
Abstract
Purpose:
This study was designed to identify underlying cardiovascular risk factors among college students including lifestyle characteristics, health behaviors and knowledge, and perception of the risk factors.
Method:
College students (N = 293), aged 19–36 years, enrolled at either a Midwestern or a Southwestern University in the United States, responded to three questionnaires: sociodemographic, knowledge of cardiovascular risk factors, and perception of cardiovascular risk factors. Anthropometric measures collected included blood pressure (BP), glucose, lipid panel, height, weight, and body mass index (BMI).
Results:
There were significant regional and gender differences in cardiovascular disease (CVD) risk among Southwestern and Midwestern college students. Students from the Southwest had a higher risk of developing CVD in 30 years compared to those in the Midwest; they also had a higher perceived risk. Males were more at risk of developing CVD than females but had a lower perceived risk than females. Dietary habits were similar between the two populations, and we found no significant differences in BMI. The two regions varied in BP levels, but the Midwestern students had significantly higher prevalence of elevated BP and Stage 2 hypertension.
Conclusion:
Our data suggest that college students are a high-risk population and tend to underestimate and misperceive their risk for developing CVD.
Cardiovascular disease (CVD) is the leading cause of death in the United States for both male and female adults, killing more than 600,000 each year (Sacks et al., 2017; Xu, Murphy, Kochanek, & Arias, 2016). Approximately half of American adults have at least one risk factor for CVD: high blood pressure (BP), smoking, or high cholesterol (Fryar, Chen, & Li, 2012). Despite the continuous research among adults on CVD risk factors, young adults, particularly college-age populations, are understudied (Go et al., 2013; Tran & Zimmerman, 2015). CVD risk factors often begin in adolescence and continue into adulthood if not modified, controlled, or treated (Luo, Agley, Hendryx, Gassman, & Lohrmann, 2015). These CVD risk factors commonly include tobacco use, alcohol abuse, high BP, sedentary lifestyle, high-fat diets, high levels of stress, obesity, high cholesterol, and Type 2 diabetes (Fryar et al., 2012; Go et al., 2013; Tran & Zimmerman, 2015). Unmodifiable factors, such as age, gender, and ethnicity, further impact CVD risk (Xu et al., 2016).
Awareness of CVD risk among college students is also understudied (Sarpong, Curry, & Williams, 2017), and few studies have explored how geographic location affects CVD risk among college students. In one study conducted at Arizona State University, researchers found that students had a low level of knowledge regarding heart disease and its risk factors compared with other health issues such as cancer and sexually transmitted infections (Collins, Dantico, Shearer, & Mossman, 2004). In the same study, authors also found that college students believed cancer kills more people than heart disease in females and that White college students are at increased risk for developing heart disease compared to students of other ethnicities, both of which are incorrect. In fact, African American and Hispanic college students are most at risk (Collins et al., 2004). Notably, college students in the United States have reported high rates of engaging in risky behaviors such as poor dietary habits, smoking, and physical inactivity (Luo et al., 2015; Xu et al., 2016). Further, one third of young adults do not understand how their current behaviors impact future risks of developing CVD (Roger et al., 2011), and most young adults grossly underestimate their CVD risk (Green, Grant, Hill, Brizzolara, & Belmont, 2003).
Regional and environmental factors influence lifestyle habits, as do sociodemographic factors such as ethnicity, age, income, and education (Ali et al., 2011). Predictors of obesity and CVD are closely correlated with geographical location. Rural populations tend to have a higher prevalence of obesity and sedentarism compared to urban populations throughout the United States (Patterson, Moore, Probst, & Shinogle, 2004). The Centers for Disease Control and Prevention (CDC, 2015) reported that 30–35% of Midwesterners qualified as obese, as compared to those living in the West, which has an obesity prevalence of 25–30%. Nevada has the highest rates of heart disease mortality in all of the states in the West and Southwest (CDC, 2019). Additionally, the Midwest has the highest incidence of binge drinking and cigarette smoking (CDC, 2016). The rates of cigarette smoking vary among areas in the Western region, with a higher prevalence of cigarette smokers in Nevada and Oregon (CDC, 2016).
