
Abstract
Sepsis is a life-threatening syndrome that occurs in response to a severe infection. In recent years, the understanding of the pathobiology of sepsis has been refined, with research describing an altered host response as the underlying cause. Survivors of sepsis often have long hospital stays and suffer from subsequent frailty and long-term health consequences. Predicting attributes of sepsis survivors remains challenging; however, an obesity paradox exists, wherein obese individuals survive sepsis at higher rates than their normal-weight counterparts. We present a model that describes the relationships between sepsis and obesity, focusing on inflammation as a shared pathway for dysregulation in obese and healthy-weight adults. Understanding the interaction of these complex variables is an important first step toward developing interventions and treatments to augment sepsis survival.
Sepsis is a life-threatening syndrome in which the pro- and anti-inflammatory responses of complex biologic systems to pathogenic invaders evolve over time, typically resulting in a dysregulated, or exaggerated, host response (Singer et al., 2016). Not only is sepsis a public health priority in the United States, where it affects 1.7 million adults per year (Centers of Disease Control and prevention [CDC], 2016), it is a global health burden, with an estimated 30 million cases and 6 million deaths per year worldwide (Reinhart et al., 2017). In response to this crisis, the World Health Assembly (WHA) has published recommendations for researchers and clinicians centered on prevention, early diagnosis, and management of sepsis to reduce premature deaths and the effects of long-term disability for survivors (Reinhart et al., 2017). The National Institute of Nursing Research (NINR) supports nursing science aimed at developing new biological knowledge that will translate into improving patient health outcomes and reducing disabling effects of symptoms (NINR, 2016).
Identifying sepsis phenotypes is critical to the goal of promoting early diagnosis and management support. In recent years, researchers have described an obesity paradox in sepsis, whereby obese patients survive at higher rates than their nonobese counterparts (Abbate et al., 2016; Arabi et al., 2013; Meyer et al., 2018; Nguyen et al., 2016; Wacharasint et al., 2013). Identifying the causal mechanisms and teasing out characteristics of an obese-sepsis phenotype is one step toward meeting the goals of the WHA and the NINR. The causal mechanisms for the obesity paradox have not been fully described, nor is there an established theoretical framework in which to test the salient variables thought to contribute to this phenomenon. In this article, we present a model that describes the relationship between sepsis and obesity, focusing on inflammation as a shared pathway for dysregulation in obese adults that affects mortality rates. By identifying patient phenotypes, research to explain the obesity paradox in sepsis may lead to interventions that aid in early diagnosis and contribute to management algorithms that can reduce the burden of debilitation and persistent symptoms for survivors.
Concepts
Inflammation
As a protective mechanism, the body responds to noxious stimuli, such as a pathogenic invader, with the inflammatory response, which communicates exposure and contains the foreign substance (Bennett et al., 2018; Del Giudice & Gangestad, 2018). Governed by immune regulatory pathways, the sympathetic nervous system (SNS) triggers peripheral pro-inflammatory responses, while the parasympathetic nervous system (PNS) and the neuroendocrine hypothalamic-pituitary-adrenal (HPA) axis balance sympathetic effects by inhibiting inflammatory responses. Cytokine and hormonal influences mediate the SNS, PNS, and HPA pathways (Bennett et al., 2018). At the intersection of the immune and neuroendocrine systems, cytokines and immune mediators released during the immune response can activate both neural responses that exaggerate local inflammation and neuroendocrine responses that restore homeostasis (Bennett et al., 2018).
Under normal circumstances, nonspecific inflammation functions to increase blood flow, dispatch white blood cells to infiltrate the area and isolate the threat, and increase phagocytosis to remove the threat. Normally, this process is followed by downregulation of inflammation to promote healing and maintain homeostasis (Bennett et al., 2018). Invasion or injury to the body activates the inflammatory response, causing the release of monocyte/macrophage cells followed by the release of cytokines and chemokines, such as interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α), that mediate nonspecific cellular, tissue, and vascular damage (Bennett et al., 2018; Del Giudice & Gangestad, 2018). The activity of monocyte/macrophage cells is heightened in the state of obesity and is a likely confounding factor contributing to the obesity paradox.
