
Abstract
Background:
Psychological state, stress level, and gastrointestinal function are intricately related and relevant to symptom exacerbation in patients with irritable bowel syndrome (IBS), but genetic contributors to this brain–gut connection are not fully understood. The purpose of this exploratory study was to compare gene expression in participants with IBS to that of healthy controls (HC) and to examine patterns of expression in participants with IBS by sex and IBS subtype.
Method:
Participants were recruited to an ongoing protocol at the National Institutes of Health. Differences in demographic and clinical characteristics were assessed using descriptive statistics and Mann–Whitney U tests. Expression levels of 84 genes were evaluated in peripheral whole blood using Custom RT2 Profiler polymerase chain reaction (PCR) Arrays, and data analysis was performed through GeneGlobe Data Analysis Center.
Results:
Participants with IBS (n = 27) reported greater levels of perceived stress (p = .037) and differed in expression values of ±2 for the genes ADIPOR1, ADIPOR2, CNR2, COMT, OXTR, and PPARA compared to HC (n = 43). Further analyses by sex and IBS subtype revealed differential patterns of gene expression related to the endocannabinoid system, cytokines, stress, and sex steroid hormones.
Conclusions:
Diverse yet interconnected processes such as metabolism, inflammation, immunity, social behavior, and pain are associated with differences in gene expression between participants with IBS and HC. These findings lend support for genomic associations with the brain–gut connection in patients with IBS and highlight the relevance of sex and IBS subtype in performing such analyses.
The discovery and validation of genomic findings in irritable bowel syndrome (IBS) is a complex research endeavor, due in part to the multifactorial pathogenesis and heterogeneous patient population of IBS. Genetic associations in IBS span the continuum from the brain to the gut, including mechanisms related to altered central processing, immune function, intestinal barrier function, and visceral sensitivity (Enck et al., 2016). Epigenetic mechanisms may also contribute to IBS symptomatology, as evidenced by reported changes in histone acetylation in preclinical models (Cao, Bai, Ji, Karpowicz, & Traub, 2016) as well as changes in DNA methylation (Mahurkar et al., 2016) and alterations of microRNA in patients with IBS (Fourie et al., 2014; Gazouli et al., 2016). Psychological state, stress level, and gastrointestinal function are intricately related and relevant to symptom exacerbation in IBS, but genetic contributors to this brain–gut connection are not fully understood. The purpose of the present exploratory study was to compare gene expression in participants with IBS to that of healthy controls (HC), with a focus on genes that may dually affect psychological and gastrointestinal processes, within the conceptual framework of the brain–gut axis (BGA). The BGA accounts for interplay among the central nervous system (CNS), autonomic nervous system (ANS), hypothalamic-pituitary-adrenal (HPA) axis, and enteric nervous system (ENS; Ohman & Simren, 2007). Secondary aims were to examine patterns of gene expression by participant sex and IBS subtype.
Psychological distress can influence the efferent output of the HPA axis and the ANS, both of which can affect gastrointestinal immune, barrier, and motor function (Van Oudenhove et al., 2016). Early life adversity may also have a lasting effect upon the physiological stress response, with stress-induced mRNA expression of genes associated with hormone activity, G protein–coupled receptor binding, and steroid binding found to vary in adults with a history of childhood adversity versus HC (Schwaiger et al., 2016). Importantly, patients with IBS are more likely to report early adverse childhood experiences (Park et al., 2016), and patients with diarrhea-predominant IBS to exhibit higher mRNA expression levels of G protein–coupled estrogen receptor, than HC (Qin et al., 2014). Research has also shown that patients with IBS exhibit lower mRNA expression levels of glucocorticoid receptor α (a finding driven primarily by male differences) and display sex-specific differences compared to HC in their HPA-axis response to hormone challenge (Videlock et al., 2016). Furthermore, investigators have noted differences in psychological and physiological markers of stress among IBS patients by sex and subtype, respectively (Weaver, Melkus, Fletcher, & Henderson, 2018).
Such findings suggest the need for a closer look at possible relationships between genes associated with sex hormones and patterns of IBS symptomatology. The relevance of sex hormones to IBS is substantiated by the higher IBS prevalence rates in females compared to males (Sperber et al., 2017) and the ability of sex hormones to influence stress susceptibility and gut motility, permeability, and pain (Meleine & Matricon, 2014). Gonadal hormones also exhibit bidirectional interactions with the endocannabinoid system (Gorzalka & Dang, 2012), a signaling system pertinent to IBS given its central and peripheral involvement in gut function, stress, and pain (Sharkey & Wiley, 2016). Estrogen also influences the production and metabolism of leptin, a hormone involved in energy homeostasis, appetite regulation, and neuroendocrine functioning (Xing et al., 2015).
Given the disproportionate rates of psychopathology in patients with IBS, evaluating genetic associations of neuromodulators might prove worthwhile; for instance, dysfunction of enteric glutamatergic pathways may be involved with visceral pain and motility disturbances (Filpa et al., 2016). Likewise, gamma-aminobutyric acid plays an inhibitory role in the CNS (Crowley, Cryan, Downer, & O’Leary, 2016) and, as Seifi et al. (2014) noted, has diverse receptor subtypes expressed within the ENS in a mouse model. Evaluating expression levels of genes associated with dual actions in the CNS and ENS may facilitate understanding of IBS. By consolidating genes of interest in a custom polymerase chain reaction (PCR) array in the present study, we aimed to examine expression of genes related to psychological and gastrointestinal processes and gain insight on the brain–gut connection, or BGA, in patients with IBS.
