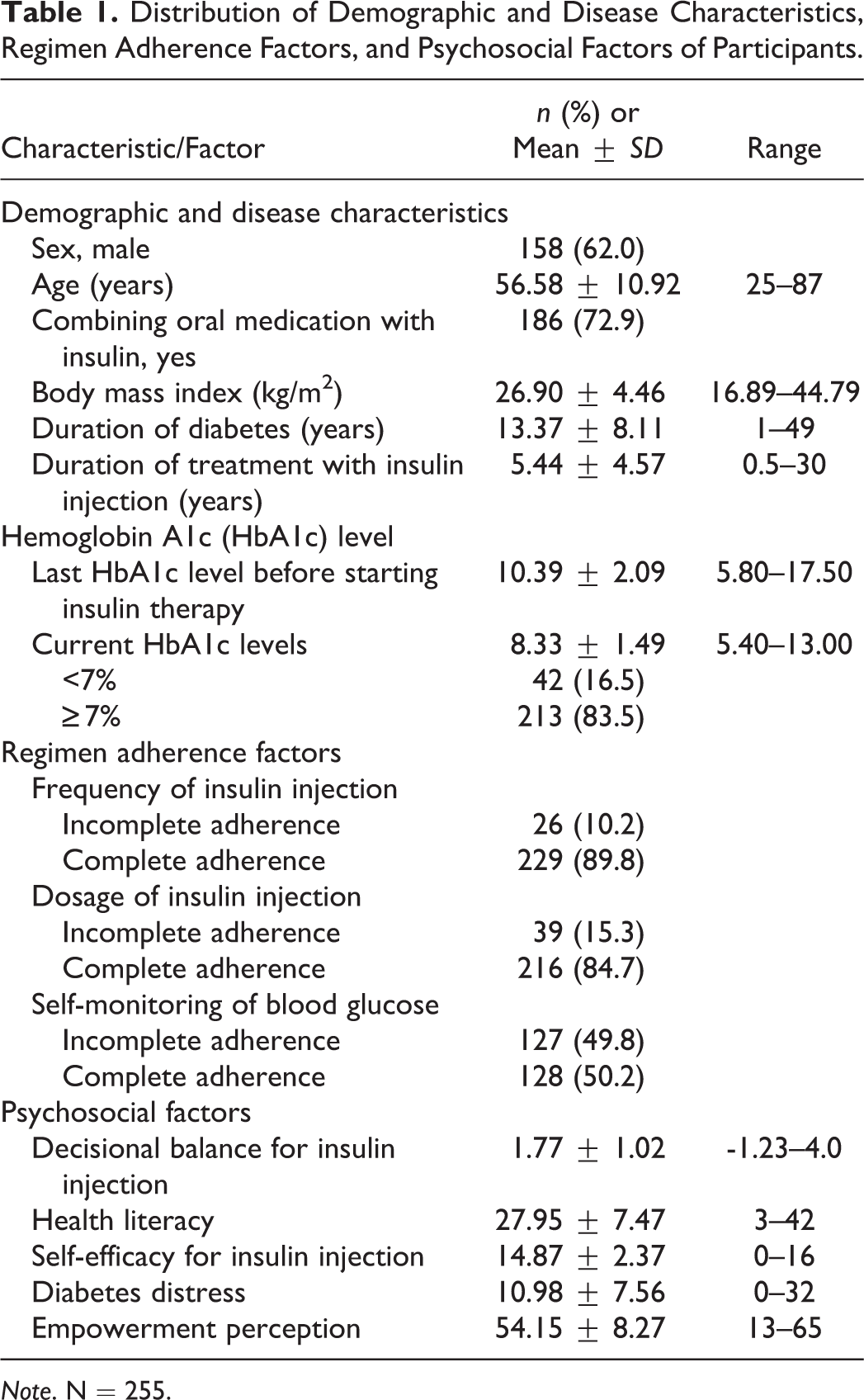
Note. N = 255.
The bivariate correlation analysis indicated that BMI and the last HbA1c level before starting insulin therapy were positively and significantly correlated with current HbA1c levels (Table 2). Adherence factors were not significantly associated with current HbA1c levels. Empowerment perception, decisional balance for insulin injection, and health literacy were significantly and negatively correlated with current HbA1c levels. Diabetes distress was significantly and positively correlated with current HbA1c levels. Self-efficacy for insulin injection did not significantly correlate with HbA1c levels.
Correlation and Hierarchical Multiple Regression for Associations of Demographic and Disease Characteristics, Regimen Adherence Factors, and Psychosocial Factors With Current Hemoglobin A1c (HbA1c) Levels.
