
Abstract
Objectives:
The aim of this study was to investigate thrombosis-related parameters (blood coagulation parameters, platelet indices, red blood cell [RBC] count, and inflammatory markers) in patients with fibromyalgia (FM).
Method:
We carried out a case–control study with 35 women with FM and 12 age-matched healthy volunteers to analyze fibrinogen levels, prothrombin time, cephaline time, platelet count, platelet distribution width (PDW), mean platelet volume (MPV), RBC count, neutrophil-to-lymphocyte ratio, and platelet-to-lymphocyte ratio (PLR).
Results:
The results showed significantly increased fibrinogen levels (p < .05), platelet count (p < .05), PDW (p = .059), RBC count (p < .05), and PLR (p < .05) in women with FM versus the healthy volunteers. Prothrombin time (p < .05) and MPV (p < .05) were significantly lower in patients with FM than in the controls.
Conclusions:
Elevated platelet and RBC counts, PDW values, and fibrinogen levels as well as decreased prothrombin time are all indicative of a prothrombotic state in FM patients, which may be enhanced by an increased inflammatory tone. This prothrombotic state may increase the risk of thrombosis-related cardiovascular disease in patients with FM.
Fibromyalgia (FM) is a chronic and complex syndrome characterized by widespread musculoskeletal pain and numerous other symptoms including fatigue, nonrestorative sleep, depression, and anxiety. Diagnosis is difficult and frequently missed because the symptoms are vague and generalized. Despite intensive research, the etiopathogenesis of FM has yet to be clarified.
A prior study by our research group in patients with FM showed increased levels of C-reactive protein (CRP) and apolipoprotein B, two biomarkers linked to cardiovascular events, which suggests that these patients may be at increased risk of cardiovascular disease (Rus et al., 2016). Thrombus formation is closely related to the development of several cardiovascular diseases (reviewed in Pifarré, 1998). Whereas arterial thrombi, formed following platelet activation, consist of an aggregate of fibrin and platelets, venous thrombi have a high red blood cell (RBC) and fibrin content (Aleman, Walton, Byrnes, & Wolberg, 2014). Fibrinogen, a soluble protein of the blood plasma, is the precursor of fibrin by the action of the protease thrombin. Prothrombin is proteolytically cleaved to form thrombin. Prothrombin time is the time it takes plasma to clot. It is used to evaluate the integrity of the coagulation pathway. The association between fibrinogen levels and the risk of cardiovascular disease has long been known (Maresca, Di Blasio, Marchioli, & Di Minno, 1999). The platelet indices such as platelet count, platelet distribution width (PDW), and mean platelet volume (MPV) are determinants of platelet activation and are associated with arterial thrombosis-related cardiovascular diseases (Aktürk & Büyükavci, 2017; Milovanovic, Nilsson, Haakara, Post, & Gerdle, 2016). Abnormalities in RBC number and/or function have been associated with venous thrombosis risk (Aleman et al., 2014). Inflammation can enhance arterial and venous thrombus formation (Fuchs et al., 2010) through promotion of the release of neutrophil extracellular traps (NETs), which are extracellular DNA fibers composed of histones and neutrophil antimicrobial proteins (Brinkmann & Zychlinsky, 2007). NETs provide a stimulus and scaffold for thrombus formation by promoting platelet activation and fibrin deposition and by recruiting RBCs (Fuchs et al., 2010).
Although patients with FM may be at increased risk of cardiovascular disease, little is known about the risk of thrombosis in these patients. Therefore, the aim of the present study was to investigate thrombosis-related parameters in FM patients, including blood–coagulation parameters, platelet indices, and RBC count. The few previous studies conducted in this area have reported conflicting results regarding these parameters in patients with FM in comparison to healthy subjects (Aktürk & Büyükavci, 2017; Alves et al., 2016; Arihan, Caglayan, Bayrak, Akinci, & Falkmarken, 2017; Berg, Berg, Couvaras, & Harrison, 1999; Elmas et al., 2016; Haliloğlu, Carlioglu, Sahiner, Karaaslan, & Kosar, 2014; Milovanovic et al., 2016). Given the association between thrombosis and inflammation, we also evaluated the inflammatory markers neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR; Uslu et al., 2015) as thrombosis-related parameters. We assessed correlations to determine whether these parameters influence FM-related clinical characteristics. Finally, to facilitate the diagnosis of FM, we determined the predictive value of thrombosis-related markers by receiver operating characteristic (ROC) analysis. FM is multifactorial, and each study contributes to our understanding of its pathophysiology, so that we are able to more effectively diagnose and manage this syndrome.
