
Abstract
Objective:
Low sleep quality (LSQ) activates the hypothalamic–pituitary–adrenal (HPA) axis and is related to arousal. Nursing staff, who work in shifts, tend to exhibit LSQ, which affects the level of vigor after awakening. This study investigated the effects of nocturnal sleep quality on diurnal cortisol profiles and sustained attention in day-shift nurses.
Method:
This study adopted a prospective cross-sectional design. Participants were recruited from a university-affiliated hospital in northern Taiwan. In the initial stage of this study, the Chinese Pittsburgh Sleep Quality Index (PSQI) Questionnaire was administered to 199 participants to categorize them as either LSQ (PSQI > 5) or high sleep quality (HSQ; PSQI ≤ 5). Participants were then randomly sampled from the two groups. Nocturnal sleep data and four diurnal saliva samples were collected for each participant. Sustained attention was measured before they started work. A total of 32 and 29 participants in the HSQ and LSQ groups, respectively, completed the data collection process.
Results:
Compared with the HSQ group, the LSQ group exhibited earlier wake-up times (p = .02), a flatter cortisol awakening response (CAR) slope (p < .01), a flatter morning-to-evening slope (p < .01), and prolonged reaction speed and mean reaction time before starting work (p < .01).
Conclusion:
Compared with the HSQ group, the LSQ group exhibited impaired HPA-axis regulation, with a flatter CAR and diurnal cortisol slope and poor sustained attention in the morning. Nursing staff are advised to achieve HSQ to improve attention and performance levels and maintain optimum work safety.
Poor sleep quality results in activation of the hypothalamic–pituitary–adrenal (HPA) axis. In turn, hyperactivity of the HPA axis inhibits sleep and increases the frequency of awakening (Balbo, Leproult, & Van Cauter, 2010). The interaction between sleep and the HPA axis is complex and bidirectional (Steiger, 2002). Activity of the HPA axis plays a significant role in modulating sleep and maintaining vigor (Balbo et al., 2010; Buckley & Schatzberg, 2005). Sleep interruption adversely affects an individual’s physical, mental, and emotional well-being. In nurses working in rotating shifts, lack of sleep increases fatigue level and reaction time (RT) and reduces attention span and judgment, thus increasing the risk of critical medical incidents and poor outcomes in patients (del Angel et al., 2015; Langner, Steinborn, Chatterjee, Sturm, & Willmes, 2010; Lo, Chiou, Huang, & Chien, 2016).
Sleep–wake rhythms are endogenously generated in the hypothalamus to maintain normal homeostatic functions and circadian processes (Gamble, Berry, Frank, & Young, 2014). These rhythms are modulated by external cues (e.g., daylight; Saper, Scammell, & Lu, 2005). Sleep onset is associated with the inhibition of cortisol secretion (Balbo et al., 2010), whereas the awakening process is associated with a rapid reciprocal interconnection between the activation of cortical and subcortical brain regions. During nonrapid eye movement sleep and awakening, the hippocampus is inhibited and the HPA axis secretes cortisol (Clow, Hucklebridge, & Thorn, 2010; Wilhelm, Born, Kudielka, Schlotz, & Wüst, 2007). Researchers often use cortisol secretion, which is controlled by the HPA axis, as a biomarker of psychological stress (Hellhammer, Wüst, & Kudielka, 2009; Kudielka & Wüst, 2010). Diurnal cortisol secretion is typically lowest during the first half of nighttime sleep, abruptly elevates during the second half of nighttime sleep, peaks shortly after awakening, then continuously decreases over the remainder of the day (Kudielka & Wüst, 2010); therefore, the graph of normal diurnal cortisol secretion exhibits a negative slope. In the diurnal pattern of cortisol secretion, the highest concentration of cortisol occurs during the cortisol awakening response (CAR) 30 min after awakening (Wilhelm et al., 2007). A rapid increase in the cortisol level following morning awakening is related to arousal (Elder, Wetherell, Barclay, & Ellis, 2014). In one study among rotating-shift workers, researchers observed the cortisol acrophase to be at 6 a.m. during the day shift, 7 a.m. during the evening shift, and 11 a.m. during the night shift (Lac & Chamoux, 2004).
Factors that affect cortisol secretion include sleep–wake and light–dark cycles, both in conjunction with neural pressure signals (Fries, Dettenborn, & Kirschbaum, 2009; Minkel et al., 2014). Sleep disturbances can reduce the cortisol level following morning awakening and lead to a flattened CAR (Castro-Diehl et al., 2015). Backhaus, Junghanns, and Hohagen (2004) found that patients with insomnia exhibited a decreased CAR and that CAR was negatively correlated with the subjective sleep quality score. Castro-Diehl et al. (2015) reported that shorter sleep durations caused smaller and more gradual declines in the diurnal cortisol slope than did longer sleep durations. Garde, Karlsson, Hansen, Persson, and Åkerstedt (2012) examined the relationship between sleep quality and cortisol concentration and found a positive correlation between sleep duration and diurnal cortisol slope, with a longer sleep duration resulting in higher and lower cortisol concentrations in the morning and evening, respectively, and steep diurnal cortisol variations. Meanwhile, other researchers have found that both restless sleep and chronic fatigue syndrome are positively associated with a flat diurnal deviation, indicating dysregulation of HPA-axis functions (Kumari et al., 2009; Roberts, Wessely, Chalder, Papadopoulos, & Cleare, 2004).
Alertness varies primarily with changes in the activation levels of the thalamus and prefrontal cortex (Balkin et al., 2002). Wu et al. (2015) used functional magnetic resonance imaging (fMRI) to examine the relationship between the CAR and brain activity and found a positive correlation between the CAR and the functional connectivity strength of the medial prefrontal cortex, which can be used to predict the intrinsic functional connectivity of the brain in the afternoon of the same day. Shi et al. (2018) indicated that the CAR could predict response inhibition (inhibition of inappropriate, unsafe behavior) in early cognitive and behavioral performance in the afternoon of the same day.
