
Abstract
Interleukin 6 (IL-6) and its receptors are expressed in approximately half of breast cancer (BC) tissues, and high serum IL-6 levels are associated with poor prognosis. African American (AA) patients with BC have higher serum IL-6 levels compared to Caucasians, suggesting additional risk of disease-related complications in AAs. The purpose of this study was to compare IL-6 complex biomarkers in AA women with and without a history of BC. We conducted a secondary analysis of phenotypic data from two studies of weight loss in AA women with and without a history of BC who had similar age and adiposity. Biomarkers analyzed included tumor necrosis factor alpha (TNF-α), IL-6, IL-6 soluble receptor (IL6sr), and soluble glycoprotein 130 (GP130); IL6sr and GP130 were newly analyzed for this study. TNF-α levels were 1.86 times higher in the BC group (N = 7) compared to those without BC (N = 10; p < 0.001) despite similar age, weight, and body mass index. GP130 levels tended to be higher in women with BC; IL-6 and Il-6 sr were not different between groups. There was a strong correlation between GP130 and TNF-α (r = .638; p = .006) in the group overall. High TNF-α levels in the BC group and a strong correlation between GP130 and TNF-α in the overall group suggest the presence of IL-6 complex initiated TNF-α production. Further study is needed to evaluate IL-6 reduction through a variety of approaches, including weight loss and anti-IL-6 therapies, which may ultimately implicate the reduction of IL-6 complex associated BC-specific recurrence and mortality.
Interleukin 6 (IL-6) and its receptors are expressed in approximately half of breast cancer (BC) tissues (Garcia-Tuñón et al., 2005), and high serum IL-6 levels are associated with poor prognosis (Zhang & Adachi, 1999). IL-6 is a pleiotropic pro-inflammatory cytokine that stimulates a variety of target cells through a membrane-bound receptor comprised of two subunits: soluble interleukin-6 receptor (IL6sr) and the signaling soluble glycoprotein 130 (GP130; Scheller et al., 2011). IL-6 binds to IL6sr and then recruits GP130 to form the IL-6/IL-6R/GP130 complex. Receptor activation induces Jak/Stat3 signaling pathway, which plays a major role in growth and metastasis of BC cell lines (Leslie et al., 2010).
African American (AA) patients with BC have higher serum IL-6 levels compared to Caucasians (Deshmukh et al., 2015), suggesting an additional risk of disease-related complications in this population. Increased body fat in BC is associated with greater inflammation, which is believed to accelerate cancer cell proliferation, cancer progression, and result in shorter survival (Pakiz et al., 2011). Both IL-6 and TNF-α, another pro-inflammatory cytokine, are secreted by adipocytes, and their concentrations are positively correlated with percentage and distribution of fat tissue in the body (Rodríguez et al., 2015).
Given the associations between high IL-6 levels and increased risk for poor BC outcomes in AA women who are also overweight and obese, we aimed to compare IL-6, IL6sr, and GP130 levels as well as TNF-α, in AA women with and without history of BC and similar adiposity. We hypothesized a strong association between all three biomarkers in the two groups and higher mean levels of the biomarkers in women with a history of BC. IL-6 has been implicated in drug resistance of BC stem cells; thus anti-IL-6/IL-6R/GP130 therapies hold promise for the treatment of BC.
Methods
We analyzed baseline data from two clinical studies which investigated the effects of weight loss in post-menopausal (amenorrheic
Subgroups from each of the primary studies were selected. From the study of women with a BC history, cases were selected based on availability of samples for additional biomarker analysis; from the larger sample of women without a history of BC, cases were selected randomly from age and BMI matched cases. In the original studies, all women underwent fasting blood draws and plasma was frozen at −80 °C. We selected from the first study of women with a BC history, cases with samples available for analysis; we then selected women without BC from the second study who were of similar BMI and age and also had samples available for the new experiments. BMI and age similar cases in both groups allowed control of covariation of inflammation with adiposity. Additional biomarkers analyzed for the purpose of this analysis included IL6sr and GP130. Membrane-bound IL6sr and GP130 are also expressed in the plasma and therefore amenable to examination for this research. IL-6, IL6sr, and GP130 assays were measured in duplicate by ELISA (Novus Human IL6sr and R&D System Quantikine ELISA, respectively) and TNF-α as previously described (Griffith et al., 2016). Descriptive analyses included means, standard deviations and ranges for continuous variables and proportions for categorical variables. Mean values for each measure were compared between the BC group and non-BC group using independent t-tests. Pearson product-moment correlation coefficients were computed to assess the relationships between GP130 and IL6sr and TNF-α. SPSS© version 26 was used for statistical analysis (IBM Corp, Armonk, NY).