Method
Participants were recruited to an ongoing protocol at the National Institutes of Health (NIH) in Bethesda, MD (ClinicalTrials.gov: NCT00824941), with recruitment strategies including, but not limited to, flyers, health-care provider referrals, and mass media advertisements. The parent investigation recruited male and female participants who were 13–45 years of age, were with or without chronic abdominal pain, and were normal (body mass index [BMI] < 25 kg/m2) or overweight (BMI ≥ 25 kg/m2). Female participants were required to have regular monthly menstrual cycles and to have had onset of menses at least 2 years prior to study participation. Inclusion criteria further required participants with abdominal pain to have a history of such for greater than 6 months prior to enrollment, without evidence of organic gastrointestinal (GI) disease, prior GI surgery, or the taking of daily medications for GI symptoms. Individuals with a history of endocrine, renal, cardiac, pulmonary, neurologic or gynecological pathology, comorbid pain, or psychiatric conditions were excluded. Medications that acted on the cortisol, catecholaminergic, or serotonergic systems were also exclusionary. Those who consumed more than two alcoholic beverages a day or more than 300 mg of caffeine in the afternoon or evening or those who engaged in shift work (during the late evening or night) were also excluded from participation.
After initial screening and eligibility determination, participants were instructed to present to the Clinical Research Center between 8 a.m. and 11 a.m. after a 12-hr fast. After participants provided written informed consent, peripheral whole blood was drawn via venipuncture into PAXgene RNA tubes (Qiagen, Germantown, MD, USA) and frozen to −80 °C until processing. Participants underwent a history and physical examination by either physician or nurse practitioner, with IBS diagnosis and subtype determined per Rome III criteria. As part of the parent investigation, participants completed a battery of self-report inventories. In the present study, we evaluated participant responses to the Perceived Stress Scale, a measure that evaluates levels of perceived stress within the past month (Cohen, Kamarck, & Mermelstein, 1983).
We analyzed gene expression with a Custom RT2 Profiler PCR Array, with each array including four replicates of the following: 84 custom-selected genes, five housekeeping genes, three positive PCR controls, three reverse-transcription controls, and a genomic DNA control. To evaluate expression levels of mRNA, briefly, PAXgene tubes were thawed and RNA extracted using a PAXgene blood miRNA kit. RNA concentration was determined via NanoDrop spectrophotometer, and RNA integrity measured via Experion StdSens Analysis Kit. RT2 First Strand Kit was used to prepare cDNA from 400 ng of purified RNA. RT2 SYBR Green Mastermix was added to the cDNA, samples were aliquoted into 384-well plates via epMotion M5073 (Eppendorf), and PCR was performed on a QuantStudio 6 Flex Real-Time PCR System (Thermo Fisher Scientific). Run settings of 1 cycle × 10 min at 95 °C, 40 cycles × 15 s at 95 °C, and 40 cycles × 1 min at 60 °C were used. A dissociation (melting) curve analysis was performed, and threshold value/cycle numbers manually defined at 0.15 and 3–15 across plates. Threshold cycle (CT ) values were transformed from 384- to 96-well format via Qiagen Patch template and uploaded into the GeneGlobe Data Analysis Center (www.qiagen.com).
To assess for differences between participants with IBS and HC in demographic and clinical characteristics, we calculated descriptive statistics and performed Mann–Whitney U tests using SPSS (IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0, IBM Corp., Armonk, NY), with level of significance set a priori as p < .05. To perform PCR data analysis, we set the CT
cutoff at 35 cycles and the boundary to 2-fold. We calculated fold change by the ΔΔCT
method, in which the average ΔCT
of the control group (CT
(gene of interest) − average CT
(housekeeping genes)) is subtracted from the average ΔCT
of the test group, and the outcome is converted to a linear scale:
Ingenuity pathway analysis (IPA) was performed on gene expression data to explore possible upstream biological regulators and downstream effects based upon previous reports in the literature (Kramer, Green, Pollard, & Tugendreich, 2014). QIAGEN IPA (Germantown, MD, USA) was accessed through the Johns Hopkins Medical Institution Transcriptomics and Deep Sequencing Core Facility, and only genes with determinable CT values in ≥80% of participant samples were uploaded for analysis, setting the expressed fold regulation cutoff at ±1.2.
Results
We have presented sample characteristics in Table 1. Participants (N = 70) comprised 31 males and 39 females of Asian (14%), African American (34%), Caucasian (44%), and mixed (7%) racial backgrounds, who were, on average, 28.23 ± 7.89 years old. Of these participants, 27 were diagnosed with IBS (63% female) and 43 served as HC (51% female). Predominant IBS subtypes were IBS-constipation (IBS-C, 44%) and IBS-diarrhea (IBS-D, 44%). Participants with IBS differed from HC in reporting greater levels of perceived stress (p = .034) but did not differ in terms of age, sex, race, years of education, or BMI.
Demographic and Clinical Characteristics of Study Participants.
