
Abstract
Background:
Autonomic dysfunction, cognitive impairment, and psychological distress are associated with poorer prognosis in patients with acute ischemic stroke (AIS). Heart rate variability (HRV) biofeedback (BF) improves autonomic dysfunction, cognitive impairment, and psychological distress in other patient populations, but its effect in patients with AIS is still unclear.
Objective:
This study investigated the effects of an HRVBF intervention on autonomic function, cognitive impairment, and psychological distress in patients with AIS.
Method:
In this randomized, controlled, single-blind trial, patients with AIS were randomly assigned to the experimental or control group. The experimental group received four HRVBF training sessions. The control group received usual care. Repeated measures of HRV, mini-mental status examination (MMSE), and Hospital Anxiety and Depression Scales (HADS) were collected prior to and at 1 and 3 months postintervention.
Results:
A total of 35 patients completed the study (19 experimental, 16 control). HRV and HADS significantly improved in the experimental group (p < .001) but not in the control group. Likewise, only the experimental group showed significant improvements in HRV, MMSE, and HADS over time (p < .05).
Conclusion:
HRVBF is a promising intervention for improving autonomic function, cognitive impairment, and psychological distress in patients with AIS. More studies of HRVBF interventions are needed to further optimize the effects of HRVBF on autonomic, cognitive, and psychological function in patients with AIS.
Keywords
Stroke is defined as the rapid loss of brain function due to a disturbance in blood supply to the brain. Ischemic stroke, a disturbance caused by cerebrovascular occlusion, accounts for 87% of all strokes (Mozaffarian et al., 2016). As the second leading cause of disability-adjusted life years in developing countries and the third in developed countries, stroke represents an enormous and growing burden to societies globally (Feigin et al., 2015).
Patients with acute ischemic stroke (AIS) may suffer from autonomic dysfunction, cognitive impairment, and psychological distress (Winstein et al., 2016). Autonomic dysfunction, such as reduction in parasympathetic activity, decrease in baroreflex sensitivity, and increase in sympathetic activity (Collins, Dillon, Finucane, Lawlor, & Kenny, 2012), has been associated with higher incidences of neurological and cardiovascular complications (Xiong et al., 2013).
Cognitive impairment in patients with AIS has been associated with greater patient vulnerability and poorer quality of life (Mellon et al., 2015). Patients with AIS may also suffer from focal neurological deficits and experience sudden and unexpected declines in cognitive function due to blood-flow disturbances to a particular region of the brain causing cell damage or cell death (Winstein et al., 2016).
Poststroke patients may also experience psychological distress such as anxiety and depression (Soros & Hachinski, 2012). Psychological distress in poststroke patients negatively impacts patients’ functional recovery and quality of life (Tseng & Chang, 2006). According to the 2016 American Heart Association/American Stroke Association’s guidelines for adult stroke rehabilitation and recovery, early attention to autonomic dysfunction, cognitive impairment, and psychological distress could improve long-term disability, morbidity, and mortality in patients with AIS (Winstein et al., 2016).
Heart rate variability (HRV), oscillations of instantaneous heart rates and between heartbeats (R-R intervals), represents one of the most promising early and quantitative markers of autonomic dysfunction (Malik, 1996). HRV has been used to detect conditions from fetal distress to diabetic neuropathy in advance of other markers of autonomic dysfunction since the 1960s (Hon & Lee, 1963; Pagani et al., 1988). Today, HRV measurements are performed with standardized instruments, allowing for more precise clinical correlations among various HRV indices (time- and frequency-domain indices; Malik, 1996). In poststroke patients, significantly lower HRV indices are an indicator of autonomic dysfunction (Xiong et al., 2013).
HRV biofeedback (BF) is a behavioral intervention that trains subjects to obtain voluntary control of the higher amplitude of HRV. By pacing breathing at a slow frequency so that resonance occurs between cardiac rhythm and respiration, subjects are able to enhance their HRV indices (Lehrer, Vaschillo, & Vaschillo, 2000). HRVBF has been associated with beneficial health outcomes (Lehrer et al., 2000). Research conducted over the past two decades or more has confirmed the efficacy of HRVBF in improving autonomic, cognitive, and psychological well-being in a variety of disease states (Lin, Ko, Fan, & Yen, 2016; Zucker, Samuelson, Muench, Greenberg, & Gevirtz, 2009). However, the effects of HRVBF in patients with AIS have not been explored. Therefore, the aim of the present study was to test the effects of HRVBF on autonomic function, cognitive impairment, and psychological distress in patients with AIS.
Method
The Institutional Review Board of the National Defense Medical Center in Taipei (Number: TSGHIRB 1-103-05-130) approved this randomized, controlled, single-blind trial (Clin icalTrials.gov no. NCT03516227).
Participants
We recruited participants from the neurological ward at a medical center in northern Taiwan. After we presented the study objectives and inclusion criteria at the medical staff meeting, physicians referred potential subjects to the study if they fit study inclusion criteria and gave permission to be contacted by a research team member. Upon receiving physicians’ referrals, the principal investigator explained the purpose and procedures of the study to patients and obtained their informed consent if they chose to participate. All patients were informed that their participation in this study was voluntary and that they could terminate or decline participation at any time.
Since no previous study has examined the effects of HRVBF in patients with AIS, we performed a power analysis based on previous studies examining the impacts of HRVBF on vagal nerve function and psychological distress in patients with posttraumatic stress disorder and in those with depressive symptoms (Lin et al., 2016; Zucker et al., 2009). We found that we needed an estimated sample size of 34 participants for the present study (Cohen’s d effect size of 1.0, 80% power, two-sided significance level of 0.05).
Patients eligible for inclusion were within 1 week of their first-ever ischemic stroke, age 20 years or older, and able to express themselves through oral or written communication. Exclusion criteria were a diagnosis of cardiac arrhythmia (e.g., atrial fibrillation, atrial flutter, ventricular tachycardia, or brady-arrhythmias), mental illness, dementia or Alzheimer’s disease, or total paralysis.
