
Abstract
Purpose:
Hepatocellular carcinoma (HCC) is the second leading cause of cancer mortality worldwide. Sleep problems are common in HCC patients and may be attributable to disturbances in the circadian rhythm. Research into the role of circadian rhythms in sleep quality among HCC patients is lacking, however. This study investigated the relationship between the diurnal cortisol profile and sleep quality among HCC patients. We aimed to identify alterations in the diurnal cortisol profile in patients with HCC compared to healthy controls and investigate whether they were associated with poor sleep quality among HCC patients.
Methods:
Participants comprised 75 HCC patients and 33 healthy individuals. The Taiwanese version of the Pittsburgh Sleep Quality Index (PSQI-T) was administered to assess sleep quality. Saliva samples were collected on 3 consecutive days at five time points daily to measure diurnal cortisol levels.
Results:
In the HCC group, 89.3% of individuals were poor sleepers (PSQI-T > 5), whereas among healthy individuals, 30.3% were poor sleepers. While the healthy participants’ diurnal cortisol profile followed a typical pattern that peaked 30 min after waking and declined gradually throughout the day, the cortisol level in the HCC patients rebounded at bedtime. Higher cortisol levels were marginally correlated with poor sleep quality (OR = 1.00007, p < .05).
Conclusions:
Our study suggests a potential association between disturbed circadian rhythm and poor sleep quality in HCC patients. Further investigation of the causal relationship between sleep and circadian rhythm is warranted.
Hepatocellular carcinoma (HCC) is the second leading cause of cancer mortality worldwide (Johnson et al., 2017). Many staging systems and liver reserve models have been proposed to predict the prognosis of HCC. Most patients with HCC have underlying cirrhosis, and liver functional reserve is one of the key prognostic factors for HCC (Jaruvongvanich, Sempokuya, & Wong, 2018). Child–Pugh scores are widely applied to estimate liver functional reserves in patients with HCC: Grade A indicates well-compensated disease, Grade B indicates disease involving significant functional compromise, and Grade C indicates decompensated liver disease (S. Y. Ho et al., 2017).
Reports indicate a high prevalence of sleep disturbances among patients with liver diseases (Chu, Yu, Chen, Peng, & Wu, 2011; Hamdan et al., 2014). HCC patients with sleep problems show a decrease in their functioning and quality of life (Chu et al., 2011; Huang & Lin, 2009). Research has also demonstrated an association between disturbed sleep and a higher rate of cancer incidence, mortality, and progression (Lehrer, Green, Ramanathan, & Rosenzweig, 2013; Liang et al., 2012; Palesh et al., 2014).
The exact mechanism of sleep disturbance in patients with HCC is not well known. Emerging evidence has indicated a strong correlation between sleep disturbances and disturbed circadian rhythms in cancer patients (Ancoli-Israel, Moore, & Jones, 2001). Circadian rhythms, defined as physiological processes that occur with a repeating period of approximately 24 hr, govern several physiologic processes, such as sleep and wakefulness, activity, temperature, and cognitive function (Barclay, Tsang, & Oster, 2012). Cortisol, the main glucocorticoid hormone produced by the adrenal glands after the activation of the hypothalamic–pituitary–adrenal (HPA) axis, is secreted in a circadian rhythm, with high levels in the early morning and low levels in the evening and night (Chrousos, 1995; Clow, Hucklebridge, & Thorn, 2010; Stone et al., 2001). Growing evidence suggests that disturbed circadian rhythms may be a risk factor in some cancers (Fu & Lee, 2003; Keith, Oleszczuk, & Laguens, 2001; Moser, Schaumberger, Schernhammer, & Stevens, 2006). In particular, research in HCC has shown that downregulation of circadian genes leads to circadian rhythm disturbances, which may promote the selective survival of cancerous cells and carcinogenesis, contributing to the development of HCC (Lin et al., 2008). In addition, a growing body of evidence based on the measurement of the daily rhythm of salivary cortisol concentrations suggests that a disruption of circadian rhythms may be associated with the progression of a variety of cancers (Kim et al., 2012; Sephton et al., 2013; Sephton, Sapolsky, Kraemer, & Spiegel, 2000). Clearly, there is an association between disturbed circadian rhythms and cancer development and progression.
Several studies have demonstrated that the diurnal cortisol profiles of women with metastatic breast cancers (Abercrombie et al., 2004) and patients with advanced cancers (Sephton et al., 2000) were more flattened compared to those of healthy individuals. Further, Kumari et al. (2009) showed that flatter diurnal slopes were linked to sleep disturbances. Elevated evening cortisol levels have been linked to increased sleep disturbances in cancer patients (Kumari et al., 2009; Weinrib et al., 2010) and might even predispose patients to cancer progression (Zeitzer et al., 2016). On the other hand, sleep disturbances and disturbed circadian rhythms may also be due, at least in part, to cancer treatments, the time of their administration, and the quality of life of cancer patients (L. Liu & Ancoli-Israel, 2008).
There has been little research on circadian rhythm disturbances and their link with sleep disturbances in HCC patients. In the present study, we aimed to (1) determine whether there are any alterations in the diurnal cortisol profile in patients with HCC as compared to healthy controls and (2) investigate whether these alterations are associated with poor sleep quality among HCC patients.
Method
Study Design
We conducted this prospective study between September 2007 and January 2010 among patients with HCC and healthy individuals. While we assessed subjective sleep quality by questionnaire during recruitment, we collected salivary samples from participants to measure cortisol levels for 3 consecutive days.