Method
Participants
We carried out this research in accordance with the Declaration of Helsinki (2008) of the World Medical Association. The Ethics Committee of the University of Jaén (Spain) approved the study. All participants provided written informed consent. We used the same cohort of FM patients and controls who had participated in a previous study (Rus, Molina, Del Moral, Ramírez-Expósito, & Martínez-Martos, 2018). Participants in the present case–control study included 35 female patients diagnosed with FM, whom we contacted via AFIXA (Association of Fibromyalgia of Jaén, Spain), and 12 age-matched healthy women whom we recruited from the University of Jaén (Spain).
The inclusion criterion for the women with FM was that their symptoms were in compliance with the 1990 American College of Rheumatology criteria for the classification of primary FM. Exclusion criteria, both for patients and for controls, were the presence of any other chronic disease (diabetes mellitus, hypertension, cancer, or ischemic heart disease), pregnancy, lactation, or Grade II obesity (body mass index ≥ 35 kg/m2). None of the participants were being treated with anticoagulants, corticosteroids, estrogens, analgesics, or anti-inflammatory drugs at the time of and for at least 2 months before the start of the study. None consumed alcohol regularly, and all were nonsmokers and sedentary.
Clinical Characteristics of Participants
We obtained demographic and clinical data from the participants by means of interviews and questionnaires. The same specialist carried out all the measurements and tests throughout the study. In patients with FM, we evaluated functional capacity in activities of daily living using the Spanish version of the Fibromyalgia Impact Questionnaire (FIQ; Rivera & González, 2004). The FIQ is the instrument most often used to estimate FM severity, and the score ranges from 0 to 100. To evaluate musculoskeletal pain in patients with FM, we used a Visual Analogue Scale (10 cm). For both questionnaires, higher values reflect worse symptomatology. We evaluated the physical (Physical Component Summary [PCS-12]) and mental (Mental Component Summary [MCS-12]) health status of patients and controls using the Spanish version of the 12-item Short-Form Health Survey (SF-12; Alonso, Prieto, & Anto, 1995). The SF-12 and both subscales have total possible scores ranging from 0 to 100, with lower values reflecting a poorer health status.
Blood Collection and Preparation of Blood Samples
After participants fasted overnight, we drew venous blood in the early morning from the antecubital vein into two tubes with anticoagulant. The tubes were centrifuged at 3,500 rpm for 5 min at 4°C to obtain plasma samples.
Laboratory Tests
We determined blood-coagulation parameters (fibrinogen levels, prothrombin time, and cephaline time) in plasma samples of patients and controls using the BCS XP analyzer (Siemens Healthineers, Erlangen, Germany). We measured determinants of platelet function (platelet count, MPV, and PDW) and RBC, neutrophil, and lymphocyte counts in plasma samples by flow cytometry using the ADVIA 2120 analyzer (Siemens Healthineers, Erlangen, Germany).
Statistical Analysis
Data management and analysis were performed using IBM SPSS Statistics 24 for Windows (SPSS Inc., Chicago, IL). We express data for continuous variables as mean ± standard deviation. The Kolmogorov–Smirnov test (α value = .05) and Levene test (α value = .05) were performed to test normality and homoscedasticity, respectively. For data that followed a normal distribution and the principle of homoscedasticity of variances, we used an unpaired Student’s t test to compare differences between means. For data that did not follow a normal distribution or the principle of homoscedasticity, we established the degree of statistical significance by applying the Mann–Whitney U test (prothrombin time, cephaline time, platelet count, PDW, RBC count, and PLR). We calculated the effect size using Pearson’s correlation coefficient. Values of .10, .30, and .50 were assumed to correspond to small, moderate, and large effect sizes, respectively. An effect size with a positive sign indicates that the parameter values were lower in the patients with FM than in the controls. Alternatively, an effect size with a negative sign indicates that the parameter values were higher in the women with FM than in the healthy women. To assess the correlations between variables, we used Pearson’s and Spearman’s correlation coefficients as parametric and nonparametric measures of rank correlation, respectively. For the ROC analysis, we used MedCalc Statistical Software (version 13.3.0.0) to calculate the area under the curve (AUC), the cutoff point, positive and negative predictive values (PV+ and PV−, respectively), and sensitivity and specificity. Specifically, we used the Youden index to determine the cutoff point of the variable in the ROC curve (Youden, 1950). We set the level of statistical significance at p < .05.