Lifestyle behaviors and dietary practices are often established in childhood and early adolescence (Kavey et al., 2003), meaning that behaviors developing during these stages have implications for an individual’s health-related behaviors throughout the life span. Almost three quarters of adults in the United States aged >20 years are overweight, and 37.9% are obese (National Center for Health Statistics, 2017). Additionally, the prevalence of obesity among adolescents in the United States aged 12–19 years has doubled, to 20.6%, over the past 20 years (National Center for Health Statistics, 2017). While epigenetic and genetic factors do affect the prevalence of obesity and the development of CVD in specific populations, risky lifestyle behaviors are currently the leading cause of developing obesity and CVD (Benyshek, 2013).
Unhealthy weight gain often occurs among college students during the transition from adolescence to adulthood (Racette, Deusinger, Strube, Highstein, & Deusinger, 2005). In a study conducted at the University of Missouri, researchers found that 70% of college students gained weight during their first 2 years in college (Racette et al., 2005). On average, college students gain approximately 6 pounds over the course of their first 4 years of college in the Midwest (Hopper & Moninger, 2017).
College students are at risk of developing risk factors that can lead to CVD later in life (Green et al., 2003; Sparling, 2007; Tran et al., 2017). Yet few studies have examined whether there are significant differences in specific CVD risk factors among college students living in different geographic regions of the United States. Lifestyle behaviors differ between individuals living in the Southwest and the West, and these behaviors might impact cardiovascular health. Therefore, the purpose of this study was to evaluate whether there are significant differences in cardiovascular risk factors, as well as in knowledge and perception regarding these risks, among college students living in the Midwestern and Southwestern regions of the United States.
Method
The present study is an extended data analysis from a published study (Tran et al., 2017) with additional data collection from another university in a different region of the United States. It is a descriptive analysis of CVD risk factors in students aged 19–36 years from two large universities, one in Nebraska in the Midwest and another in Nevada in the Southwest. Institutional review boards at both institutions approved the study.
Sample
Inclusion criteria for the present study were enrollment at one of the two university sites and age of 19–36 years. Exclusion criteria were diagnosis with CVD such as myocardial infarction, stroke, or coronary heart disease (CHD). Students were recruited using flyers posted around campus, social media announcements, and recruitment booths set up at both universities, where students received information about the study, completed informed consent, and had their biometric measurements taken. The final analysis included a total of 169 college students from the Midwestern University and 155 college students from the Southwestern University.
Measures
Data collection took an average of 2 days for each participant. On the day of recruitment, we obtained informed consent, participants completed the study questionnaires, and we collected at least some of the biological measures. If participants had not been fasting, we made an appointment for them to return for a fasting blood draw. Random blood draw was also accepted. All data collection took place at the university health center.
Participants completed three questionnaires: (1) a sociodemographic questionnaire collecting data on age, gender, marital status, education level, insurance status, race/ethnicity, smoking status, medication, and family history of heart disease along with a brief 3-item Food-Recall Questionnaire, (2) the Heart Disease Fact Questionnaire (HDFQ), which assesses respondents’ knowledge of cardiovascular risks, and lastly, (3) the Health Beliefs Related to Cardiovascular Disease (HBCVD) Questionnaire, which evaluates the respondent’s perception of his or her own cardiovascular risks. The food-recall questionnaire collected information about the students’ consumption of red meat, intake of sugary beverages, and average number of times they ate out per week. The HDFQ and HBCVD are both self-report measurements. The HDFQ (16 items) evaluates knowledge regarding CVD risk and the HBVCD (10 items) assesses perception of CVD risk on a Likert-type scale. Researchers previously validated the HDFQ Questionnaire with sufficient reliability (Kuder–Richardson formula 20 [KR-20] = 0.73; Wagner, Lacey, Chyun, & Abbott, 2005; Winham & Jones, 2011). Researchers previously validated the HBCVD Questionnaire with a Susceptibility subscale Cronbach’s α = .93 and Severity subscale Cronbach’s α = .71 (see Tovar et al., 2010). Both of these assessments have good content and face validity in the studied population (Tran, Zimmerman, & Kupzyk, 2016).
Biological and anthropometric measurements included systolic blood pressure (SBP), diastolic blood pressure (DBP), lipid panel, and glucose level. The blood draw and analysis procedure for the Midwest sample are detailed in Tran et al. (2017). We used a similar procedure for the Southwest sample except the students were required to fast for at least 8 hr prior to the blood draw. We took two BP measurements with a rest of at least 5 min between them and used the average of the two measurements for SBP and DBP. We used a digital scale (stadiometer) to measure height and weight to calculate body mass index (BMI).