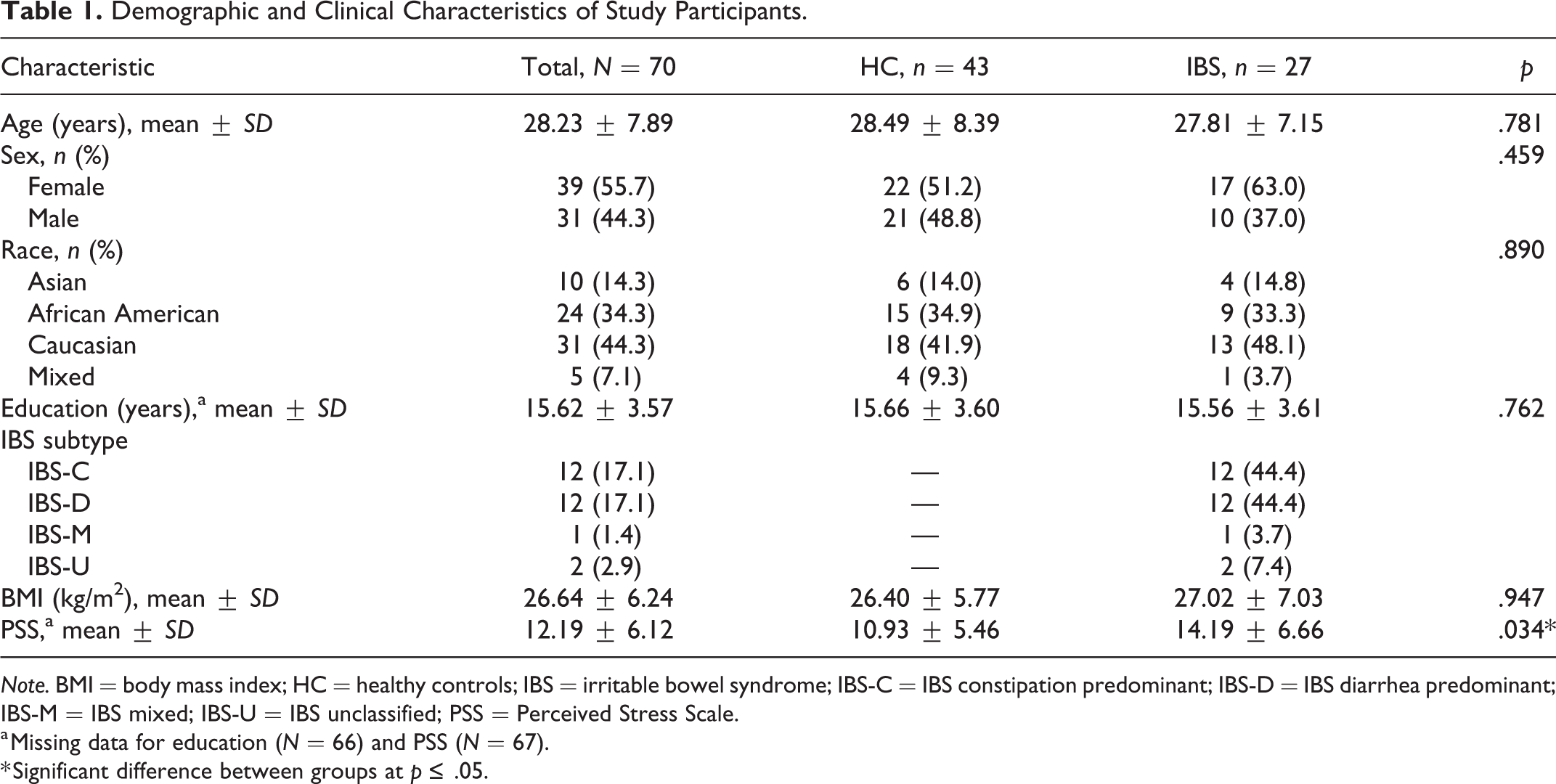
Note. BMI = body mass index; HC = healthy controls; IBS = irritable bowel syndrome; IBS-C = IBS constipation predominant; IBS-D = IBS diarrhea predominant; IBS-M = IBS mixed; IBS-U = IBS unclassified; PSS = Perceived Stress Scale.
a Missing data for education (N = 66) and PSS (N = 67).
* Significant difference between groups at p ≤ .05.
Table 2 lists selected genes of interest in the custom PCR array (gene symbol, reference sequence [Refseq.] number, and name). DECR1 and GAPDH served as housekeeping genes (HKG). All samples for data analysis passed internal quality checks including PCR array reproducibility, reverse transcription (RT) efficiency, and genomic DNA contamination. We found that participants with IBS differed from HC in fold regulation values of ±2 for the following six genes, with statistically significant differences as noted (see Table 3): ADIPOR1, ADIPOR2, CNR2, COMT, OXTR (p = .014), and PPARA.
Selected Genes of Interest for Custom RT2 Polymerase Chain Reaction Array.
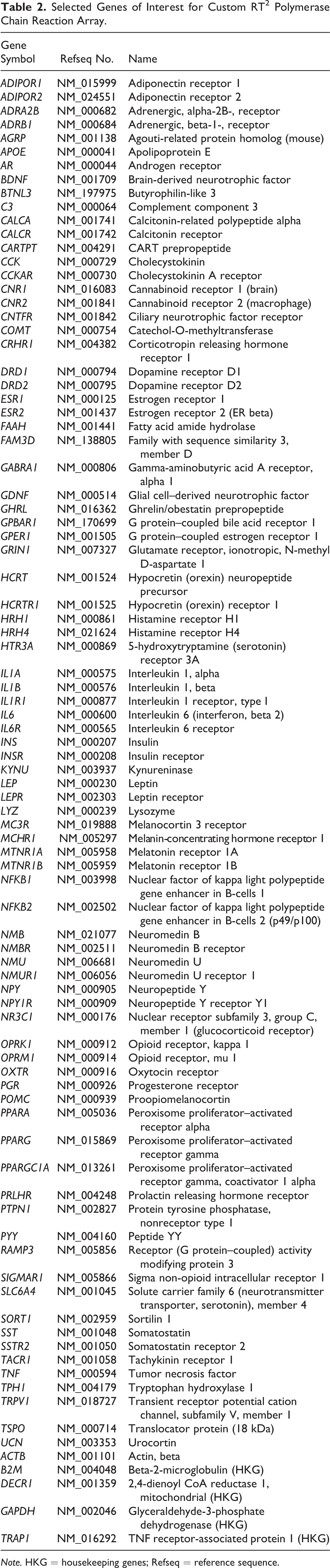
Note. HKG = housekeeping genes; Refseq = reference sequence.
