
Abstract
Background:
Trauma and management of injuries can result in reduction or loss of mobility, which can lead to skeletal muscle deconditioning and sustained disability. Prior investigators have examined changes in skeletal muscle due to injury and immobility separately. The muscular consequences of combined immobility and trauma have not been systematically investigated.
Objective:
The purpose of this study was to explore the association of time to first ambulation with skeletal muscle size and strength in patients after major trauma.
Methods:
Adults (N = 19) admitted for major trauma (Injury Severity Score [ISS] > 15) provided daily measures of muscle size (ultrasound) and strength (dynamometry) during hospitalization. Participants were grouped based on time to first ambulation. Repeated measures analysis of variance was used to compare muscle measures between the groups across 5 days while controlling for age and gender.
Results:
Participants were primarily male (63%) aged 40 ± 17 years with a mean ISS of 21 ± 4. Early ambulation was associated with a 10% increase from baseline in bicep size on Days 3 and 4 and a 15% increase from baseline on Day 5. There were no changes in rectus femoris size in either group. The early ambulation group was significantly stronger than the delayed ambulation group throughout the study in measures taken with the biceps (22%–37%) and quadriceps (26%–46%).
Conclusion:
Early ambulation following major trauma was associated with increased bicep size and greater muscle strength in the biceps and quadriceps muscles over time.
In the United States, trauma and unintentional injury is the leading cause of death for individuals aged 1–44 years and accounted for 5.4% of all deaths in 2015 (Centers for Disease Control and Prevention, 2016). From 2010 to 2015 the mortality rate for injured persons decreased from 2.72% to 2.63% (American College of Surgeons, 2011, 2016); however, the prevalence of trauma and unintentional injury increased by nearly 20% during the same period (American College of Surgeons, 2011, 2016). The combined direct and indirect cost of trauma in the United States is estimated to be approaching $700 billion. Nearly half (44%) of patients who survive their injuries have not returned to their pre-injury functional status at 12 months after injury (Davydow et al., 2009; World Health Organization, 2011). Thus, this population uses significant direct and indirect health care resources and exhibits long-term functional consequences. Systematic study to improve outcomes during and following hospitalization could provide substantial benefits for these patients.
Traumatic injuries and their management often result in reduction in or loss of mobility, which can lead to skeletal muscle deconditioning and degradation and, ultimately, sustained disability (Holtslag et al., 2007). Historically, health care providers prescribed periods of immobility to preserve energy and promote healing in injured individuals (Allen et al., 1999; Saunders, 2015). However, research has shown that the benefits of immobility are far outweighed by the negative consequences on multiple organ systems (Morris, 2007; Morris et al., 2011; Winkelman, 2009). Immobility reduces muscle strength by as much as 1.5% per day of bed rest (Saunders, 2015) and decreases cross-sectional muscle size by 2% over 7 days of strict immobility (Berg et al., 2007). Thus, immobility, even for a short period, can result in debilitating changes in skeletal muscle size and function.
Compounding the effects of immobility are the skeletal muscle changes associated with trauma (Hazeldine et al., 2014; Lord et al., 2014; Saunders, 2015; Vanzant et al., 2014). Scientists have estimated that the combination of immobility and traumatic injury decreases skeletal muscle strength by up to 28% (Paddon-Jones et al., 2006) and produces triple the loss of muscle mass compared to the effects of immobility alone (Ferrando et al., 1999; Paddon-Jones et al., 2006). The combination of trauma and immobility negatively affect outcomes including degree of disability and time to return to previous functional level (Davydow et al., 2009; Richmond et al., 2009, 2014). Prior investigators have assessed changes in skeletal muscle due to prolonged immobility and traumatic injury in separate investigations. A systematic investigation of the effects of the combination of immobility and trauma on skeletal muscle is needed for a comprehensive understanding of skeletal muscle responses after trauma.
The purpose of the present exploratory study was to examine the association of time to first ambulation with upper- and lower-extremity skeletal muscle size and strength in patients after major trauma. The specific aim was to compare five daily measures of skeletal muscle size using ultrasound of the biceps and rectus femoris muscles and of skeletal muscle strength using dynamometry of the biceps and quadriceps muscle while controlling for age and sex in two groups of adult patients hospitalized for major trauma: early (first ambulation achieved within 48 hr from admission) and delayed (first ambulation achieved after 48 hr from admission) ambulation.