Based on the data collected, we calculated the Framingham 30-year CVD risk score for each participant, which estimates an individual’s risk of developing CVD over the next 30 years as a percentage ranging from 0 to 100 (Schnabel et al., 2009).
Statistical Analysis
We used the IBM statistical package for social sciences (SPSS), version 25, for data entry and analysis. The cutoff for statistical significance was set at p < .05 for correlational relationships among the variables. We completed a test of normality on continuous variables and used nonparametric tests when the variables deviated from normal distribution. To summarize sample characteristics and objective measurements, we used descriptive statistics for continuous variables and frequency distributions for categorical variables. We analyzed the relationships among knowledge and perception of cardiovascular risk factors and the 30-year CVD risk assessment using Spearman’s correlations and the Mann–Whitney U test. We used the latter to determine the differences in multiple variables between students at the two universities, included age, gender, education levels, marital status, insurance coverage, history of heart disease, smoking status, BP levels (SBP and DBP), lipid profile, glucose level, BMI, scores on the knowledge and perception of cardiovascular risk factors questionnaires, and the Framingham 30-year CVD risk assessment.
Results
The final sample for this study included 293 college students. Table 1 summarizes the sociodemographic data by region. The mean age of participating students was 24.37 ± 4.32 years, with the majority (62.5%) aged between 19 and 24 years. There was no significant difference in mean age between the two universities. There was, however, a significant difference in gender. Nearly half of the total sample was male (47.8%), but the proportion of students who were male was significantly higher at the Midwestern University compared to the Southwestern school (54.2% vs. 40.6%). The sample was predominantly White (51%), especially at the Midwestern University (63% White vs. 37.7% at the Southwestern University). More than three fourth (79.9%) of the total sample was single. An overwhelming majority of the students had insurance coverage (92.5% of the total sample).
Demographic Characteristics of Participating University Students by Region.
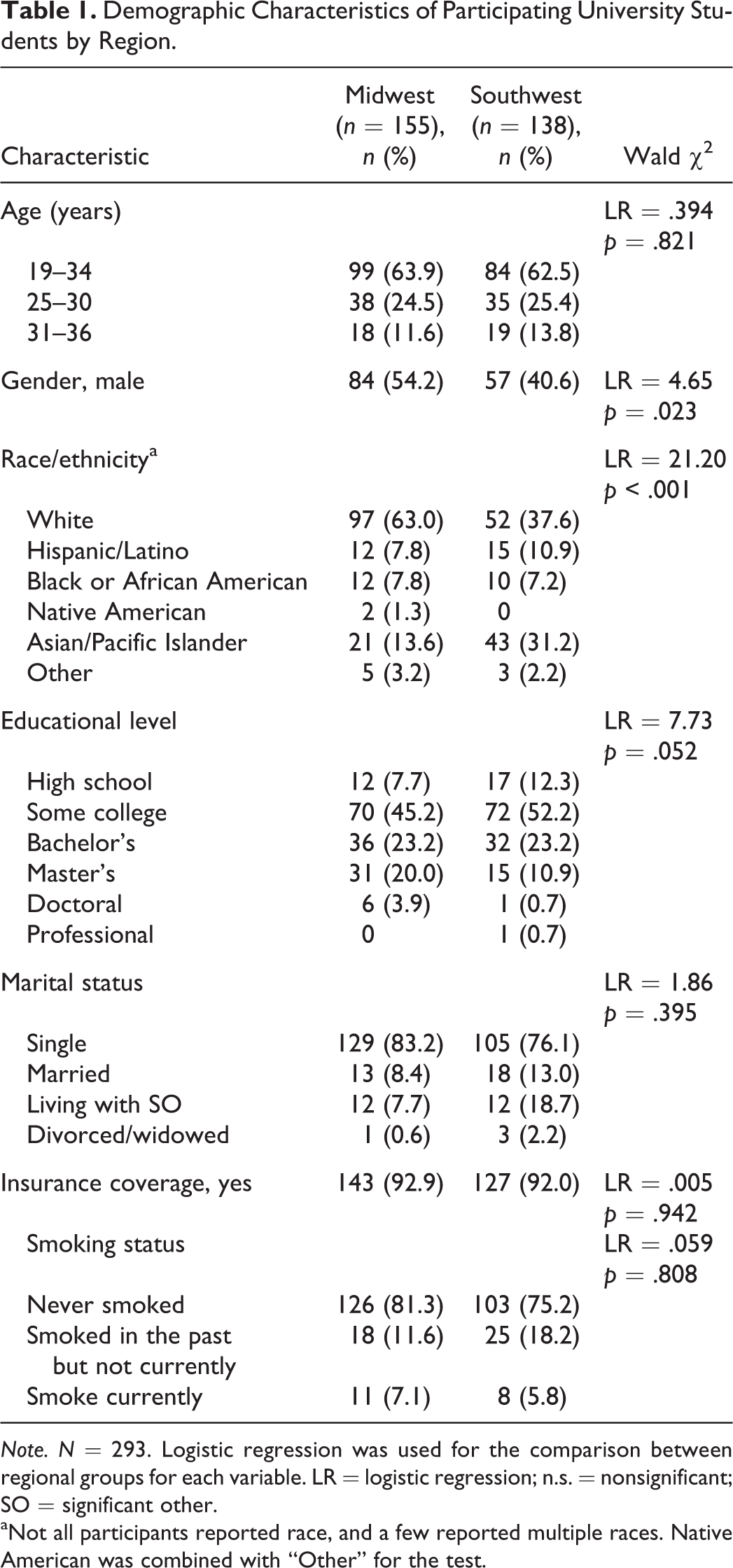