Study Protocol
Participants who provided signed consent were randomly assigned to the HRVBF or control group (Excel BINOMDIST function). Group assignment was concealed in an opaque envelope until participants’ baseline measurements were completed. The HRVBF group received four BF training sessions over 4 days, and the control group received usual care. We followed all participants for 3 months, telephoning them biweekly (totaling five phone calls) during this period. Each telephone follow-up lasted 10−15 min. During these calls, we encouraged participants in the HRVBF group to practice slow breathing for 10 min twice a day and participants in the control group to continue with care as prescribed by their physician. An independent investigator blinded to group assignment reassessed all measurements at 1 and 3 months after the intervention.
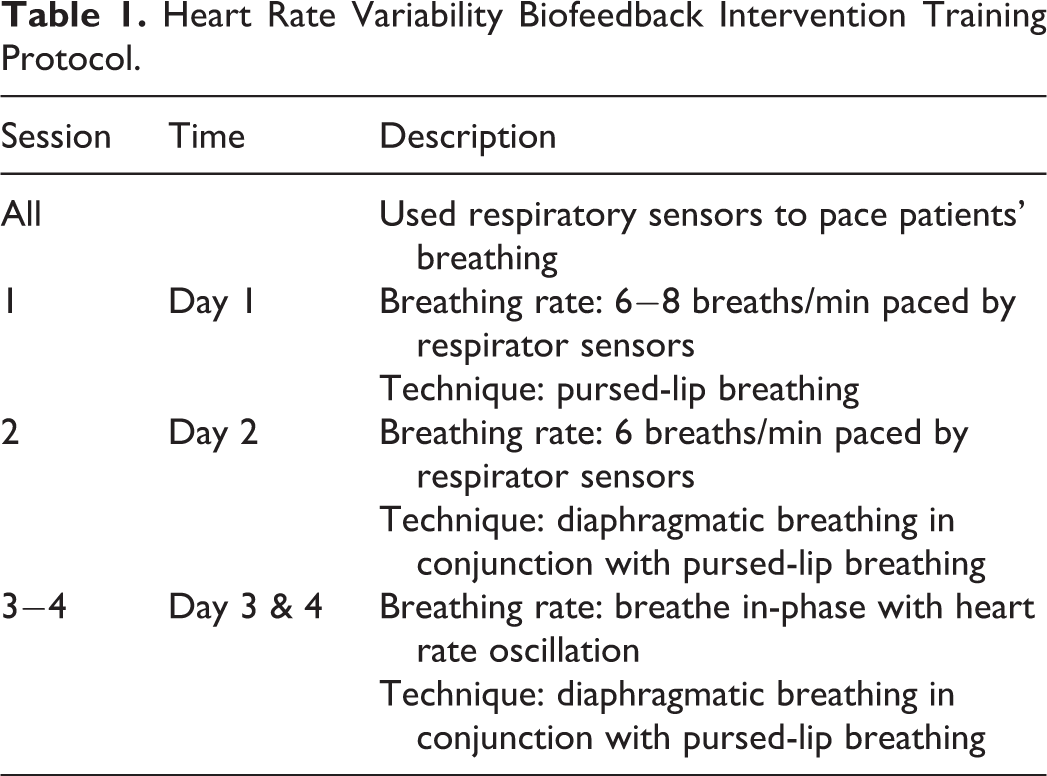
The HRVBF protocol was modified from Lehrer’s HRVBF manual (Table 1; Lehrer et al., 2000). Participants in the HRVBF group received four, one-on-one bedside training sessions (20 min a day) in the hospital. We used a noninvasive visual BF system and a laptop computer for the intervention (NeXus-10 with BioTrace+, Mind Media B.V., the Netherlands). Additionally, we asked participants in the intervention group to practice HRVBF on their own for 10 min twice a day during the 4-day training period using the StressEraser (FDA-regulated as a class II 510[k] exempt medical device, hand-held mobile BF device; Helico Inc., New York, NY). The StressEraser has a built-in feature that records subjects’ daily self-practice sessions (Prinsloo, Derman, Lambert, & Laurie Rauch, 2013). The researcher providing the training reviewed records of patients’ self-practice sessions and addressed any questions they had at every training session. All patients in the HRVBF group were able to complete HRVBF self-practice for 10 min twice a day during the training period.
Heart Rate Variability Biofeedback Intervention Training Protocol.
Measurements
Demographic data
We obtained demographic data from patient files, including age, sex, educational level, body mass index (BMI), risk factors for stroke, disease severity (National Institutes of Health Stroke Scale [NIHSS] score assessed at admission), area of AIS, and cardiac medications right before collecting baseline measurements.
Autonomic function
We measured autonomic function by HRV using a three-way electrocardiogram recorder interfaced with a computer program (NeXus-10, Mind Media B.V., the Netherlands) at baseline, 1 month, and 3 months. All HRV measures were collected in the hospital. Participants’ cardiac interbeat intervals (IBIs) were recorded at a rate of 256 samples per second between 9 and 11 in the morning. For further HRV analyses using Kubios HRV software (ver. 3.2, Biosignal Analysis and Medical Imaging Group, Finland), we needed 5 min of IBI time series. However, we initially collected 6 min of IBI time series to ensure sufficient IBI data for Kubio analyses (NeXus-10, Mind Media B.V.-). This extra time allowed us to shift the start time for the recordings manually using the built-in function in the NeXus-10 computer program to avoid signal artifacts (ectopic beats and motion artifacts) that sometimes occurred at the start of recordings and obtain the steadiest 5 min of IBI recording for analyses. We further enhanced data quality using two methods provided within the Kubios HRV software. First, we applied the threshold-based correction for interpolation of artifacts and ectopic beats (Tarvainen, Lipponen, Niskanen, & Ranta-Aho, 2019). Second, we applied the smoothness priors for removal of disturbingly low-frequency (LF) trend components (Tarvainen, Niskanen, Lipponen, Ranta-Aho, & Karjalainen, 2014). The HRV time-domain indices that we calculated included the standard deviation of normal-to-normal R-R intervals (SDNN) and the root mean square of successive heartbeat interval differences (rMSSD). For the HRV frequency-domain indices, we used the fast Fourier transformation; these indices included power spectral components reported at very LF (< 0.04 Hz), LF (0.04−0.15 Hz), and high frequency (HF; 0.15−0.4 Hz) and their summed total power (TP). The computer program and HRV software we used in the present study were the same as those used in a number of previous studies (Y. J. Chen et al., 2017; Cornforth, Tarvainen, & Jelinek, 2014).