Differential Gene Expression: Participants With Irritable Bowel Syndrome Versus Healthy Controls.
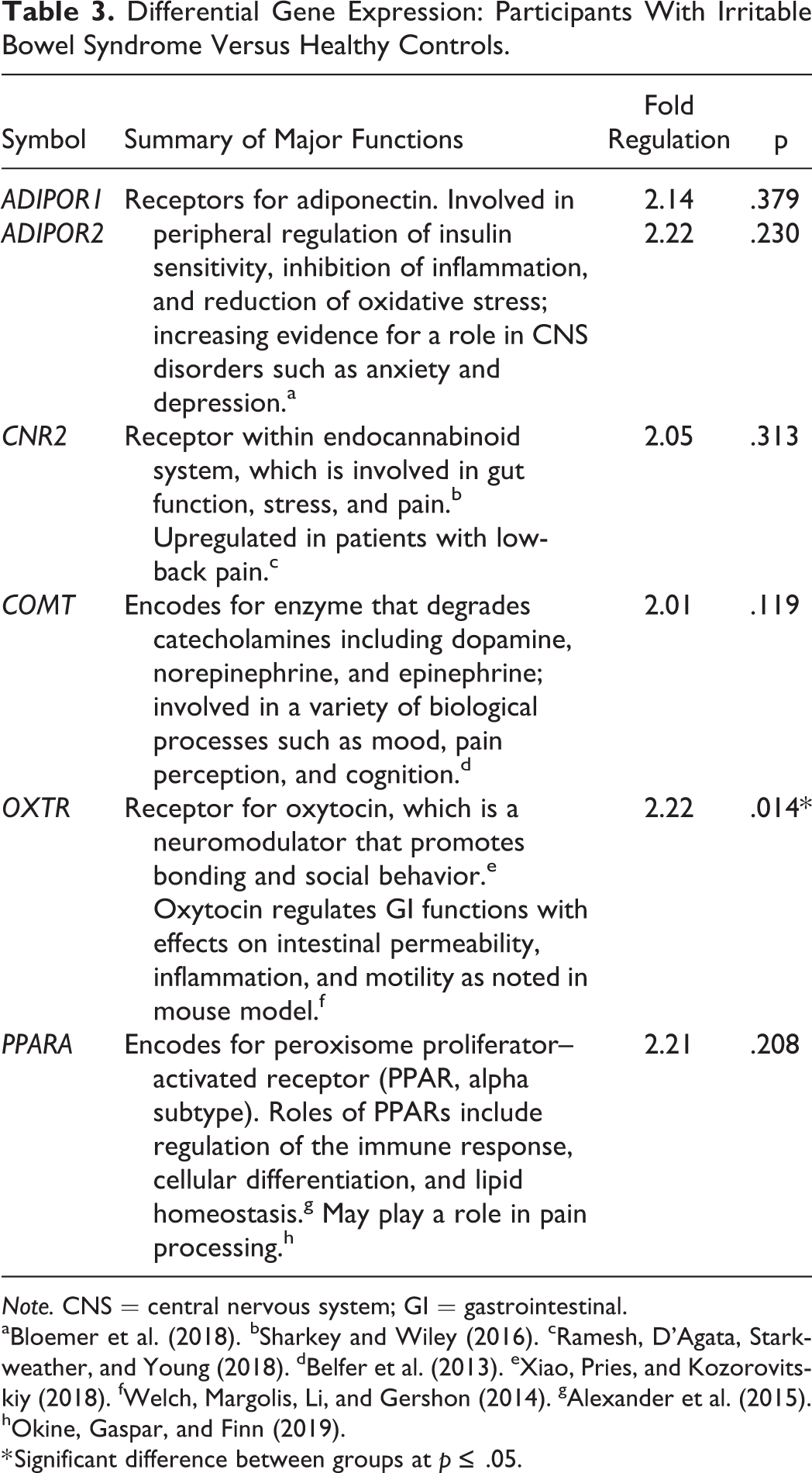
Note. CNS = central nervous system; GI = gastrointestinal.
a Bloemer et al. (2018). b Sharkey and Wiley (2016). c Ramesh, D’Agata, Starkweather, and Young (2018). d Belfer et al. (2013). e Xiao, Pries, and Kozorovitskiy (2018). f Welch, Margolis, Li, and Gershon (2014). g Alexander et al. (2015). h Okine, Gaspar, and Finn (2019).
* Significant difference between groups at p ≤ .05.
We then analyzed gene expression data by participant sex and IBS subtype, with a focus on participants with IBS-C and IBS-D, given their greater prevalence in this cohort (see Table 4). Among female participants, those with IBS-C differed from HC in fold regulation values of ±2 for nine genes, with statistically significant differences for genes ADIPOR1 and COMT. Male participants with IBS-C differed from male HC in fold regulation of ±2 for five genes, although none reached statistical significance. Among female participants with IBS-D, three genes differed from female HC in fold regulation of ±2, with a statistically significant difference noted for the gene ESR1. Male participants with IBS-D differed from male HC in fold regulation of ±2 for 23 genes, with 10 reaching statistical significance: CNR1, IL1B, IL1R1, IL6R, NFKB1, NFKB2, NMUR1, NR3C1, OXTR, and PTPN1.