Methods
We conducted this prospective, exploratory study at a single large, academic, Level I trauma center in the South Central United States. All patients admitted to the trauma service between April 2018 and August 2018 were screened for eligibility. We recruited 19 patients who met the following criteria for participation: 1) had a primary diagnosis of trauma with an Injury Severity Score (ISS) ≥ 15, indicating severe injury (Baker et al., 1974); 2) were 18 years of age or older; and 3) were able to read and write in English. Patients were excluded if they 1) had a diagnosis of unstable pelvic or spine fractures, spinal cord injury resulting in quadriplegia or paraplegia, or traumatic brain injury with inability to follow commands or communicate; 2) were determined to have terminal status; 3) had a written prescription for continued mobility restriction; 4) had a burn injury; 5) had been diagnosed with preexisting conditions that impaired mobility (e.g., neuromuscular diseases) or any other condition that could confound the effects of mobility status and skeletal muscle structure and function (Corneille et al., 2010; Grissom et al., 2010; Murray et al., 2017; Saunders, 2015).
Sociodemographic and Clinical Variables
We obtained sociodemographic and clinical variables from the electronic medical record and patient interview, including age; gender; race; body mass index; marital status; medical history including functional limitations, hypertension, chronic pain, and diabetes; type of trauma (blunt versus penetrating); ISS; admission to ICU; hospital and ICU length of stay; and discharge disposition (home versus other inpatient facility).
Time to First Ambulation
Our operational definition of mobility was a full gait cycle or full ambulation. A full gait cycle was conceptually defined as the exchange of energy from the initial contact of one foot to the progressive contact of the same foot in the same event, which met criteria for a score of 5 on the trauma unit’s mobility scorecard (Table 1; Shultz et al., 2005; Stryker, 2013; Taborri et al., 2016). We recorded the time to first ambulation in hours from admission. We categorized participants into one of two ambulation groups: early (within 48 hr of admission) or delayed (greater than 48 hr after admission) ambulation based on the trauma unit’s ambulation protocol (Table 1).
Trauma Service Early Mobility Protocol and Study Institution Mobility Scoring Instrument.
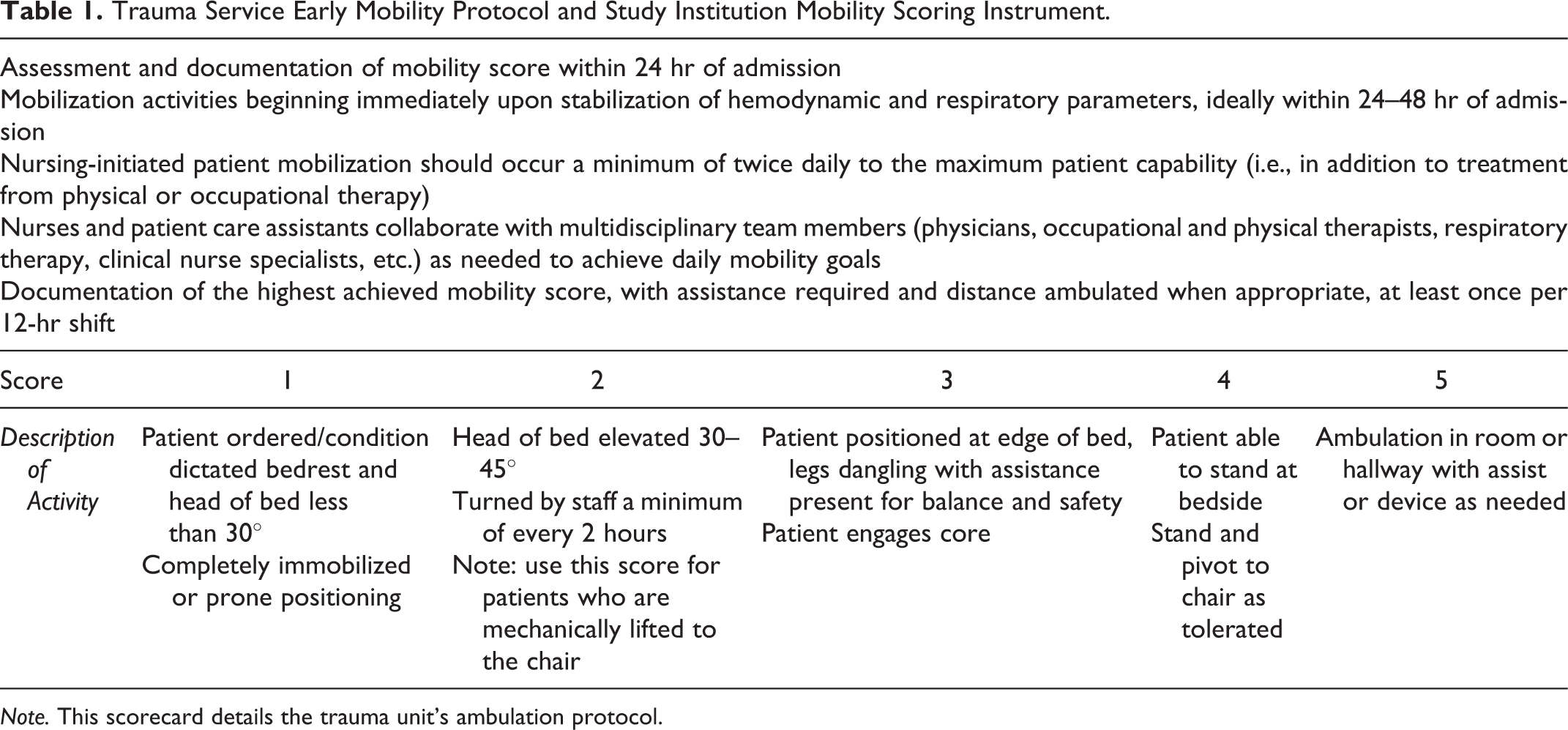
Note. This scorecard details the trauma unit’s ambulation protocol.