Obesity
Characterized by excess adipose tissue, obesity is a global health concern that increases the risk of comorbidities, decreases life expectancy, and results in 2.8 million deaths annually (Pal et al., 2015). Antecedents of obesity include energy intake and usage imbalance, decreased physical activity, and genetic predisposition (Pal et al., 2015). Recent observations point to socioeconomic status and environmental factors causing relevant epigenetic modifications as well (Vecchié et al., 2018). Obesity is associated with several disorders such as metabolic syndrome, type 2 diabetes, cardiovascular disease, lipid disorders, stroke, sleep apnea, and cancer (CDC, 2018). In the United States, middle-aged (40.2%) and older adults (37%), non-Hispanic Black (48.1%) and Hispanic individuals (42.5%) have higher rates of obesity than other groups (CDC, 2018). The CDC (2018) estimated the economic burden of obesity in the United States in 2008 to be $147 billion.
The World Health Organization (WHO, 2020a) defines obesity as an accumulation of abnormal or excessive fat that is a risk to health. The Obesity Society elaborates, defining obesity as a chronic disease with multiple phenotypes resulting from long-term positive energy balance and excess adiposity that leads to physiologic abnormalities (Jastreboff et al., 2019). Obesity is a clinical diagnosis that is determined by body mass index (BMI), an index of weight adjusted for height (kg/m2), that serves as a surrogate measure of body fat (CDC, n.d.). Individuals are classified based on BMI ranges, such that BMI < 18.50 kg/m2 defines underweight, BMI = 18.50–24.99 kg/m2 defines normal weight, BMI = 25.0–29.99 kg/m2 defines overweight, BMI = 30.0–39.99 kg/m2 defines obese, and BMI > 40 kg/m2 defines very obese (WHO, 2020b). A limitation of the use of BMI as the basis for classification is that individuals with varying clinical and biochemical characteristics are placed in the same category regardless of emerging evidence of obesity phenotypes (Vecchié et al., 2018). Despite this limitation, researchers still accept BMI internationally as the standard method for identifying and defining obesity (Engin, 2017).
Neurophysiologic control of energy balance and regulation of body weight occurs along the HPA axis. In obesity, chronic low-grade inflammation increases pro-inflammatory cytokines while alteration in the HPA axis increases catecholamine and glucocorticoid levels that, together, contribute to modulation of immune function (Pal et al., 2015; Figure 1). The consequences of obesity stem from the activity of adipose tissue, which is upregulated when the tissue is present in excess. Adipose tissue secretes a large number of adipokines that have integral roles in immunometabolism. For example, chronic low-grade inflammation occurs when macrophages preferentially take up residence in adipose tissue (Na et al., 2018) leading to upregulation of cytokine IL-6, C-reactive protein (CRP), and TNF-α, while parallel upregulation of the pro-inflammatory adipokine leptin and downregulation of the anti-inflammatory adipokine adiponectin takes place (Cottam et al., 2004). Despite the subsequent hyperleptinemia, leptin is biologically unavailable; thus, the effects of leptin are often not observed in obesity, and leptin resistance is independently associated with insulin resistance in obesity, suggesting that leptin receptor activity may be altered (Sudhakar et al., 2018). Concentration of the protein CRP increases significantly during inflammation and obesity and is independently associated with changes in leptin levels. Researchers have hypothesized that CRP interacts with the leptin receptor, linking CRP and leptin to immune function. Receptor resistance associated with obesity is not a novel concept. Insulin resistance is widely accepted to be a consequence of obesity (Dandona et al., 2004; Jung et al., 2018).