Subgroup Analyses (Fold Regulation) by Sex and IBS Subtype.
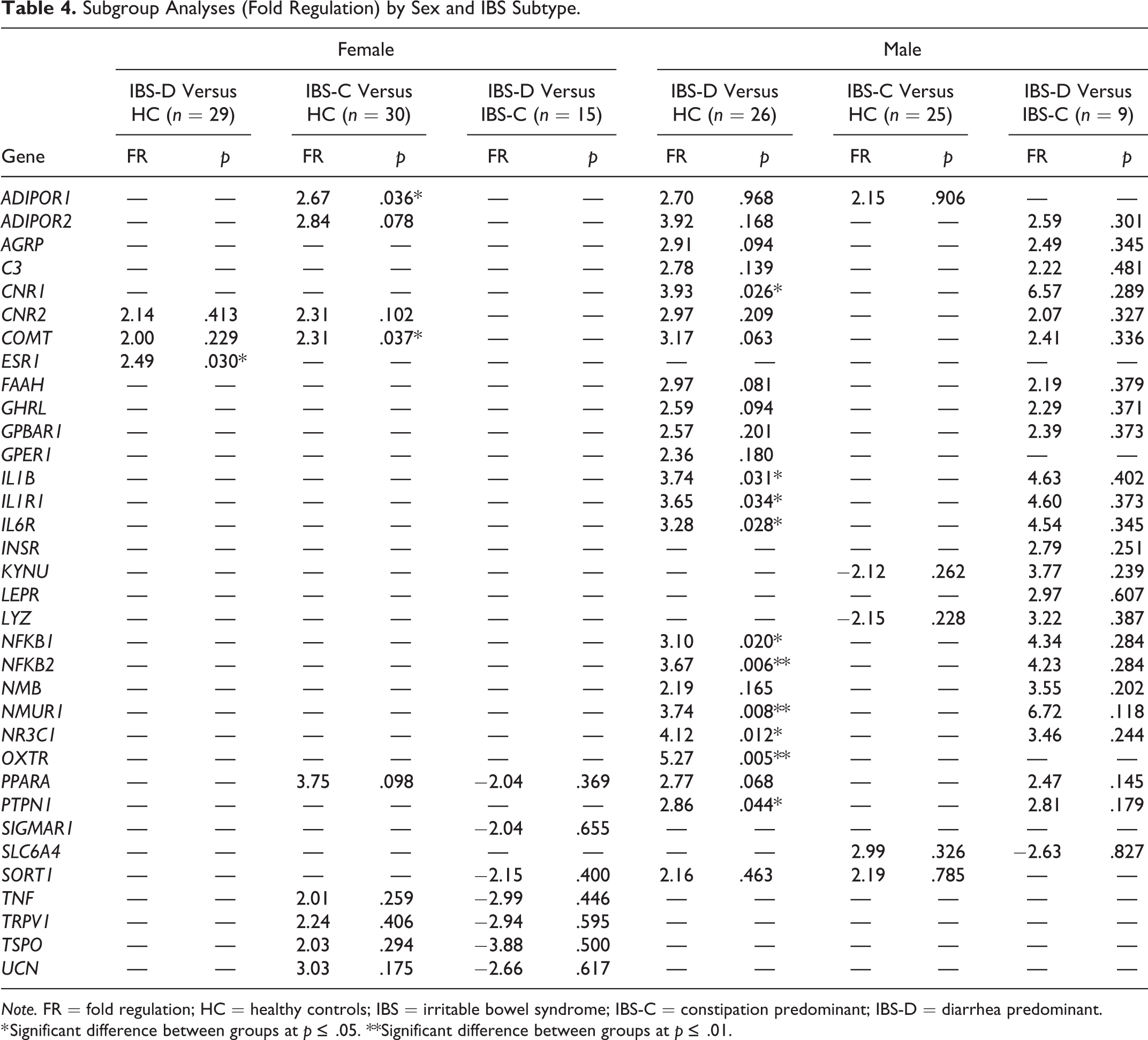
Note. FR = fold regulation; HC = healthy controls; IBS = irritable bowel syndrome; IBS-C = constipation predominant; IBS-D = diarrhea predominant.
* Significant difference between groups at p ≤ .05. **Significant difference between groups at p ≤ .01.
Lastly, we compared females with IBS-C to females with IBS-D and males with IBS-C to males with IBS-D. Although expression of seven genes differed in fold regulation of ±2 between females with the two different subtypes of IBS, none of the differences were statistically significant. Likewise, 24 genes differed in fold regulation values of ±2 between males with the two different subtypes of IBS, but again, none of the differences reached statistical significance (see Table 4).
We then used IPA to compare patterns of gene expression in the total sample from the present study (N = 70) to those reported in the literature and to compare patterns of expression between subgroups. For the overall sample, BDNF was a predicted upstream regulator of differentially expressed molecules, with an activation Z-score of 2.22 and fold change of 1.80. Inhibition of IL1B was an upstream regulator of the expression data for female IBS-D participants in comparison to female HC, with a Z-score of −3.21 and fold change of −1.63. IL6 was an upstream regulator of the expression data for male IBS-D participants in comparison with male HCs, with an activated Z-score of 2.96 and fold change of 1.60. BDNF was also an upstream regulator of the expression data for female IBS-C participants compared with female HC, with an activated Z-score of 2.22 and fold change of 2.25. Lastly, inhibition of CNR1 was a predicted upstream regulator of the expression data for male IBS-C participants compared with male HC, with an activated Z-score of 1.29 and a fold change of −1.67.