Note. N = 293. Logistic regression was used for the comparison between regional groups for each variable. LR = logistic regression; n.s. = nonsignificant; SO = significant other.
aNot all participants reported race, and a few reported multiple races. Native American was combined with “Other” for the test.
Among the CVD risk factors we analyzed, we found statistically significant differences between regions in the family history of heart disease (p < .048), SBP (p < .001), DBP (p < .001), low-density lipoprotein cholesterol level (LDL-C; p < .002), high-density lipoprotein cholesterol level (HDL-C; p < .005), level of triglycerides (p < .038), hyperlipidemia (p < .000), diabetes (p < .000), and the 30-year CVD risk (p < .009). Specifically, the Midwest students had a higher mean rank on family history of heart disease, HDL-C and triglycerides levels, and SBP, while the Southwest students had a higher mean rank on DBP, LDL-C level, hyperlipidemia, diabetes prevalence of the HDFQ, and the 30-year CVD risk assessment. We also found a significant difference in the HDFQ score (p < .038) between groups.
The Southwest had a higher mean rank of LDL-C level (z = −3.103; 162.23 vs. 131.56) and lower rank of HDL-C level (z = −2.802; 132.31 vs. 160.08), meaning that the Midwest sample had a significantly better lipid profile compared to the Southwest sample. We used levels of LDL-C, total cholesterol, and triglycerides to determine which students had hyperlipidemia and glucose levels to calculate which had diabetes. We calculated the proportion of students with either hyperlipidemia (n = 9) or diabetes (n = 9) in each region and found that the students at the Southwestern University had a significantly higher prevalence of both hyperlipidemia (z = −16.515; 222.57 vs. 79.72) and diabetes (z = −16.337; 221.57 vs. 80.61) compared to the Midwestern students. We found no significant differences between regions for total cholesterol, smoking status, or BMI. Table 2 summarizes the biological and anthropometric measures for students in the two regions, specifically the findings on hyperlipidemia, diabetes, and BMI. As an exploratory analysis, we performed the Mann–Whitney U test on smoking status and found that the incidence of current smokers was significantly higher in the Southwestern versus the Midwestern sample.
Clinical and Anthropometric Variables for University Students in the Two Regions.
