
Abstract
Objectives:
Fibromyalgia (FM) is a chronic pain condition of unclear etiology. We have analyzed, for the first time, the activity of a broad spectrum of aminopeptidases (APs) in patients with FM and controls to investigate whether they are involved in the pathophysiology of this syndrome.
Method:
In this case–control study, we fluorometrically measured specific AP activities in serum samples of 75 patients with FM and 29 healthy controls. The predictive value of AP activities in FM was determined by receiver operating characteristic (ROC) analysis.
Results:
Oxytocinase activity was higher in patients with FM than in controls (p < .001). A subgroup of patients with FM (n = 18; 24%) showed low levels of enkephalin-degrading aminopeptidase (EDA) activity when compared with the healthy controls (p < .001) and with the rest of FM patients (p < .001). There were no significant differences in the activity levels of aminopeptidase A, aminopeptidase B, aspartyl aminopeptidase, insulin-regulated aminopeptidase, pyroglutamyl aminopeptidase, or aminopeptidase N between FM patients and controls. According to ROC analysis, oxytocinase activity may be a good marker for differentiating individuals with FM from healthy subjects.
Conclusions:
Our findings show that serum oxytocinase activity is increased in patients with FM, which could alter the metabolism of peptides with analgesic effects such as oxytocin and enkephalins. The determination of serum oxytocinase activity may aid in FM diagnosis. Additionally, we have identified a subpopulation of FM patients with abnormally low serum EDA activity.
Fibromyalgia (FM) is characterized by widespread pain and is often associated with fatigue, sleep disturbances, anxiety, and headache. It is present in as much as 2–8% of the population (reviewed in Clauw, 2014). FM shows different phenotypes and disease expression across patients and even within one patient over time. The etiology of FM remains unclear, although authors have proposed a number of factors that might be related. These factors include central sensitization (reviewed in Bellato et al., 2012), inflammation (Molina et al., 2019), and oxidative stress (La Rubia, Rus, Molina, & Del Moral, 2013). Due to the unknown nature of the pathophysiology of this syndrome, both precise FM diagnosis and effective treatment are elusive.
Aminopeptidases (APs) are zinc metalloenzymes that catalyze the cleavage of amino acids from the N-terminus of peptides and proteins. AP functions are related to the renin–angiotensin system (aminopeptidase A [APA], aminopeptidase B [APB], aspartyl aminopeptidase [ASAP], insulin-regulated aminopeptidase [IRAP]), oxytocin regulation (oxytocinase or cystinyl aminopeptidase), secretion of gonadal and thyroid hormones (pyroglutamyl aminopeptidase [PAP]), and enkephalins metabolism (aminopeptidase N [APN], enkephalin-degrading aminopeptidase [EDA]), among other systems and processes (Sánchez-Agesta Ortega et al., 2013). Research has found several APs to be related to the pathophysiology of a number of diseases such as hypertension, Alzheimer’s disease, cancer, and some immune-mediated inflammatory diseases (Larrinaga et al., 2013; Puertas et al., 2013; Sánchez-Agesta Ortega et al., 2013; reviewed in Schreiber & Smith, 2018; reviewed in Tran & Colbert, 2015).
The enkephalinases, such as EDA, degrade enkephalins, endogenous opioid pentapeptides with analgesic effects that are involved in regulating nociception. Enkephalins are also involved in the stress response and in emotional and behavioral processes such as anxiety and depression (reviewed in Henry, Gendron, Tremblay, & Drolet, 2017). Another type of enkephalinase is oxytocinase, an enzyme that metabolizes endogenous oxytocin and Met-enkephalin (reviewed in Tsujimoto & Hattori, 2005). Researchers have long recognized oxytocin for its role in reproduction and social behavior, but recent research has revealed it to also be an analgesic, anxiolytic, and anti-stress factor (reviewed in Neumann & Slattery, 2016; reviewed in Xin, Bai, & Liu, 2017).
Patients with FM have an altered perception of pain, presumably due to central nervous system (CNS) alterations (central sensitization; reviewed in Sluka & Clauw, 2016). Central sensitization is defined as increased response to stimulation mediated by CNS signaling. It is characterized by enhanced excitability of dorsal horn neurons, which leads to transmission of altered nociceptive information to the brain (reviewed in Stisi et al., 2008). A number of neurotransmitters and neuropeptides are likely involved in central sensitization in FM, including serotonin, norepinephrine, dopamine, substance P, endorphins, and enkephalins (reviewed in Bellato et al., 2012). Enkephalinases are related to nociception because they participate in the metabolism of enkephalins. Previous findings on levels of enkephalins in FM patients are conflicting. While several studies have reported increased Met-enkephalin levels in cerebrospinal fluid (CSF) from patients with FM in comparison to controls (Baraniuk, Whalen, Cunningham, & Clauw, 2004; Vaerøy, Nyberg, & Terenius, 1991), others have found decreased levels of Met-enkephalin in CSF from FM patients versus healthy subjects (Liu, Welin, Bragee, & Nyberg, 2000).