Sleep deprivation impairs neurobehavioral functions and reduces cortical functional responses. Drummond et al. (1999) used fMRI to examine arithmetic performance and cerebral activation after sleep deprivation and found decreased prefrontal cortex responsiveness in sleep-deprived participants. Participants with low sleep quality (LSQ) exhibited longer RTs in performance tests of vigilant attention (Yang et al., 2018). Researchers also reported that a sleep deprivation-induced reduction in the phonological and visuospatial components of the working memory (del Angel et al., 2015) was associated with cognitive impairment and reduction in the speed of processing information (Waters & Bucks, 2011). Not surprisingly, authors have reported that sleep deprivation increases the risk of work-related injuries (Hägg, Torén, & Lindberg, 2015; Rhéaume & Mullen, 2018).
Sleep quality is defined as a person’s satisfaction with the sleep experience, including sleep initiation, sleep maintenance, sleep quantity, and the feeling of being refreshed on awakening (Kline, 2013). Delayed sleep onset, nocturnal awakening, and short sleep durations lead to poor sleep quality and affect the diurnal cortisol rhythm profile during the subsequent day (Balbo et al., 2010). The functions of the HPA axis are associated with sleep quality and are involved in maintaining vigor and attention, which affect work safety. To date, there have been no studies examining the effect of sleep quality on diurnal HPA-axis function and attention in nursing staff; hence, an investigation of the effects of nocturnal sleep quality on diurnal cortisol profiles and sustained attention in the morning among nurses is necessary.
In the present study, we investigated the effects of nocturnal sleep quality on diurnal cortisol profiles and sustained attention before starting work in day-shift nurses. We hypothesized that the CAR and diurnal cortisol slopes would be flatter, and sustained attention in the morning would be lower in nurses with LSQ compared to nurses with high sleep quality (HSQ).
Materials and Methods
Study Design
We used a prospective, cross-sectional design for this study, which we conducted between January and August 2018. We recruited participants from a hospital affiliated with a university in northern Taiwan.
Participants
We enrolled female nursing staff who worked full time in medical and surgical wards, worked 8 hr per shift, and had at least 1 year of work experience. We excluded participants who had used sedatives, hypnotics, antihistamines, or hormonal drugs within the 4 weeks before the initiation of the study; were pregnant; or had been diagnosed with metabolic or neurological disorders. We posted advertisements on an electronic bulletin board in the study hospital to recruit participants. Upon confirmation that a nurse was eligible and willing to participate, a researcher held a face-to-face meeting at the nurse’s ward to introduce the study.
We determined the minimum required number of participants using a G-power calculation with a linear multiple regression model and a medium effect size. Statistical significance was set at α = .05 (two-tailed tests), and the power was set at 0.8. According to the estimate, the study required 29 participants in each group (LSQ and HSQ). On the assumption that 10% of recruited participants would withdraw from the study, we decided to include 32 participants in each group.
We initially recruited a total of 199 eligible participants to complete the Chinese Pittsburgh Sleep Quality Index (CPSQI) Questionnaire in the 4th week of the day-shift schedule. Of these participants, 91 (45.7%) reported subjective HSQ (CPSQI ≤ 5) and 108 (54.3%) LSQ (CPSQI > 5). Subsequently, we randomly sampled 32 participants from each of these two groups for the remainder of the data collection. Of these 64 participants, 3 withdrew from the study because they were unable to follow the assigned work schedules. Hence, a total of 61 participants (32 and 29 in the HSQ and LSQ groups, respectively) were included (Figure 1).
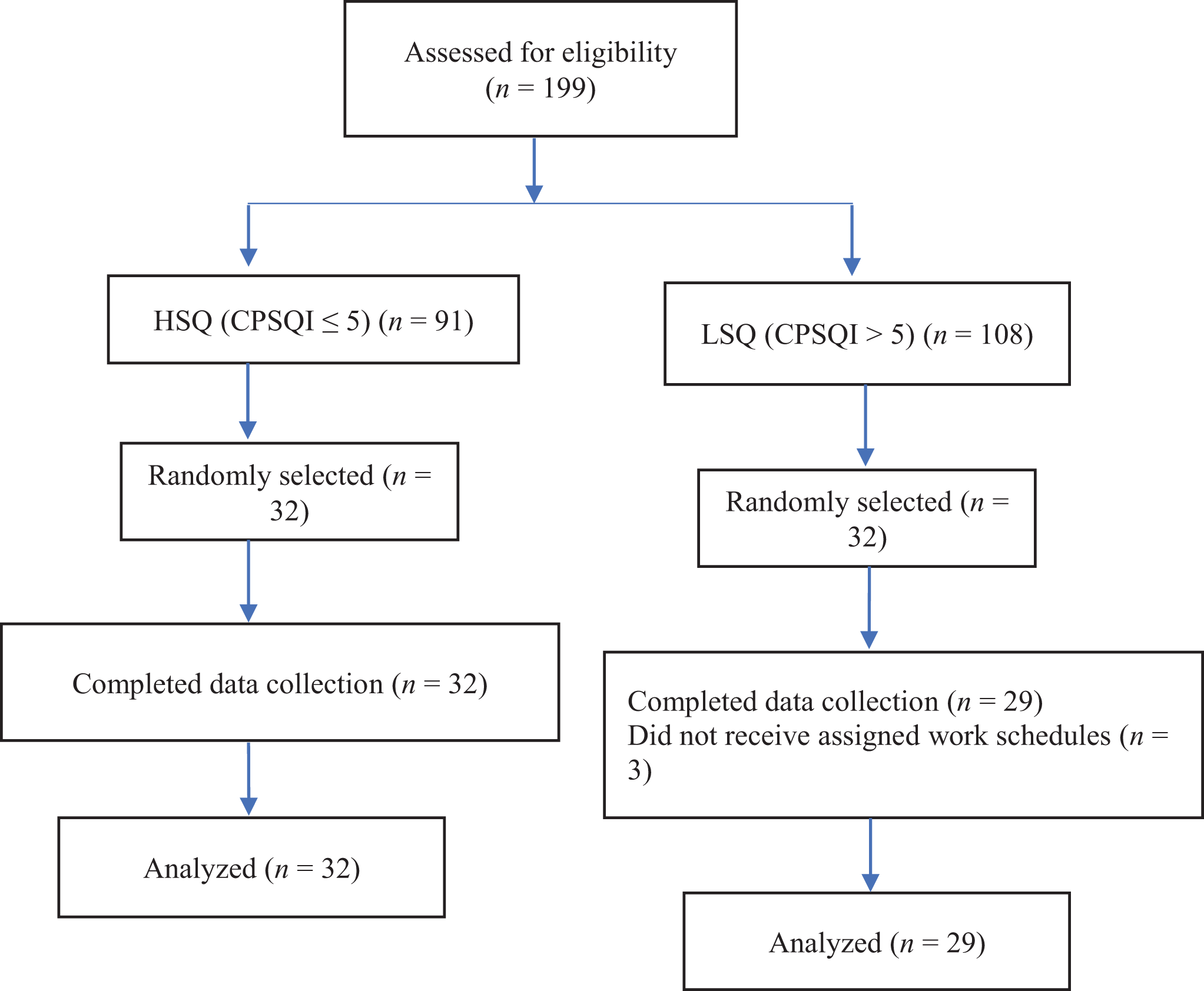
Participant flow diagram. CPSQI = Chinese Pittsburgh Sleep Quality Index; HSQ = high sleep quality; LSQ = low sleep quality.