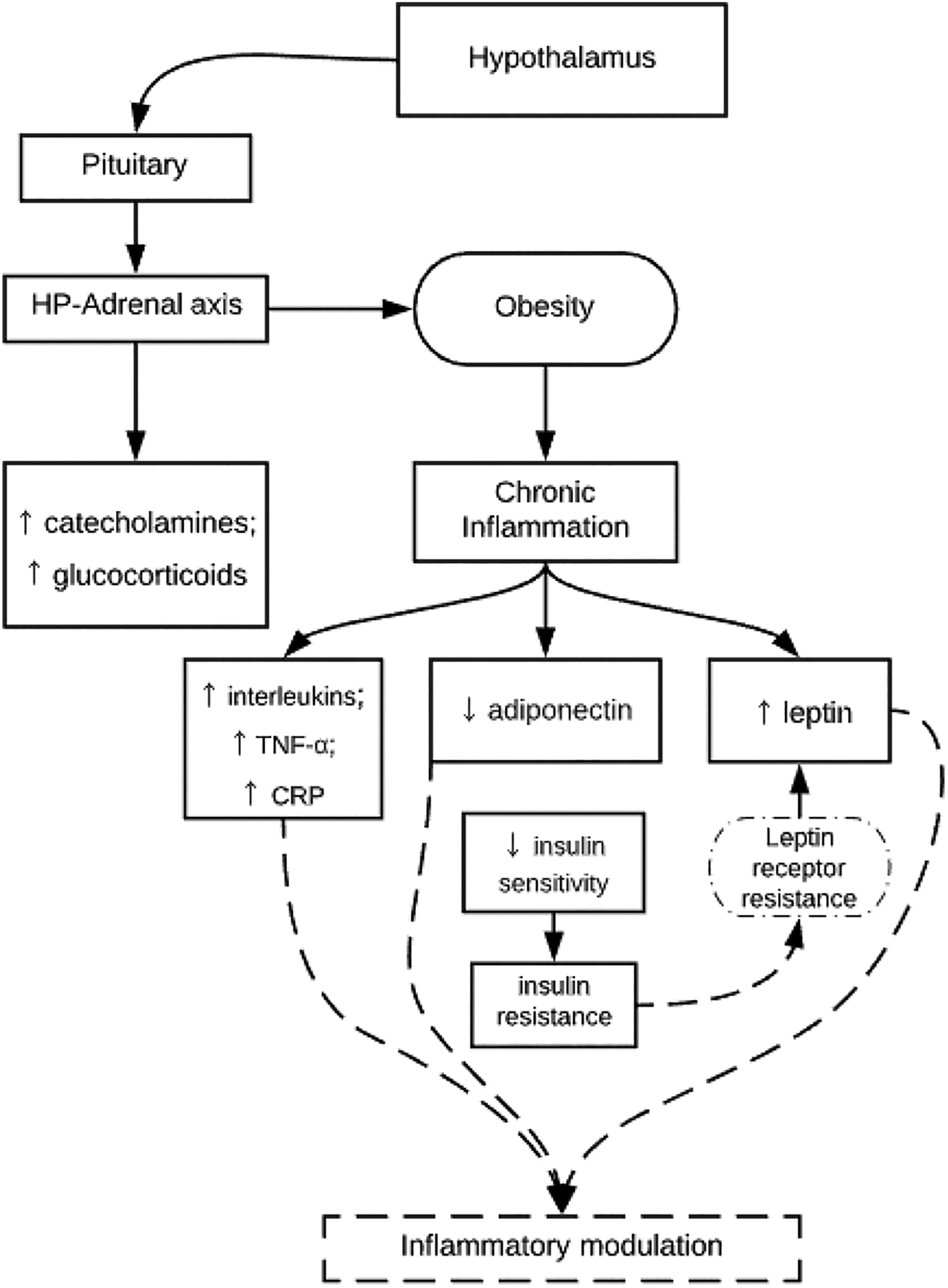
A hypothesized model of inflammatory modulation in obesity. The hypothalamic–pituitary–adrenal (HP–Adrenal) axis exerts action on cellular mechanisms in both obesity and inflammation (adapted from Pal et al., 2015). In obesity, there is heightened immunometabolic activity, inducing a state of chronic low-grade inflammation. Macrophages/monocytes that take up residence in adipose tissue alter immunometabolic inflammation, such that the cytokines interleukin (IL)-6, C-reactive protein (CRP), tumor necrosis factor (TNF)-α, and leptin are upregulated while parallel downregulation of the anti-inflammatory adipokine adiponectin occurs (Cottam et al., 2004). There is a relationship between adipokines (adiponectin and leptin) and decreased insulin sensitivity and insulin resistance. As shown by the dashed lines, the present model hypothesizes that a similar mechanism occurs in the case of leptin, wherein leptin is increased but biologically unavailable due to leptin receptor resistance, which contributes to inflammatory modulation.