Results
We drew the demographic and clinical characteristics of the participants from Rus, Molina, Del Moral, Ramírez-Expósito, and Martínez-Martos (2018). There were no statistically significant differences between the study groups by age (50 ± 8.28 years for the controls and 52.34 ± 7.82 years for the FM patients) or body mass index (24.07 ± 3.05 kg/m2 for the controls and 26.14 ± 3.48 kg/m2 for the FM patients). Table 1, which presents the clinical characteristics of the participants, shows that the PCS-12 and the MCS-12 scores of the women with FM were significantly lower than those of the controls (both p < .05). The PCS-12 showed a large effect size and the MCS-12 a moderate one.
Clinical Characteristics of Patients and Controls.
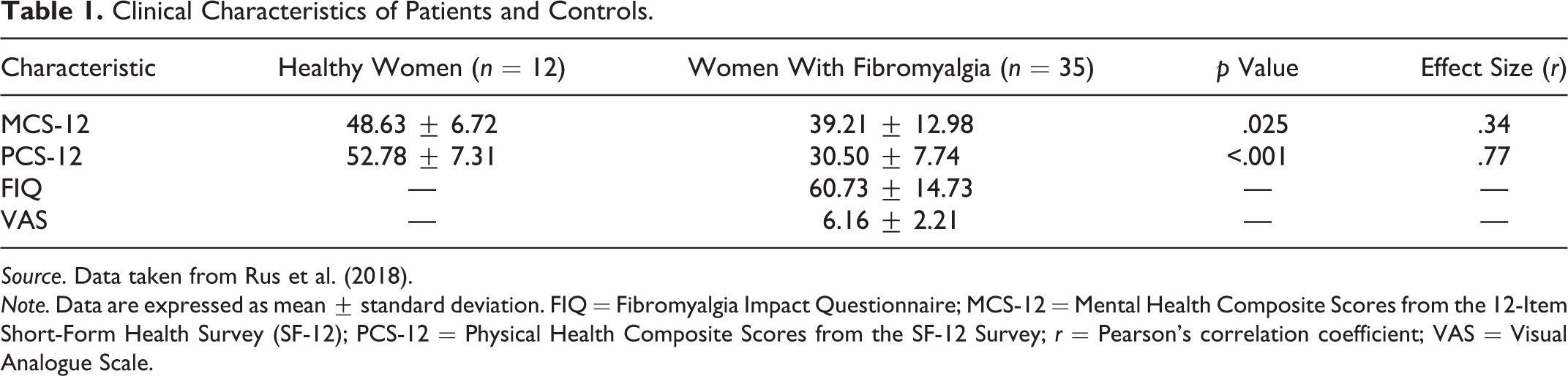
Source. Data taken from Rus et al. (2018).
Note. Data are expressed as mean ± standard deviation. FIQ = Fibromyalgia Impact Questionnaire; MCS-12 = Mental Health Composite Scores from the 12-Item Short-Form Health Survey (SF-12); PCS-12 = Physical Health Composite Scores from the SF-12 Survey; r = Pearson’s correlation coefficient; VAS = Visual Analogue Scale.