Participants and Settings
We recruited 75 patients with HCC and 33 age- and gender-matched healthy controls for the study, based on a male-to-female ratio of liver cancer incidence of 3:1 (C. H. Liu, Tsai, & Chen, 2013). Participant recruitment for the HCC group occurred at the gastrointestinal outpatient clinics of a medical center (ChangHua Christian Hospital) and a regional hospital (Jen-Ai Hospital) in Taiwan, in which patients were treated on an outpatient basis and were not under surgical treatment. The inclusion criteria were as follows: (a) age ≥ 20 years, (b) diagnosis of HCC without cirrhosis or with stable cirrhosis, and (c) ability to understand Mandarin. The exclusion criteria were as follows: diagnosis of a sleep disorder (e.g., narcolepsy, obstructive sleep apnea, restless legs syndrome, or chronic insomnia), hepatic encephalopathy, or employment in a job with rotating shifts or permanent night shift. We recruited healthy participants from a leisure club in the mid-Taiwan area. The inclusion criteria were as follows: (a) age ≥ 20 years, (b) negative history of any chronic illness, and (c) ability to understand Mandarin. A recruitment flowchart appears in Figure 1. The institutional review boards of ChangHua Christian Hospital, ChangHua, Taiwan (CCH IRB 070707), and Jen-Ai Hospital, Taichung (97-03) approved the study. Each patient received appropriate information about the study objectives and methods and signed an informed consent form.
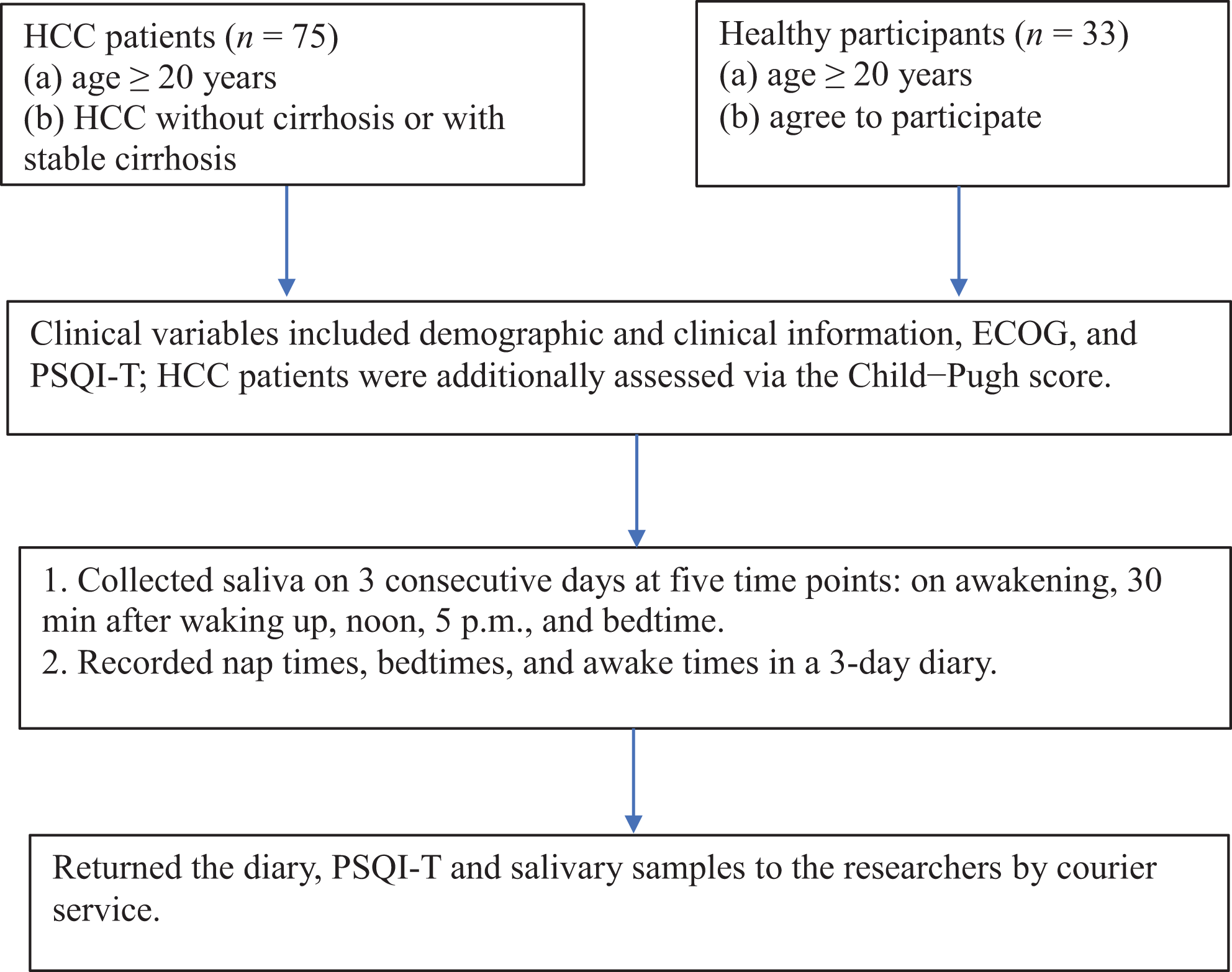
Flowchart of the recruitment and data collection process. CI = confidence interval; ECOG = Eastern Cooperative Oncology Group status; HCC = hepatocellular carcinoma; OR = odds ratio; PSQI-T = Taiwanese version of the adjusted Pittsburgh Sleep Quality Index.
Salivary Cortisol Measurement
We measured salivary cortisol levels as a proxy for the levels of physiologically active free cortisol in the blood (Maruyama et al., 2012; Monteleone et al., 2011) to capture the diurnal cortisol profile in a relatively noninvasive way. A previous study comparing salivary cortisol levels with serum total cortisol levels through radioimmunoassay revealed that they were comparable under both basal and stimulated conditions (Gozansky, Lynn, Laudenslager, & Kohrt, 2005).