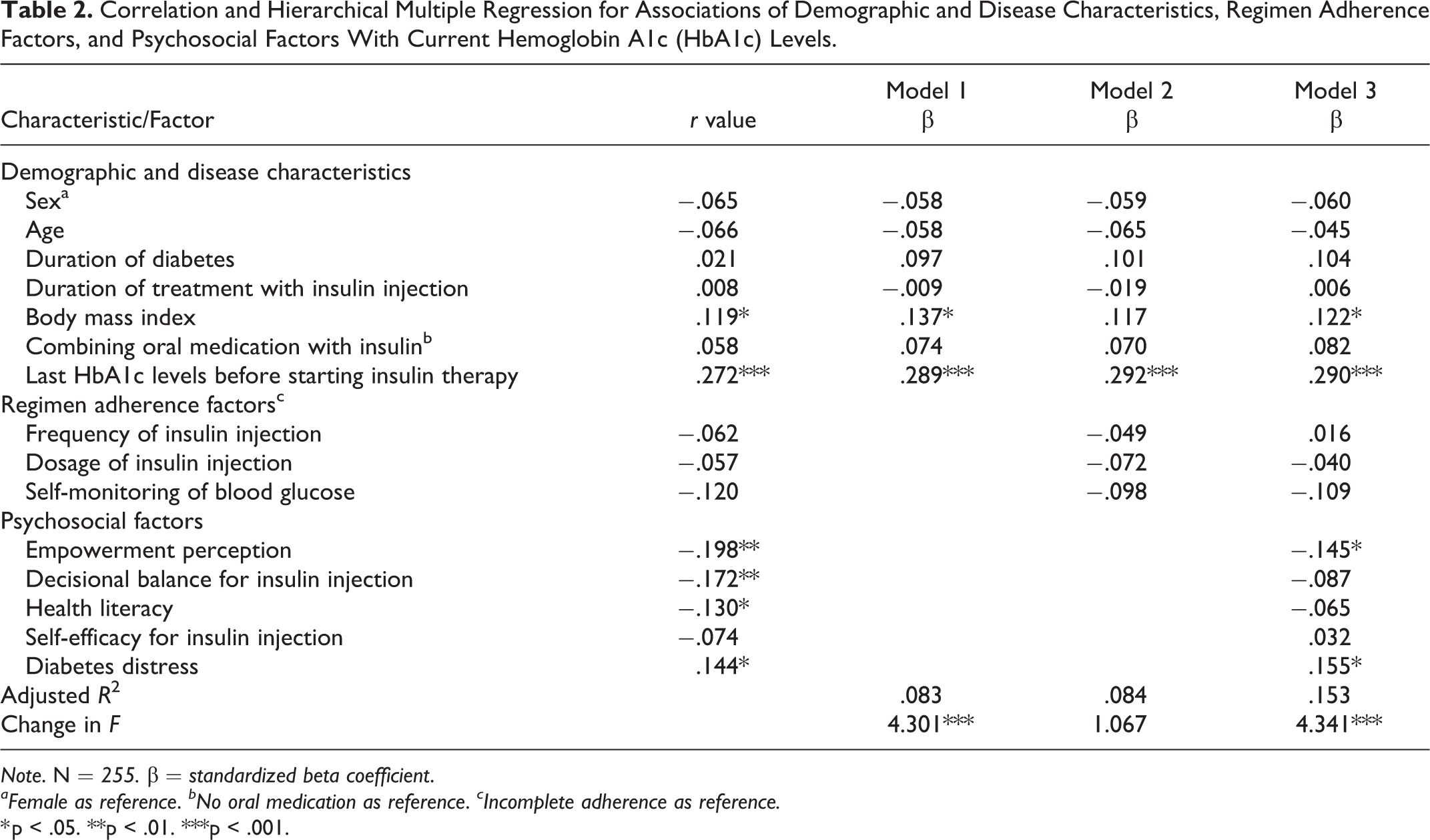
Note. N = 255. β = standardized beta coefficient.
aFemale as reference. bNo oral medication as reference. cIncomplete adherence as reference.
* p < .05. **p < .01. ***p < .001.
The hierarchical multiple regression analyses that only included demographic and disease characteristics indicated that BMI and the last HbA1c levels before starting insulin therapy were significantly associated with current HbA1c levels (Model 1 of Table 2). After incorporation of regimen adherence factors, the hierarchical multiple regression analyses indicated that the last HbA1c level before starting insulin therapy was still significantly associated with current HbA1c levels. Adherence to insulin regimen and SMBG, however, was not significantly associated with current HbA1c levels (Model 2 of Table 2). We then added psychosocial factors including decisional balance for insulin injection, health literacy, self-efficacy for insulin injection, diabetes distress, and empowerment perceptions into the hierarchical multiple regression analysis. The results indicated that BMI and the last HbA1c level before starting insulin therapy were still significantly associated with current HbA1c levels as were empowerment perception and diabetes distress (Model 3 of Table 2). Increases by one unit in empowerment perception scores decreased current HbA1c levels by 0.145%, whereas increases by one unit in the diabetes distress score increased current HbA1c levels by 0.155%.