Sepsis
Sepsis is a heterogeneous syndrome in which the host response to inflammation and infection becomes excessive, causing harm to the epithelium and capillary leakage, leading to organ failure and death (Cohen et al., 2015). Sepsis with organ dysfunction (severe sepsis) and septic shock is associated with higher mortality rates, up to 50%, while general sepsis has a mortality rate of less than 20% (De La Rica et al., 2016). Mansur et al. (2015) reported a 71% increase in cases of severe sepsis between 2003 and 2007 and reported that total costs for all patients with severe sepsis increased by 57% over the same time period. The approximate cost of sepsis care in 2008 was $14.6 billion in the United States (Hall et al., 2011).
The risk factors for sepsis are varied. More than half of the cases of severe sepsis occur in adults above age 65 (Mayr et al., 2014). Although sepsis can occur in both sexes, it is more common in males (De La Rica et al., 2016; Sakr et al., 2012). Black patients have a higher incidence of both sepsis and severe sepsis than their White counterparts (Barnato et al., 2008; Dombrovskiy et al., 2007); in fact, De La Rica and colleagues (2016) found that Black patients had a 2-fold greater probability of experiencing sepsis in the United States compared to White patients. Over half of the patients with sepsis have chronic comorbid conditions such as diabetes, congestive heart failure, chronic pulmonary disease, cancer, or chronic renal failure (De La Rica et al., 2016; Mayr et al., 2014).
While systemic inflammatory response syndrome has been the focus of sepsis research for the last 2 decades (Bone et al., 1992; Levy et al., 2003), a refined understanding of the pathophysiology now points to an altered host response as the underlying cause of sepsis (Singer et al., 2016). When the body encounters a pathogenic invader, an inflammatory and immune response occurs in an attempt to isolate the threat. If not contained, the pathogenic invader can cause infection, and the immune response will trigger the release of leukocytes to systemically counteract the pathogenic invader in an attempt to recover (Figure 2). In sepsis, the host inflammatory response is so excessive that the cytokine storm causes epithelial damage, increased capillary permeability, organ dysfunction, and even death (Winters et al., 2010). Of course, at any point in this process, recovery can occur either spontaneously or, more likely, due to aggressive medical treatment. Currently, one in three hospital deaths is due to sepsis (CDC, 2016). As discussed above, however, researchers have documented an obesity paradox, whereby obese patients with sepsis survive at higher rates than do their nonobese counterparts (Abbate et al., 2016; Nguyen et al., 2016; Prescott et al., 2014; Wacharasint et al., 2013). In fact, increased BMI has been associated with decreased mortality from postoperative sepsis (Davenport et al., 2009; Memtsoudis et al., 2012), community-acquired pneumonia (Braun et al., 2017), and septic shock (Arabi et al., 2013; Wacharasint et al., 2013).