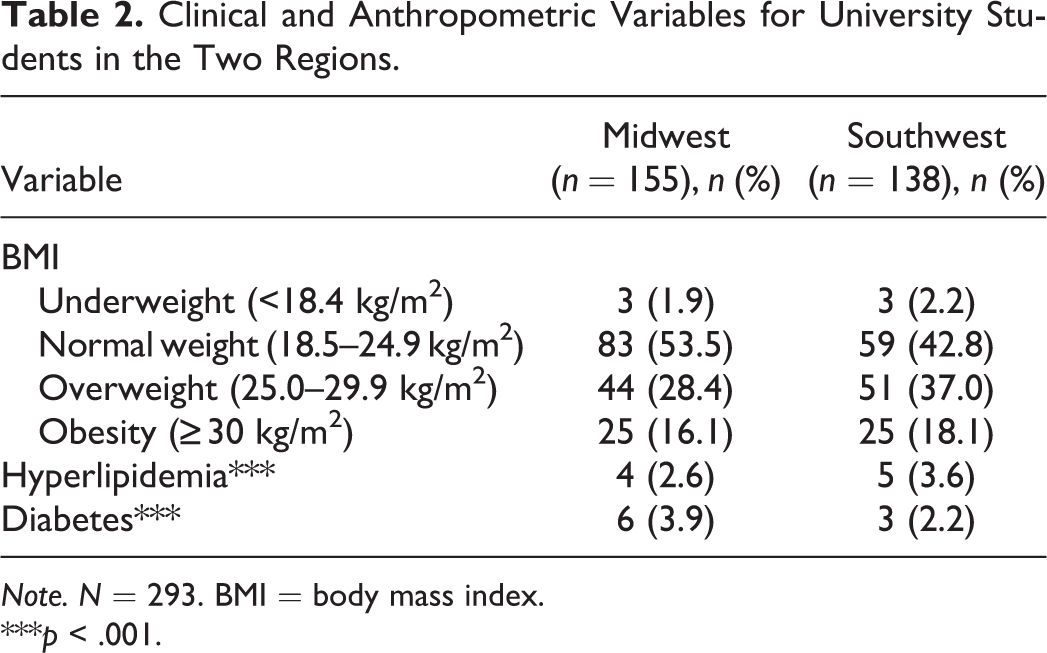
Note. N = 293. BMI = body mass index.
***p < .001.
Students at the Southwestern University had a higher mean rank on 30-year CVD risk score compared to those at the Midwestern University (z = −2.630, 156.87 vs. 131.36, respectively), meaning that students from the Southwest were more likely to develop CVD in the next 30 years. Furthermore, we found that females had a significantly lower risk of developing CVD in the next 30 years compared to their male counterparts from both regions (2.0 vs. 2.52 risk factors, respectively, p < .05). Although there were no significant gender differences on the HDFQ, we found that students at the Southwestern University had significantly more knowledge on CVD risk than those at the Midwestern school (z = −2.072, 157.551 vs. 137.60).
Food consumption patterns were similar between the two regional groups, and we found no significant differences. The majority of students (53.1%) as a whole reported eating meals outside the home at least 2–3 times per week, 42.3% reported consuming a sugary beverage at least 1 time per week, and 26.6% reported occasionally drinking a sugary beverage. The consumption of red meat was similar between students in the two regions, with 36.1% overall reporting consuming red meat 2 to 3 times per week. In the Midwestern group, 12.3% reported consuming red meat daily, with males in that group consuming significantly more red meat than females (z = −2.767, 86.54 vs. 67.90, respectively). Among the Southwestern students, there were no significant gender differences in consumption of red meat.
We found statistically significant differences in BP between students in the two regions (p < .018). Table 3 categorizes students from each region by BP based on the newly published BP guidelines (Whelton et al., 2018). The Midwestern students had a higher mean rank for SBP compared to the Southwestern students (z = −3.828, 164.87 vs. 126.92, respectively). Meanwhile, students in the Southwest had a higher mean rank for DBP (z = −3.973, 167.83 vs. 128.46). Of the sample as a whole, 43% had elevated BP or Stage 1 or 2 hypertension according to the new guidelines. The Midwestern students had a higher mean rank of elevated BP than the Southwestern students (SBP > 120 mmHg and DBP < 80 mmHg, 25.2% vs. 13.8%, respectively, z = −2.37, 157.29 vs. 135.45). We found that the proportions of students with normal and elevated BP as well as Stage 2 hypertension differed significantly between the two regions (p = .009, p = .015, and p = .007, respectively). A larger proportion of students from the Midwestern University also had Stage 2 hypertension than those from the Southwestern school (SBP ≥ 140 mm Hg or DBP ≥ 90 mm Hg; 12.3% vs. 3.6%, respectively). However, more students from the Southwestern University than from the Midwestern University had Stage 1 hypertension (SBP 130–139 mm Hg or DBP 80–89 mm Hg; 25.4% vs. 20.6%, respectively). Males had significantly higher levels of elevated SBP (p < .000) than females in both regions. In the Southwest, males also had significantly higher levels of DBP (p < .000) than females; however, there was no significant difference by sex for DBP in the Midwest. Additionally, less than 2% of the sample from both regions reported taking antihypertensive medication to control their high BP.
Blood Pressure-Related Variables for Students at a Midwestern and Southwestern University.