We further utilized IPA to evaluate which diseases or functions were predicted or relevant to the gene expression findings. For the overall sample (N = 70), the category of “lipid metabolism, molecular transport, small molecule biochemistry” with the function “quantity of steroid” was predicted to be decreased in IBS participants relative to HC, with a Z-score of −2.45 and including 18 molecules (see Figure 1). Utilizing IPA for subgroup comparisons, we found that relevant diseases and identified categories often differed by IBS subtype, and the direction of expression often differed by participant sex. For instance, the function “release of fatty acid” within the category of “lipid metabolism, molecular transport, small molecule biochemistry” was predicted as diminished for the expression data of females with IBS-D compared with female HC (Z-score = −2.51, 11 molecules), though neither that function nor that category was identified as relevant for females with IBS-C. Conversely, the function “release of fatty acid” was predicted to be increased for the expression data of males with IBS-D versus male HC (Z-score = 2.10, 12 molecules) but was not relevant for males with IBS-C.
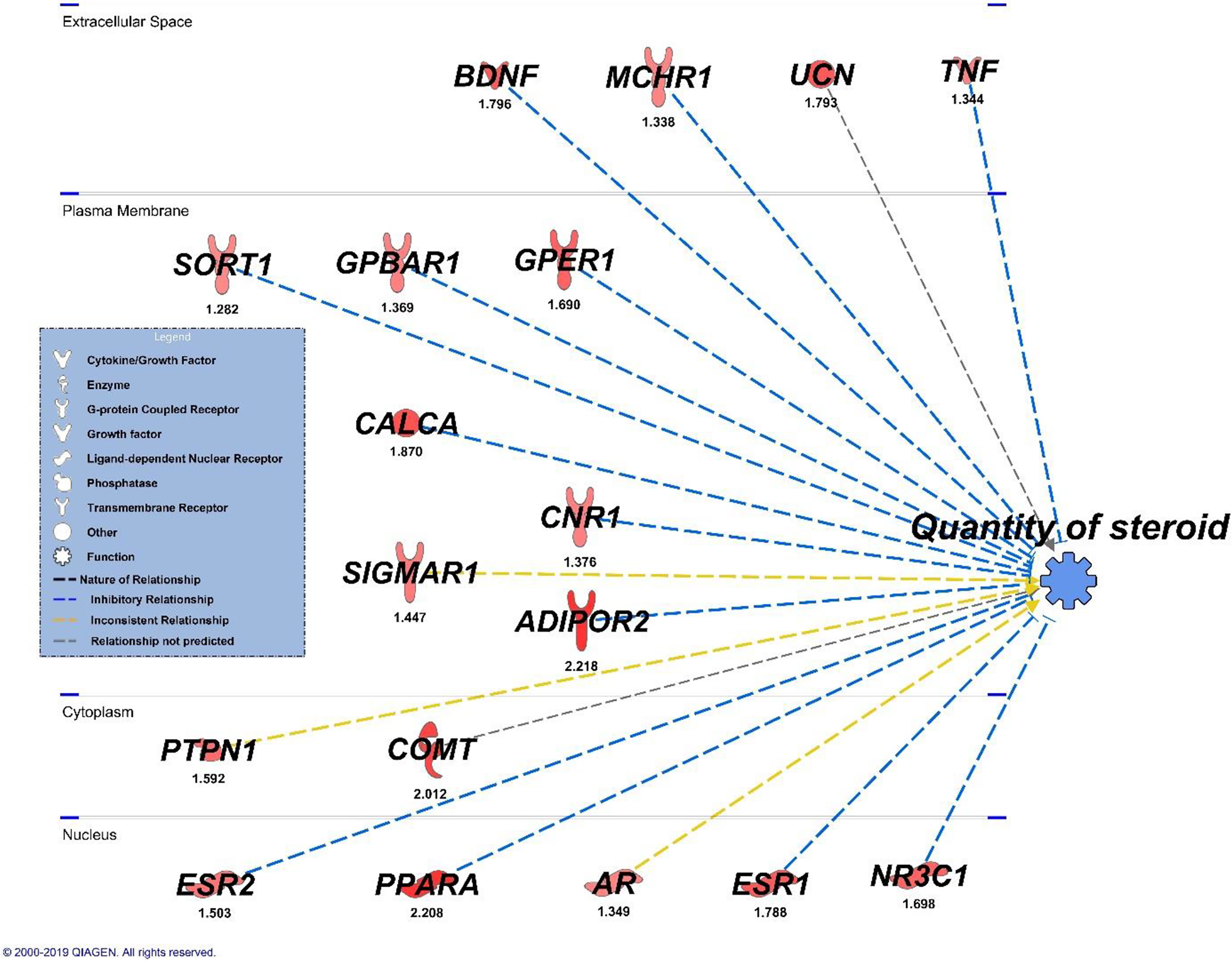
Ingenuity pathway analysis—total sample.
Discussion
The purpose of this exploratory study was to analyze levels of gene expression in participants with IBS compared with HC, focusing on genes that may dually affect gastrointestinal and psychological processes, operationalized within the conceptual framework of the BGA. Our findings contribute to the development of knowledge of genomic associations in IBS by identifying differential patterns of gene expression between participants with IBS and HC and by highlighting the relevance of sex and subtype stratification for such analyses. Recognizing the heterogeneity of the population of patients with IBS and conducting specific analyses accordingly will help advance the field for a disorder that imposes a significant societal burden and adversely affects patients’ quality of life.