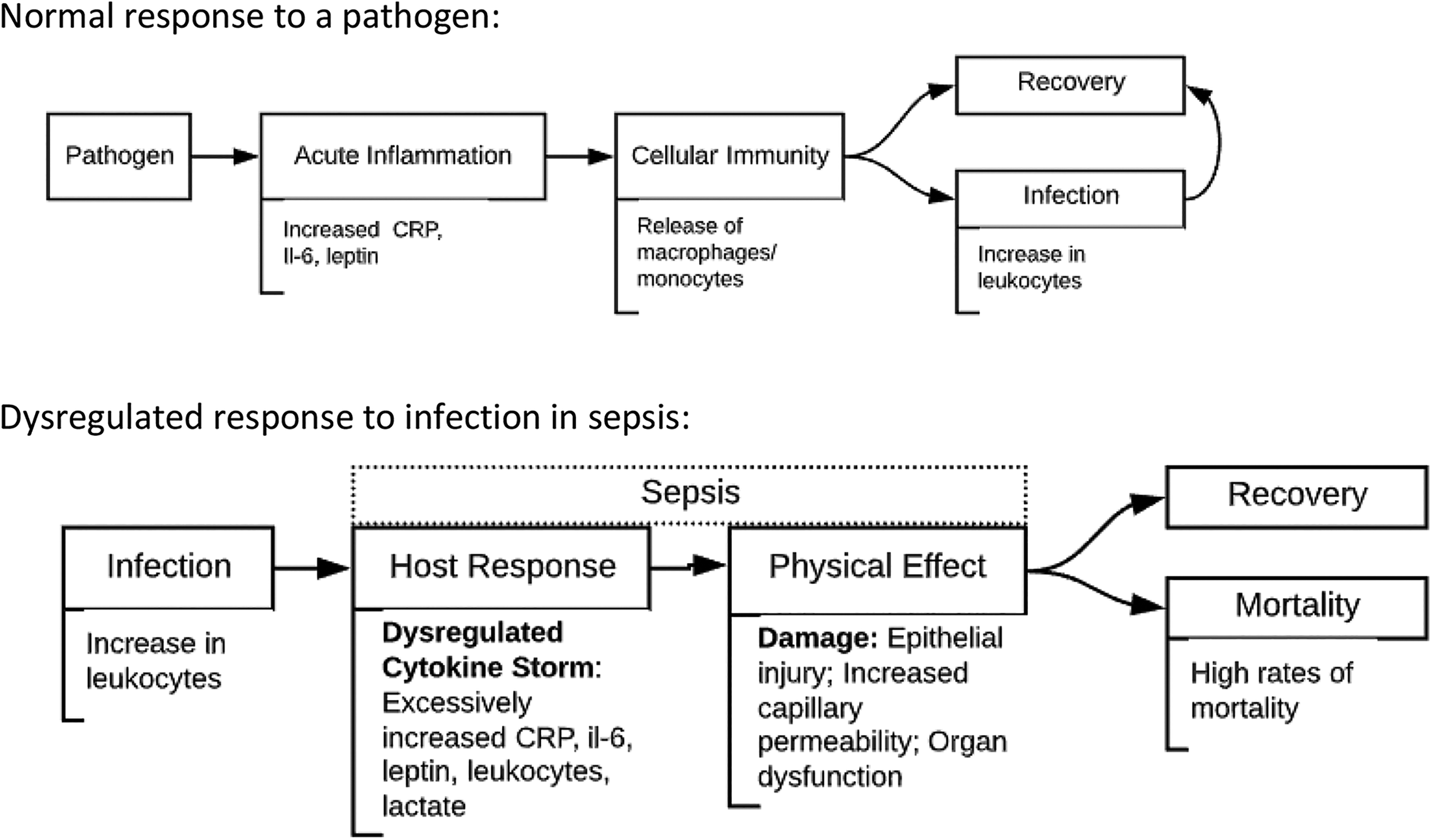
A comparison of the normal response to a pathogen and the dysregulated response in sepsis. The top figure depicts the normal response to a pathogen, in which a pathogen elicits the ubiquitous acute inflammatory response, which is followed by the activation of cellular immunity, including release of the leukocytes called macrophages/monocytes, followed by recovery or a state of infection that typically leads to recovery. In sepsis, as depicted in the bottom figure, the body responds to infection in a dysregulated, overactive manner by releasing cytokines excessively. The physical effect of the cytokine storm is damage from epithelial injury, increased capillary permeability, and organ dysfunction. Together this damage is responsible for high mortality rates from sepsis. CRP = C-reactive protein; IL-6 = interleukin 6.
Relationship Between Obesity and Sepsis
Obesity and sepsis share the inflammation pathway. Obesity is associated with chronic low-grade inflammation, whereas sepsis is an acute state of inflammation and dysregulated host response. The model presented in Figure 3 is based on the hypothesis that obesity-related chronic inflammation, characterized by upregulation of the pro-inflammatory markers IL-6, CRP, and leptin, actually modulates the insult from sepsis. Therefore, when the excessive inflammation of sepsis occurs, the effect is less severe and the result is a more balanced physiologic response that causes less endothelial damage, less capillary permeability, and ultimately, less organ dysfunction (Figure 3).