Table 2 summarizes the results obtained for the laboratory parameters. The FM patients showed significantly higher fibrinogen levels (p < .05) and lower prothrombin time (p < .05) than the controls. Cephaline time remained unchanged in women with FM in comparison to healthy volunteers. The women with FM had a significantly higher platelet count (p < .05) and lower MPV values (p < .05) than the healthy women. PDW values were higher in the patients with FM than in the controls, and the difference approached statistical significance (p = .059). There were also significantly higher values for RBC count (p < .05) and PLR (p < .05) in the women with FM than in the healthy women. NLR was similar in patients and controls. All the laboratory parameters showed a moderate effect size, except for MPV (large effect size), cephaline time (small effect size), and NLR (small effect size).
Results of the Laboratory Parameters in Patients and Controls.
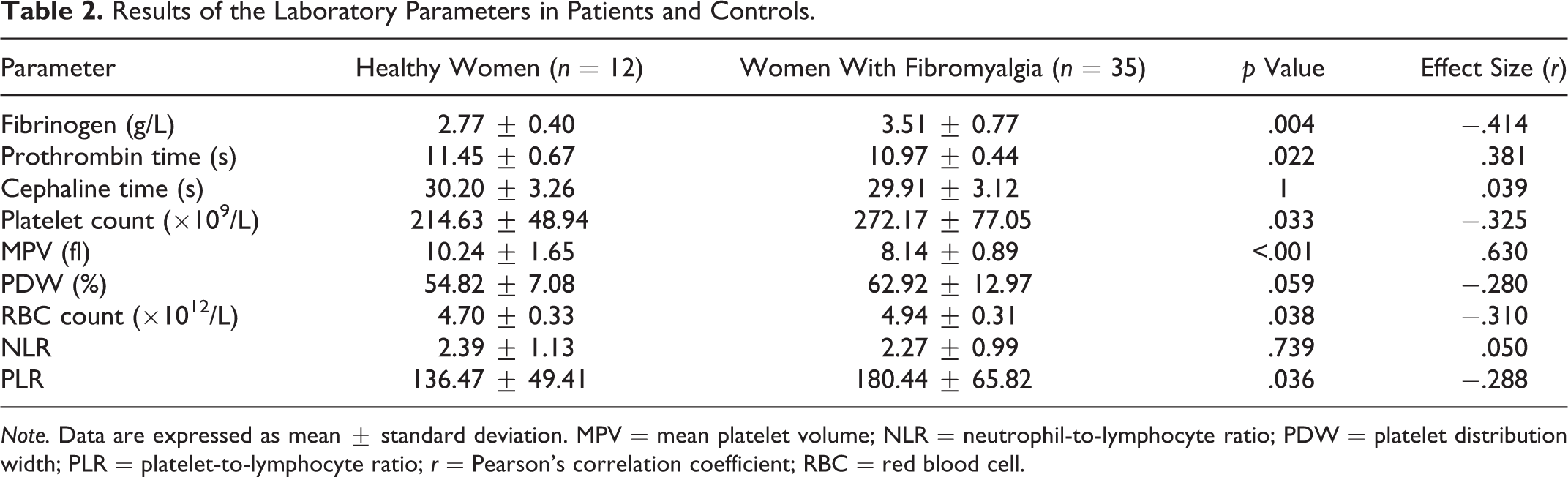
Note. Data are expressed as mean ± standard deviation. MPV = mean platelet volume; NLR = neutrophil-to-lymphocyte ratio; PDW = platelet distribution width; PLR = platelet-to-lymphocyte ratio; r = Pearson’s correlation coefficient; RBC = red blood cell.
There were no statistically significant correlations between laboratory parameters and clinical features in patients with FM. However, the correlations of fibrinogen with severity of FM determined by the FIQ, and with mental health status, assessed by the MCS-12, and approached statistical significance (p < .10). Fibrinogen levels correlated positively with the FIQ score (Pearson’s correlation coefficient, r = .287; p = .099) and negatively with the MCS-12 (r = −.311; p = .073) in the women with FM.