We provided 15 take-home salivary cortisol sampling kits (Salivette devices: Sarstedt, Newton, NC) for each participant with instructions on how to collect the saliva. To collect whole, unstimulated saliva, participants tilted their head forward, allowing the saliva to pool on the floor of the mouth and then passed the pooled saliva through a short straw into the kit. We asked participants to collect their saliva on 3 consecutive days at five time points: on waking, 30 min after waking, 12 p.m., 5 p.m., and bedtime. During the 3 days, we contacted participants by telephone to ensure compliance. Participants also recorded their nap times, bedtimes, and wake times in a 3-day diary. They stored the kits in their refrigerator until returning them to us by courier service together with the diary.
We centrifuged, aliquoted, and stored the samples at −70°C until further analysis using an enzyme immunoassay (Salimetrics, State College, PA). We used five parameters for cortisol levels in the present study, including (a) mean daily cortisol levels, (b) mean cortisol levels at each sampling time point, (c) peak cortisol levels (i.e., the highest cortisol level of each day), (d) slope produced by regressing the cortisol level of the second time point (30 min after waking) on the first time point (waking), and (e) total cortisol concentration from waking to 30 min after waking area under curve (AUC).
Sleep Quality Measurement
We measured sleep quality using the Taiwanese version of the 19-item Pittsburgh Sleep Quality Index (PSQI-T), which covers seven domains: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction. Domain scores range from 0 (no difficulty) to 3 (severe difficulty), while total scores range from 0 to 21, with higher scores indicating more severe sleep problems. A global PSQI-T score > 5 is indicative of poor sleep quality with high sensitivity and specificity (Buysse, Reynolds, Monk, Berman, & Kupfer, 1989). To match the time frame of cortisol measurement, we replaced the term last month in the respondent instructions for the PSQI to last week. A previous study in Taiwan showed that the PSQI-T has a Cronbach’s α of .79 and a test–retest reliability of .91 (Tzeng, Fu, & Lin, 2012). In the present study, the Cronbach’s α for the global PSQI-T was .80.
Other Variables
We administered an investigator-designed questionnaire to record demographic information, performance status, and the Child–Pugh score. We assessed performance status based on the Eastern Cooperative Oncology Group Scale (ECOG; Oken et al., 1982). The ECOG Scale describes a patient’s level of functioning in terms of their ability to care for themselves, daily activity, and physical ability, with scores ranging from 0 (fully active) to 5 (dead). It is widely used for measuring performance status due to its simplicity and intra-observer reproducibility. We retrieved the Child–Pugh score, a scoring system used to determine the prognosis of cirrhosis, from the medical records (Sloss & Kubler, 2009). The score incorporates five variables (i.e., bilirubin, albumin, prothrombin time, ascites, and encephalopathy). The score allows for the categorization of patients into Child–Pugh Grades A, B, and C, with prognosis worsening from A to C.
Data Analysis
We used a t test and χ2 test to determine the differences in the demographic and clinical variables and the PSQI scores between the groups for continuous and categorical data, respectively. To examine the relationship between cortisol levels and poor sleep in HCC patients and healthy controls separately, we employed generalized estimating equations (GEEs). In addition to cortisol levels, we added age, sex, occupational status, ECOG, and sampling time points to the model either because they showed significant between-group differences in the t tests or were considered to be confounding variables that could affect sleep quality. We chose to use the GEE approach because it is suitable for analyzing nonindependent longitudinal data, such as data collected over 3 consecutive days. We conducted all statistical analyses using the Statistical Package for the Social Sciences (Version 23; SPSS Inc., Chicago, IL). In addition, we calculated the following descriptive statistics to display the parameters associated with the diurnal cortisol profile: mean daily cortisol levels, mean cortisol levels at each sampling time point, peak cortisol levels, slope, and AUC. We used t tests to assess the difference in mean cortisol levels at each time point between the following subgroups: healthy controls versus HCC patients, Class A HCC patients versus Classes B and C patients (we pooled B and C patients because of the particularly high prevalence of Class A patients), good sleepers with Class A HCC versus healthy good sleepers (we did not select Classes B and C HCC patients because of the absence of good sleepers), and poor sleepers with Class A HCC versus healthy poor sleepers.
Results
Descriptive Statistics for the Demographic Data
The sample consisted of 75 HCC patients and 33 healthy individuals. The questionnaire data were available for all 108 participants, while the salivary cortisol data of 6 HCC patients were incomplete because the participants had forgotten to collect their saliva at certain time points. The demographic characteristics of the participants are presented in Table 1. The mean ages of the HCC and healthy groups were 61.25 (SD = 12.56) and 55.55 (SD = 11.55) years, respectively. The mean global PSQI-T scores were 11.17 (SD = 4.65) and 4.97 (SD = 3.07) in the patients with HCC and healthy controls, respectively (p < .001), indicating that patients with HCC had a poorer sleep quality. Within the HCC group, the proportions assigned to Child–Pugh Classes A, B, and C were 74.7%, 22.7%, and 2.6%, respectively. Based on the cutoff score of the PSQI-T (>5), 30.3% of healthy individuals were poor sleepers, while 89.3% of the HCC patients were poor sleepers. All patients in Child–Pugh Classes B and C were poor sleepers, while 85.7% of those in Child–Pugh Class A were poor sleepers.
Demographic and Clinical Characteristics (Mean [SD]) of the Participants.