The hypothesized relationships among obesity, sepsis, and sepsis mortality. Obesity is accompanied by chronic inflammation. In this model, chronic inflammation is hypothesized to modulate the sepsis host response (indicated with dotted lines), which results in an attenuated cytokine release and physical effect. Together, the attenuated cytokine release and lessened physical damage lead to lower mortality rates than in normal-weight individuals. CRP = C-reactive protein; IL-6 = interleukin 6.
Discussion
The conceptual model we have presented is a theoretical construct based on what is understood about pathophysiology and reports of the obesity paradox. While offering a sound base upon which to test the salient variables of obesity, sepsis, and mortality, this model also allows for adaptability to test for associations between variables that will help to distinguish sepsis phenotypes. For example, investigators could test the relationships between obesity, demographic variables, biologic indicators of host response to infection, and degree of sepsis severity and the dependent variables of mortality time points and long-term effects (Figure 4). Examination of these potential relationships is important to fully understand risk factors for individuals based on their unique phenotypical context.
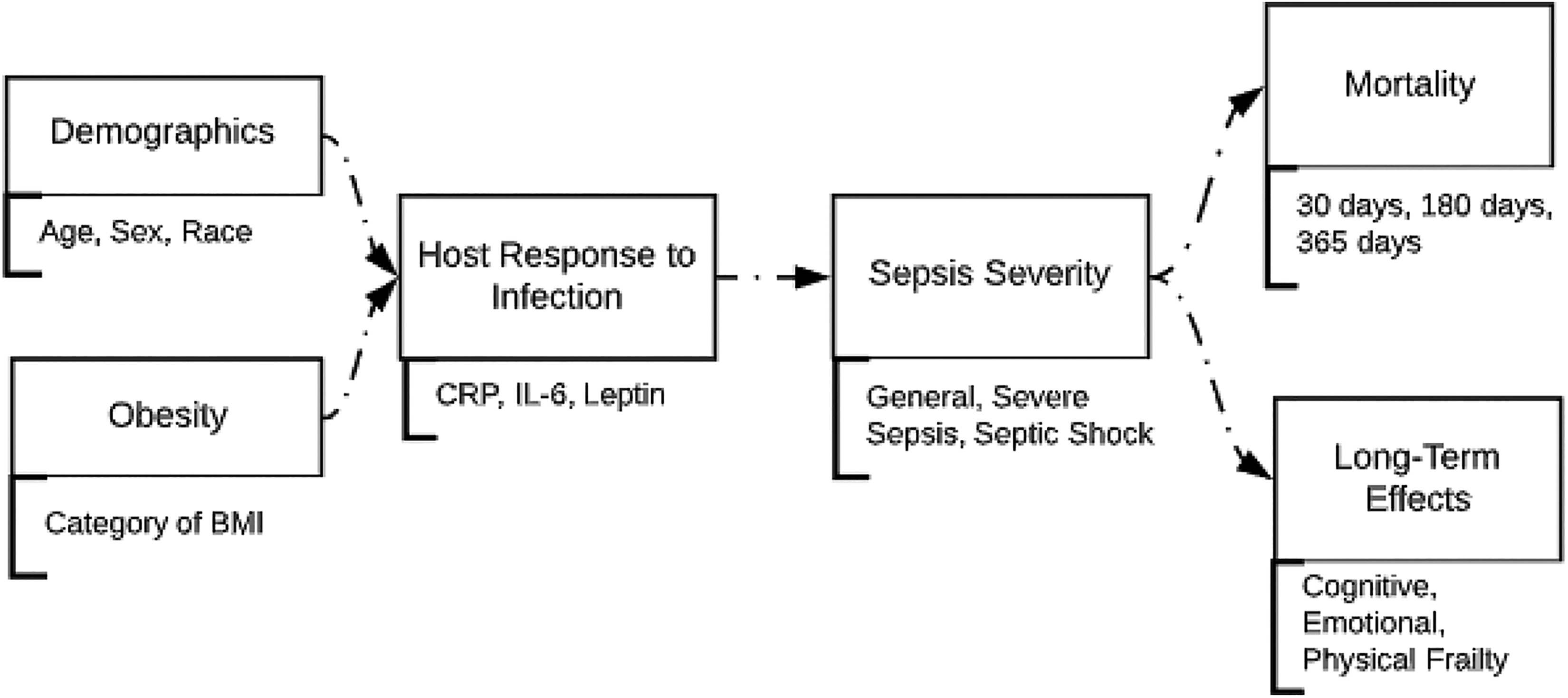
Proposed model to test relationships between variables associated with sepsis to allow for the identification of sepsis phenotypes. In this representation, the relationship between the host response and severity of sepsis remains constant; however, different variables are added to further explicate potential relationships. This model tests the relationships between the independent variables of demographic information, obesity, biologic indicators of host response to infection, and sepsis severity and the dependent variables of mortality time points and long-term effects of sepsis. BMI = body mass index; CRP = C-reactive protein; IL-6 = interleukin 6.