In our overall sample analysis, we noted that participants with IBS had an upregulation of genes associated with diverse, yet interconnected, processes such as metabolism, inflammation, immunity, social behavior, and pain compared with HC. Although BMI did not differ significantly between participants with IBS and HC, the expression of ADIPOR1 and ADIPOR2 was upregulated in participants with IBS. Adiponectin receptors are involved in the peripheral regulation of insulin sensitivity, inhibition of inflammation, and the reduction of oxidative stress, with increasing evidence pointing to a role in CNS disorders such as anxiety and depression (Bloemer et al., 2018). Bloemer and colleagues also report the involvement of adiponectin receptor 2 in the pathway activation of peroxisome proliferator–activated receptor alpha (PPARA). In the present study, we found expression of the gene for PPARA to be upregulated in participants with IBS compared with HC.
Peroxisome proliferator–activated receptors (PPARs) are nuclear hormone receptors that perform numerous tasks including regulation of the immune response, cellular differentiation, and lipid homeostasis (Alexander et al., 2015). Research also suggests that PPARs play a role in pain processing, with demonstrated expression along key pain-pathway sites (Okine, Gaspar, & Finn, 2019). Endocannabinoids can activate PPARs, which may mediate the physiological reaction caused by cannabinoid activation, including analgesia, reward, neuroprotection, and anti-inflammatory processes (O’Sullivan, 2016). In the present investigation, we found that gene expression of CNR2, which is related to the endocannabinoid system, differed between participants with IBS and HC overall, and we noted further differences when stratifying by sex and IBS subtype.
Specifically, males with IBS-D displayed an upregulation of CNR1, CNR2, and FAAH in comparison with male HC, while females with either IBS-D or IBS-C showed an upregulation of CNR2 compared with female HC. Prior researchers reported a similar upregulation of CNR2 in patients with low back pain compared with HC, suggesting it may serve as a protective mechanism for those with chronic pain (Ramesh, D’Agata, Starkweather, & Young, 2018). In an earlier pilot investigation, Fichna et al. (2013) reported variations in the expression of genes related to the endocannabinoid system by IBS subtype. Specifically, they found that females with IBS-C, but not females with IBS-D, displayed a significant decrease in FAAH mRNA expression in comparison with HC as measured in colonic biopsies.
The endocannabinoid system is also involved in the regulation of oxytocin (Tasker et al., 2015), a neuromodulator known to promote bonding and social behavior (Xiao, Priest, & Kozorovitskiy, 2018). Oxytocin also regulates numerous GI functions and had demonstrable effects upon intestinal permeability, inflammation, and motility in a mouse model (Welch, Margolis, Li, & Gershon, 2014). Researchers have identified oxytocin and oxytocin-receptor mRNA throughout the human GI tract (Monstein, Grahn, Truedsson, & Ohlsson, 2004), and exogenous administration in healthy women stimulates colonic peristalsis (Ohlsson, Ringstrom, Abrahamasson, Simren, & Bjornsson, 2004). Such observations are relevant to the present study findings in that participants with IBS displayed significantly upregulated levels of OXTR gene expression in comparison with HC. Upon further analysis, we found that males with IBS-D expressed significantly upregulated levels of OXTR in comparison with male HC, whereas other subgroups did not. This variation in gene expression underscores the importance of conducting analyses in IBS patients by sex and subtype in order to gain greater understanding of diverse symptomatology.
We also noted that the expression of COMT was upregulated in IBS participants versus HC overall. However, unlike the findings regarding OXTR, COMT expression was upregulated in males and females with IBS-D and reached statistical significance in females with IBS-C. The catechol-O-methyltransferase (COMT) enzyme is involved in a variety of biological functions, such as mood, pain perception, and cognition, and degrades catecholamines including dopamine, norepinephrine, and epinephrine (Belfer et al., 2013). Although not specific to patients with IBS, an earlier investigation of COMT expression in peripheral blood showed a downregulation in persons displaying higher levels of anxiety and depression and lower resilience in response to stress (Azadmarzabadi, Haghighatfard, & Mohammadi, 2018). Previous studies of a COMT polymorphism, Val158Met, suggest some association with IBS symptoms such as bowel pattern and pain as well as reduced psychological distress in IBS patients undergoing a cognitively focused intervention (Han et al., 2017). Authors have also noted, however, that the relationship between psychological health and the COMT genotype may vary by sex (Hill et al., 2018). The present cohort of participants with IBS reported significantly higher levels of perceived stress than did HC, a subjective finding that could be related to differential expression of stress-related genes such as COMT.
In reviewing genes that may dually affect gastrointestinal and psychological processes in the present study, we noted an upregulation of expression for UCN in females with IBS-C and a downregulation of expression for KYNU in males with IBS-C. The kynurenine pathway catabolizes tryptophan, the precursor to serotonin, and prior investigators have reported diminished levels of kynureic acid and serotonin in the intestinal mucosa of IBS patients compared with HC (Keszthelyi et al., 2013). Serotonin is located in both the ENS and CNS and serves an important role in the development, function, and linking of the BGA (Khlevner, Park, & Margolis, 2018). Meanwhile, UCN encodes for a peptide within the corticotrophin-releasing factor family, which is dually expressed in the brain and colon and plays a role in stress-related colonic transit and visceral hyperalgesia (Tache & Million, 2015). It is worthwhile to note differential expression of such genes by participant sex and IBS subtype as it may relate to the heterogeneity in IBS patients’ clinical presentation. For instance, prior researchers have noted that patients with IBS-C, who in the present investigation displayed ± 2-fold change in expression of KYNU and UCN in comparison with HC, report more anxiety and depression than patients with IBS-D (Eriksson, Andren, Eriksson, & Kurlberg, 2008).