Cognitive function
We measured cognitive impairment using the mini-mental state examination (MMSE)[Please note that both the expansions “mini-mental status examination” and “mini-mental state examination” are used as the abbreviation for “MMSE.” Please indicate the changes required]. The MMSE includes 11 items for the assessment of five facets of orientation (space and time, registration, attention and calculation, recall, and language). The maximum possible score is 30 (Folstein, Folstein, & McHugh, 1975). A score of 24 or lower is suggestive of dementia in elderly patients (sensitivity = .85, specificity = .90; Creavin et al., 2016).
Psychological distress
We measured psychological distress using the Hospital Anxiety and Depression Scale (HADS; Zigmond & Snaith, 1983). The HADS is a 14-item self-rated ordinal scale (0 indicates no distress and 3 indicates serious distress). A score of 8 or higher is suggestive of anxiety or depression with good specificity and sensitivity in somatic, psychiatric, and primary-care patients and in the general population (Bjelland, Dahl, Haug, & Neckelmann, 2002). The Chinese version of the HADS has demonstrated greater accuracy than the Visual Analogue Mood Scale and the Geriatric Depression Scale in screening for poststroke depression in Chinese patients with their first-ever stroke (Tang et al., 2004). The internal consistencies of the HADS for anxiety and depression in the present study were 0.73 and 0.80, respectively.
Statistical Methods
We have reported demographics, HRV, MMSE, and HADS using descriptive statistics. Due to data skewness, we converted all HRV indices into natural logarithms (ln SDNN, ln rMSSD, ln HF, ln LF, and ln TP) for further analysis. To test for differences between and within groups in all outcome variables, we used independent samples t tests, χ2 tests, and paired samples t tests. As participant drop-outs were due to the lack of baseline or outcome evaluation, the intention-to-treat analysis was identical to the per-protocol analysis (Gupta, 2011). Thus, we used the per-protocol analysis for outcome evaluation.
After adjusting for age, educational level, and NIHSS as covariates, we used linear mixed model tests to analyze the intervention effect on outcome variables. Group (intervention), time, and Group × Time interactions were tested. Under the model of a compound symmetry variance–covariance structure, we treated participants as random effects and all other effects as fixed. We used the baseline condition of the control group as the reference group, so that the regression coefficients for the variables represented the differences between the HRVBF and the control groups. We used a statistical software package (SPSS 19.0, SPSS, Inc., Chicago, IL) for statistical analyses and a p value < .05 to indicate statistical significance.
Results
We screened 57 patients with AIS for participation. Of these, we excluded three due to arrhythmias, and 14 declined to participate. Of the remaining 40 patients we enrolled and randomly assigned to the intervention or control group, 5 did not receive the allocated group treatment protocol (2 had arrhythmias after inclusion and 3 refused baseline measurements; Figure 1). The remaining 35 patients completed the study (19 intervention, 16 control). The characteristics (age, gender, education, risk factors of stroke, and stroke severity) of the five participants who dropped out of the study were not significantly different from those that stayed in the study (p > .05).
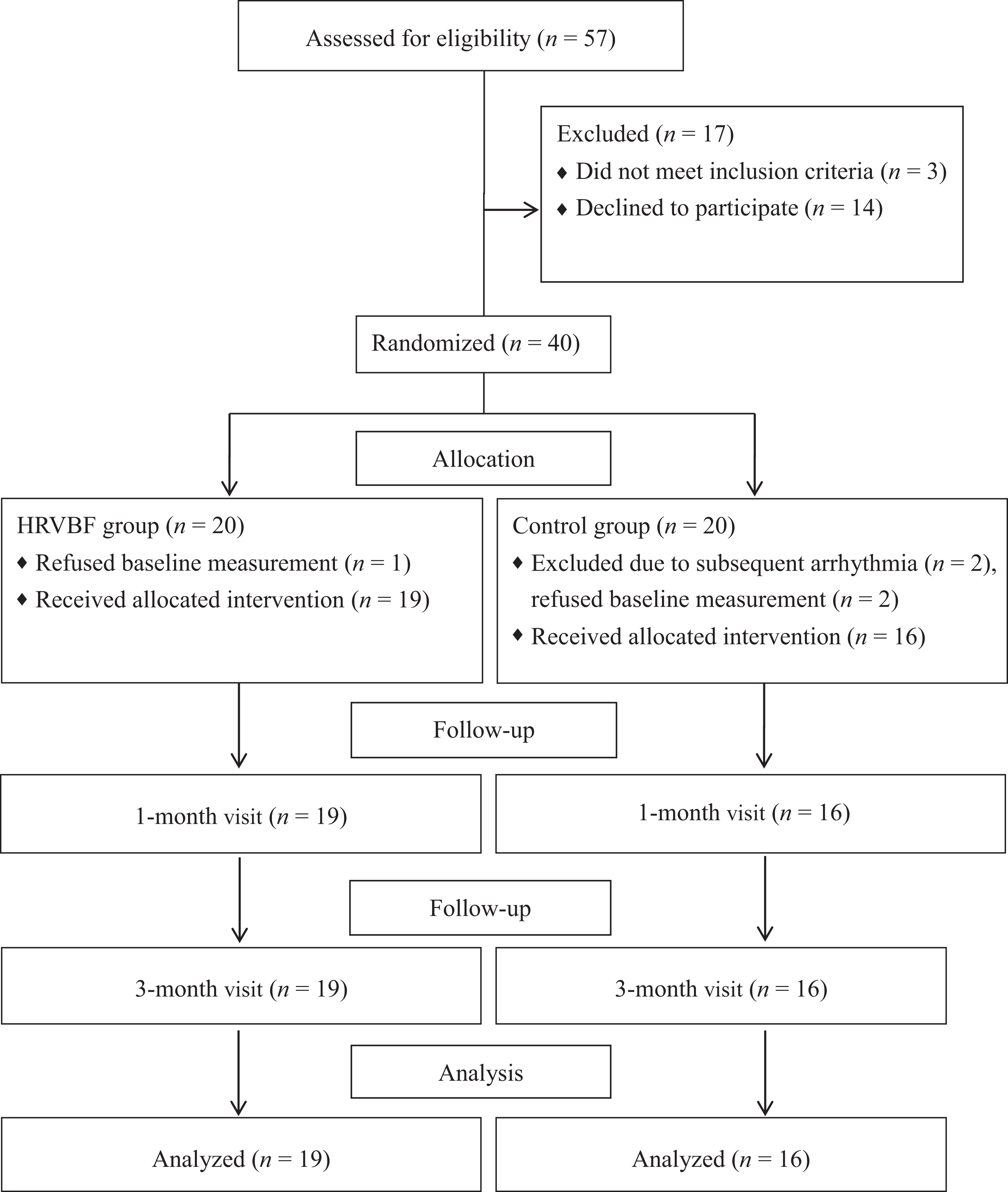
Flow diagram of the study. HRVBF = heart rate variability biofeedback intervention.