Discussion
In the present study, 83.5% of participants, all insulin-treated patients with diabetes, had current HbA1c levels ≥7%, the recommended cutoff for HbA1c control (ADA, 2018). This finding is similar to that of Angamo, Melese, and Ayen (2013), in which 81.7% of insulin-treated patients had HbA1c levels ≥7%. Around 73% of the participants in the present study combined oral medication with insulin to treat their diabetes, which was similar to the 73.8% that researchers reported in a previous study in Taiwan (Chen et al., 2015). Insulin combined with oral drug therapy based on glycemic control is the regimen that the ADA (2018) recommends for insulin-treated patients. Interestingly, combining oral medication with insulin was not significantly associated with current HbA1c level in the present study. By contrast, a previous study found that the number of oral agents insulin-treated patients was taking was significantly associated with whether their HbA1c levels were <7% (Lin et al., 2015). Thus, further studies would be useful that assessed the number of oral agents taken and explored the association with HbA1c levels in insulin-treated patients with T2DM.
Our findings in the present study revealed that the last HbA1c level measured before patients started insulin therapy was an important determinant of current HbA1c levels. The higher the last HbA1c level before starting insulin therapy, the higher the current HbA1c level. This finding supports previous research suggesting that beginning insulin therapy early, before glycemic control becomes poor, would lead to improved glycemic control after the start of insulin therapy compared to starting insulin therapy later (Hanefeld, Fleischmann, Schiffhorst, & Bramlage, 2014).
We also found that high BMI was an important determinant of current HbA1c levels among participants in the present study. Preventing overweight is always recommended for patients with T2DM regardless of their treatment status (ADA, 2018). Furthermore, insulin-treated patients with T2DM have an increased risk of weight gain (Tong et al., 2015). Health-care providers should thus continue to emphasize encouraging insulin-treated patients with T2DM to maintain a healthy weight.
Adherence to recommended insulin regimens, in terms of both frequency and dosage, was relatively high in participants in the present study compared with previous studies (Farsaei, Radfar, Heydari, Abbasi, & Qorbani, 2014; Mashitani et al., 2015), with around 85% reporting complete adherence. When adherence rate in a population is high, the impact of adherence behaviors on HbA1c levels is less significant (DiBonaventura et al., 2014). This phenomenon might explain why insulin regimen adherence for frequency and dosage of injection was not significantly associated with current HbA1c levels in the present study. By contrast, only 50.2% of participants completely adhered to SMBG in the present study. The fact that glucose test strips are not covered by national health insurance in Taiwan might lead to low adherence to SMBG in insulin-treated patients. However, in the present study, adherence to SMBG was not significantly associated with current HbA1c levels, a finding that is consistent with that of Charity et al. (2016) in a previous study. This finding might be explained because performing SMBG does not necessarily lead to taking effective actions to improve glycemic control. Further studies are needed to confirm this hypothesis. In addition, we assessed regimen adherence by self-report, which might not accurately reflect adherence behaviors. Combining self-report with more objective measures such as the Medication Adherence Scale (Morisky, Ang, Krousel-Wood, & Ward, 2008) might allow future investigators to more accurately assess the regimen adherence of insulin-treated patients with T2DM.
Levels of diabetes distress were not high in the present study. Nevertheless, according to our analysis, diabetes distress was a stronger determinant of current HbA1c levels than decisional balance for insulin injection, health literacy, and self-efficacy for insulin injection. This finding was similar to that of a previous study (Linetzky et al., 2017). In another study, increasing psychological distress stimulated the release of hormones and, subsequently, increased HbA1c levels (Ely, Zavaskis, & Wilson, 2011). In a qualitative study, investigators also suggested that emotional hurdles might result in the adoption of unhealthy eating habits, which would, ultimately, lead to poor glycemic control (Tong et al., 2015). Although the specific mechanism underlying the association between diabetes distress and HbA1c levels has not been identified, health-care providers should be mindful of the negative effects of diabetes distress on HbA1c levels when caring for insulin-treated patients with T2DM.
Few studies have assessed the association of provider–patient interaction with HbA1c levels in insulin-treated patients. In the present study, we found empowerment perception to be a significant determinant of current HbA1c levels. In the patriarchal authoritarian-obedient societies of Asian countries such as Taiwan, health-care providers often request patients to follow specific regimens. Nevertheless, the insulin regimen might not be feasible or fit into the daily activities of insulin-treated patients. Insulin-treated patients who feel highly empowered by health-care providers might have an increased sense of control of their diabetes and, consequently, might become more actively involved in disease management, resulting in decreased HbA1c levels. This finding suggests that an empowerment approach to health care, as opposed to an authoritative obedience approach, might improve glycemic control in insulin-treated patients with T2DM.