An exploration of pathophysiology points to inflammation as the common characteristic shared by obesity and sepsis. The underlying mechanism of insulin resistance is due to the immunometabolic actions of adipose tissue. The same mechanism may be responsible for hyperleptinemia in obesity. Adipocytes produce the pro-inflammatory adipokine leptin and the pro-inflammatory cytokine IL-6, which are upregulated in obesity and sepsis, and leptin and IL-6 independently promote the synthesis of CRP, a protein released during inflammation (Hribal et al., 2014). These same players are known to be elevated in obesity-related insulin resistance, providing a physiologic precedent for receptor resistance (Figure 1; D’Alessandris et al., 2007; Osborn & Olefsky, 2012). Leptin receptor resistance causes hyperleptinemia, in which higher than normal leptin levels are present but the leptin is biologically unavailable. In other words, hyperleptinemia is the result of a physiologic attempt to activate leptin receptors by increasing leptin levels, causing the unexpected effect of an attenuated inflammatory response. This modulated physiologic response seems to provide protection in cases where both obesity and sepsis are present, leading to an inflammatory response that is attenuated rather than excessive and resulting in less tissue damage, less severe systemic response, and ultimately lower rates of severe sepsis, septic shock, and death (Hillenbrand et al., 2010). The conceptual model we have presented here allows for the testing of these relationships to build upon the current body of knowledge (Figure 4).
Due to the serious nature of sepsis, theories continue to emerge, and research is underway examining factors impacting the long-term effects of sepsis. The persistent inflammation, immunosuppression, and catabolism syndrome hypothesis builds on the chronic critical illness model and attempts to define a phenotype of critical illness (Kamel et al., 2018). The main tenet is that, given the excess energy stores in obesity, catabolism may not be as deleterious as it is in lean individuals. The researchers state that further research is needed to control for increased adiposity. This theory may offer an additional lens through which to view the complexity of sepsis mortality in obesity. We propose that this theory does not negate the conceptual model we have presented here. Instead, we agree that this theory has merit and could be tested within the model we have proposed.
Researchers have observed the association between obesity and decreased sepsis mortality in several populations yet have not yet fully described the mechanism. For example, investigators have documented associations between increased BMI and decreased mortality in postoperative sepsis in vascular surgery (Davenport et al., 2009) and laparoscopic gastric bypass (Villamere et al., 2014), in sepsis from pneumonia (Corrales-Medina et al., 2011; Kahlon et al., 2013; King et al., 2013; Nie et al., 2014; Reiner et al., 2009), and in septic shock (Arabi et al., 2013; Wacharasint et al., 2013). While obesity puts patients at higher risk of contracting adult respiratory distress syndrome after surgery, the risk of mortality is lower in obese patients than in normal-weight patients (Memtsoudis et al., 2012). Authors have proposed that because obese individuals are more likely to have sepsis caused by the less virulent gram-positive infections such as from skin and soft tissue infection compared to nonobese patients, their survival rate is higher (Arabi et al., 2013). However, we suggest that obesity-related chronic low-grade inflammation attenuates the host response, resulting in lower mortality (Figure 3). The variability in postoperative sepsis mortality could, in fact, be related to pathogenic virulence in combination with obesity-related inflammation modulation (Figure 3). Sepsis in obese patients from underlying respiratory infections, which are predominantly caused by virulent gram-negative organisms, is associated with reduced 30-day mortality, suggesting that obesity offers a protective effect (Corrales-Medina et al., 2011; Kahlon et al., 2013; King et al., 2013; Nie et al., 2014; Reiner et al., 2009). Investigators have also found that obesity is associated with increased survival in septic shock, indicating that the host response may be as important as microbial virulence when it comes to sepsis mortality (Arabi et al., 2013; Wacharasint et al., 2013). However, in the case of the highly pathogenic H1N1 influenza, obese patients with sepsis had a higher 30-day mortality rate compared to normal-weight patients, which could be explained by the rapidity of the onset of illness associated with influenza, wherein the attenuation of the host response might not be strong enough to halt its effects (Kwong et al., 2011).