APs are implicated in the enzymatic activation and degradation of several biologically active peptides. Therefore, changes in their activity levels may modify the regulatory events in which such peptides are involved, which may ultimately result in a pathologic state. An alteration in the activity of enkephalinases, which participate in the metabolism of enkephalins, could hypothetically contribute to the altered nociception presented by patients with FM. To date, the activity of APs in patients with FM is completely unknown. Therefore, our aim in the present study was to investigate the specific activity of a broad spectrum of circulating APs in FM patients and healthy controls including APA, APB, ASAP, IRAP, oxytocinase, PAP, APN, and EDA. We also examined the ability of AP activities to differentiate individuals with FM from healthy subjects. Finally, we assessed correlations to determine whether AP activities influence FM-related clinical features.
Materials and Methods
Participants
We contacted patients with FM via both AGRAFIM (Association of Fibromyalgia of Granada, Spain) and AFIXA (Association of Fibromyalgia of Jaén, Spain) and recruited healthy subjects from friends and relatives of the patients, from friends and colleagues of the healthy subjects, and from the Faculty of Health Sciences staff (University of Granada, Spain). The patients had been previously diagnosed with FM by a professional rheumatologist and met the 1990 American College of Rheumatology criteria for FM (inclusion criterion). Exclusion criteria, both for patients and for controls, were the presence of any other chronic disease (diabetes mellitus, hypertension, cancer, or ischemic heart disease), pregnancy, and lactation. None of the participants were being treated with enkephalinase or oxytocinase inhibitors, opioid receptor agonists or antagonists (morphine, tramadol, oxycodone, naltrexone, etc.), anticoagulants, corticosteroids, or estrogens. We conducted this research in accordance with the provisions of the Declaration of Helsinki of the World Medical Association. The Ethics Committee of the University of Granada (Spain) approved this study, and 11 participants provided written informed consent.
Measures
Potential participants visited our laboratory at the Faculty of Health Science of the Universities of Granada and Jaén (Spain) to provide demographic and clinical data. We selected participants for the FM and control groups based on these data and the inclusion and exclusion criteria. Selected participants returned for a second visit, at which time we collected blood samples, and the participants completed several questionnaires. FM patients and healthy controls completed all questionnaires with the exception of the Revised Fibromyalgia Impact Questionnaire (FIQ-R), which only the patients completed.
We evaluated the severity of FM using the Spanish version of the FIQ-R, which has an internal consistency (Cronbach’s α) of .91 (Salgueiro et al., 2013). The questionnaire consists of 21 items; total scores range from 0 to 100. We measured self-reported musculoskeletal pain using a Visual Analog Scale (VAS), whose score ranged from 0 to 100. We used the Spanish version of the Multidimensional Fatigue Inventory (MFI; Munguía-Izquierdo et al., 2012) to assess fatigue. This instrument consists of 20 items and has a potential score range of 20–100. The Spanish version of the MFI has shown high internal consistency, with a Cronbach’s α of .93 (Soriano-Maldonado et al., 2015). To evaluate the psychological aspects and common symptoms of anxiety, we used a Spanish version of the Beck Anxiety Inventory (BAI; Sanz & Navarro, 2003), which has a Cronbach’s α of .93 (Magán, Sanz, & García-Vera, 2008). The BAI consists of 21 items, and scores range from 0 to 63. We assessed sleep quality using the Spanish version of the Pittsburgh Sleep Quality Index (PSQI), which has an internal consistency (Cronbach’s α) of .805 (Hita-Contreras et al., 2014). The questionnaire consists of 24 items, and total score ranges from 0 to 21. For all of these questionnaires, higher values reflect worse symptomatology.
Blood Collection
We drew blood from all participants at the same time of day to avoid circadian variations. Venous blood was taken from the antecubital vein into an anticoagulant-free tube. Blood was allowed to clot for 30 min at room temperature and then centrifuged at 3,500 rpm for 5 min at 4 °C to obtain serum samples.
AP Activity Assays
We measured specific AP activities fluorometrically in triplicate in serum samples using the corresponding aminoacyl-β-naphthylamides as substrates. Next, we identified each AP by the Enzyme Commission number (EC number), a numerical classification scheme for enzymes based on the chemical reactions they catalyze. Activities of APA (EC. 3.4.11.7), APN (EC. 3.4.11.2), APB (EC. 3.4.11.6), and ASAP (EC. 3.4.11.21) were measured using glutamyl-β-naphthylamide, alanyl-β-naphthylamide, arginyl-β-naphthylamide, and aspartyl-β-naphthylamide, respectively, as the substrates following the method previously described by our research group (Ramirez-Expósito et al., 2012). Activities of IRAP (EC. 3.4.11.3), EDA (EC. 3.4.24.11), oxytocinase (EC. 3.4.11.3), and PAP (EC. 3.4.19.6) were measured using leucyl-β-naphthylamide, tyrosyl-β-naphthylamide, cystyl-β-naphthylamide, and pyroglutamyl-β-naphthylamide, respectively, as the substrates according to the methods we described previously (Arrazola-Saniger et al., 2011; Carrera et al., 2004; Carrera-Gonzalez et al., 2012; Garcia-Lopez, Martínez-Martos, Mayas, Carrera, & Ramirez-Expósito, 2003). All reactions were stopped by adding 100 µL of .1-M acetate buffer, pH 4.2. The amount of aminoacyl-β-naphthylamine released as a result of the enzymatic activities was measured fluorometrically at 412-nm emission wavelength with an excitation wavelength of 345 nm. Proteins were quantified in triplicate via the Bradford method (Bradford, 1976), using bovine serum albumin as standard. Specific enzyme activities were expressed as picomoles of the corresponding aminoacyl-β-naphthylamide hydrolyzed per minute per milligram protein, using a standard curve prepared with the latter compound under corresponding assay conditions.