Muscle Size
We defined muscle size as the thickness, measured in centimeters, of the biceps brachii and rectus femoris muscles. Specifically, we identified the site for measurement of the biceps brachii muscle along the medial aspect of the upper arm, two-thirds the distance from the medial acromion of the scapula to the fossa cubit, with the arm abducted and the forearm extended at the elbow and supported on the adjustable bedside table (Jenkins et al., 2015). We identified the rectus femoris muscle along the anterior surface of the thigh, two-thirds distance from the anterior superior iliac spine to the superior patella border (Sanada et al., 2006). The measurement was the distance from the adipose–muscle interface to the muscle–bone interface for the biceps brachii and to the muscle–muscle interface for the rectus femoris (Figure 1; Sanada et al., 2006; Toda et al., 2016). We selected the biceps brachii and rectus femoris because of their roles in mobility, specifically the gait cycle (Annaswamy et al., 1999; Dietz et al., 2001).
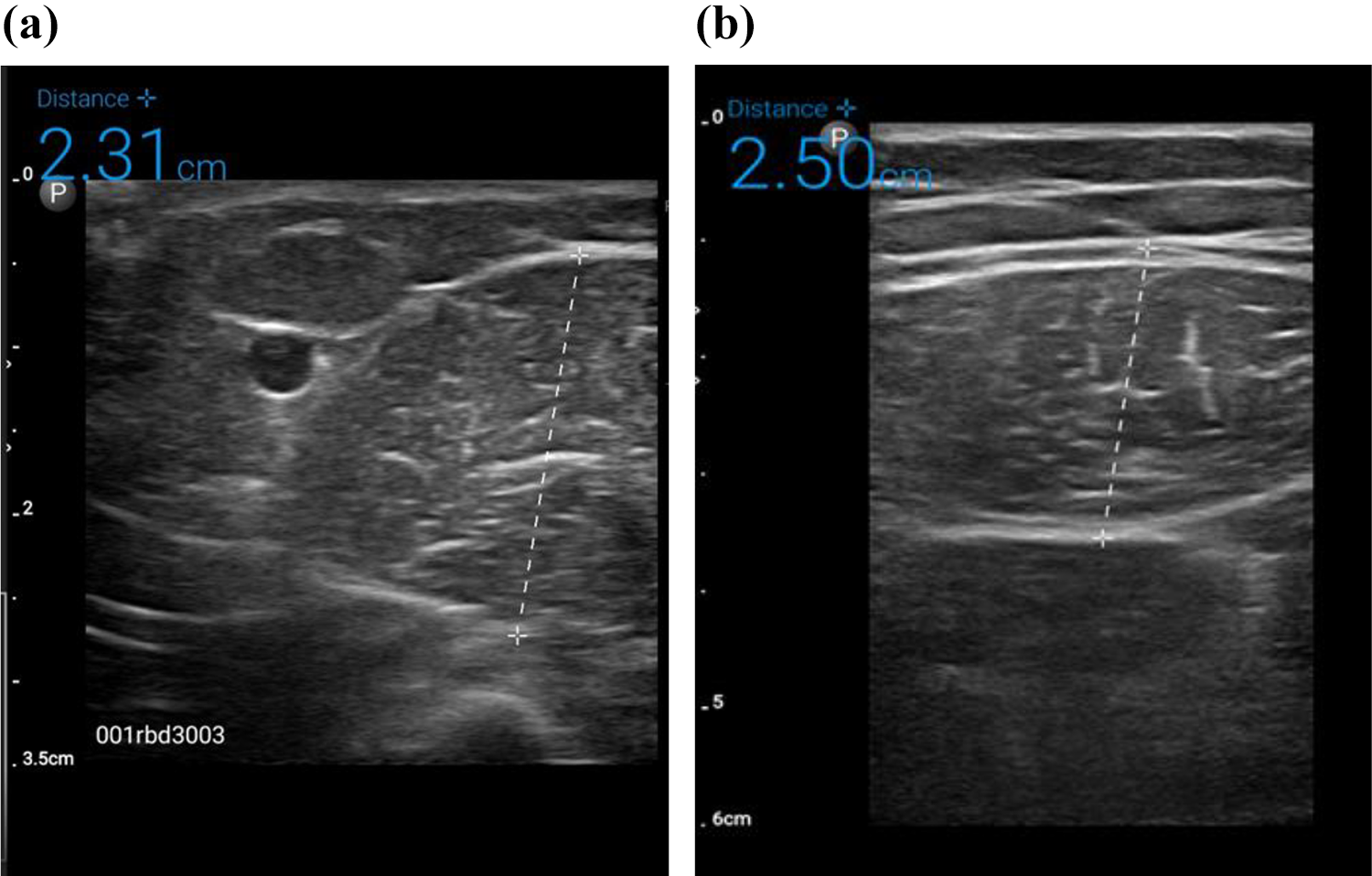
Measurement of muscle size using a portable Doppler ultrasound. (a) Measurement of the thickness of the biceps brachii was defined as the distance from the adipose–muscle interface to the muscle–bone interface, as indicated by the dotted line between each +. (b) Measurement of the thickness of the rectus femoris was defined as the distance from the adipose–muscle interface to the muscle–muscle interface, as indicated by the dotted line between each +.