Figure 1 shows the ROC curves for the parameters with a statistically significant AUC (fibrinogen, prothrombin time, platelet count, MPV, PDW, RBC count, and PLR). Table 3 shows the AUC, p value, cutoff point, sensitivity, specificity, PV+, and PV− for these parameters. In our study, the higher the AUC value, the greater the capacity of a parameter to differentiate the patients with FM from the healthy subjects. Fibrinogen and MPV showed the highest AUC values. For example, Table 3 shows the data corresponding to the ROC curve for fibrinogen, including the cutoff point (>3.1 g/L), sensitivity (70.59%), specificity (81.82%), PV+ (8.7), and PV− (99.1). These data indicate that the probability of classifying a healthy person as such (fibrinogen levels ≤3.1 g/L) is greater than 99% with high sensitivity and specificity, which would rule out a diagnosis of FM. Likewise, almost 9% of persons with fibrinogen levels >3.1 g/L may be diagnosed with FM. Therefore, fibrinogen levels ≤3.1 g/L can be used as an excluding marker of a person having FM.
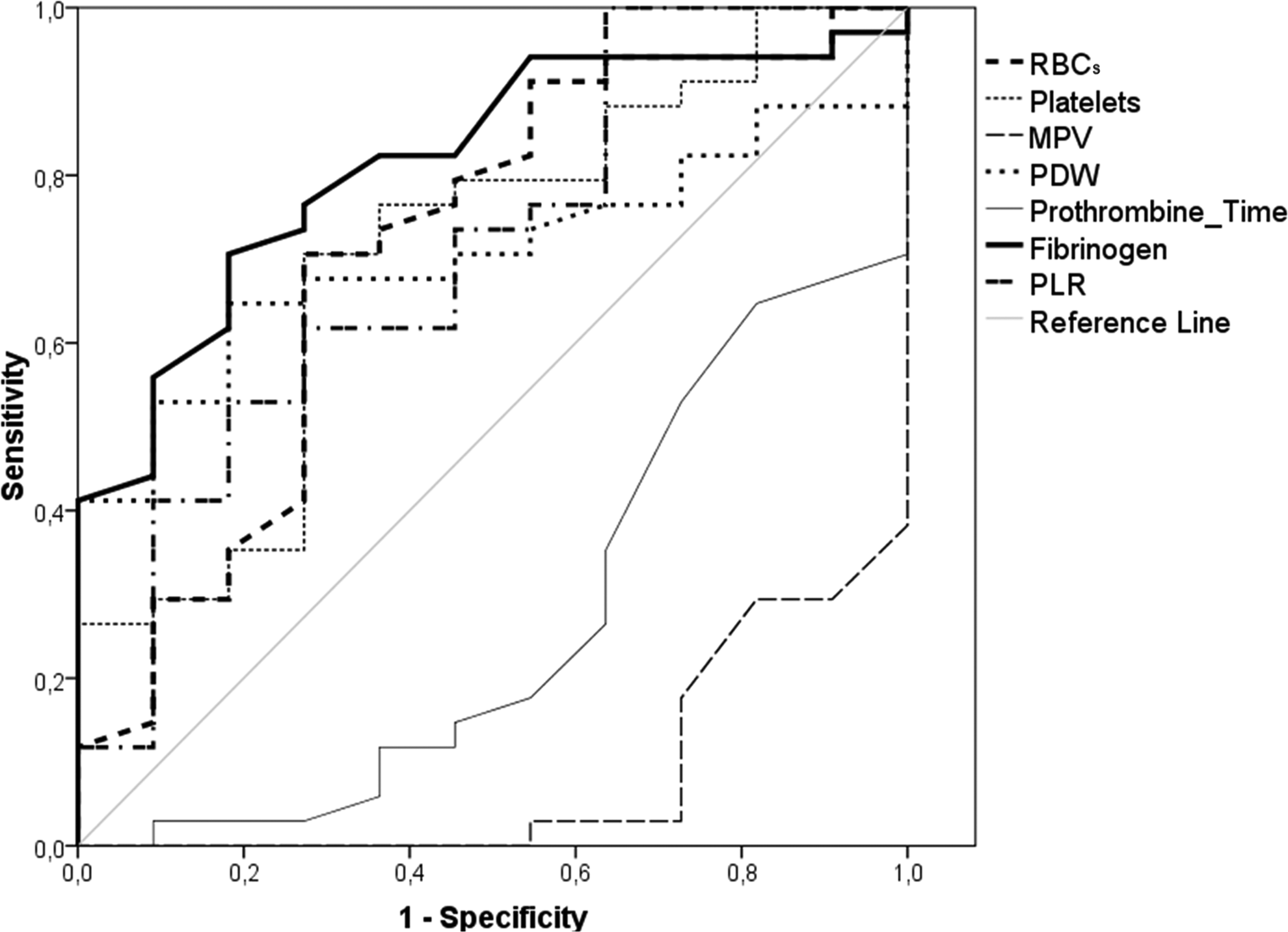
Receiver operating characteristic curves. RBCs = red blood cells; MPV = mean platelet volume; PDW = platelet distribution width; PLR = platelet-to-lymphocyte ratio.