Statistical Analysis
We have expressed data for continuous variables as mean ± standard deviation (SD). To perform the statistical analysis of the data, we used the statistical package IBM SPSS Statistics Version 24 for Windows (SPSS Inc., Chicago, IL). We performed the Kolmogorov–Smirnov test (α value = .05) and Levene’s test (α value = .05) to test for normality and homoscedasticity, respectively. We tested data that followed a normal distribution and the principle of homoscedasticity of variances using an unpaired Student’s t test to compare differences between means (IRAP, APN, oxytocinase, BAI, age, body mass index). To establish the degree of statistical significance in data that did not follow a normal distribution or the principle of homoscedasticity, we applied the Mann–Whitney U test. We calculated the effect size using Cohen’s d for parametric tests and the eta squared (η2) for nonparametric tests. Values of Cohen’s d of .2, .5, and .8 correspond to the classical Cohen bands of interpretation of the effect size as small, medium, and large, respectively. Values of η2 of .02, .13, and .26 correspond to small, medium, and large effect sizes, respectively. To assess relationships between variables, we used Pearson’s and Spearman’s correlation coefficients as parametric and nonparametric measures of rank correlation, respectively. For the receiver operating characteristic (ROC) curve analysis, we used MedCalc Statistical Software (version 13.3.0.0) to calculate area under the curve (AUC), cutoff point, positive and negative predictive values (PV+ and PV−, respectively), sensitivity, and specificity. To determine the cutoff point of the variable in the ROC curve, we used the Youden (1950) index. We set the level of statistical significance at p < .05.
Results
Participants
We show the demographic and clinical data of the participants in Table 1. A total of 128 patients and controls voluntarily enrolled in the study, and we selected 104 to participate based on the inclusion and exclusion criteria (n = 75 FM patients, n = 29 healthy controls). There were no statistically significant differences between the study groups for age or body mass index. The VAS, MFI, BAI, and PSQI scores of FM patients, which had a large effect size, were significantly higher than those of the healthy controls (all p < .001).
Demographic and Clinical Data of Patients With Fibromyalgia and Healthy Controls.
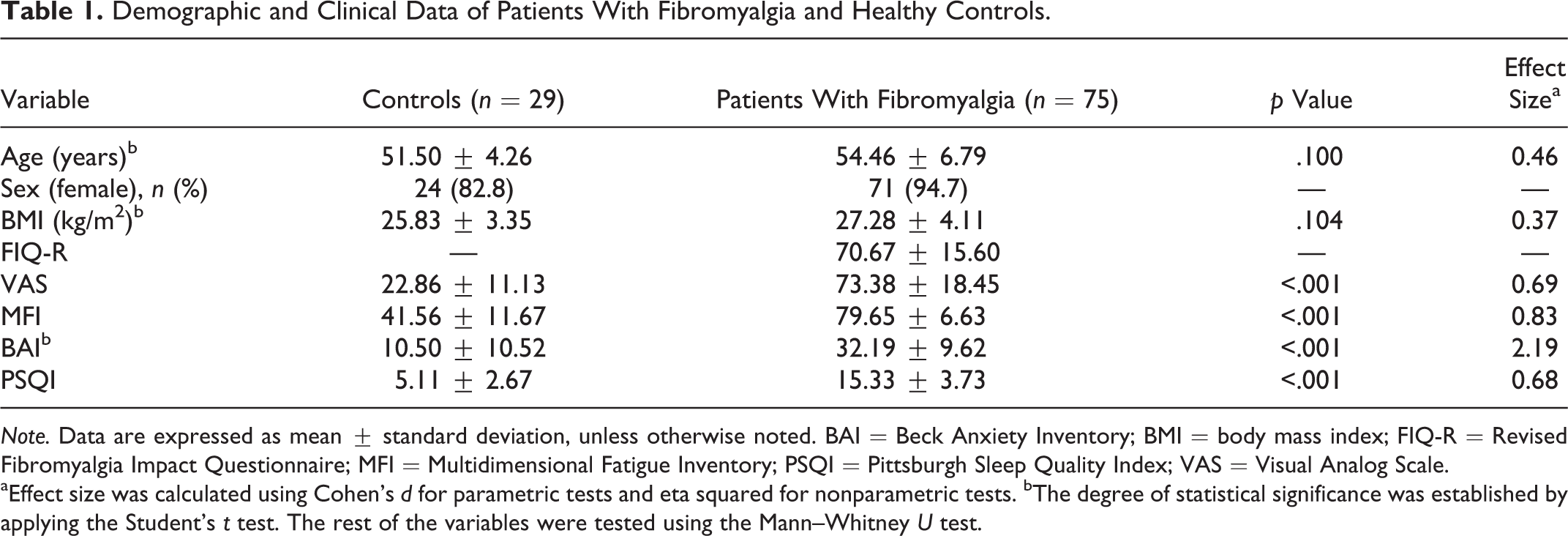
Note. Data are expressed as mean ± standard deviation, unless otherwise noted. BAI = Beck Anxiety Inventory; BMI = body mass index; FIQ-R = Revised Fibromyalgia Impact Questionnaire; MFI = Multidimensional Fatigue Inventory; PSQI = Pittsburgh Sleep Quality Index; VAS = Visual Analog Scale.
aEffect size was calculated using Cohen’s d for parametric tests and eta squared for nonparametric tests. bThe degree of statistical significance was established by applying the Student’s t test. The rest of the variables were tested using the Mann–Whitney U test.