To measure muscle size in the present study we used ultrasonography, a valid and highly reliable measurement that has been widely used to measure muscle size in prior studies (Jenkins et al., 2015; Nozoe et al., 2016; Reeves et al., 2004; Sanada et al., 2006). In comparison to the gold standard, magnetic resonance imaging, ultrasound-based measures of quadriceps muscle size demonstrated excellent correlation, low coefficient of variation, and good visual agreement on Bland–Altman plots (Reeves et al., 2004; Scott et al., 2012; Worsley et al., 2014). The PI (JTH) participated in an intensive, 10-hr training program in ultrasonography provided by a qualified emergency medicine physician with fellowship training in ultrasonography (JA). Prior scientists demonstrated that novice ultrasound examiners achieved accurate and precise recordings and assessment of images following training from an expert in ultrasonography (Dudley-Javoroski et al., 2010; Teyhen & Koppenhaver, 2011). The expert trainer for the present study also provided secondary ratings for 10% of collected images for assessment of interrater reliability, which we determined to be acceptable (interclass correlation coefficient [ICC]: 0.856).
Muscle Strength
We defined muscle strength as the peak isometric force a muscle exerted against resistance in pounds (Gittings et al., 2016; Milner-Brown & Miller, 1988). We measured strength of the biceps and quadriceps daily as the average of three separate dynamometry (Commander Muscle Tester, JTECH Medical, UT, USA) measures taken 5 min apart. Previous authors described the landmarking for dynamometry measure of the biceps and quadriceps, and we followed those guidelines for the present study (Gittings et al., 2016). We used the dominant-side muscle for all measures when available.
Investigators previously demonstrated adequate reliability and validity of dynamometers to measure muscle strength in the clinical setting (Gittings et al., 2016; Mentiplay et al., 2015). Concurrent validity analysis supported good relationships (ICC ≥ 0.70) between handheld dynamometry and the gold standard for strength measurement, fixed dynamometry, when analyzing peak force generation among muscle groups tested (Mentiplay et al., 2015). The PI (JTH) participated in an intensive 5-hr training program provided by a doctorally prepared physical therapist in the use of handheld dynamometry with this population.
Procedure
We received Institutional Review Board approval for this study following full review. Each day, all patients admitted to the trauma service were evaluated for study inclusion. We approached those who met inclusion criteria for study participation. To determine ability to provide consent we used the University of California, San Diego, Brief Assessment of Capacity to Consent instrument (Jeste et al., 2007). We obtained informed consent from participants deemed capable of providing informed consent. We measured muscle size then strength at the bedside as follows.
We measured muscle size with a portable, color Doppler, 34 mm. aperture, M-mode, high resolution, broadband linear array transducer (Philips Lumify L12-4, Amsterdam, Holland). We identified the sites of muscle-size measurement using specific landmarks, as previously described, marked them with an indelible pen, and covered them with a waterproof, transparent dressing to ensure daily consistency of measures (Reeves et al., 2004). We took three separate ultrasound images daily, screen captured the images, and used built-in calipers to determine thickness, recording the average of the three measures as the daily measure.
After completion of muscle-size measures, we seated participants on the edge of the bed with their feet dangling (Gittings et al., 2016). If a participant could not tolerate sitting on the edge of the bed, we placed them in a high Fowler’s position for strength testing of the biceps and a dorsal recumbent position for strength testing of the quadriceps (Baldwin et al., 2013). The PI positioned the dynamometer and applied gentle pressure against the skin. We instructed the participant to exert force against the resistance of the PI as if attempting to extend the leg into a straight line or to touch the unilateral shoulder in a linear fashion with as much effort as possible without causing pain. We determined the peak isometric contraction in pounds of force achieved across three separate measures taken 5 min apart and recorded the mean value of the three tests as the daily muscle strength measure.