Demographics of the Participants
Participants’ mean age was 67.4 ± 9.7 years. Just over half of the participants (51.4%, n = 18) were men, and 22 (62.9%) had a left-side stroke. The median (interquartile range) NIHSS stroke severity score was 7 (5–10). Risk factors for stroke included hypertension (60%, n = 21), diabetes (48.6%, n = 17), and heart disease (34.3%, n = 12). Demographic characteristics (i.e., age, sex, educational level, BMI, risk factors of stroke, median NIHSS score, area of AIS, and cardiac medications) are listed in Table 2 and did not differ significantly between groups (p > .05; Table 2).
Participant Characteristics.
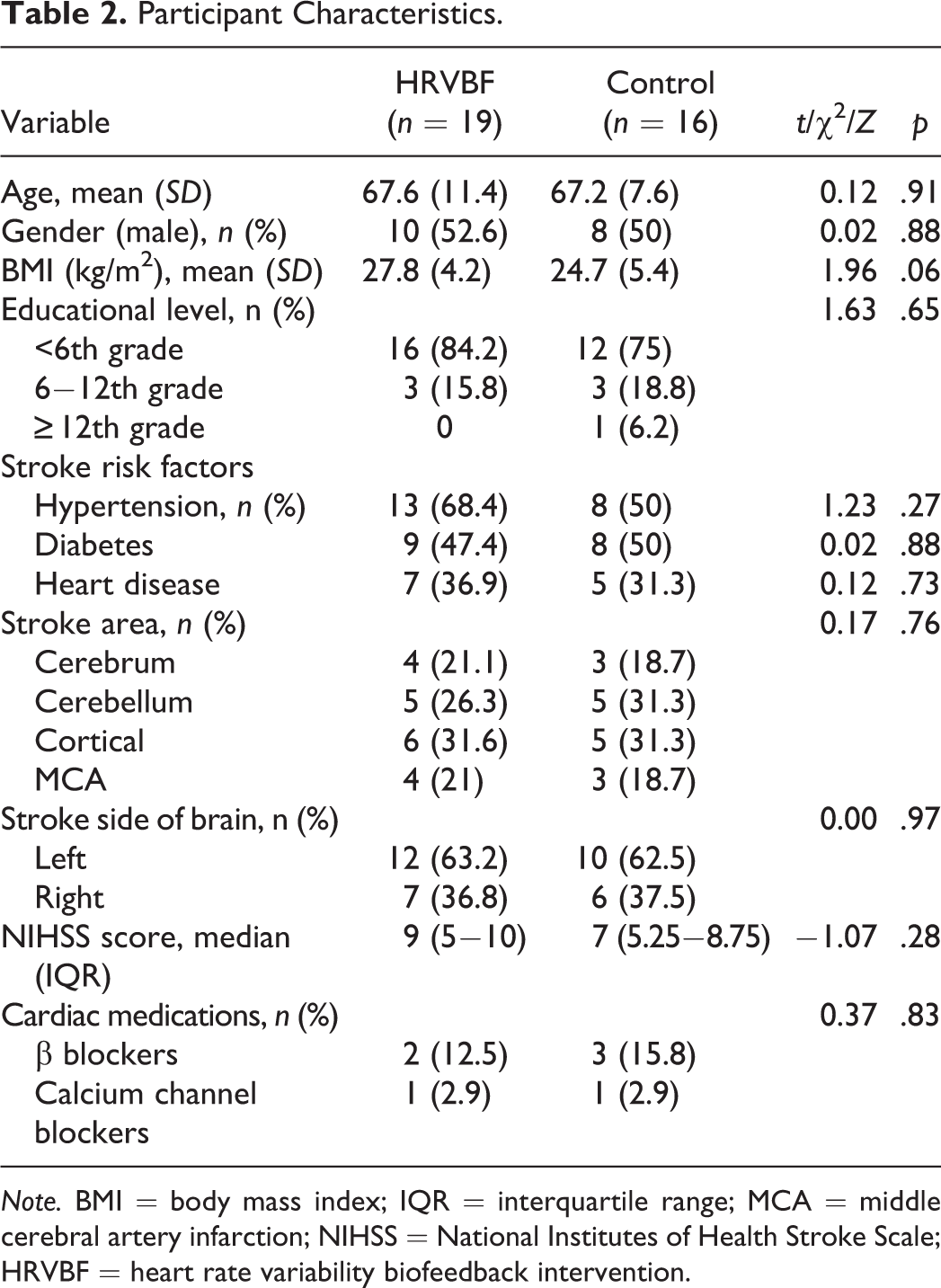
Note. BMI = body mass index; IQR = interquartile range; MCA = middle cerebral artery infarction; NIHSS = National Institutes of Health Stroke Scale; HRVBF = heart rate variability biofeedback intervention.