Schedule Assignment
Shift work can affect circadian rhythms and sleep quality. In the present study, we assigned 4 weeks of regular day-shift work (8:00–16:00) to both groups to eliminate the effects of sleep–wake cycles that might occur with different shifts. For both groups, 5 days of work were followed by 2 days of leave. Participants recorded their nocturnal sleep data on the 4th day of the 4th week and collected their four diurnal saliva samples and underwent their prework psychomotor vigilance test (PVT) on the 5th day of the 4th week.
Instruments
The collected data comprised demographics, CPSQI scores, actigraphy sleep parameters, salivary cortisol concentrations, and PVT parameters.
Demographic data
Demographic data included age, work experience, marital status, education level, smoking and drinking habits, and consumption of caffeinated beverages.
CPSQI
Tsai et al. (2005) translated the PSQI, developed by Buysse et al. (1989), into Chinese (CPSQI). We used this translated version to measure the quality of sleep in participating nurses during the previous month. The instrument comprises 19 self-rated questions; higher scores indicate lower sleep quality. The sensitivity and specificity of global CPSQI scores of >5 (the cutoff for the LSQ group in the present study) were 98% and 55%, respectively, in patients with primary insomnia compared with controls (Tsai et al., 2005). The CPSQI had an overall reliability coefficient of .82–.83, and the test–retest reliability of Cronbach’s coefficient α was .85 for all patients and controls and .77 for patients with primary insomnia. The global CPSQI score was significantly correlated with the sleep quality Visual Analog Scale (r = −.30), sleep-onset latency (SOL; r = .30), and sleep efficiency (r = −.37) derived from the sleep diary of individuals with primary insomnia (Tsai et al., 2005). The global CPSQI score is considered a reliable measure for distinguishing between LSQ and HSQ. In the preparatory stage of the present study, each participant completed the CPSQI in the 4th week of the day-shift schedule.
Actigraphy
Participants wore an actigraph (Ambulatory Monitoring Inc., Ardsley, NY) on their nondominant wrists to collect objective sleep parameters including total sleep time (TST, amount of actual sleep time), SOL (the length of time from lights off to sleep), wake after sleep onset (WASO, the time spent awake between sleep onset and wake time), and sleep efficiency (SE, the ratio of TST to the amount of time spent in bed, multiplied by 100 to yield a percentage). Actigraphy, which uses zero-crossing threshold detection, measures arm movements and collects activity data in 1-min epochs. Researchers reported that, compared with polysomnography, actigraphy had favorable validity, with a correlation coefficient of .92 and an agreement of 91% (Jean-Louis, Kripke, Cole, Assmus, & Langer, 2001). We used Act Millennium software to download actigraphy data, subsequently transferred these data to Action4 software (Ambulatory Monitoring Inc.), and used the Cole–Kripke algorithm to process and calculate parameters. All actigraphy sleep parameters as well as bedtime (lights out; the actigraph had light sensor) and waking time were recorded on a single day, from the 4th workday (8:00) to the 5th workday (8:00) in the 4th week.
Salivary cortisol
We asked participants to collect four saliva samples (at awakening [0 min] and at 30 min, 6 hr, and 12 hr after awakening; Fuller-Rowell, Doan, & Eccles, 2012) on the 5th workday during Week 4 of the work schedule. Further, we asked them to ensure that the time of sample collection did not vary from the scheduled time by >5 min for the first two samples or >30 min for the remaining two samples. If a participant missed a collection time by more than these times, we instructed them to not collect that sample and we treated it as missing data. Participants used a Salivette device (SARSTEDT, Germany) to collect saliva samples. The saliva samples were stored at 2–8 °C for 7 days. To analyze the cortisol concentrations in the saliva samples, we used Cayman’s cortisol enzyme-linked immunosorbent assay kit (Cortisol Express, Cayman Chemical, Ann Arbor, MI). This kit is used to determine cortisol concentrations based on the principle of competitive antigen–antibody binding. The reproducibility of the correlation coefficient of 61 samples in duplicate (r = .97) was 15%, and the intra-assay coefficient of variability (CV) of 10 samples assayed 10 times was 17.8%. The smallest testing profile was 0.012 ng/ml. We explained the procedure for collecting the saliva to each participant. Participants placed the cotton swab of the collector device under their tongue for at least 3 min. We asked them not to brush or floss their teeth to avoid bleeding of the gums and to refrain from consuming food or fluids 30 min prior to each sample collection. Furthermore, we instructed them to store collected saliva samples in the freezer until they transported them to us using cold packs and bags.