Receiver Operating Characteristic Analysis.
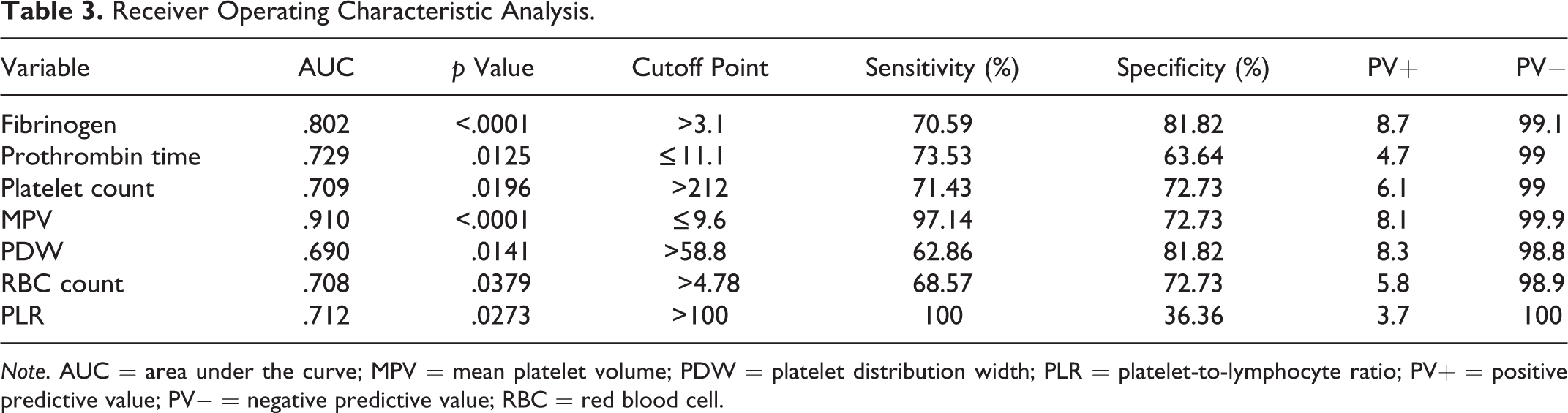
Note. AUC = area under the curve; MPV = mean platelet volume; PDW = platelet distribution width; PLR = platelet-to-lymphocyte ratio; PV+ = positive predictive value; PV− = negative predictive value; RBC = red blood cell.
Discussion
FM is a complex illness to treat due to its unclear etiology. Therefore, a better understanding of the underlying mechanisms of FM may enable health-care providers to more effectively manage this syndrome. In the present study, we investigated thrombosis-related parameters (blood-coagulation parameters, platelet indices, RBC count, and inflammatory markers) in FM patients. In addition, we assessed the correlations between these parameters and FM-related clinical features and determined the predictive value of thrombosis-related parameters in FM via ROC analysis.
Coagulation State
We observed a statistically significant increase in fibrinogen levels and a statistically significant decrease in prothrombin time in the women with FM compared to the healthy controls. Whereas elevated fibrinogen levels have been associated with a greater risk of cardiovascular disease (Maresca et al., 1999), a low prothrombin time suggests a higher risk of a clot developing. These results, therefore, suggest patients with FM may be in a procoagulant state, which may be related to an increased risk of thrombosis-related cardiovascular disease. These data agree with the findings of our previous study in the same cohort of women with FM. We found increased levels of two biomarkers linked to cardiovascular events (CRP and apolipoprotein B), which are also indicative of a greater risk of cardiovascular disease in these patients (Rus et al., 2016). Other researchers have found that chronic pain, the main symptom of FM patients, is associated with a higher prevalence of cardiovascular risk factors (Goodson et al., 2013). To the best of our knowledge, ours is the first study to measure the prothrombin time in patients with FM.