Comparison of Autonomic Function, Cognitive Impairment, and Psychological Distress Within and Between Groups
Heart rate, autonomic function, cognitive impairment, and psychological distress were not significantly different between groups at baseline (Table 3). Over the course of the study, the average heart rate decreased significantly in the HRVBF group but not in the control group. However, the difference in heart rate between the groups was not significant at either the 1- or 3-month follow-up. For the HRVBF group, all time- and frequency-domain HRV indices increased significantly at the 1- and 3-month follow-ups (p < .01). For the control group, only SDNN measured at the 1-month follow-up increased significantly (p = .02; Table 3). MMSE score improved significantly at the 1- and 3-month follow-ups for both the HRVBF (p < .001 and p < .001, respectively) and control groups (p = .04 and p < .001, respectively). The HADS score significantly decreased in the HRVBF group at 1 and 3 months (anxiety p = .01 and p < .001, respectively, depression p = .04 and p < .001, respectively) but not in the control group (anxiety p = .49 and p = .15, respectively, depression p = .15 and p = .46, respectively; Table 3).
Heart Rate Variability, Cognitive Function, and Psychological Status in the Two Study Groups Across Three Measurement Time Points.
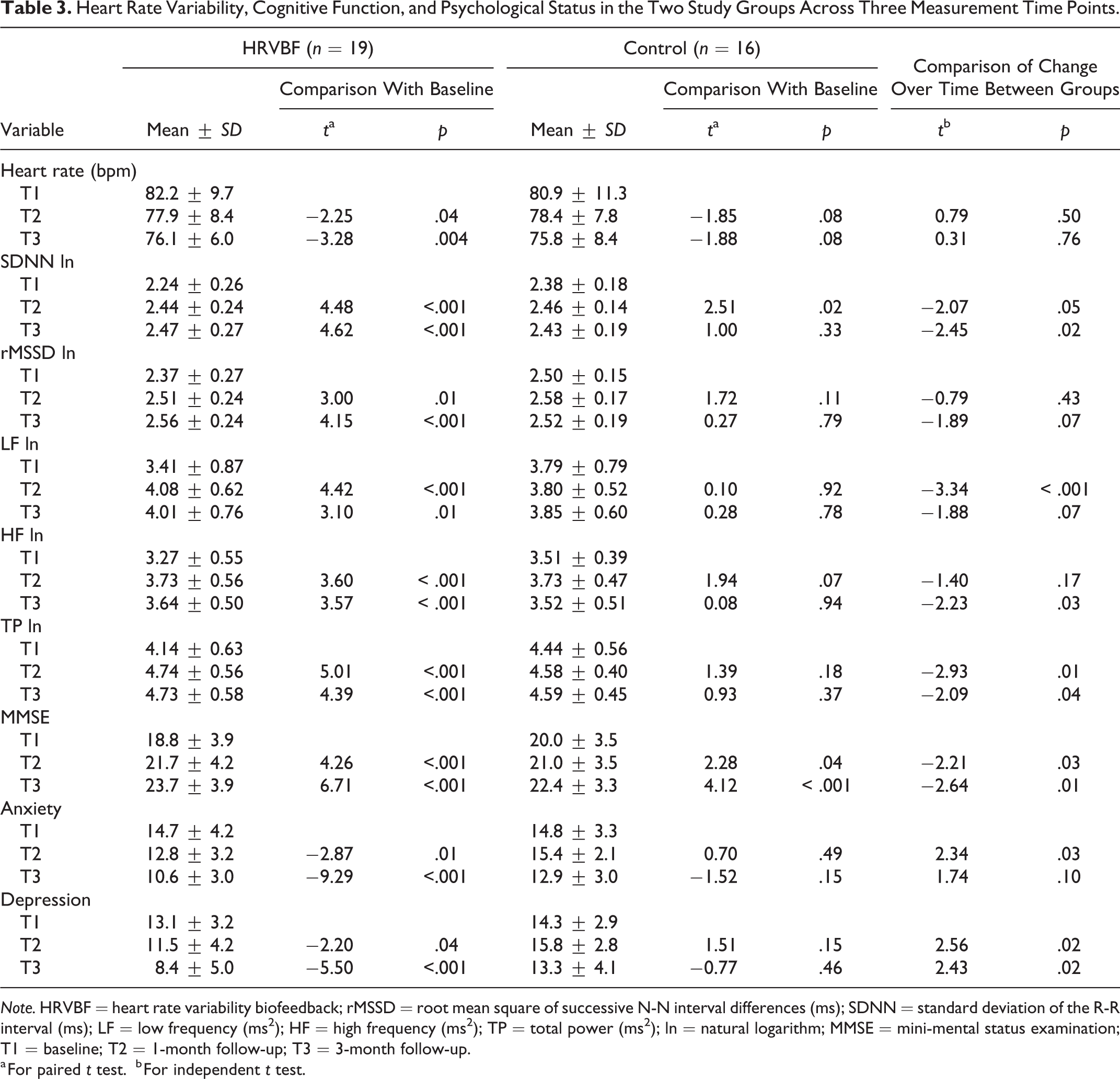
Note. HRVBF = heart rate variability biofeedback; rMSSD = root mean square of successive N-N interval differences (ms); SDNN = standard deviation of the R-R interval (ms); LF = low frequency (ms2); HF = high frequency (ms2); TP = total power (ms2); ln = natural logarithm; MMSE = mini-mental status examination; T1 = baseline; T2 = 1-month follow-up; T3 = 3-month follow-up.
a For paired t test.
b For independent t test.