PVT
The 5-min PVT was performed using PVT-192 (Ambulatory Monitoring Inc.). The PVT measures readiness for rapid response to a stimulus in order to assess sustained attention. Numbers are presented at randomly varying intervals from 3 to 7 s. Participants are instructed to quickly press a button immediately after a red number appears on a millisecond counter. This test is the gold standard for measuring the neurological behavior associated with sleep loss (Basner & Dinges, 2011; Basner, Mcguire, Goel, Rao, & Dinges, 2015). Researchers report it to be highly reliable, have a high intra-class correlation for key indicators, and have high sensitivity to the association between behavioral alertness and sleep loss (Basner & Dinges, 2011). In the present study, we recorded the following attention parameters: (a) mean RT, average correct RT; (b) median RT, median of the correct RT; (c) lapses, RT > 500 ms; (d) fastest 10% RT, the fastest 10% of response times for all trials, which indicated the best performance a participant was capable of producing; (e) slowest 10% 1/RT, the slowest 10% of reciprocal response times for all trials, which indicated slowing of the vigilance response; and (f) reaction speed, reciprocal response time (mean 1/RT) measured in seconds. We analyzed PVT data using standard REACT software, version 1.1.05. The research assistant brought the PVT instrument to participants and assisted them in completing the PVT test before work (7:30–8:00) on the 5th workday in the 4th week of the work schedule.
Statistical Analysis
SPSS, Version 23.0 (SPSS Inc., Chicago, IL), was used to perform data entry and statistical analysis. We describe continuous variables as means and standard deviations and categorical variables as frequencies and percentages. To compare differences in continuous variables between the HSQ and LSQ groups, we used Student’s t test. Because the distribution of SOL was not symmetrical, we used the Mann–Whitney U test to compare differences in SOL between the two groups. To compare differences in categorical variables between the groups, we used the χ2 test. For demographic variables, such as marital status, we used Fisher’s exact test to compare differences between the HSQ and LSQ groups.
Analysis of the cortisol slope involved calculation of slope0–30 min, slope0–6 hr, slope0–12 hr, slope30 min to 12 hr, and slope6–12 hr, which indicated differences in the cortisol concentration between two time points. A flatter slope represented a slower decline in the cortisol concentration during the day. We performed linear regression to analyze associations between independent demographic factors and cortisol profile slopes and PVT parameters. We subsequently modeled significant factors in multiple linear regressions. Statistical significance was defined as p < .05, and missing values were excluded from the analysis.
Ethical Considerations
The Taipei Medical University Joint Institutional Review Board approved this study (IRB: N201711007). We obtained written informed consent from each participant and assured participants that their personal information would be kept confidential and used only for academic purposes. Moreover, we informed them that they could withdraw from the study at any time, irrespective of the reason, without any negative consequences.
Results
We collected a total of 61 sleep recordings and PVT tests. Out of 244 collected saliva samples, we excluded two with missing data (missing data rate = 0.82%), resulting in 242 saliva samples. Table 1 lists demographic variables, lifestyle habits, and sleep parameters for participants by group. We found no significant differences in age, work experience, marital status, education level, or smoking and drinking habits between the LSQ and HSQ groups. A higher percentage of the nurses in the LSQ group reported consuming caffeinated beverages compared to the HSQ group (44.8% vs. 18.8%; p = .03). While the average bedtime did not differ significantly between the two groups (23:05 ± 1:02 for HSQ vs. 22:44 ± 1:10 for LSQ; p = .22), the average wake-up time did (6:18 ± 0.26 for HSQ vs. 5:55 ± 0.47 for LSQ; p = .02). Among the actigraphy sleep parameters, TST and SE were longer and higher, respectively, in the HSQ group than in the LSQ group. Furthermore, WASO and SOL were shorter in the HSQ group than in the LSQ group; however, the difference was not significant.
Demographic Variables, Lifestyle Habits, and Sleep Parameters by Study Group.