Several studies have presented contradictory evidence on the association between obesity and decreased sepsis mortality in adults. We propose that methodological stringency and use of the present conceptual model would help to strengthen interpretability of the results. Gaulton et al. (2014) reported no difference in sepsis survival between obese and normal-weight individuals, but subjects were patients with presumed, rather than confirmed, sepsis, meaning that they may not have had sepsis, severe sepsis, or septic shock. Papadimitriou-Olivgeris et al. (2016) reported no difference in survival rates in obese individuals when comparing sepsis outcomes to those of other critical illnesses such as intracranial hemorrhage, respiratory insufficiency, trauma, and a category of “others.” However, comparison of survival from sepsis to that from other critical illnesses with different pathophysiologies is difficult to interpret and limits generalizability of the findings.
Given the charge from the WHA (2017) to focus research and clinical practice on prevention, early diagnosis and treatment of sepsis, it is not surprising that treatment guidelines focus on advances in supportive care, source control, maintenance of hemodynamic stability, and anti-infective agents (Teng et al., 2018). Indeed, the Surviving Sepsis Campaign (2018) recommends measurement of biologic indicators, such as serum lactate, to guide treatment and administration of anti-infective drugs after obtaining blood cultures. Recent research has shown adjuvant targeted therapies such as activated protein C, toll-like receptor 4 antagonist, tumor necrosis factor receptor antagonist, and interleukin receptor antagonist to be ineffective or harmful (Teng et al., 2018). Using the conceptual model described here to test relationships among the biologic indicators CRP, IL-6, and leptin might result in changes to clinical practice by providing a guide to risk stratification and early recognition or by providing a road map to reducing long-term debilitation.
One adjuvant approach that warrants investigation is the administration of leptin (metreleptin) to nonobese sepsis patients to simulate the immunomodulatory effect that obesity has in sepsis (Figure 3). Currently metreleptin is used to treat congenital leptin deficiency and lipodystrophy, but there is no Food and Drug Administration approval at this time for other uses (Blüher & Mantzoros, 2015). A risk of treating nonobese individuals with leptin relates to the orexigenic, or loss of appetite, effect that leptin is known for, which could reduce energy stores. More research to better understand how exogenous leptin administration might affect nonobese individuals and sepsis mortality is needed.
Conclusion
Inflammation is the common thread linking obesity and sepsis. While it may be unusual to describe protective effects of obesity, it is important to acknowledge paradoxes in the human body that may converge to convey a benefit of obesity in sepsis survival. Whether for risk stratification, phenotype identification, or development of new treatments, understanding the complexities of the obesity paradox is of primary importance. The NINR (2016) explicitly cites research into symptom precursors, such as biologic indicators, as part of its strategic plan to determine symptom risk, disease severity, and disease duration. This focus reinforces the importance of biological research in nursing science to provide a strong foundation upon which to close knowledge gaps in patient care, such as those that have been identified in the obesity paradox.
Harnessing known biologic mechanisms is the basis of research that identifies possible new drug targets and classification of disease (Darden et al., 2018). Consideration of new ways to exploit biologic mechanisms is needed to advance patient care. Models that provide a basis for discovering causal factors of complex biologic diseases such as sepsis are needed to set forth a road map for systematic investigation of variables that affect disease outcomes.
Footnotes
Author Contributions
Jamie Robinson, Jeanne Salyer, and Terry Jones contributed to conception and design, acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; and gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy. Theresa Swift-Scanlan contributed to conception and design, acquisition, analysis, and interpretation; critically revised manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.