Linear Mixed Model Test Results
After controlling for age and NIHSS, we found that the group-by-time effects on the HRV indices, except for HF (p = .12), were all significant (p < .05; Table 4). SDNN (p = .07) and rMSSD (p = .43) were not significantly different between groups at 1 month. However, at 3 months, the HRVBF group showed significantly greater increases than did the control group in SDNN (p = .005) and rMSSD (p = .01). For LF and TP, the HRVBF group had significantly greater increases than the control group at both 1 month (LF p = .007, TP p = .01) and 3 months (LF p = .03, TP p = .02).
Results of Linear Mixed Model Analyses on Heart Rate Variability Indices of Autonomic Nervous System Function.
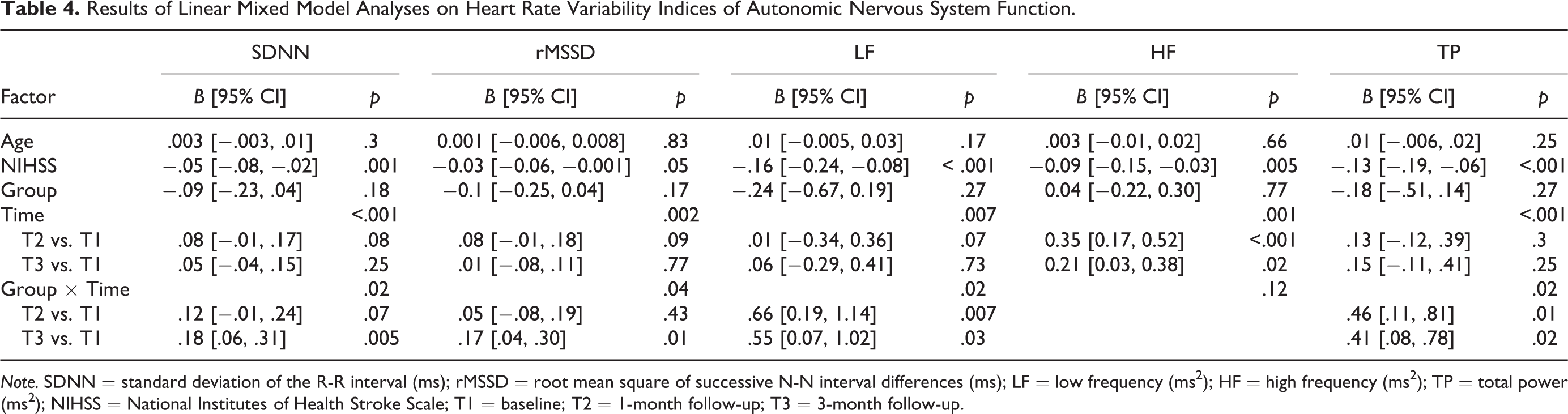
Note. SDNN = standard deviation of the R-R interval (ms); rMSSD = root mean square of successive N-N interval differences (ms); LF = low frequency (ms2); HF = high frequency (ms2); TP = total power (ms2); NIHSS = National Institutes of Health Stroke Scale; T1 = baseline; T2 = 1-month follow-up; T3 = 3-month follow-up.
After controlling for age, NIHSS, and educational level, we found that the group-by-time effects on MMSE remained unchanged and statistically significant (p = .008). The HRVBF group had significantly greater increases in cognitive function than the control group at 1 month (p = .03) and 3 months (p = .003; Table 5).
Results of Linear Mixed Model Analyses on Cognitive Function and Psychological Status.
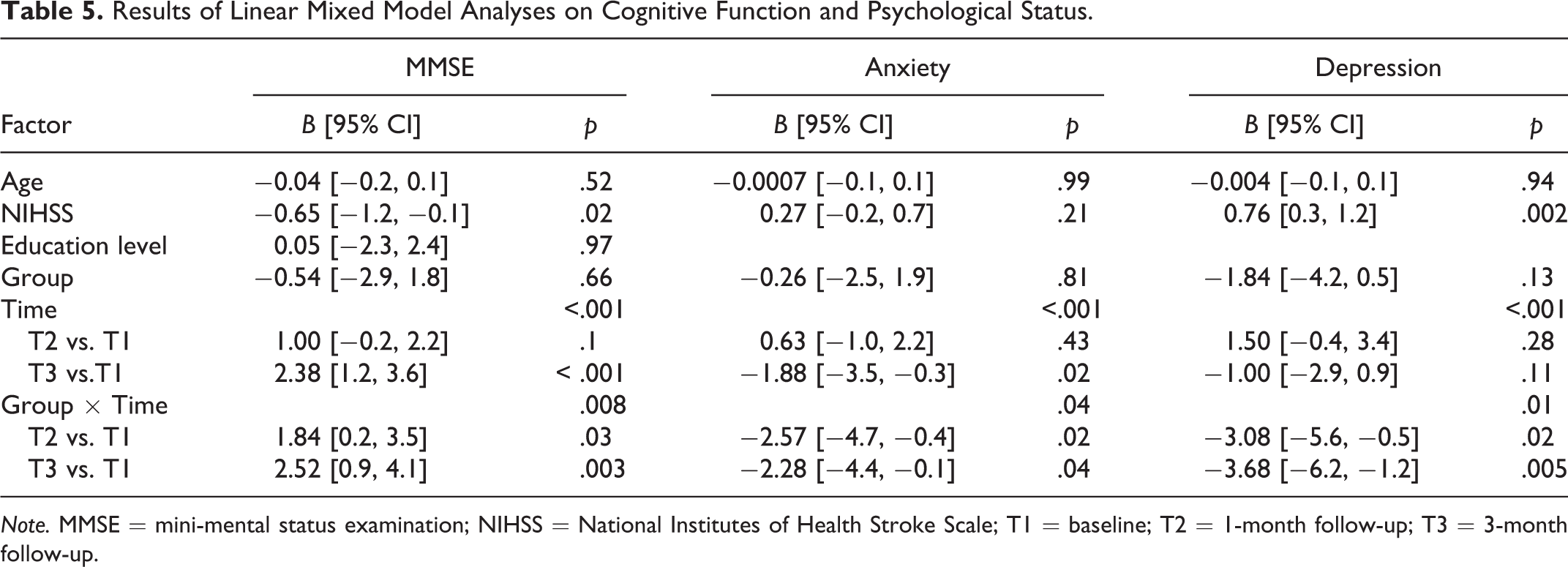
Note. MMSE = mini-mental status examination; NIHSS = National Institutes of Health Stroke Scale; T1 = baseline; T2 = 1-month follow-up; T3 = 3-month follow-up.