Data Analysis
We entered all data into an electronic spreadsheet and transferred them to IBM SPSS Statistics for Mac, Version 24.0 (IBM, Armonk, NY) and SAS for Windows, Version 9.3 (SAS Institute, Inc., Cary, NC) for analyses. Descriptive statistics including means (standard deviations) and frequencies (percent) were used to characterize the sample. Patients were categorized as early (within 48 hr after admission) or delayed (after 48 hr after admission) ambulation based on the time of first ambulation after admission. We compared sociodemographic and clinical variables for these two groups using independent t-tests and Chi-square or Fisher’s exact statistics based on the level of measurement.
To address our specific aim, we used mixed modeling for repeated measures. Fixed effects included ambulation group (early or delayed) and time (study day) as well as the group-by-time interaction. Fisher’s least significant difference procedure for post-hoc comparisons identified the significant pairwise differences in main or interaction effects. Because the mean length of stay across the sample was 5.6 ± 3.2 days, analyses were conducted using the first 5 days of measurements (baseline/Day 1, Day 2, Day 3, Day 4, and Day 5). This analysis strategy was appropriate for our repeated-measures design and allowed for retention of all patient data in the model (Littell et al., 2006). As a correction for multiple comparisons, a conservative alpha level of .01 was used throughout.
Results
Participant Characteristics