The mean score of decisional balance for insulin injection was positive in the present study, indicating that participants’ perceptions of pros outweighed their perceptions of the cons of insulin injection. Results of the bivariate analysis indicate that the more the pros outweighed the cons of insulin injection, the better the glycemic control. To our knowledge, this study is the first to present evidence supporting decisional balance of insulin injection as being significantly associated with HbA1c levels in insulin-treated patients with T2DM. More studies are needed to confirm the finding. Although decisional balance did not remain a significant determinant of HbA1c levels when we controlled for other psychosocial factors, we nevertheless suggest that health-care providers should consider that emphasizing the pros of insulin injection while helping patients to minimize the cons might help to improve glycemic control in insulin-treated patients with T2DM.
Few studies have examined the association of health literacy with HbA1c levels specifically in insulin-treated patients. In the present study, our bivariate analysis indicated that health literacy was significantly associated with current HbA1c levels, though subsequent analyses found that health literacy was not a significant determinant of current HbA1c levels. It may be that health literacy is a precedent of self-efficacy or decisional balance for insulin injection (Lee et al., 2016) that health literacy, itself, was not as salient with a factor for HbA1c levels in insulin-treated patients with T2DM. To our surprise, self-efficacy for insulin injection was not significantly associated with current HbA1c levels in the present study. One explanation for this finding may be that, because the participants in this study had been performing insulin injection for a mean of more than 5 years, their self-efficacy for insulin injection might be relatively high, thus reducing its importance as a factor in the determination of current HbA1c levels.
There were a number of limitations in the present study. Comorbid conditions such as hypertension or dyslipidemia that require beta blocker or statins for control might affect HbA1c levels. We did not collect data on these conditions. Future researchers should collect data on comorbid conditions and assess their association with HbA1c levels. We recruited participants from two clinics in Taiwan by convenience sampling, and some measurements were self-reported. The self-selection effect could lead to values for certain factors, such as regimen adherence, empowerment perception, and self-efficacy for insulin injection, that are not representative of the larger population of insulin-treated patients with T2DM. Recruitment of insulin-treated patients with T2DM from diverse hospitals or countries using random sampling would help to address this issue in future studies. Finally, because of the cross-sectional design, we cannot confirm causal relationships between significant determinants and HbA1c levels. Longitudinal and experimental studies are needed to further explore the causal relationships and mechanisms of action between diabetes distress and empowerment perceptions and HbA1c levels in insulin-treated patients with T2DM.
Conclusions
Few studies have comprehensively examined the determinants of glycemic control among demographic and disease characteristics, regimen adherence factors, and psychosocial factors specifically in Asian insulin-treated patients with T2DM. Findings of the present study provide evidence that will be useful for nurses designing intervention programs to improve glycemic control among these patients. In particular, we found that psychosocial factors, but not insulin-regimen adherence factors, were significantly associated with HbA1c levels. Given that regimen adherence was relatively strong in the present study, we might preliminarily conclude that psychosocial factors are important determinants of glycemic control in insulin-treated patients with T2DM when adherence to insulin-treatment regimens is relatively strong. Due to the potential bias inherent in the self-report measure used to assess insulin-adherence behaviors, however, additional research is needed to confirm this conclusion.
Nevertheless, our findings suggest that nurses should be cognizant of the potential effects of psychosocial factors on glycemic control and provide needed intervention for insulin-treated patients who are compliant with the treatment plan but are still struggling with glycemic control. Empowerment perception and diabetes distress were both significant determinants of HbA1c levels in the present study; thus, nurses might focus on reducing diabetes distress and practicing an empowering approach to the patient–provider relationship to improve glycemic control in insulin-treated patients. For example, nurses could periodically assess the diabetes distress of insulin-treated patients with T2DM and refer them to mental health professionals when needed. Furthermore, applying empowerment approaches such as enhancing self-awareness of improved glycemic control and sharing more decision-making power with insulin-treated patients with T2DM could be beneficial.
Compliance With Ethical Standards
This study was conducted according to the principles of the Declaration of Helsinki and the International Committee on the Harmonization of Good Clinical Practices. The protocol was approved by each study site’s IRB, and patients provided written informed consent prior to the conduct of any study-related procedures.
Footnotes
Author Contributions
Shi-Yu Chen designed the study, collected data, wrote the manuscript and reviewed/edited the manuscript. Hui-Chun Hsu collected data, assisted with writing the manuscript, and reviewed/edited the manuscript. Ruey-Hsia Wang designed the study, analyzed data, wrote the manuscript, and reviewed/edited the manuscript. Yau-Jiunn Lee collected data, assisted with writing the manuscript, and reviewed/edited the manuscript. Chang-Hsun Hsieh assisted with data collection and data analysis and edited the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Ministry of Science and Technology, Taiwan (MOST-105-2314-B-037-060-MY3).