The group-by-time effects on HADS were also significant (anxiety p = .04, depression p = .01; Table 5). The HRVBF group had significantly greater decreases than the control group in anxiety and depression at 1 month (anxiety p = .02, depression p = .02) and at 3 months (anxiety p = .04, depression p = .005; Table 5).
Discussion
The present study demonstrates that HRVBF training is feasible in patients with AIS. The finding that daily one-on-one bedside HRVBF training sessions over 4 consecutive days (20 min/day) were effective in improving participants’ autonomic function, cognitive impairment, and psychological distress is both surprising and exciting. Contemporary theoretical postulations and research findings suggest that HRVBF guides participants to breathe in a manner (6 breaths/min) that promotes the rise and fall of the heart rate along the same pattern as the tidal breath, enhancing parasympathetic function via stimulation of the vagus nerve and baroreflex gain (Lehrer, 2018). Accordingly, HRVBF can eliminate phase differences between heart rate fluctuation and respiration to strengthen the modulatory processes of the respiratory, cardiovascular, and emotional systems (Lehrer & Gevirtz, 2014).
Consistent with a previous study conducted in Taiwan (C. F. Chen, Lai, Lin, Liou, & Lin, 2011), in the present study we found autonomic dysfunction, represented by low time (SDNN and rMSSD) and frequency (LF, HF, and TP) domains of HRV, in a sample of patients with AIS. HRV is still an evolving field in terms of its theoretical underpinnings, its methodology, and its clinical utilization. Although the physiological interpretations of HRV indices are still being debated, reviews generally agree that SDNN and TP are representations of autonomic function in general (Malik, 1996) and that LF may represent cardiac vagal tone and baroreceptor activity (Porges, 2007). HF is thought to be an index of parasympathetic function because in clinical and experimental studies, results have shown it to be a major contributor to efferent vagal activity (Malik, 1996). In addition, research has demonstrated that HF is closely correlated with rMSSD, another measure of parasympathetic function (Frenneaux, 2004).
Specifically, our present findings suggest that HRVBF can significantly improve autonomic function, as indicated by improvements in the HRV indices of LF, TP, and SDNN after HRVBF training (Kromenacker, Sanova, Marcus, Allen, & Lane, 2018; Zaccaro et al., 2018). In previous studies, HRVBF with slow-paced breathing enhanced vagal activity and produced positive changes in HRV indices (Kromenacker et al., 2018). HRVBF has also improved the HRV indices of SDNN and LF in patients with poststroke depression (Li et al., 2015). LF and TP have demonstrated predictive validity with prognostic value in patients with cardiovascular disease (Melillo et al., 2015), and some authors posit that they may be the two most important indices of autonomic function.
In another study, Nolan et al. (2005) found that HRVBF enhanced vagal HR regulation, as represented by HF HRV, in patients with coronary heart disease. The authors postulated that HF’s effect might be related to the interface between cognitive and emotional functioning and neurocardiac regulation through the training process. In the present study, we did not observe significant improvement in HF HRV after HRVBF, whereas rMSSD, another measure of parasympathetic function, significantly increased at 3 months postintervention in the HRVBF group. A possible explanation for these divergent results is that HF is most reliable within respiratory rates of 12–15 breaths per min (Ernst, 2017; Frenneaux, 2004), and most of our participants had rates higher than 15 breaths per min.
Parasympathetic dysfunction is common and more deterious than sympathetic dysfunction, and research has shown it to be correlated with poor prognosis after ischemic stroke (Xiong et al., 2013). It is not clear whether the intervention we tested in the current study took place too soon after the ischemic stroke or was too brief or whether our follow-up period was too short to fully demonstrate the positive effects of HRVBF training on all parasympathetic indices in our sample of patients with AIS. In addition, we did not measure respiratory sinus arrhythmia, a description of heart rate fluctuation during the respiratory cycle and another indicator of a type of parasympathetic function (Grossman & Taylor, 2007). Inclusion of this indicator in future studies could provide a more comprehensive evaluation of parasympathetic enhancement by HRVBF.
Cognitive impairment scores in our participants improved over time, as one would expect during the first year after a stroke (Appelros & Andersson, 2006). However, it is notable that participants in the HRVBF training group demonstrated significantly greater cognitive improvements than their counterparts in the usual-care group in just 1 month. The beneficial effects continued over time, and the gap between the two groups appeared to widen further by 3 months. Prior studies have demonstrated beneficial effects of HRVBF on cognitive impairment in healthy males with work-related stress (Sutarto, Wahab, & Zin, 2013) and in patients with chronic brain injury (Kim et al., 2013). Possible mechanisms of the observed positive effect of HRVBF on cognitive function may be related to integral connections between the heart and the brain. Findings from prior studies have suggested that strengthening cardiac autonomic function using HRVBF restores cerebral blood flow. Augmentation of blood flow to the prefrontal cortex might enhance prefrontal activity and improve cognitive function (Conder & Conder, 2014; Kim et al., 2013; Smith, Thayer, Khalsa, & Lane, 2017). Our results in the present study showed that patients with AIS may experience similar improvements in cognitive impairment from HRVBF.
During the BF process, participants must modulate their own breathing by synchronizing their breathing with their heart rate curve. These purposeful efforts require cognitive engagement, which may also benefit cognitive functioning. Additionally, participants may gain a greater sense of self-efficacy through seeing themselves master their physiological changes (HRV) by regulating their breathing (McCraty & Shaffer, 2015). Therefore, another possible benefit of HRVBF that needs further study is whether HRVBF enhances self-regulation and self-efficacy.