Furthermore, only two previous studies have analyzed fibrinogen levels in FM. One reported increased levels of fibrinogen in patients with chronic fatigue syndrome and/or FM (Berg et al., 1999), but the other detected no differences in fibrinogen levels between FM patients and controls (Arihan et al., 2017). In the present study, both parameters presented a moderate effect size, indicating that the differences we observed between the groups may be meaningful. We also assessed correlations between laboratory and clinical parameters in women with FM to investigate whether thrombosis-related parameters influenced FM clinical characteristics. The correlations only approached statistical significance (p < .10), but they might become statistically significant with a larger sample size. Thus, higher fibrinogen levels may be associated with greater severity of FM and with a poorer mental health status in our FM patients, suggesting that altered fibrinogen levels may be related to the physiopathology of FM.
Determinants of Platelet Activation
Our results showed that there was a statistically significant increase in platelet count and PDW values (in the latter case, the difference approached statistical significance with p = .059) and a statistically significant decrease in MPV in women with FM versus healthy women. Previous authors have reported that increased values of platelet count, MPV, and PDW constitute a risk factor for cardiovascular diseases (Aktürk & Büyükavci, 2017; Milovanovic et al., 2016). However, this finding contradicts that of Levin and Bessman (1983), who reported finding an inverse relationship between MPV and platelet count, as we observed in the FM patients in our study. In this regard, PDW is considered a more specific marker of platelet activity than MPV because it does not increase during simple platelet swelling (Vagdatli et al., 2010). Our results of elevated platelet count and PDW value may indicate a platelet hyperactivation that could contribute to the prothrombotic state of FM patients. Oxidative stress promotes platelet hyperactivation and, consequently, increases the risk of arterial thrombosis (reviewed in Santhakumar, Bulmer, & Singh, 2014). In a previous study, we found that oxidative stress was increased in FM patients (La Rubia, Rus, Molina, & Del Moral, 2013). Our results, all told, suggest that patients with FM may have a tendency to a prothrombotic state, to which oxidative stress may contribute.
Previous research into platelet indices in patients with FM has produced conflicting findings. Some studies concur with our results, recording higher platelet counts in FM patients than in healthy subjects (Elmas et al., 2016). Others, however, have found no significant differences (Alves et al., 2016; Arihan et al., 2017; Haliloğlu et al., 2014). Researchers have also reported elevated platelet activity in patients with FM (Milovanovic et al., 2016) and with chronic fatigue syndrome and/or FM versus healthy subjects (Berg et al., 1999). Contrary to our results, several studies have found that patients with FM had higher MPV (Arihan et al., 2017; Haliloğlu et al., 2014) and lower PDW values (Arihan et al., 2017) than healthy subjects. In the present study, platelet count and PDW showed a moderate effect size and MPV a large effect size, indicating that the differences between the groups may be significant. These conflicting results may be due to the characteristics of the study groups considered (women with FM vs. controls). Not all studies employ the same inclusion and exclusion criteria to select participants. Moreover, patients with FM usually have many comorbidities, which could explain the diversity of results obtained in these studies.
RBC Count
Because fibrinogen and RBC count are both determinants of venous thrombosis risk (Aleman et al., 2014), we also examined RBC count. In women with FM, we found a statistically significant increase in RBC count, which presented a moderate effect size. On the other hand, some previous authors have not found differences in RBC count between FM patients and healthy subjects (Arihan et al., 2017). The increased RBC count and fibrinogen levels we observed in our patients with FM may promote the formation of venous thrombi, which is associated with a higher risk of venous thrombosis. Moreover, patients with FM present alterations in the shape of RBCs, with a higher percentage of flat cells rather than the normal biconcave ones. Flat cells are less deformable, and therefore the rate of capillary blood flow is reduced, suggesting that the use of anticoagulants could be beneficial in these patients (Simpson & O’Neill, 2001). This finding supports our result of a procoagulant state in patients diagnosed with FM.