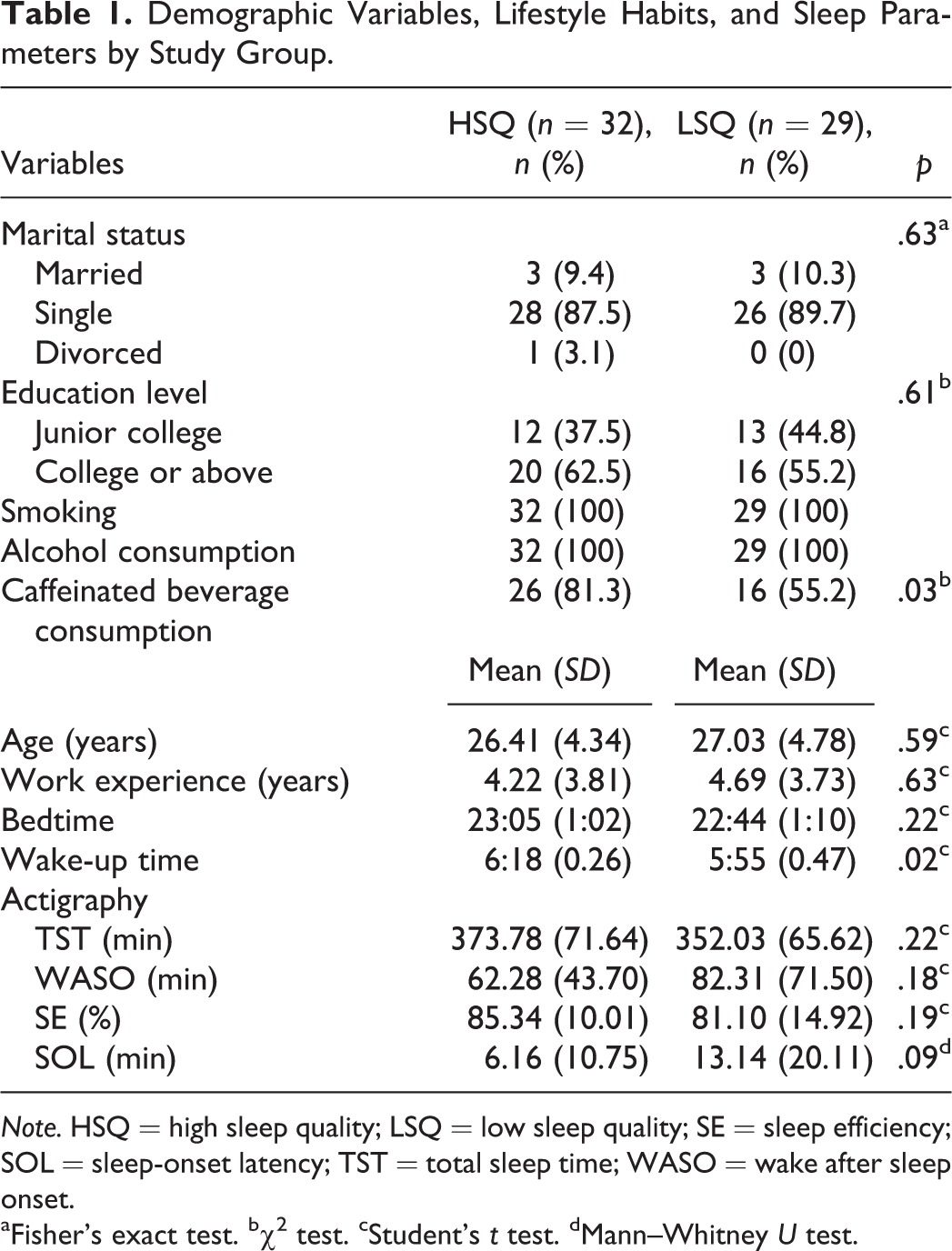
Note. HSQ = high sleep quality; LSQ = low sleep quality; SE = sleep efficiency; SOL = sleep-onset latency; TST = total sleep time; WASO = wake after sleep onset.
aFisher’s exact test. bχ2 test. cStudent’s t test. dMann–Whitney U test.
We compared the diurnal cortisol profiles of the two groups. At 30 min after awakening, the mean cortisol concentration in the HSQ group (11.79 ± 5.80 ng/mL) was significantly higher than that in the LSQ group (9.15 ± 3.33 ng/mL; p = .04). Moreover, at 12 hr after awakening, the mean cortisol concentration in the HSQ group (2.40 ± 2.48 ng/ml) was significantly lower than that in the LSQ group (4.37 ± 4.92 ng/mL; p = .05). The cortisol profile slopes also differed significantly between the two groups (slope0–30 min: 3.91 ± 5.90 for HSQ vs. −.46 ± 5.77 for LSQ, p < .01; slope30 min to 12 hr: −.78 ± .53 for HSQ vs. −.39 ± .39 for LSQ; p < .01; Table 2 and Figure 2).
Cortisol Profiles, Cortisol Slopes, and Psychomotor Vigilance Task (PVT) Parameters by Study Group.
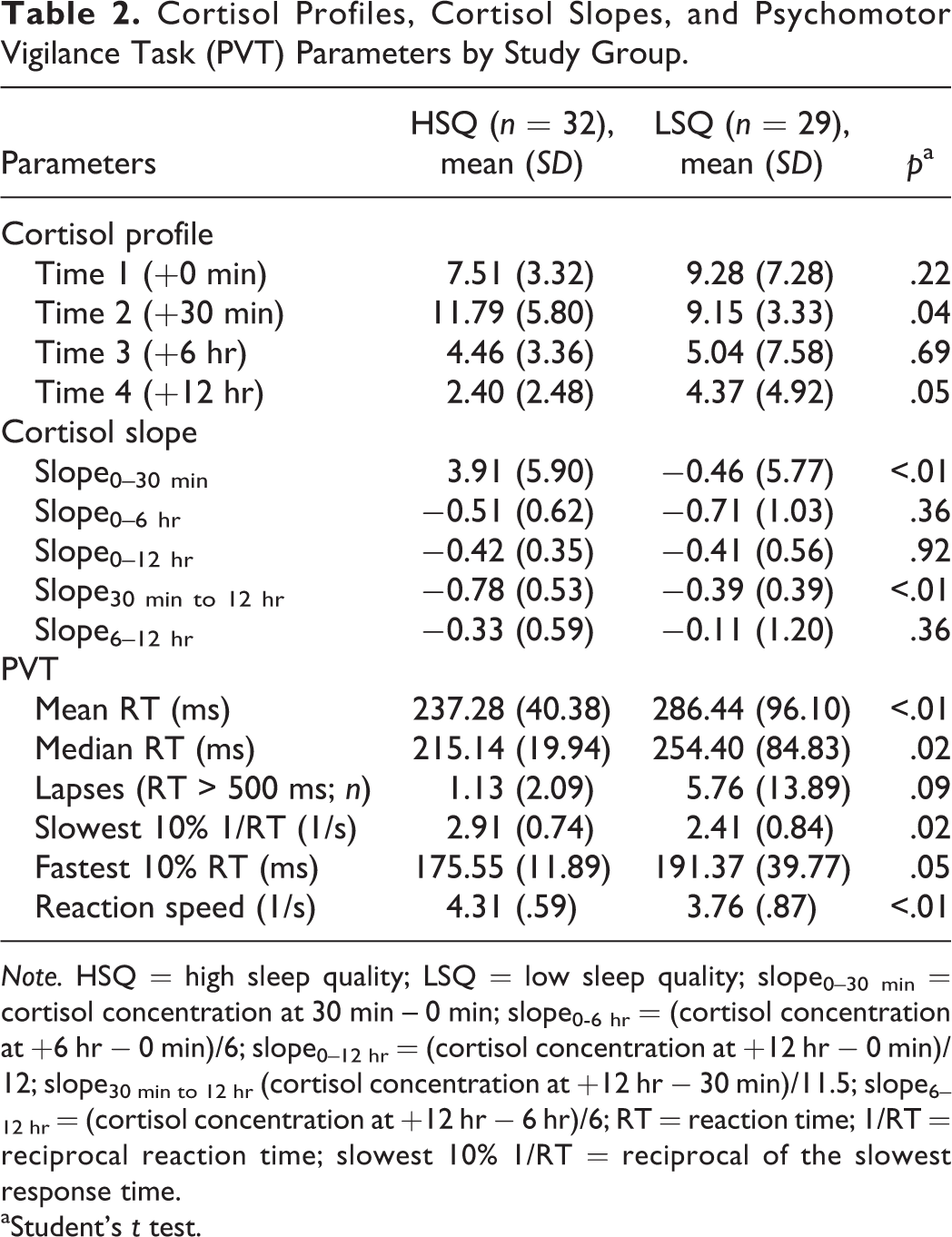