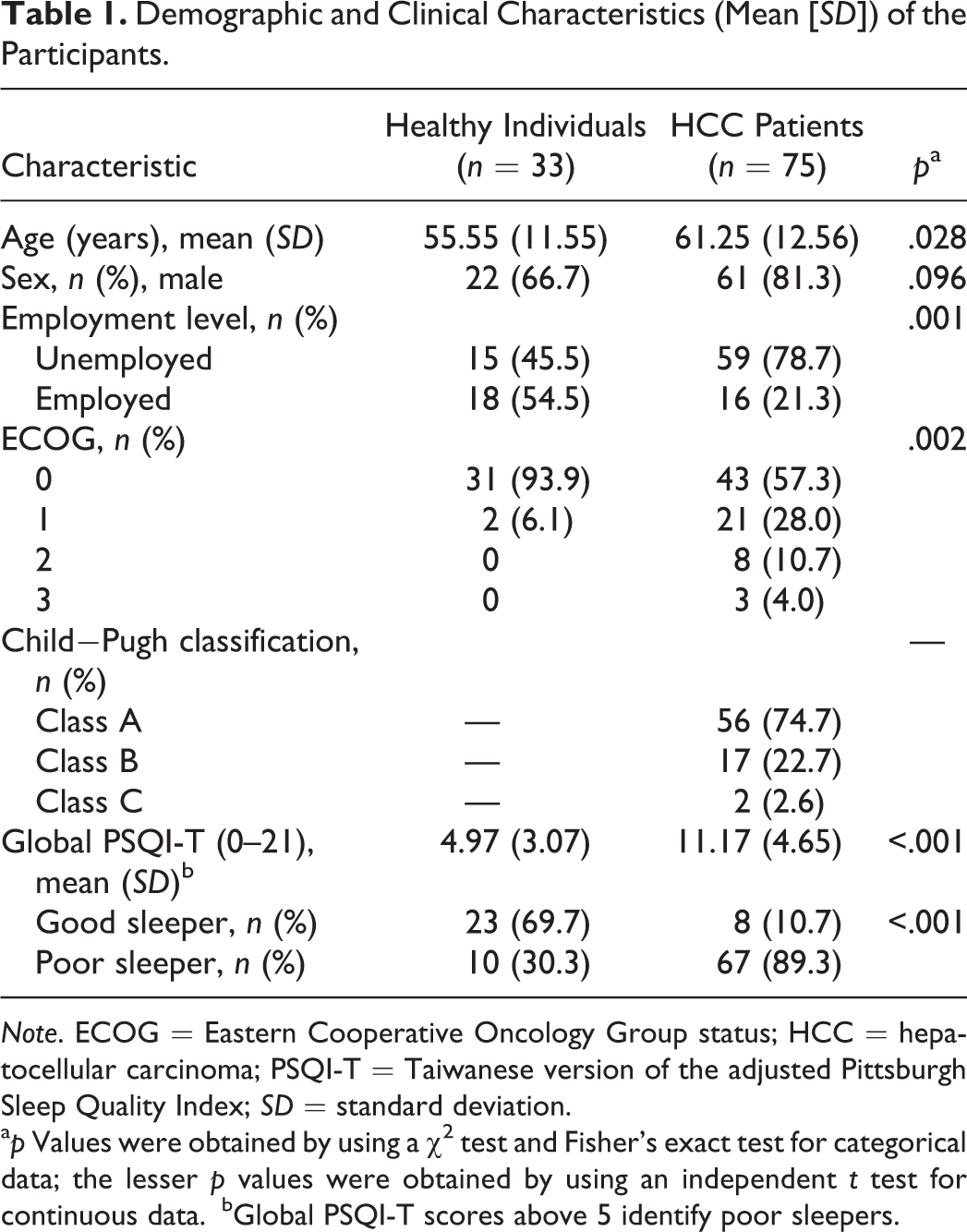
Note. ECOG = Eastern Cooperative Oncology Group status; HCC = hepatocellular carcinoma; PSQI-T = Taiwanese version of the adjusted Pittsburgh Sleep Quality Index; SD = standard deviation.
a p Values were obtained by using a χ2 test and Fisher’s exact test for categorical data; the lesser p values were obtained by using an independent t test for continuous data.
bGlobal PSQI-T scores above 5 identify poor sleepers.
Comparison of the Diurnal Cortisol Profile of HCC Patients and Healthy Individuals
The mean daily and peak cortisol levels in HCC patients on Days 1–3 were significantly higher than those in the healthy controls (Table 2). We also compared the mean cortisol levels between patients with HCC and healthy controls for each sampling time point. The cortisol levels at all five time points were significantly higher in patients with HCC than in the healthy controls (Table 3). In healthy individuals, cortisol secretion followed a diurnal rhythm that peaked 30 min after waking and declined throughout the day until bedtime. However, in patients with HCC, cortisol levels only slightly increased 30 min after waking in the morning, dropped throughout the day, and then rebounded at bedtime.
Daily Mean (SD) for Measurement Parameters Related to Salivary Cortisol Profile in Patients With Hepatocellular Carcinoma (HCC) and Healthy Controls.