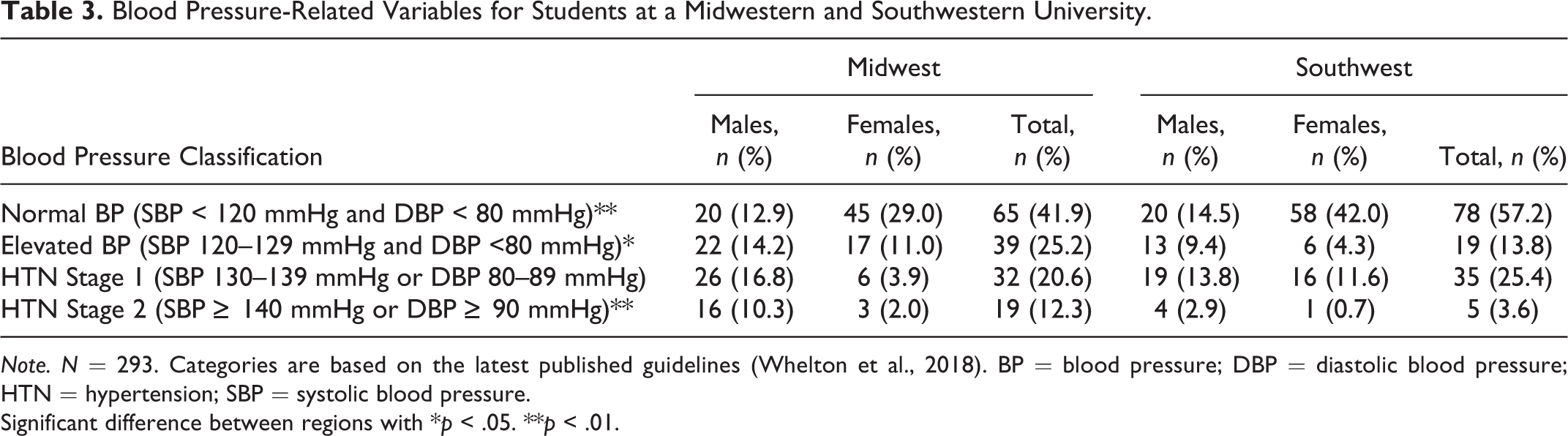
Note. N = 293. Categories are based on the latest published guidelines (Whelton et al., 2018). BP = blood pressure; DBP = diastolic blood pressure; HTN = hypertension; SBP = systolic blood pressure.
Significant difference between regions with *p < .05. **p < .01.
Discussion
In the present sample, male college students overall had more risk factors for CVD compared to females, including elevated BP levels and a higher score on the CVD 30-year risk. This finding is consistent with those of previous studies among college students (Green et al., 2003; Luo et al., 2015; Spencer, 2002). CVD risks tend to increase later in females than in males due to their hormonal profiles (Dib, Alameddine, Geitany, & Afiouni, 2008).
Regarding the risk factor of smoking, we found no significant difference in the incidence of current smokers between the two regional groups, though we did find that males smoked more than females in the Southwest region. These findings were inconsistent with those of previous studies (Pearson, LaCroix, Mead, & Liang, 1990; Tran et al., 2017) and with the estimate of the CDC (2015) that prevalence of smoking is highest in the Midwestern United States. The CDC did also estimate, however, that smoking rates in Nevada are equal to or higher than the national prevalence rate and, importantly, that Asian Americans, Hispanic Americans, and African Americans smoke more than their White counterparts in Nevada. Our sample of Southwestern college students was more ethnically diverse than our sample from the Midwest. This diversity along with the fact that our Southwestern sample had proportionally more males than our Midwestern sample could be contributing factors as to why we did not see a higher prevalence of smokers in the Midwest.
Although the difference was not statistically significant, we found that the students at the Southwestern University had a higher rate of obesity than those in the Midwest, a finding that contradicts the CDC (2016) estimate that the Midwest has higher prevalence of obesity (CDC, 2016). We also found that male students overall had a higher mean BMI compared to their female counterparts, though this difference was also not statistically significant. In a previous study conducted across five universities, researchers found that 50% of male students and more than 25% of female students were overweight or obese (Morrell, Lofgren, Burke, & Reilly, 2012).
Despite our findings that a third of the students in our overall sample were hypertensive (Stage 1 or Stage 2), less than 2% were taking antihypertensive medication to control their high BP. Zhang and Moran (2017) found strong associations between high BP and obesity for all age groups; in particular, they found that young adults with high BP are more than twice as likely to also be obese compared to individuals in all other age groups with high BP.