Serum AP Activities
Oxytocinase activity was higher in patients with FM than in healthy subjects (p < .001, Table 2). A subgroup of patients with FM (n = 18, 24%) showed significantly lower levels of EDA activity when compared with the healthy controls (p < .001, Table 2) and with the rest of FM patients (n = 57, 76%; p < .001, Table 3). The rationale for creating two subgroups of FM patients based on the values of EDA activity was this large difference found in EDA activity values within the FM group. In the ROC analysis for EDA activity in FM patients, the cutoff point was .73 pmol/min/mg protein (AUC = 1, 95% CI [0.938, −1.000], p < .0001, 100% sensitivity, 100% specificity). Therefore, we created a subgroup that included the FM patients with EDA activity values ≤.73 pmol/min/mg protein (n = 18) and another subgroup that included patients with FM with EDA activity values >.73 pmol/min/mg protein (n = 57). There were no significant differences between the two subgroups of FM patients in the other variables analyzed (demographic data, clinical features, other AP activities; Table 3). The activity levels of APA, APB, ASAP, IRAP, PAP, and APN did not show significant differences between FM patients and controls (Table 2). Oxytocinase activity (Table 2) and EDA activity in the subgroup of 18 patients (Tables 2 and 3) presented a large effect size, while the rest of the parameters had a small effect size.
Serum Aminopeptidase Activity in Patients With Fibromyalgia and Healthy Controls.
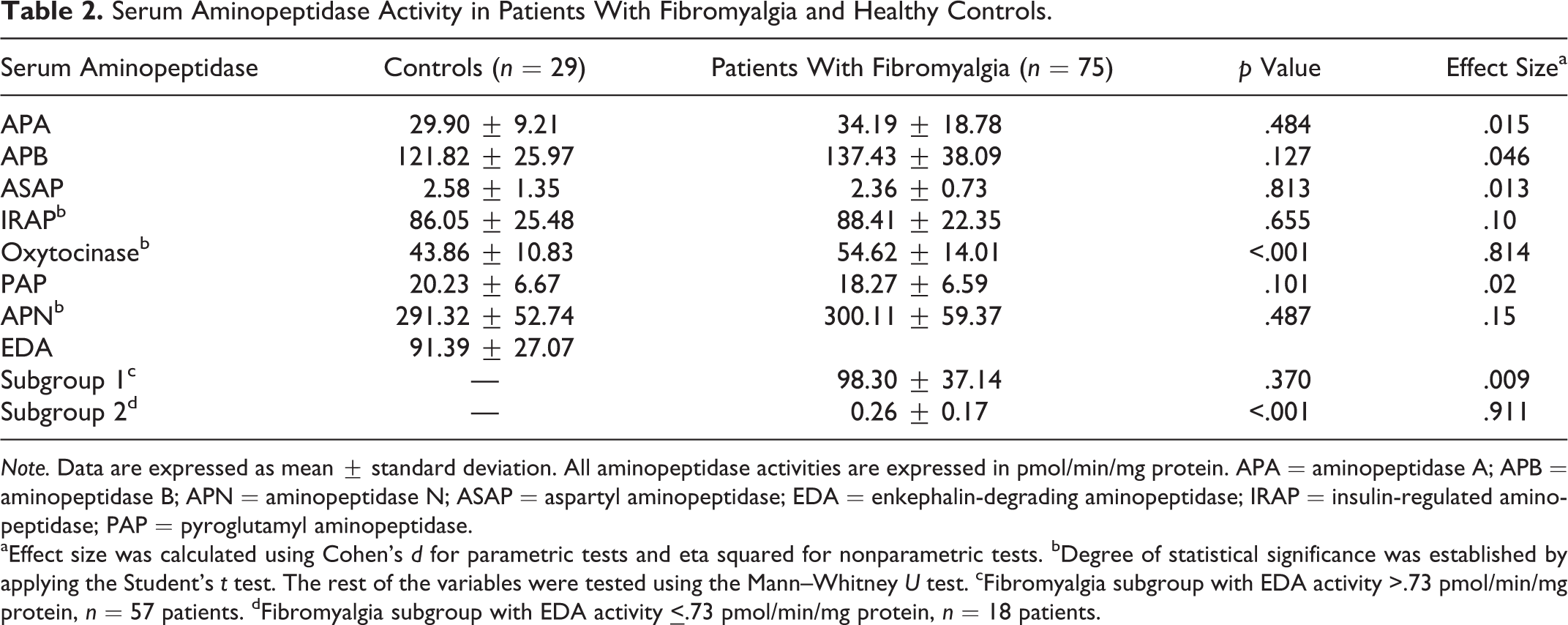
Note. Data are expressed as mean ± standard deviation. All aminopeptidase activities are expressed in pmol/min/mg protein. APA = aminopeptidase A; APB = aminopeptidase B; APN = aminopeptidase N; ASAP = aspartyl aminopeptidase; EDA = enkephalin-degrading aminopeptidase; IRAP = insulin-regulated aminopeptidase; PAP = pyroglutamyl aminopeptidase.