Note. HSQ = high sleep quality; LSQ = low sleep quality; slope0–30 min = cortisol concentration at 30 min – 0 min; slope0-6 hr = (cortisol concentration at +6 hr − 0 min)/6; slope0–12 hr = (cortisol concentration at +12 hr − 0 min)/12; slope30 min to 12 hr (cortisol concentration at +12 hr − 30 min)/11.5; slope6–12 hr = (cortisol concentration at +12 hr − 6 hr)/6; RT = reaction time; 1/RT = reciprocal reaction time; slowest 10% 1/RT = reciprocal of the slowest response time.
aStudent’s t test.
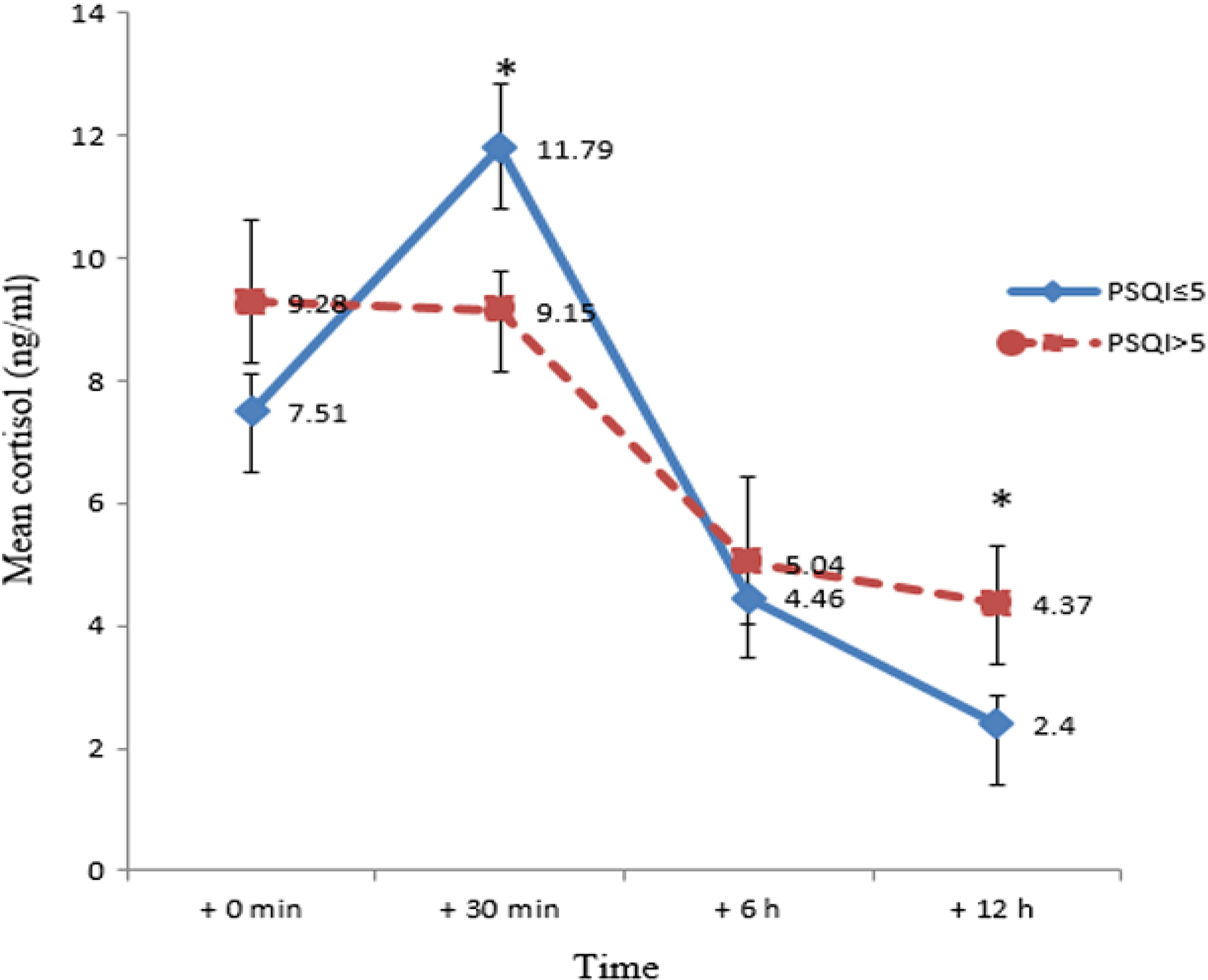
Mean cortisol concentrations at study time points for the high sleep quality (Pittsburgh Sleep Quality Index [PSQI]
With regard to PVT parameters, the two groups exhibited significant differences in mean RT (237.28 ± 40.38 ms for HSQ vs. 286.44 ± 96.10 ms for LSQ, p < 0.01), median RT (215.14 ± 19.94 ms for HSQ vs. 254.40 ± 84.83 ms for LSQ, p = .02), slowest 10% 1/RT speed (1/2.91 ± 1/.74 s for HSQ vs. 1/2.41 ± 1/.84 s for LSQ, p = .02), fastest 10% RT (175.55 ± 11.89 ms for HSQ vs. 191.37 ± 39.77 ms for LSQ, p = .05), and reaction speed (1/4.31 ± 1/.59 s for HSQ vs. 1/3.76 ± 1/.87 s for LSQ, p < .01). The LSQ group had a longer RT and slower speed than did the HSQ group (Table 2).