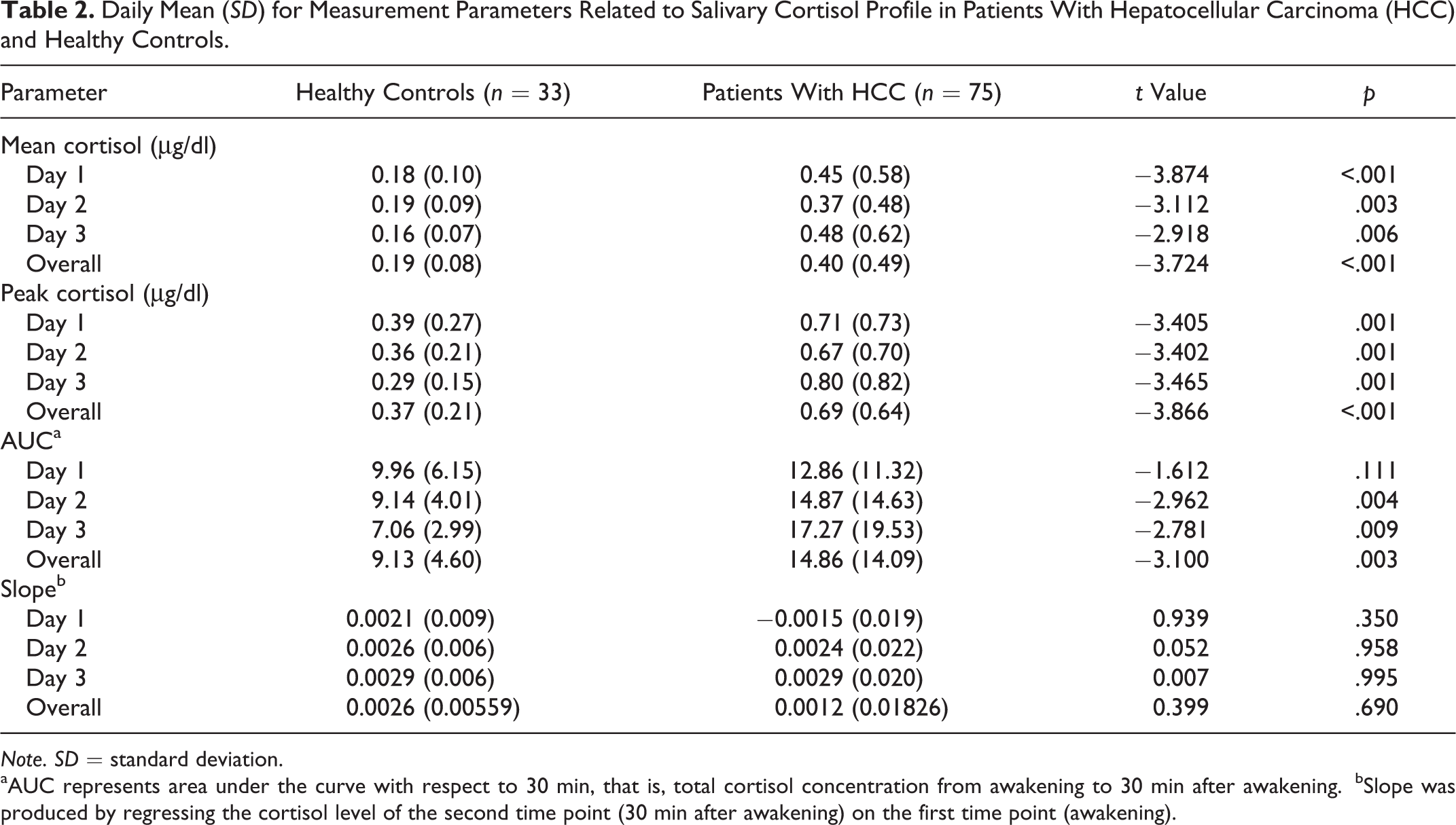
Note. SD = standard deviation.
aAUC represents area under the curve with respect to 30 min, that is, total cortisol concentration from awakening to 30 min after awakening.
bSlope was produced by regressing the cortisol level of the second time point (30 min after awakening) on the first time point (awakening).
Mean (SD) Salivary Cortisol Levels of Participants at Each Sampling Time Point.
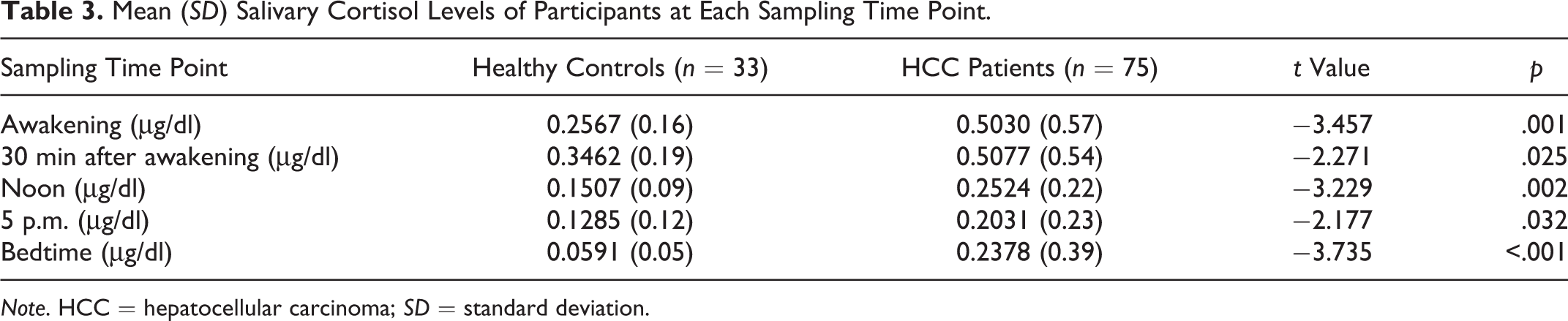
Note. HCC = hepatocellular carcinoma; SD = standard deviation.
In addition, within the HCC sample, we compared the salivary cortisol levels at each sampling time point between the Child–Pugh Class A group and the combined Child–Pugh Classes B and C groups (Figure 2). We pooled Child–Pugh Classes B and C patients into one group because of the low number of patients in those classes compared to Class A. The mean cortisol levels of the Classes B and C patients were higher than those of Class A patients at all time points except 5 p.m. However, the differences did not reach statistical significance.