aEffect size was calculated using Cohen’s d for parametric tests and eta squared for nonparametric tests. bDegree of statistical significance was established by applying the Student’s t test. The rest of the variables were tested using the Mann–Whitney U test. cFibromyalgia subgroup with EDA activity >.73 pmol/min/mg protein, n = 57 patients. dFibromyalgia subgroup with EDA activity
Demographic Data, Clinical Features, and Serum Aminopeptidase Activity in the Two Subgroups of Patients With Fibromyalgia.
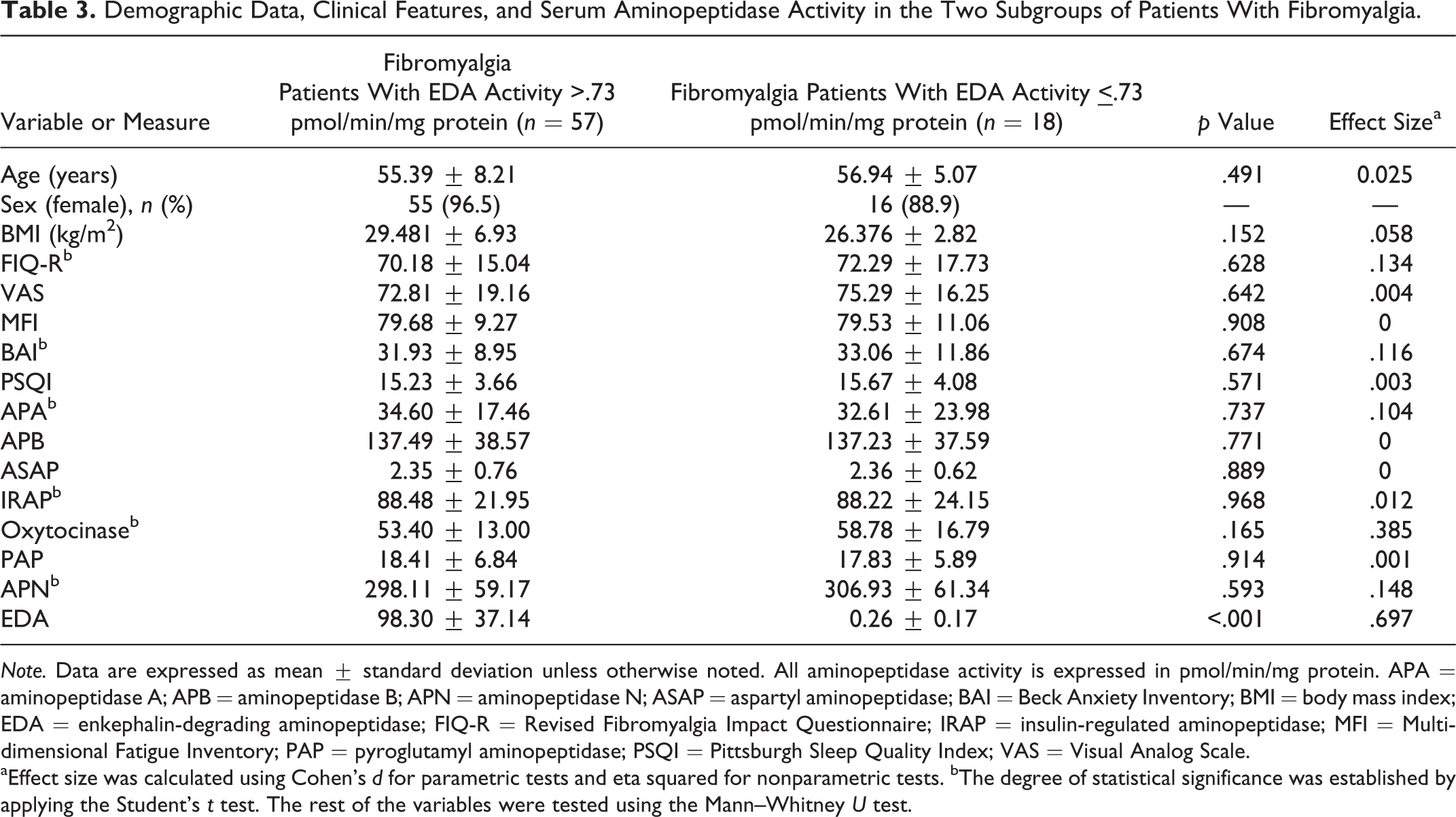
Note. Data are expressed as mean ± standard deviation unless otherwise noted. All aminopeptidase activity is expressed in pmol/min/mg protein. APA = aminopeptidase A; APB = aminopeptidase B; APN = aminopeptidase N; ASAP = aspartyl aminopeptidase; BAI = Beck Anxiety Inventory; BMI = body mass index; EDA = enkephalin-degrading aminopeptidase; FIQ-R = Revised Fibromyalgia Impact Questionnaire; IRAP = insulin-regulated aminopeptidase; MFI = Multidimensional Fatigue Inventory; PAP = pyroglutamyl aminopeptidase; PSQI = Pittsburgh Sleep Quality Index; VAS = Visual Analog Scale.
aEffect size was calculated using Cohen’s d for parametric tests and eta squared for nonparametric tests. bThe degree of statistical significance was established by applying the Student’s t test. The rest of the variables were tested using the Mann–Whitney U test.