Anxiety and depression can be precipitated by stressful experiences, and stress can also induce physiological changes, including changes to immunological factors (Bekhbat & Neigh, 2018). Suggested pathophysiologic mechanisms for IBS include, but are not limited to, infection, immune activation, low-grade mucosal inflammation, and a disordered gut–brain axis (Holtmann, Shah, & Morrison, 2017). In the present investigation, we found that male participants with IBS-D displayed an upregulation of genes associated with immune/inflammatory processes such as IL1B, IL1R1, IL6R, NFKB1, and NFKB2 in comparison with male HC. Our finding that IL1B was upregulated in IBS-D corroborates findings of one earlier investigation (Gwee et al., 2003) but contradicts those of another (Camilleri et al., 2016). Differences among studies include sample type for gene expression analysis and sex of included participants. It is worthwhile to note that researchers have reported males and females with IBS to display differential levels of circulating cytokines (Bashashati et al., 2014; Choghakhori, Abbasnezhad, Amani, & Alipour, 2017); thus, sex differences in cytokine profiles may contribute to the difficulty in understanding the mechanisms of IBS. Furthermore, if cytokine differences exist between the sexes, variations can also occur within a single sex due to physiological regulators such as sex steroid hormones. In the present investigation, the expression of ESR1 was significantly upregulated in females with IBS-D compared with female HC but did not differ between females with IBS-C and female HC. Therefore, differences in gene expression may translate into downstream effects and play a role in the heterogeneous symptom presentation of patients with IBS.
In an effort to detect patterns or pathways associated with differential gene expression, we utilized IPA in the present exploratory investigation. Predicted upstream regulators of BDNF and IL6 and inhibition of IL1B lend insight into overarching processes that could be related to differences between participants with IBS and HC and among participants with IBS. Similarly, diseases or functions predicted from differential gene expression using IPA could help direct future avenues of clinical research. For instance, expression differences related to lipid metabolism might encourage future research related to steroids and inflammatory mechanisms, with enhanced attention to participant sex and IBS subtype. We noted many differences in gene expression by IBS subtype in the present study that can serve as a starting point for future investigations. By conducting such specific analyses in larger cohorts, we may glean insight into etiological and perpetuating factors of IBS.
Limitations of this investigation include the small sample size, which restricted the scope of inquiry and generalizability of findings. We may not have detected some patterns of gene expression and were not able to explore some variations, such as race, that may affect IBS symptomatology. Participants with IBS in the present sample did not carry a psychiatric diagnosis; therefore, gene expression related to psychological processes may be less robust than in other IBS populations. Furthermore, we did not include early life trauma/childhood adversity in our study analysis, though this factor is relevant to levels of gene expression. Lastly, we evaluated gene expression in peripheral whole blood. Although our sample type is less specific than, for instance, tissue from colonic biopsies, we chose accessibility of measurement and potential for hypothesis-generating findings over more invasive methods of specimen collection.
In conclusion, in the present exploratory investigation, we analyzed expression levels of genes that may dually affect gastrointestinal and psychological processes to further our understanding of the BGA in patients with IBS. In comparing participants with IBS to HC and conducting further analyses by sex and IBS subtype, we found differential expression of genes involved in processes such as pain, stress, social behavior, inflammation, immunity, and metabolism, all the while recognizing that manifestation of symptoms is likely related to the interplay among these signaling systems. Such findings are relevant to nursing practice in that we gain an appreciation of the interrelated processes that may underlie symptom presentation in patients with IBS. Such insight can help direct future avenues of patient-related research, accelerate our understanding of patient symptomatology, and facilitate the design of personalized interventions to improve outcomes in this patient population.
Footnotes
Acknowledgments
The authors would like to acknowledge funding and support from the U.S. Department of Health and Human Services, National Institutes of Health, National Institute of Nursing Research (G.D.M.: NR018075), Division of Intramural Research (W.A.H.:1ZIANR000018, 10; KRW: Intramural Research Training Award, Graduate Partnership Program). K.R.W. also received support from the National Institute of Neurological Diseases and Stroke while at Johns Hopkins University (grant no. T32NS070201) and would like to thank Conover Talbot, Jr., from the JHMI Transcriptomics and Deep Sequencing Core Facility for expression and pathway analytical assistance. Further thanks are extended to Drs. Wang, Kim, and Tamez for their input and support as part of the Intramural Program of NINR.
Author Contributions
Kristen R. Weaver contributed to conception and design, acquisition, analysis, and interpretation; drafted the manuscript; critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Gail D’Eramo Melkus contributed to conception and design, analysis, and interpretation; critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Jason Fletcher contributed to conception and design, analysis, and interpretation; critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Wendy A. Henderson contributed to conception and design, acquisition, analysis, and interpretation; critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: U.S. Department of Health and Human Services, National Institutes of Health, National Institute of Nursing Research (G.D.M.: NR018075), Division of Intramural Research (W.A.H.:1ZIANR000018, 10; K.R.W.: Intramural Research Training Award, Graduate Partnership Program). K.R.W. also received support from the National Institute of Neurological Diseases and Stroke while at Johns Hopkins University (grant no. T32NS070201).