Results
All participants (N = 17) self-identified as AA or Black, and no differences between groups were noted on mean values for age, weight, or BMI, where both groups had class 1 obesity (Table 1). Among women with a history of BC, all were at least two years post diagnosis (range 2–12 years). Other BC-specific characteristics are described in Table 1. TNF-α values were different between groups, with the BC group nearly twice that of non-BC (p < .001). No other differences between groups were found. Mean (SD) GP130 values were 294.5 (35.4) ng/mL in the BC group compared to 255.9 (61.0) ng/mL in those without a BC history. Although the difference between groups was not significant, there was a trend toward higher mean GP130 levels in women with BC as well as less variability at the individual levels (p = 0.12), as shown in Figure 1. GP130 was associated with IL6sr (r = .49; p = .05) in the group overall (Figure 2A). There was also a strong correlation between GP130 and TNF-α, r = .638; p = .006 in the group overall (Figure 2B).
Participant Characteristics According to Breast Cancer History.
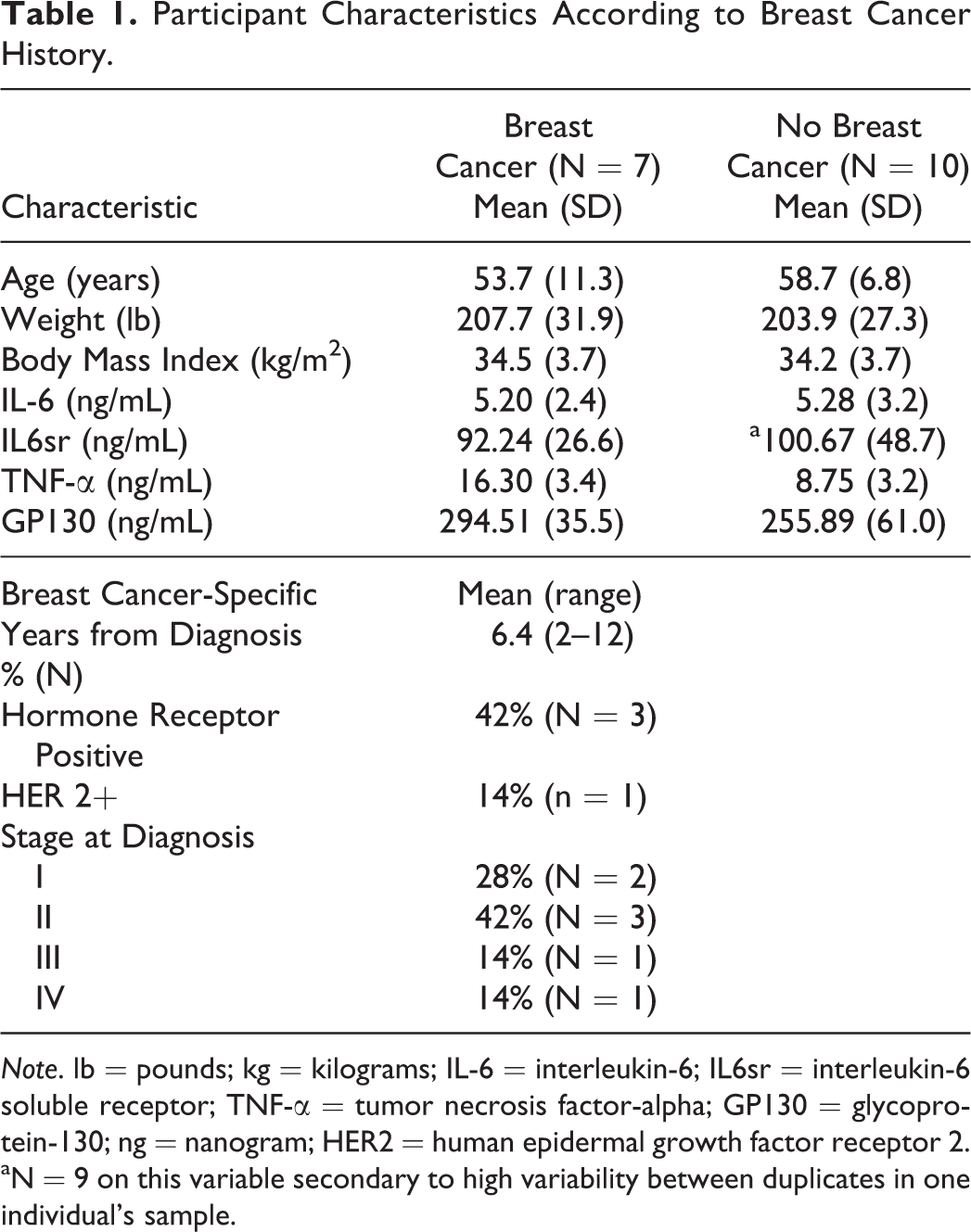
Note. lb = pounds; kg = kilograms; IL-6 = interleukin-6; IL6sr = interleukin-6 soluble receptor; TNF-α = tumor necrosis factor-alpha; GP130 = glycoprotein-130; ng = nanogram; HER2 = human epidermal growth factor receptor 2.
aN = 9 on this variable secondary to high variability between duplicates in one individual’s sample.