In our multiple linear regression analyses, we adjusted for age, work experience, marital status, education level, and caffeinated beverage consumption. Because we did not find wake-up time to be significant via multiple linear regression, we did not adjust for this variable in the final model. The cortisol slope0–30 min was 4.67 points higher in the HSQ group than in the LSQ group (95% confidence interval [CI] = [1.33, 8.01], p < .01). The cortisol slope30 min to 12 hr was 0.34 points lower in the HSQ group than in the LSQ group (95% CI = [−.62, −.7], p = .02). The mean and median RT were 44.16 ms (95% CI = [−82.11, −6.20], p = .02) and 33.75 ms (95% CI = [−64.39, −3.11], p = .03) shorter in the HSQ group than in the LSQ group. The slowest 10% 1/RT and reaction speed were .50 s (95% CI = [0.06, 0.94], p = .03) and .51 s faster in the HSQ group than in the LSQ group (Table 3).
Multiple Linear Regression Analysis Factors with the Cortisol Profile Slope and Psychomotor Vigilance Task (PVT).
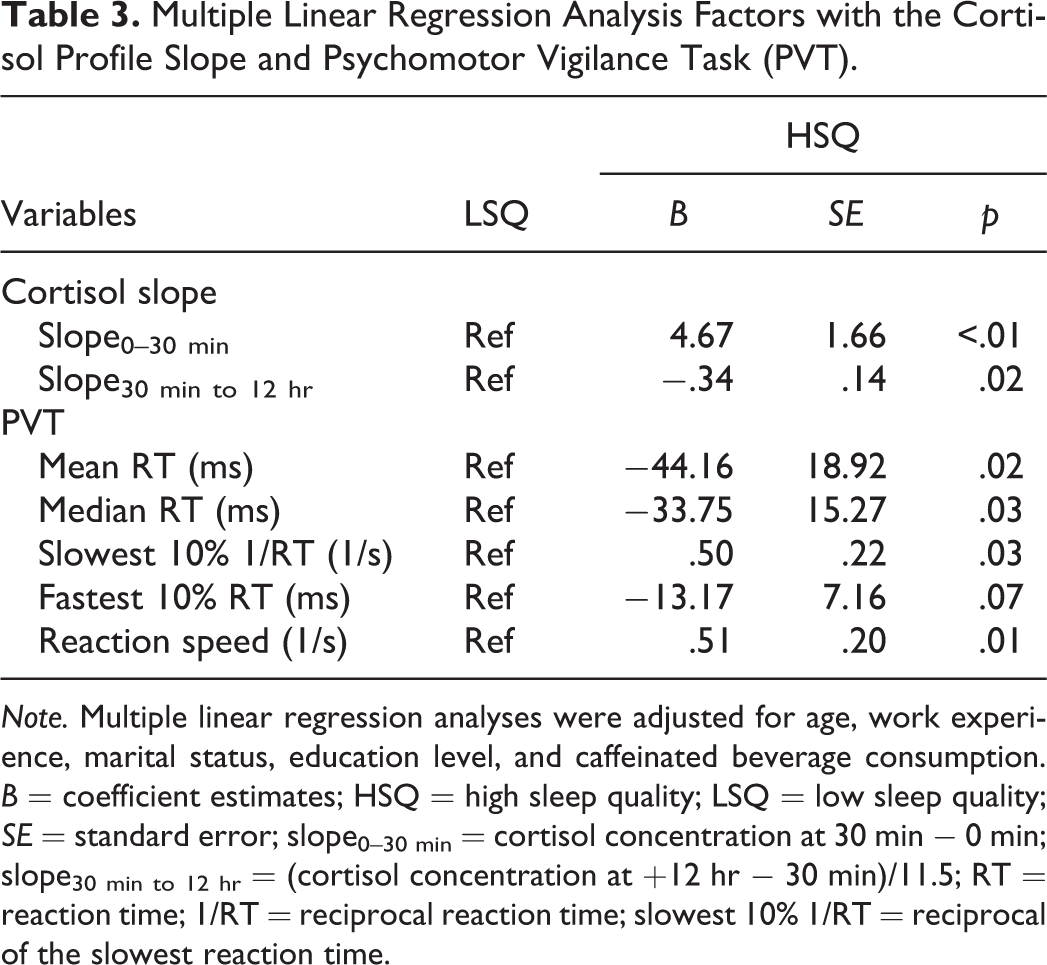
Note. Multiple linear regression analyses were adjusted for age, work experience, marital status, education level, and caffeinated beverage consumption. B = coefficient estimates; HSQ = high sleep quality; LSQ = low sleep quality; SE = standard error; slope0–30 min = cortisol concentration at 30 min − 0 min; slope30 min to 12 hr = (cortisol concentration at +12 hr − 30 min)/11.5; RT = reaction time; 1/RT = reciprocal reaction time; slowest 10% 1/RT = reciprocal of the slowest reaction time.
Discussion
In the present study, we investigated whether nighttime sleep quality affected the diurnal cortisol profile and attention after wake up during the subsequent day in nurses working the day shift. As we hypothesized, compared with the HSQ group, the LSQ group exhibited impaired HPA-axis regulation, with a flatter CAR and diurnal cortisol slope and poor sustained attention in the morning.