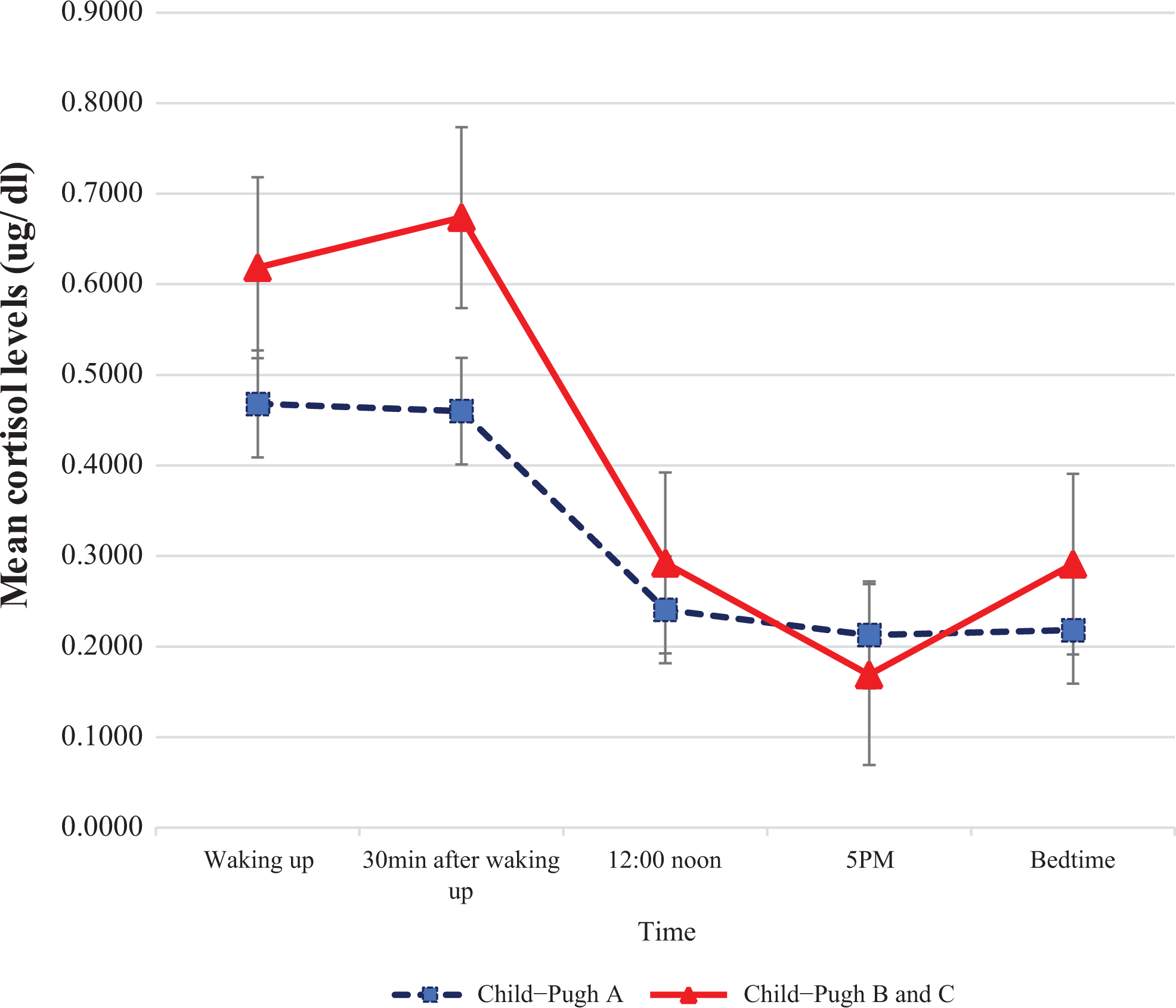
Mean cortisol levels at each time point across 3 consecutive days in hepatocellular carcinoma patients in Child−Pugh Class A versus Classes B and C together. t Tests indicated no significant differences between the groups.
Association Between Sleep Quality and Cortisol Profiles in HCC Patients
We performed separate GEEs that included poor sleep quality (PSQI-T > 5) as the exposure variable for patients with HCC and healthy controls. Age, sex, occupational status, ECOG, sampling time point, and cortisol level were also included in the GEE models. Table 4 lists the variables for which we found significant results. HCC patients who were employed were less likely to report poor sleep quality (OR = 0.218, p < .05) than HCC patients who were not employed. HCC patients with higher daily cortisol levels tended to report poorer sleep quality; however, the association was very weak (OR = 1.00007, p = .045). Among healthy participants, we found no predictor of poor sleep.
Generalized Estimating Equation Model Evaluating the Effects of Different Variables on Poor Sleep in Participants.
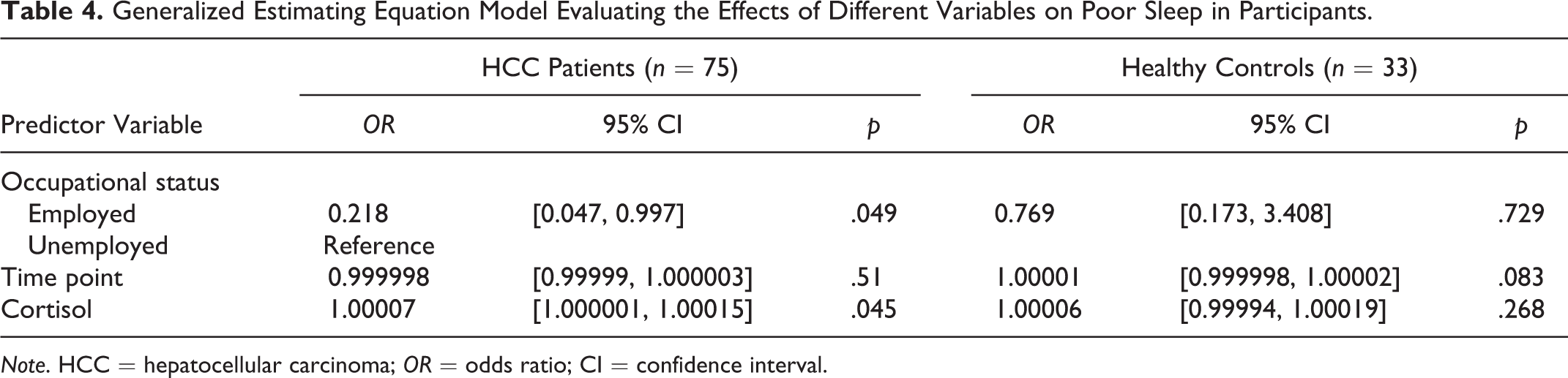
Note. HCC = hepatocellular carcinoma; OR = odds ratio; CI = confidence interval.