ROC Curves
ROC curve analysis is a procedure widely used to assess the accuracy of a diagnostic test. We used this analysis to determine the predictive value of AP activities in FM. Figure 1 shows the ROC curve for serum oxytocinase activity. This curve represents the true positive fraction (sensitivity) on the x-axis and the false positive fraction (1 specificity) on the y-axis of the diagnostic test at several values of the test. Accuracy of the diagnostic test is measured by the AUC, which ranges from 0 to 1 (an AUC of 1 represents a perfect test, while an AUC of 0.5 represents a worthless test). Only oxytocinase activity showed a statistically significant AUC (0.725, 95% CI [0.629, 0.809], p < .0001), indicating that it may be a good marker for differentiating individuals with FM from healthy subjects. The AUC indicates that there is 72.5% probability that, given two randomly chosen individuals, one with FM and one a healthy individual without FM, oxytocinase activity values would distinguish between the two. We also calculated several data related to the ROC curve for oxytocinase activity, including the cutoff point (53.01 pmol/min/mg protein), sensitivity (85.71%), specificity (50.67%), PV+ (4.1), and PV− (93.3). The predictive values indicate that the probability of accurately cataloguing a person with values of oxytocinase activity ≤53.01 pmol/min/mg protein as healthy is 93.3% and that 4.1% of subjects who have oxytocinase activity values >53.01 pmol/min/mg protein may be diagnosed with FM with high sensitivity and specificity.
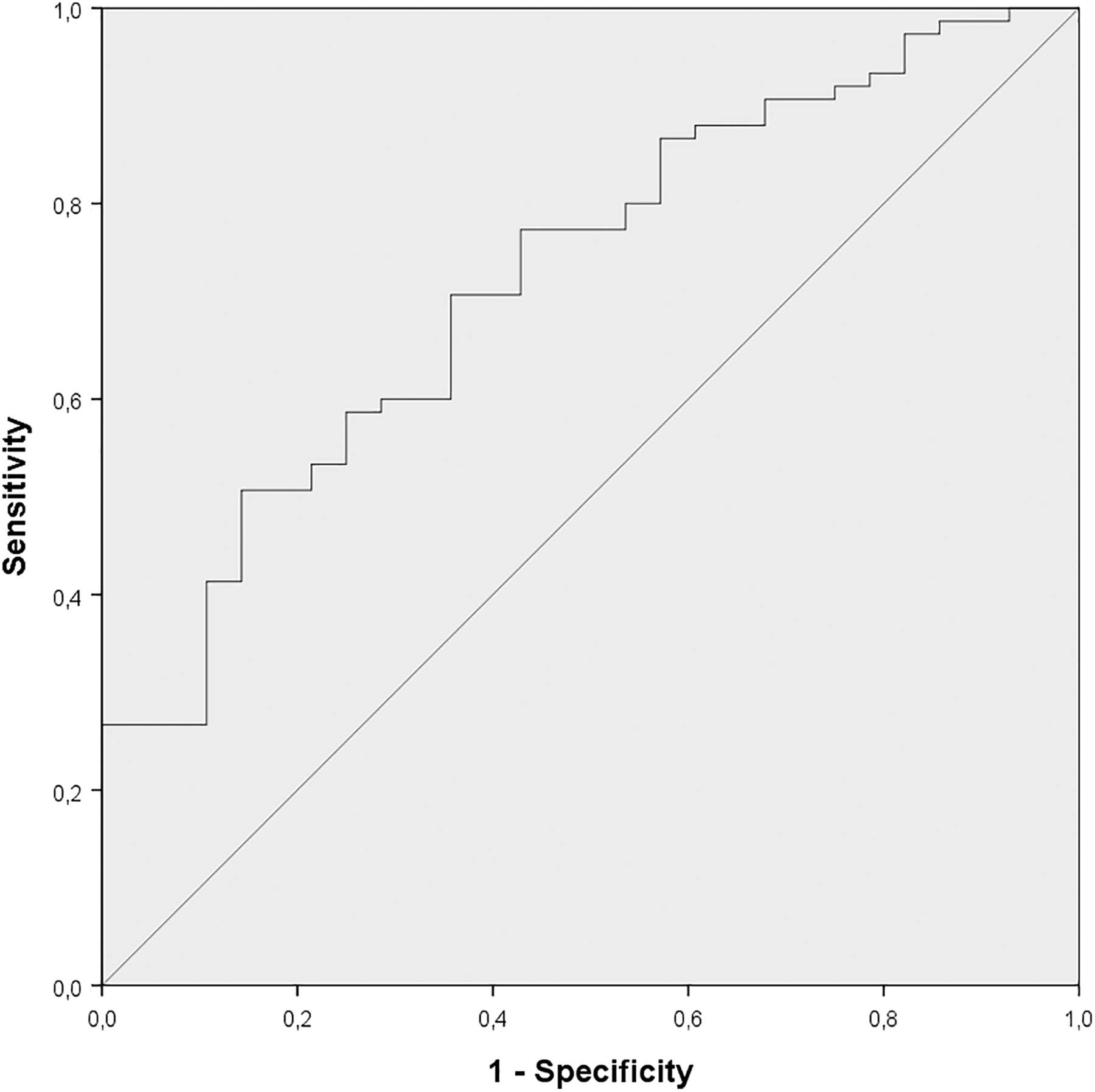
Receiver operating characteristic curve for serum oxytocinase activity.