Participants were primarily male (63%) and Caucasian (68%), with a mean age of 40 ± 17 years (range 19–69 years; Table 2). Most participants had experienced blunt trauma (84%), and the average ISS was 21 ± 4. All patients survived their injuries, the average ICU length of stay was 1.4 ± 2.1 days, and the average hospital length of stay was 5.6 ± 3.2 days. The average time to first ambulation was 59 ± 50 hr (2.5 days). Nearly three-fourths (74%) of participants were discharged home. We categorized 10 participants (53%) as early ambulators and 9 as delayed ambulators (47%). There were no differences in sociodemographic or clinical variables between these two groups (Table 2).
Characteristics of the Sample by Time to Ambulation.
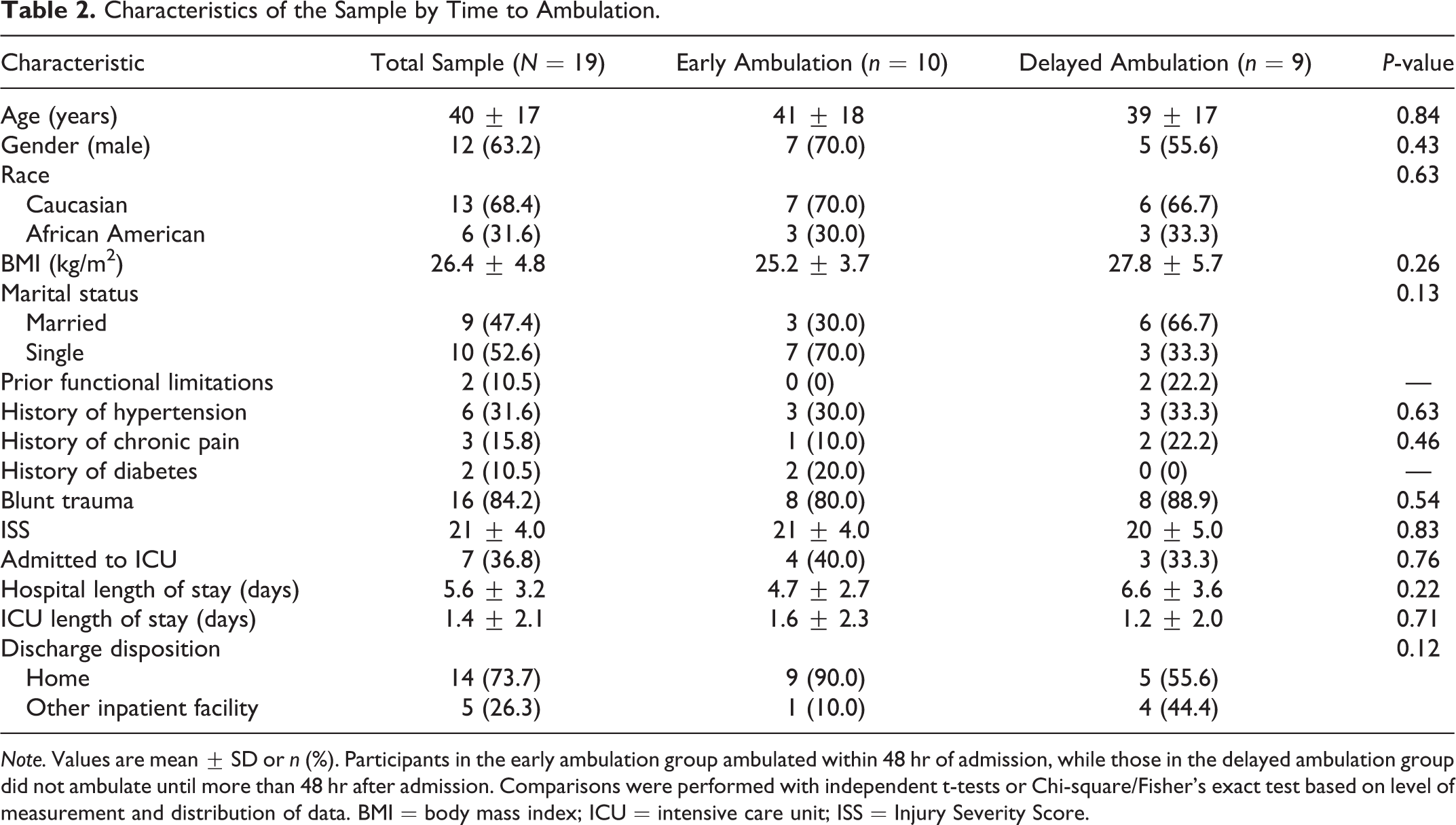
Note. Values are mean ± SD or n (%). Participants in the early ambulation group ambulated within 48 hr of admission, while those in the delayed ambulation group did not ambulate until more than 48 hr after admission. Comparisons were performed with independent t-tests or Chi-square/Fisher’s exact test based on level of measurement and distribution of data. BMI = body mass index; ICU = intensive care unit; ISS = Injury Severity Score.
Muscle Size
We report comparison of the sizes of the biceps brachii and rectus femoris muscles between groups by mixed modeling for repeated measures in Table 3. The assumptions of the mixed-model procedure were met. For biceps size, the interaction term group-by-day was significant (F[4, 47], 3.68, p = 0.01). There were no differences in biceps size between groups; however, post-hoc analysis determined that in the early ambulation group there was significant increase in biceps size from Day 1 to Days 3, 4, and 5 (Table 3). There were no differences between or within groups over 5 days of measurement for the rectus femoris muscle.
Muscle Size and Strength.
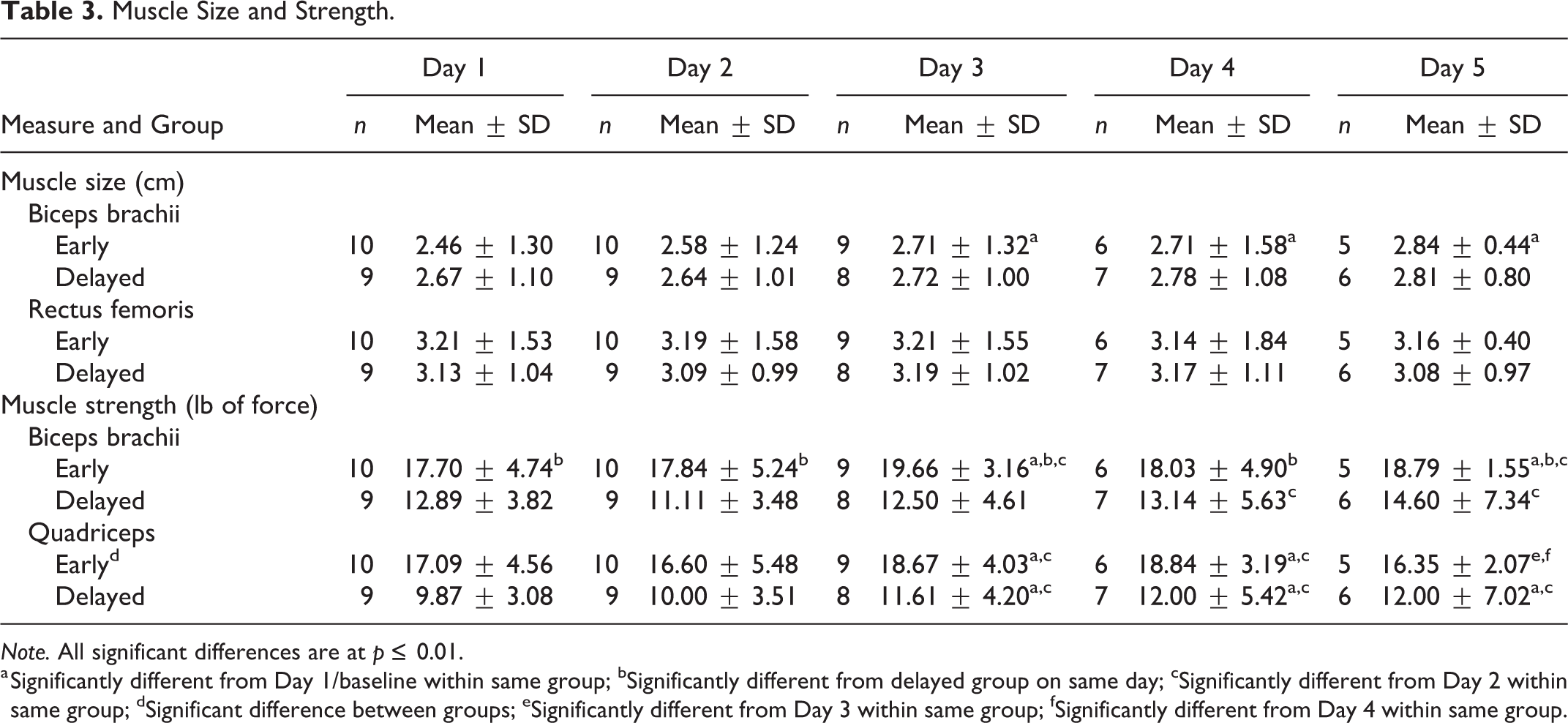
Note. All significant differences are at p ≤ 0.01.