Salivary Cortisol Profiles Compared Between Good and Poor Sleepers in the HCC and Control Groups
We also compared the salivary cortisol profiles of good and poor sleepers in the HCC patients in Child–Pugh A group with those of the healthy control group (Figure 3). We did not include Child–Pugh B and C patients because all were poor sleepers. The mean cortisol levels at all five time points appeared higher in patients with Child–Pugh A than in the healthy participants, but the difference did not reach statistical significance. Among the healthy participants, good and poor sleepers reported a close cortisol level from noon to bedtime, dropping to the nadir of the five time points at bedtime. On the contrary, poor sleepers with Child–Pugh Class A HCC showed a slight increase in cortisol level at bedtime, and the bedtime cortisol level of poor sleepers with Child–Pugh Class A was significantly higher than that of healthy poor sleepers (p < .0001).
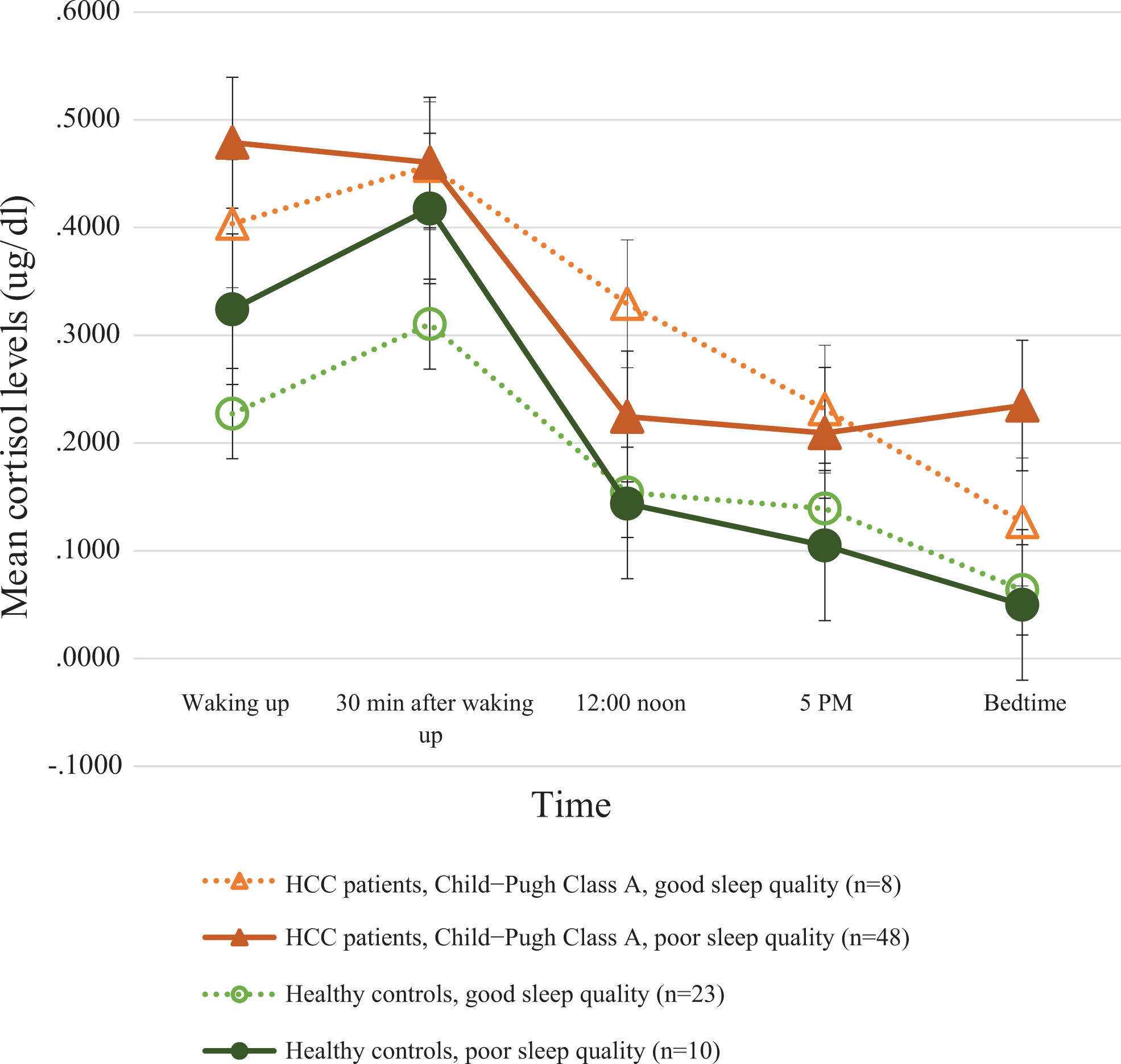
Mean cortisol levels at each time point across 3 consecutive days in good and poor sleepers among hepatocellular carcinoma (HCC) patients in Child−Pugh Class A and healthy controls. The only significant difference was between poor sleepers in the two groups, as indicated by the reported p value.
Discussion
The present study is the first to explore circadian rhythm disturbance in HCC patients and its link with sleep disturbances. Our findings demonstrate the presence of a disturbed diurnal cortisol profile and higher levels of sleep disturbance among patients with HCC compared to healthy individuals. Specifically, the self-reported sleep quality of HCC patients was significantly poorer than that of healthy controls. The mean daily and peak cortisol levels were significantly higher in patients with HCC than in healthy controls. While the healthy participants’ diurnal cortisol secretion followed a typical pattern that peaked 30 min after waking and declined gradually throughout the day, the cortisol level in the HCC patients rebounded at bedtime, reflecting a potential disturbance in their circadian rhythm. Higher daily cortisol levels were marginally correlated with poor sleep quality in HCC patients but not controls. These findings should be considered in clinical care and in the development of treatment approaches.