Inflammatory Markers
An inflammatory state may promote the release of NETs, which are strongly thrombogenic (Brinkmann & Zychlinsky, 2007; Fuchs et al., 2010). Therefore, in the present study, we also evaluated the inflammatory markers NLR and PLR in patients diagnosed with FM. While we did find a statistically significant increase in PLR in the women with FM, NLR remained unchanged. PLR showed a moderate effect size and NLR a small effect size. To the best of our knowledge, ours is the first study to investigate PLR in patients with FM. Contrasting with our results, other authors found higher NLR in FM patients than in the control group (Aktürk & Büyükavci, 2017). In agreement with the elevated values of the inflammatory marker PLR that we found in our patients, investigators have previously described an inflammatory state in patients with FM (Bote, Garcia, Hinchado, & Ortega, 2013). Supporting this finding, we found increased levels of CRP, an acute phase reagent related to inflammatory processes, in a previous study in women with FM (Rus et al., 2016). However, in the same work, we found no significant differences in the levels of two interleukins (6 and 10) between patients with FM and controls. Although in our patients with FM not all the inflammatory markers analyzed were altered, our assumption is that not all will necessarily be increased during an inflammatory process. Therefore, the prothrombotic state we found in FM patients may be enhanced by an increased inflammatory tone. On the other hand, reactive oxygen species are required for NET formation (Brinkmann & Zychlinsky, 2007). Consequently, an increase in oxidative stress, which we found in FM patients in a previous study, may contribute to the prothrombotic state of these patients (La Rubia et al., 2013).
ROC Analysis
The syndrome of FM presents difficulties for diagnosis. Therefore, we also investigated the predictive value of thrombosis-related parameters in FM via ROC analysis. Our results showed that the determination of fibrinogen level, prothrombin time, platelet count, MPV, PDW, RBC count, and PLR may assist in making the FM diagnosis. In particular, these parameters may be useful as excluding markers of the presence of FM; that is, they may be used to classify healthy people as such with a probability of nearly 99% (see Table 3).
Limitations
The main limitation of this study is the small sample size. Consequently, we recommend that additional studies with larger numbers of participants should be undertaken to verify the present findings. Nevertheless, all the parameters that showed statistically significant differences between the FM patients and the controls presented moderate and large effect sizes, indicating that the differences observed between the groups may be meaningful regardless of sample size.
Conclusions
Elevated platelet and RBC counts, PDW values, and fibrinogen levels as well as decreased prothrombin time are all suggestive of a prothrombotic state in FM patients, which may be enhanced by an increased inflammatory tone. This prothrombotic state may lead to increased cardiovascular risk in these patients, making it advisable to perform a follow-up of FM patients for the early detection of cardiovascular diseases. Moreover, the determination of these parameters may be an uncomplicated and inexpensive means of improving the diagnosis of FM.
These results contribute to the knowledge base of nursing science. Moreover, they can help improve the guidelines for the care of patients with FM, for example, by giving recommendations for the prevention/early detection of cardiovascular events, or for taking precautions if the administration of hemostatic drugs is necessary in a patient with FM or by highlighting the need for special care to be provided to bedridden FM patients who may be at even higher risk of thrombosis.
Footnotes
Acknowledgments
We wish to thank AFIXA (Association of Fibromyalgia of Jaén, Spain) for collaborating in this study.
Author Contributions
F. Molina contributed to conception, design, acquisition, analysis, and interpretation; critically revised the manuscript; gave final approval; and agreed to be accountable for all aspects of work ensuring integrity and accuracy. M. L. del Moral contributed to conception, design, acquisition, and interpretation; critically revised the manuscript; gave final approval; and agreed to be accountable for all aspects of work ensuring integrity and accuracy. M. La Rubia contributed to analysis and interpretation, drafted the manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy. S. Blanco contributed to acquisition, critically revised the manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy. R. Carmona contributed to conception, critically revised the manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy. A. Rus contributed to conception, design, acquisition, analysis, and interpretation; drafted the manuscript; critically revised the manuscript; gave final approval; and agreed to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work has been supported by Junta de Andalucía, Spain (AGR-6235).