Correlations Between Serum AP Activity and Clinical Features in Patients With FM
We explored the possibility of significant correlations between FM clinical features and the activity of EDA and oxytocinase, the APs for which activity differed significantly between patients with FM and healthy controls. We found that EDA activity was positively correlated with PSQI score in the subgroup of 18 FM patients with EDA activity
Discussion
FM is a poorly understood condition that presents challenges for both diagnosis and treatment. APs comprise a group of hydrolases that potentiate or inhibit peptide functions that are related to important physiologic and pathologic processes. We analyzed the specific activity of a broad spectrum of APs in patients diagnosed with FM and healthy controls to investigate whether they are involved in the pathophysiology of this syndrome. To the best of our knowledge, this work is the first to explore serum AP activity in FM.
Serum Oxytocinase Activity in FM
The mechanisms responsible for the increased perception of pain in FM are unclear. Enkephalinases, such as EDA and oxytocinase, are a type of enzyme that hydrolyzes the endogenous opioid enkephalins. Enkephalins have antinociceptive effects through their binding to opioid receptors. Enkephalinase inhibitors, which inhibit one or more members of the enkephalinase class of enzymes, seem to be promising as pharmacological agents due to their antinociceptive actions (reviewed in Thanawala, Kadam, & Ghosh, 2008).
Oxytocinase metabolizes endogenous oxytocin in addition to enkephalins. In the present study, serum oxytocinase activity was significantly higher in patients with FM than in healthy controls, suggesting that oxytocinase dysregulation could be related to the pathophysiology of FM. Increased oxytocinase activity may result in greater degradation of oxytocin. Recent research has explored the antinociceptive and anxiolytic effects of oxytocin (reviewed in Neumann & Slattery, 2016; reviewed in Xin et al., 2017). FM patients in the present study showed higher levels of both self-perceived pain and anxiety than the controls. Our findings suggest that these increased levels could be due to the putative decrease in the analgesic and anxiolytic effects of oxytocin in these patients. Similarly, Anderberg and Uvnäs-Moberg (2000) found significantly lower levels of oxytocin in women with FM who had high scores for pain, stress, and depression in comparison to nondepressed FM patients and healthy controls. We did not, however, find any significant correlation between serum oxytocinase activity and clinical features of the FM patients in the present study. In a study that examined the efficacy of exogenous oxytocin administration in 14 patients with FM, researchers reported that oxytocin nasal spray did not have any beneficial effect on pain, anxiety, depression, or quality of life, though it also had no side effects (Mameli et al., 2014).
Pain or stressful stimulation can cause an increase in levels of endogenous opioid peptides such as enkephalins (reviewed in Thanawala et al., 2008). In patients with FM, specifically, research has shown that plasma Met-enkephalin levels increase after local injection (Figuerola, Loe, Sormani, & Barontini, 1998). As oxytocinase also degrades Met-enkephalin (reviewed in Tsujimoto & Hattori, 2005), its increased activity in the FM patients in the present study may indicate a decrease in the levels of antinociceptive enkephalins in comparison to the healthy subjects. This finding could be related to the higher levels of pain that patients with FM show in relation to healthy subjects.
Previous data on enkephalin levels in FM patients are conflicting. While some authors found decreased Met-enkephalin levels in CSF from patients with FM when compared to healthy subjects (Liu et al., 2000), other studies reported increased levels of Met-enkephalin in CSF from patients with FM in comparison to controls (Baraniuk et al., 2004; Vaerøy et al., 1991). These conflicting results might be explained by the different protocols for sample preparation used by the researchers and the selection of the study groups (patients with FM vs. controls). Patients with FM frequently have many comorbidities (reviewed in Lichtenstein, Tiosano, & Amital, 2018) that researchers usually do not take into account during the selection of patients, so undocumented differences in patient groups could account for the different results on Met-enkephalin levels reported in these studies. Although researchers in these previous studies determined levels of Met-enkephalin in CSF, we chose to measure AP activity in serum samples because collection of CSF is more invasive.
Despite the conflicting results found in the levels of enkephalins in FM patients, researchers from previous studies seem to agree that there may be dysregulation in the endogenous opioid system in patients with FM. For example, Harris et al. (2007) reported that µ-opioid receptor availability was reduced within several brain regions known to play a role in pain modulation in patients with FM as compared with healthy controls, indicating altered endogenous opioid analgesic activity in FM. Other authors proposed that dysfunction of endogenous opioid peptides such as enkephalins could predispose FM patients to chronic pain (Baraniuk et al., 2004). Schrepf et al. (2016) proposed that dysregulation of the endogenous opioid system in FM patients could lead to less excitation in antinociceptive brain regions in response to incoming noxious stimulation, resulting in the hyperalgesia and allodynia that these patients often report. In the present study, we found, for the first time, that the activity of an enzyme implicated in the metabolism of enkephalins, oxytocinase, is altered in FM. This alteration may be related to the dysregulation of the endogenous opioid system in FM patients that several previous authors have suggested.