We used the subjective self-administered CPSQI Questionnaire to categorize the participants into the HSQ and LSQ groups. The subjective sleep-quality assessment results were consistent with the objective actigraphy measurements, with the HSQ group having greater TST, higher SE, and shorter WASO and SOL than the LSQ group. This consistency between instruments suggests the accuracy of our categorization based on subjective sleep quality.
We also found that a greater percentage of nurses in the LSQ group reported consumption of caffeinated beverages than in the HSQ group. Shilo et al. (2002) found that the consumption of caffeinated beverages reduced TST and sleep quality to a larger extent than did the consumption of decaffeinated beverages. Lemma et al. (2012) reported that participants who consumed caffeinated beverages every week had a sleep latency that was 1.48 times longer than that of those who consumed noncaffeinated beverages. Our present findings are consistent with these previous findings, as the LSQ group also had shorter TST and longer SOL than did the HSQ group.
Our results revealed that the LSQ group had a higher cortisol concentration at awakening (+0 min) than did the HSQ group. Cortisol secretion is normally lowest at approximately midnight and increases gradually toward morning. During restless sleep, corticotropin-releasing hormone (CRH) impairs sleep and enhances vigilance. CRH stimulates the release of adrenocorticotropic hormone, which is the prime regulator of nocturnal cortisol secretion. The increasing cortisol level during the early morning results in shallow sleep and intermittent wakefulness (Steiger, 2002). Hatzinger et al. (2008) reported that an LSQ group with a greater WASO exhibited significantly higher morning awakening cortisol levels than did an HSQ group.
In the present study, the LSQ group also exhibited a flatter CAR and smaller diurnal slope30 min to 12 hr than did the HSQ group. These findings are consistent with those of Castro-Diehl et al. (2015) and Hansen et al. (2012), who reported that LSQ caused a flatter CAR and a less pronounced wake-to-bed slope. The HPA axis is one of the major components contributing to a higher cortisol level upon awakening (Buckley & Schatzberg, 2005). The normal diurnal circadian cortisol concentration is highest at approximately 30 min after awakening, which reflects a healthy cortisol circadian rhythm and is an indicator of optimal HPA-axis function (Fries et al., 2009; Tsigos & Chrousos, 2002). The CAR plays a crucial role in an organism’s efforts to adjust to psychological, behavioral, and physiological changes (Clow et al., 2010; Tsigos & Chrousos, 2002). Backhaus et al. (2004) reported that the CAR significantly decreased with a higher frequency of nocturnal awakenings, which reduced the feeling of recovery after awakening; furthermore, the LSQ group in their study had a flatter diurnal cortisol slope than did the control group between 30 min after awakening and evening.
Sleep regulation is controlled by the brain and neurotransmitter system. Researchers have found associations between LSQ and cognitive problems (Waters & Bucks, 2011). Cognitive function depends on the integrity of the hippocampal and prefrontal cortical circuits. In one study, researchers reported that an attenuated CAR and subsequently less steep diurnal cortisol slope were associated with poor declarative memory and executive function (Evans et al., 2011). With a well-functioning system, at 20–30 min after awakening, cerebral blood flow is most rapidly reestablished in the centrencephalic regions, and the reactivation of these regions underlies the reestablishment of conscious awareness (Balkin et al., 2002). A greater CAR results in greater cognitive neural activity and fewer false alarms (Shi et al., 2018). The PVT assesses sustained attention as a measure of neurocognition after sleep loss (Basner & Dinges, 2011). In the present study, PVT results showed that the LSQ group had significantly slower RTs than did the HSQ group. These results are consistent with those of Yang et al. (2018), who indicated that sleep deprivation increased RT and reduced processing speed and attention.
The present study had several limitations to keep in mind. Although light and noise affect the circadian pattern of cortisol secretion, we did not control these variables in the present study. In future studies, researchers should consider controlling ambient lighting and noise. Furthermore, the HPA axis is adversely affected by stress. In the present study, we enrolled participants from the general medical or surgical ward to increase the likelihood that they experienced an average level of job stress. However, we did not control for additional potential confounders such as the menstrual cycle phase. In addition, we only measured the attention status of day-shift nurses before they began work to determine the effects of sleep quality on attention status after waking up; therefore, we do not know the status of the attention of these nurses when they were off duty. Finally, we sampled only a single day in the present study. In future research, investigators should consider measuring longitudinal associations between sleep quality and cortisol and attention over several days.
Conclusions
In the present study, LSQ resulted in a smaller CAR and flatter morning−evening cortisol slope, which indicate dysregulation of HPA-axis function. Such dysregulation adversely affects the level of sustained attention in the morning, which was also evident in our findings. Nursing staff play a critical role in patient care. They must maintain a high level of concentration while working to maximize their efficiency and ensure optimal work performance. Factors that cause sleep interruptions should be eliminated to reduce nocturnal awakening and promote HSQ. A comprehensive understanding of the effects of sleep quality on circadian cortisol secretion and attention performance may provide incentive for nursing staff to develop optimal sleep patterns for maintaining health and work safety, such as eliminating factors that cause sleep interruptions to reduce nocturnal awakenings.
Footnotes
Authors' Note
Shu-Fen Niu is also affiliated with Department of Nursing, Shin Kong Wu Ho-Su Memorial Hospital, Taipei, Taiwan.
Author Contribution
J. C. Tsai contributed to conception and acquisition, critically revised manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy. K. R. Chou contributed to conception and interpretation, critically revised manuscript, and gave final approval. H. T. Tsai contributed to design and interpretation, drafted manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Y. C. Yen contributed to design and analysis, drafted manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy. S. F. Niu contributed to conception, design, acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Science and Technology, Taiwan (MOST 107-2314-B-038-008) and Taipei Medical University, Taiwan (TMU106-AE1-B11).