Research has shown significant associations between anxiety and depression in the acute stage (the first 2 weeks) of stroke and cognitive dysfunction, physiological disability, and psychological disorders at later follow-ups (Huang et al., 2017; Jeong et al., 2012; Wright, Wu, Chun, & Mead, 2017). HRVBF interventions have reduced psychological distress and depression in patients undergoing chemotherapy or invasive procedures and in those with coronary heart disease and posttraumatic stress disorder (Goessl, Curtiss, & Hofmann, 2017; Hayama & Inoue, 2012; Mikosch et al., 2010; Nolan et al., 2005: Zucker et al., 2009). In addition, Li et al. (2015) found that HRVBF significantly improved depressive symptoms in poststroke patients. In the present study, we showed that using an HRVBF intervention as an adjunctive treatment could also augment usual care in patients with AIS and significantly decrease their psychological distress, in particular, their depression. A potential mechanism through which HRVBF may have improved psychological distress and depression is that BF training can evoke focused concentration in an individual. By engaging participants in a goal-directed activity, HRVBF promotes emotional self-control. Greater ability to modulate one’s cognitive–emotional response increases one’s perceived self-efficacy and decreases negative emotionality (McCraty & Shaffer, 2015; Thayer & Lane, 2000).
Some methodological issues could affect the interpretation of the present study. One consideration is the small sample size; another is the short-term follow-up period of 3 months. Both of these factors could have limited the study’s power to detect the effects of HRVBF on participants’ parasympathetic ANS responses. During the follow-up period, we telephoned the HRVBF group biweekly to encourage continued self-directed practice. However, we did not ask participants to log their practice sessions at home. To better discern how each participant applied the HRVBF training at home, we recommend that future studies consider adding a practice log to fine tune the long-term dose effect of HRVBF on outcome measures. Also, since we chose to sample participants representative of patients with AIS in general, with variances in their areas of cerebral infarction and degrees of ANS dysfunction, we cannot draw any conclusions about the effect of HRVBF on any specific categories of patients with AIS (Kuriyama, Mizuno, Niwa, Watanabe, & Nakagawa, 2010). Future studies with larger sample sizes, stratified for different areas of cerebral infraction and varying degrees of ANS dysfunction, could further elucidate the effects of HRVBF on specific categories of patients with AIS.
Another limitation of the present study is the use of the MMSE to assess cognitive impairment. In a previous study, authors suggested that baseline MMSE scores in patients with AIS may not be stable enough to predict cognitive performance over time (Bour, Rasquin, Boreas, Limburg, & Verhey, 2010). Although no participant in our study had difficulty following training instructions, it is not clear how, or if, their baseline MMSE scores (mean of 19.4 ± 3.7, moderate cognitive impairment) influenced study results. A recent systematic review indicated that the Montreal Cognitive Assessment might be more useful than the MMSE for examining cognitive impairment in the stroke population (Burton & Tyson, 2015).
Although there have been no studies related to nonlinear HRV indices in stroke patients, and the physiological or pathophysiological variations in nonlinear HRV indices and their clinical significance in stroke remain unclear (de Godoy, 2016; Huikuri, Makikallio, & Perkiomaki, 2003), it is nevertheless an interesting area for future studies to explore. Certain nonlinear representations of HRV data might provide clinically significant information. Authors have suggested that nonlinear HRV indices (such as short- and long-term fluctuations of detrended fluctuation analyses [DFA α1 and DFA α2, respectively] and short- and long-term standard deviations of the Poincaré plot [SD1 and SD2, respectively]) are useful for quantifying the unpredictability and complexity of a series of IBIs (Shaffer & Ginsberg, 2017). In the present study, the SD2, or length of the Poincaré plot graphed by plotting every R-R interval, which is related to LF HRV (Brennan, Palaniswami, & Kamen, 2001), was the only nonlinear HRV index that significantly increased over time in the HRVBF group. However, the relevance of this increase is unclear, as the methodology and clinical utility of nonlinear HRV indices are still evolving. Nevertheless, exploring various nonlinear representations of HRV data and their significance remains an interesting area for future studies.
Hyperglycemia is common (40−60%) in patients with AIS (Marulaiah, Reddy, Basavegowda, Ramaswamy, & Adarsh, 2017). Recent studies have shown that diabetes has an effect on HRV (Benichou et al., 2018). In addition, HRVBF appears to be beneficial for improving HbA1C and ameliorating anxiety and depression in patients with Type 2 diabetes (McGinnis, McGrady, Cox, & Grower-Dowling, 2005). Although it was outside the scope of the current study, future studies on whether stroke patients with diabetes might respond differently to HRVBF than those without diabetes may be an interesting area of study.
Conclusions
In this preliminary study, we demonstrated that HRVBF training is feasible in patients with AIS. We also found that four daily 20-min sessions over consecutive days significantly reduced participants’ anxiety and depression, improved cognitive impairment, and facilitated ANS recovery measured at 1 and 3 months after HRVBF training. These results show that HRVBF is a promising adjunctive intervention to usual care in patient with AIS. Future studies are needed to cross-validate findings from the current study. Larger sample sizes with longer follow-ups could fine tune our understanding of dose–response relationships of HRVBF and further delineate how early optimization of ANS, cognitive, and psychological function impact long-term recovery in patients with AIS.
Footnotes
Acknowledgments
We sincerely appreciate the generous assistance of physicians and nurses in the neurological ward of Tri-Service General Hospital in completing this study. In addition, we are grateful to all of the study participants.
Author Contributions
Yu-Ju Chen contributed to conception and design, acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy. Wan-Ling Chang contributed to conception, acquisition, and interpretation; drafted manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy. Jiunn-Tay Lee contributed to interpretation, critically revised manuscript, gave final approval, agrees to be accountable for all aspects of work ensuring integrity and accuracy. Chi-Rong Li contributed to acquisition and analysis, critically revised manuscript, gave final approval, agrees to be accountable for all aspects of work ensuring integrity and accuracy. Amy H. T. Davis contributed to conception, interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy. Chia-Chen Yang contributed to analysis, drafted manuscript, gave final approval, agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.