According to our ROC analysis, serum oxytocinase activity may be a good marker for differentiating individuals with FM from healthy subjects because the probability of accurately identifying a person with oxytocinase activity levels ≤53.01 pmol/min/mg protein as healthy is 93.3% and that 4.1% of individuals who have oxytocinase activity values >53.01 pmol/min/mg protein can be diagnosed with FM with high sensitivity and specificity. Serum oxytocinase activity may thus be useful for identifying individuals who do not have FM.
Serum EDA Activity in FM
We found that a subgroup of patients with FM (n = 18, 24%) showed significantly lower serum activity levels of EDA when compared with the healthy subjects and the rest of FM patients (n = 57, 76%). In fact, the level of EDA enzyme activity in this subgroup of patients was close to 0. Given that our FM patients were not taking medications that could affect the activity of EDA (enkephalinase inhibitors or opioid receptor agonists or antagonists), we propose that there could be a subtype of FM characterized by abnormally reduced values of EDA activity. In other words, our data suggest the existence of different subgroups of FM patients with different biochemical characteristics that are all currently included within the broad diagnosis of FM. The identification of subgroups within the FM syndrome could facilitate the search for the pathophysiological mechanisms of the disease and lead to better management of this condition. Similarly, previous authors have proposed the existence of a subset of FM patients who have elevated levels of erythrocyte sedimentation rate and C-reactive protein and labeled this subtype inflammatory FM (Metyas, Solyman, & Arkfeld, 2015).
The low levels of EDA activity we found in a subgroup of patients with FM in the present study could result in an increase in the accumulation of enkephalins in these patients. However, there were no significant differences in the other variables we analyzed (demographic data, clinical features, other AP activities) between the two subgroups of FM patients. Therefore, future studies are needed to elucidate the pathophysiological basis of the difference we found in EDA activity between the two subgroups of FM patients, which would improve our understanding of the pathophysiology of this complex syndrome. In the present study, we did find a significant correlation between serum EDA activity and the clinical features of FM patients. Contrary to expectations, EDA activity positively correlated with PSQI score in the subgroup of FM patients with low levels of EDA activity. That is, the lower activity level of EDA was associated with improved sleep quality. Previous authors have suggested that endogenous opioids are involved in the regulation of sleep and wakefulness (King, Masserano, Codd, & Byrne, 1981). However, our result is difficult to explain and could also be related to miscalculation of correlations attributable to the small sample size.
Other Serum AP Activity in FM
We found no significant differences in the activity level of the other enzymes we analyzed (ASAP, APA, APN, APB, IRAP, and PAP) between FM patients and healthy controls, which may indicate that they are not involved in the pathophysiology of this syndrome.
Study Limitations
The main limitation of the present study is the imbalance in sample size between the control and FM groups. Nevertheless, the sample size estimation we performed prior to the study showed that the number of subjects in each of our two study groups was adequate (estimation data not shown). Our findings provide new insights into the pathogenesis of FM. However, our results need replication in larger samples of participants and in participants from different geographical areas.
Conclusion
The search for the mechanisms responsible for the chronic widespread pain FM patients report is an important area of clinical research. Our findings in the present study show, for the first time, that serum oxytocinase activity is increased in patients with FM compared to healthy controls, which may alter the metabolism of peptides with analgesic effects such as oxytocin and enkephalins, ultimately resulting in inadequate activity of endogenous pain attenuation mechanisms. The determination of serum oxytocinase activity may aid in the FM diagnosis. Additionally, we have identified a subpopulation of FM patients with an abnormally low level of serum activity of EDA, which suggests the existence of different subgroups of FM patients with different biochemical characteristics. The present results increase our understanding of the pathophysiology of FM and are another step toward more effectively diagnosing and managing this syndrome.
Footnotes
Acknowledgment
We wish to thank AFIXA (Association of Fibromyalgia of Jaén, Spain) and AGRAFIM (Association of Fibromyalgia of Granada, Spain) for collaborating in this study.
Author Contributions
José Manuel Martínez-Martos contributed to analysis, critically revised manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy. María Correa-Rodríguez contributed to conception, design, and acquisition; critically revised manuscript; gave final approval; and agreed to be accountable for all aspects of work ensuring integrity and accuracy. Alma Rus contributed to analysis and interpretation, drafted manuscript, critically revised manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy. Francisco Molina contributed to conception, design, and acquisition; critically revised manuscript; gave final approval; and agreed to be accountable for all aspects of work ensuring integrity and accuracy. María Jesús Ramírez-Expósito contributed to analysis, critically revised manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy. María Encarnación Aguilar-Ferrandiz contributed to conception, design, and acquisition; critically revised manuscript; gave final approval; and agreed to be accountable for all aspects of work ensuring integrity and accuracy. José Manuel Martínez-Martos, PhD, and María Correa-Rodríguez, PhD, contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.