a Significantly different from Day 1/baseline within same group; bSignificantly different from delayed group on same day; cSignificantly different from Day 2 within same group; dSignificant difference between groups; eSignificantly different from Day 3 within same group; fSignificantly different from Day 4 within same group.
Muscle Strength
We also report comparison of the strength of the biceps brachii and quadriceps muscles between groups by mixed modeling for repeated measures in Table 3. The assumptions of the mixed-model procedure were met. Participants in the early group had significantly more strength in both the biceps and quadriceps at baseline and throughout the study. The interaction term of group-by-day was significant for biceps strength (F[4, 47], 3.66, p = 0.01). Participants in the early group had significantly increased biceps strength on Days 3 and 5 compared to Days 1 and 2. In the delayed group, participants had significantly increased strength on Days 4 and 5 compared to Day 2.
The main effects of group (F[1, 13], 19.55, p = 0.0007) and day (F[4, 47], 5.68, p = 0.0008) were significant for quadriceps strength; however, the interaction of group by day was not (p = 0.69). On average, the participants in the early ambulation group were 6.2 pounds of force stronger compared with the delayed group (p = 0. 0007). On Days 3 and 4, participants in the early group were nearly 2 pounds of force stronger compared to Day 1 measures and more than 2 pounds of force stronger compared to Day 2 measures. This group displayed a significant loss of strength on Day 5 compared with Days 3 and 4. In the delayed ambulation group, participants displayed increased strength on Days 3, 4, and 5 compared to Days 1 and 2 (Table 3.).
Discussion
We evaluated the association between time to first ambulation and skeletal muscle size and strength in patients after major injury. Although this was a small exploratory study, our preliminary results demonstrate that there are associations between time to ambulation and skeletal muscle measures in patients who are hospitalized following traumatic injury. Our findings suggest that promotion and engagement of early ambulation in this population might mitigate acquired muscular changes.
Our finding that bicep size increased from baseline to Day 3 and later in the early-ambulation group contrasts with that of Mulder and colleagues (2015), who reported that 5 days of bed rest with a daily 25 min out-of-bed activity only maintained muscle size. Other investigators who implemented prescribed, short, out-of-bed exercise regimens during bed rest found that engagement in activity reduced the loss of muscle compared to bed rest alone (Krainski et al., 2014; Trappe et al., 2007). Comparison between our findings and those of prior investigators is precluded due to the difference in samples: these prior investigators evaluated skeletal-muscle response in young, healthy volunteers, thus limiting the comparison of findings. One possible explanation for the increase in biceps size of participants in the present study might be activity prior to first ambulation. However, neither we nor prior investigators measured the level and frequency of all activity, both in and out of bed, so we cannot confirm this proposition (Krainski et al., 2014; Mulder et al., 2015; Trappe et al., 2007). Taken together, findings in the present study and those of prior investigations suggest that activity, particularly ambulation, may mitigate muscle loss and, in some cases, increase muscle size in patients prescribed bed rest Subsequent studies among trauma patients, however, should include measures of all activities, such as wearable activity trackers, to both in-bed and out-of-bed activity and determine their influence on skeletal-muscle maintenance after injury (Leaf Healthcare, 2018).
In contrast to our finding of no loss in muscle size in the rectus femoris, prior investigators reported a 9% reduction in the cross-sectional area of the rectus femoris in critically ill patients as early as 72 hr after ICU admission and a 3-fold loss after 10 days in the ICU (Parry et al., 2015; Puthucheary et al., 2013). Direct comparisons between the present study and these prior studies is not possible as participants in the present study were, on average, 16 years younger and had a lower severity of illness than those in the prior studies and were also not on strict bed rest; meanwhile, most participants in the prior studies had not experienced traumatic injury (Parry et al., 2015). A potential explanation for maintenance of rectus femoris size in the present study may have been, at least in part, our exclusion criteria, which may have led to our participants maintaining a greater degree of activity while on bed rest than those in prior studies. Further investigation of how differing levels of activity after trauma can influence muscle size is warranted.