Dietary habits impact lipid profiles, especially LDL-C and HDL-C. Students from the Southwestern University had significantly higher levels of LDL-C and lower levels of HDL-C. Higher levels of LDL-C are associated with poorer cardiovascular health outcomes including increased risk of developing CVD (Ray et al., 2014). Several studies have found that consuming red meat is positively associated with high BP, risk for CVD, and increased mortality rate (Micha, Wallace, & Mozaffarian, 2010; Miura et al., 2004; Pan et al., 2012; Pearson et al., 1990). In the present study, students in the two regions reported similar levels of consumption of red meat; however, males from the Midwest were significantly more likely to consume red meat compared to females from the Midwest. We also found that students at the two universities reported similar consumption of sugary drinks and the number of weekly incidents of eating out. College students as a whole tend to have poor dietary habits that impact their risk factors for CVD, especially obesity. College campuses are often near fast-food and cheap restaurants, which increases the likelihood that students will consume fatty foods and have high caloric intake (Abraham, Martinez, Salas, & Smith, 2018). In one study, researchers found that 70% of freshman and sophomore students ate less than the five recommended servings of fruits and vegetables per day, and 50% of both male and female students ate fried foods and fast foods at least 3 times per week (Racette et al., 2005). Abraham, Martinez, Salas, and Smith (2018) found that the majority of a Midwestern student population agreed that fast food increased the likelihood of obesity; however, that belief did not cause them to change their eating habits.
Based on the present findings and those of prior studies, it is apparent that CVD risk factors are prevalent among college students. Given that prevalence, students’ awareness of CVD risk factors is lower than it should be (Green et al., 2003; Sarpong et al., 2017; Tran & Zimmerman, 2015; Tran et al., 2017). College students often underestimate their CVD risk (Green et al., 2003; Sarpong et al., 2017; Tran & Zimmerman, 2015; Tran et al., 2017). Young males indicate a higher positive bias than young females (Green et al., 2003; McMahan, Cathorall, & Romero, 2007). Collins, Dantico, Shearer, and Mossman (2004) found that college students in most ethnic groups believed that Whites were more likely than other ethnic groups to develop heart disease; however, in reality, heart disease is more prevalent among African Americans and Hispanics than Whites.
Most young adults do not understand the connection between their current health behaviors and their risk for developing CVD (Green et al., 2003). In the present analysis, however, we found that students from the Southwestern University both had a higher risk of developing CVD in 30 years and perceived themselves being at greater risk compared to those at the Midwestern University
Limitations
The present study had a number of limitations. First, the study was cross sectional; therefore, generalizability is limited. Second, our sample comprised young adults from two universities in two different regions of the country. However, these samples may not be representative of the general population of young adults in these regions. A cross-sectional comparison of students at multiple universities in each of the four regions of the United States would be ideal for future research and would enhance the strength of the findings.
Conclusion
College students in our sample had many risk factors associated with developing CVD. Similar to other studies conducted among this population, males overall had a larger number of CVD risk factors compared to females, such as higher BMI, increased prevalence of smoking, and higher BP levels. Students at the Southwestern University had a higher 30-year risk of developing CVD than those at the Midwestern University and accurately perceived themselves to be at higher risk.
Findings from this study can inform future research studies among this population, as young adults are underrepresented in the scientific literature. Although college campuses have established programs to manage substance abuse and improve sexual behaviors, assistance with reduction of obesity, increase in physical activity, and decrease in other CVD risks remain few and far between. Although the CDC and various public health campaigns have made efforts to improve awareness about CVD risk factors among the general population, and specifically among high-risk subpopulations such as minorities, more clearly needs to be done to educate college-age young adults (Green et al., 2003). In young adulthood, people begin to form habitual lifestyle behaviors that will impact their health throughout their life span. It is thus essential to establish interventions that address risky behaviors related to CVD among college students in the United States.
Footnotes
Acknowledgment
The authors would like to thank Alyssa N. Crittenden, PhD, and Trevor R. Pollom, MA, for assistance with editing in the final drafts of this article.
Author Contributions
Kristen N. Herlosky contributed to analysis and interpretation, drafted the article, critically revised the article, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy. Dieu-My T. Tran contributed to conception, design, acquisition, analysis, and interpretation; critically revised the article; gave final approval; and agreed to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.