Previous research has found a high prevalence of sleep disturbance in patients with liver diseases (Chu et al., 2011; Hamdan et al., 2014). Our findings indicate that the self-reported sleep disturbance of HCC patients was significantly higher than that of the healthy controls. Compared to previous literature on cancer patients (Beck, Schwartz, Towsley, Dudley, & Barsevick, 2004; Fontes et al., 2017), the level of sleep disturbances in HCC patients as assessed by the PSQI-T in the present study was particularly high (current study 11.17 vs. a range for previous studies of 7.31–8.10). Although methodological differences should be considered, the marked difference in the PSQI global scores between HCC patients in the present study and patients with other cancer types in previous studies is worthy of further exploration. Future studies should use objective measures in conjunction with subjective measures to fully characterize sleep disturbances in patients across different cancer diagnoses.
Our findings extend previous studies reporting disturbed cortisol rhythms in patients with other cancer types and demonstrate for the first time that such disturbances also exist in HCC patients. Previous reports have noted disturbed patterns of cortisol secretion, often characterized by elevated nocturnal cortisol, in patients with various cancer types including breast and ovarian (Abercrombie et al., 2004; Jehn et al., 2010; Palesh et al., 2008; Weinrib et al., 2010). Schrepf et al. (2013) also found elevated cortisol levels in ovarian cancer patients compared to healthy controls. There are some plausible explanations for the disturbed cortisol rhythms present in HCC patients. First, they could be secondary to tumor-derived inflammation (Schrepf et al., 2015; Weinrib et al., 2010). Cancer cells release high levels of proinflammatory cytokines, such as interleukin-6, which, along with other proinflammatory cytokines, have potent effects on the HPA axis and may activate that axis to the extent that its regulatory mechanisms fail to maintain cortisol levels within a normal range, particularly at night when negative feedback should be most potent (Chrousos, 1995). Second, cortisol dysregulation has been associated with chronic stress, fatigue, and depression in cancer patients (Bower et al., 2005; Jehn et al., 2010). Altered psychological states may impair the negative feedback system that regulates cortisol, leading to a disturbance in the diurnal cortisol profile and resulting in chronically elevated cortisol, particularly at night. For example, depression has been correlated with decreased diurnal variation of cortisol in advanced cancer patients (Hoyt, Bower, Irwin, Weierich, & Stanton, 2016; Jehn et al., 2006), and poor social support was associated with higher mean daily cortisol in patients with breast cancer (R. T. Ho, Fong, Chan, & Chan, 2013; Turner-Cobb, Sephton, Koopman, Blake-Mortimer, & Spiegel, 2000). Finally, in patients with hepatic diseases, impaired metabolism and reduced protein binding of cortisol may lead to elevation in the levels of plasma non-protein-bound 11-hydroxycorticosteroid (McCann & Fulton, 1975), giving rise to the features of hypercortisolism seen in such patients. However, these mechanisms are yet to be confirmed, as we did not include data related to psychological states and specific measurement of HPA-axis function in the present study. Further investigation is needed to examine the direct and indirect mechanisms associated with a disturbed pattern of cortisol secretion in HCC patients.
The hypothesized relationship between a disturbed circadian rhythm and poor sleep in HCC patients is partly supported by our findings. Poor sleepers with HCC had increased cortisol levels at bedtime, consistent with previous literature involving large community-dwelling populations (Kumari et al., 2009; Weinrib et al., 2010). However, the GEE model showed higher cortisol levels to be only marginally correlated with poor sleep. Because the present study is correlational, we cannot make causal interpretations regarding the relationship between poor sleep and disturbances in the diurnal cortisol profile. Of note, alterations in the diurnal cortisol profile and disturbed sleep may have long-term implications for cancer survival and progression. A previous study showed that, in women with breast cancer, aberrant nocturnal cortisol is associated with the length of the disease-free interval, a measure of disease progression (Zeitzer et al., 2016). Substantial evidence also suggests that disturbed sleep is correlated with a higher rate of cancer progression (Lehrer et al., 2013; Palesh et al., 2014). Further studies are required to examine the causes and long-term impacts of the observed disturbances in diurnal cortisol profile and sleep in HCC patients, since such dysregulations may have implications for cancer treatment and prognosis.
There are some limitations to our study. First, some participants may not have collected the saliva in an appropriate way due to physical weakness or disease complications, although we did provide instructions and reminders. Second, many factors may have affected cortisol levels and/or sleep quality, for example, acute stress, seasonal changes, traveling and jetlag, or physical activity (Roveda et al., 2011). We did not control for these factors in our analyses, and they might have contributed to the low statistical association between cortisol levels and poor sleep. Third, we did not collect data on psychological states, cancer treatment, hypnotic drugs, or HCC staging, and these could be useful for interpreting the differential diurnal cortisol profiles among patients with different disease conditions. Fourth, more specific stimulation studies are required to study the feedback disturbances and/or inflammatory pathways to explain the underlying biological mechanisms. Lastly, the current study is limited by a small sample size and the ensuing lack of power to detect the relationship between diurnal cortisol profile and sleep disturbance. The number of HCC patients and healthy controls was not balanced due to budget constraints. Future research should involve larger samples with longitudinal designs. Also, studies should include more psychological variables and biological indicators so as to enable determination of the causal relationship between poor sleep and circadian rhythm disturbances more precisely.
Footnotes
Acknowledgments
We would like to thank all the participants in the study. We are grateful to Drs. Mandy Man Nga Yeung and Pui Hing Chau in the School of Nursing, the University of Hong Kong, for their advice on the biomedical and statistical aspects.
Author Contribution
Tsai-Wei Huang and Chia-Chin Lin contributed to the conception and design. Jun-Hung Lai, Wei-Wen Su, and Shun-Sheng Wu contributed to the acquisition; critically revised manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Denise Shuk Ting Cheung, Xinyi Xu, El-Wui Loh, and Chia-Chin Lin contributed to analysis and interpretation, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Tsai-Wei Huang contributed to acquisition, analysis, and interpretation; drafted the manuscript; critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.