Participants in the early ambulation group in the present study were significantly stronger at baseline and demonstrated greater strength across the 5 days of the study compared with those who ambulated later. Previous investigators determined that there was a predictive relationship between baseline handgrip strength and time to return to ambulation in hospitalized older adults (Savino et al., 2013). Savino and colleagues also found that geriatric patients who experienced hip fracture and were in the highest tertile of grip strength at baseline had a nearly 3-fold increase in likelihood of walking after surgery compared to those in the lower tertiles. Thus, our finding that participants with greater baseline strength ambulated earlier than those with less baseline strength is consistent with prior research findings across multiple age groups, suggesting that pre-injury functional capacity might influence the trajectory of in-hospital ambulation.
Patients in the early group demonstrated peak strength between Days 3 and 4, and those in the delayed group peaked on Days 4 and 5. However, those in the early group had a significant reduction in quadriceps strength on Day 5. This finding could be due to the volitional nature of the measure or, more likely, to the discharge of stronger patients prior to Day 5 measures. It is also possible that, because those in the delayed group were weaker at baseline they had greater room for improvement in strength. The improvement in strength in the delayed group could also be related to resolution of confounding clinical variables such as achievement of pain control.
The ability of skeletal muscle to sustain damage, such as injury or disuse atrophy, but preserve strength can be explained by its modular structure (Schiaffino, 2017). Skeletal muscle fibers are long, multinucleated cells with the contractile units organized into myofibrils further arranged into units called sarcomeres; a single muscle fiber can contain millions of sarcomeres. This structure allows normal contractile units to compensate for damaged units nearby (Schiaffino, 2017). The theory of the myonuclear domain also proposes that the myonucleus directs an area of nearby cytoplasm and regulates the protein turnover to support the domain. Thus, when myonuclei are damaged they are removed, primarily by apoptosis, resulting in muscle atrophy (Brooks & Myburgh, 2014). However, Zhong and colleagues found that during disuse the removal of myonuclei resulted, not in atrophy, but in a change in fiber type; thus, the unit retained size and contractile ability (Zhong et al., 2005). This theory may explain, at least in part, the lack of significant reduction in muscle size and the preservation of strength in both groups in the present investigation. Further investigation is required to provide a more comprehensive understanding of the complex interaction of the effects of traumatic injury and subsequent immobilization as it relates to skeletal-muscle size and strength. Such knowledge could lead to improved treatments and interventions related to physical rehabilitation for patients after trauma.
Limitations
We conducted the present study in a single center with a small, homogeneous sample that may not represent the trauma population as a whole. The small sample may also have led to a lack of statistical power to identify additional differences between the early- and delayed-ambulation groups. We did not capture other variables that can affect ambulation, including medications received and pain levels. Additionally, we did not account for mobility activities performed during bed rest or between nurse mobilization sessions (including physical/occupational therapy), pre-injury functional level, or nutritional status, which may have affected muscle size and strength. Collection of these variables would have helped provide a more complete explanation of our results. Other measures that may be a better indicator of muscle size require specialized computer software and conversion algorithms that were not available for this investigation. Regardless, our measures were sufficient to identify group differences. Lastly, dynamometry is a volitional measure that requires exertion of maximal effort by the participant. Although we caclulated the mean of three measures for analysis, degree of patient effort cannot be controlled.
Implications
The findings in the present investigation provide additional evidence of the benefits of early ambulation in preserving muscle size and strength. Further, they suggest that assessment of strength on admission for traumatic injury might identify patients at highest risk for delayed ambulation. Routinely measuring strength on admission would allow for care planning based on this measure to promote earlier ambulation. Implementing early and sequential documentation of strength could thus guide the creation of a more personalized plan of care that optimizes physical recovery following hospitalization for traumatic injury.
Conclusions
The present study is among the first to collect sequential measures of muscle size in patients admitted for traumatic injury. We found that ambulation within 48 hr of admission for major trauma was associated with increased bicep size and greater muscle strength in the biceps and quadriceps muscles over time. Participants who ambulated earlier also exhibited greater muscle strength at all time points compared with those who ambulated later. Preservation of skeletal-muscle size and strength during hospitalization after injury is vital for reducing short- and long-term disability. Additional research is needed to provide further evidence regarding the relationships among traumatic injury, time to ambulation, and muscle size and strength in order to develop interventions to reduce long-term disability after trauma.
Footnotes
Authors’ Note
An earlier version of this manuscript was included as a chapter in a dissertation at the University of Kentucky entitled “Association of Skeletal Muscle and Psychological Responses to Immobility After Major Injury.”
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Robert Wood Johnson Foundation, Future of Nursing Scholars Program (RWJF Grant ID# 72586, PI: T. Lennie, Scholar: J. Higgins).