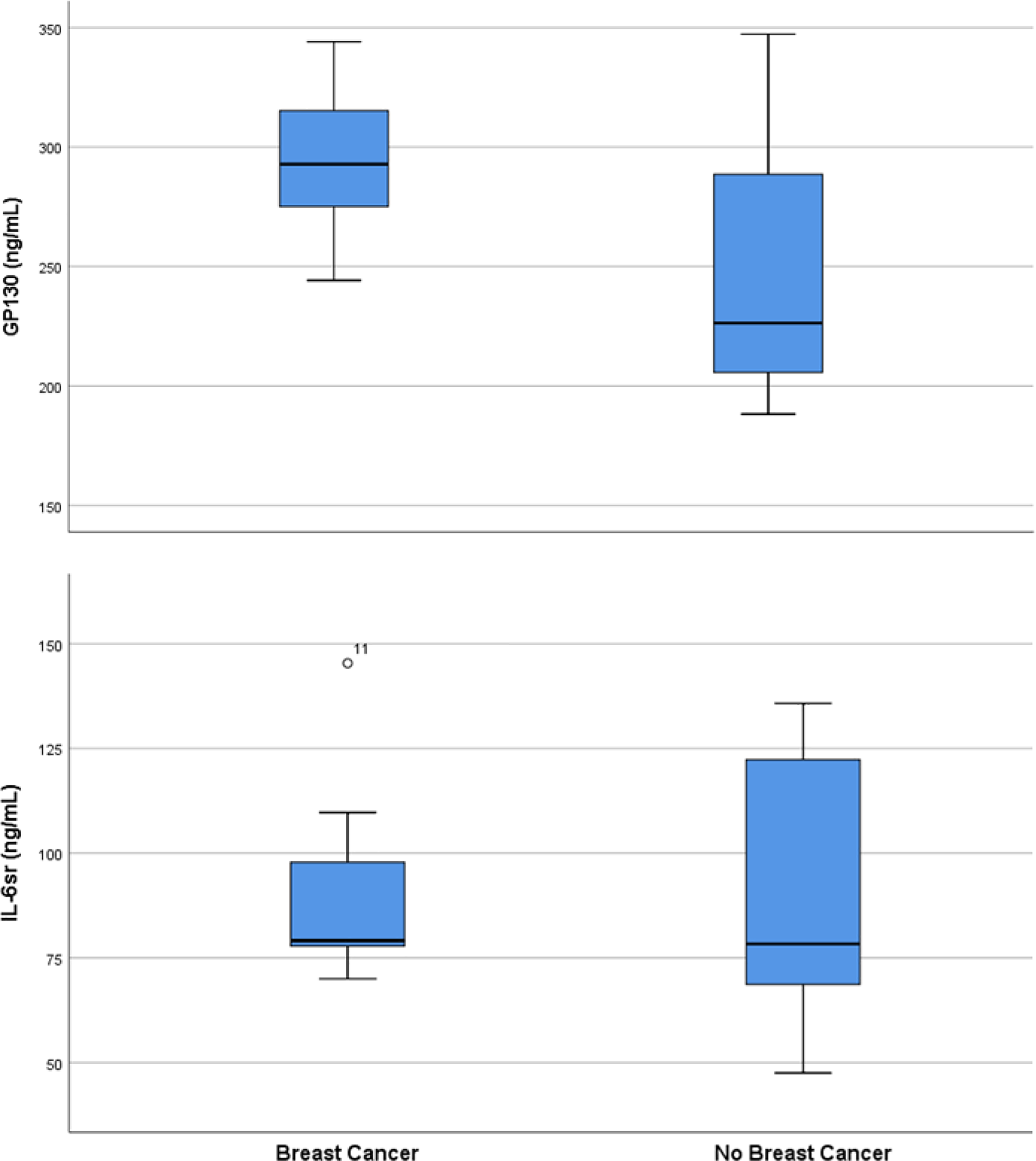
Distribution of IL6sr and GP130 values in women with and without a history of breast cancer.
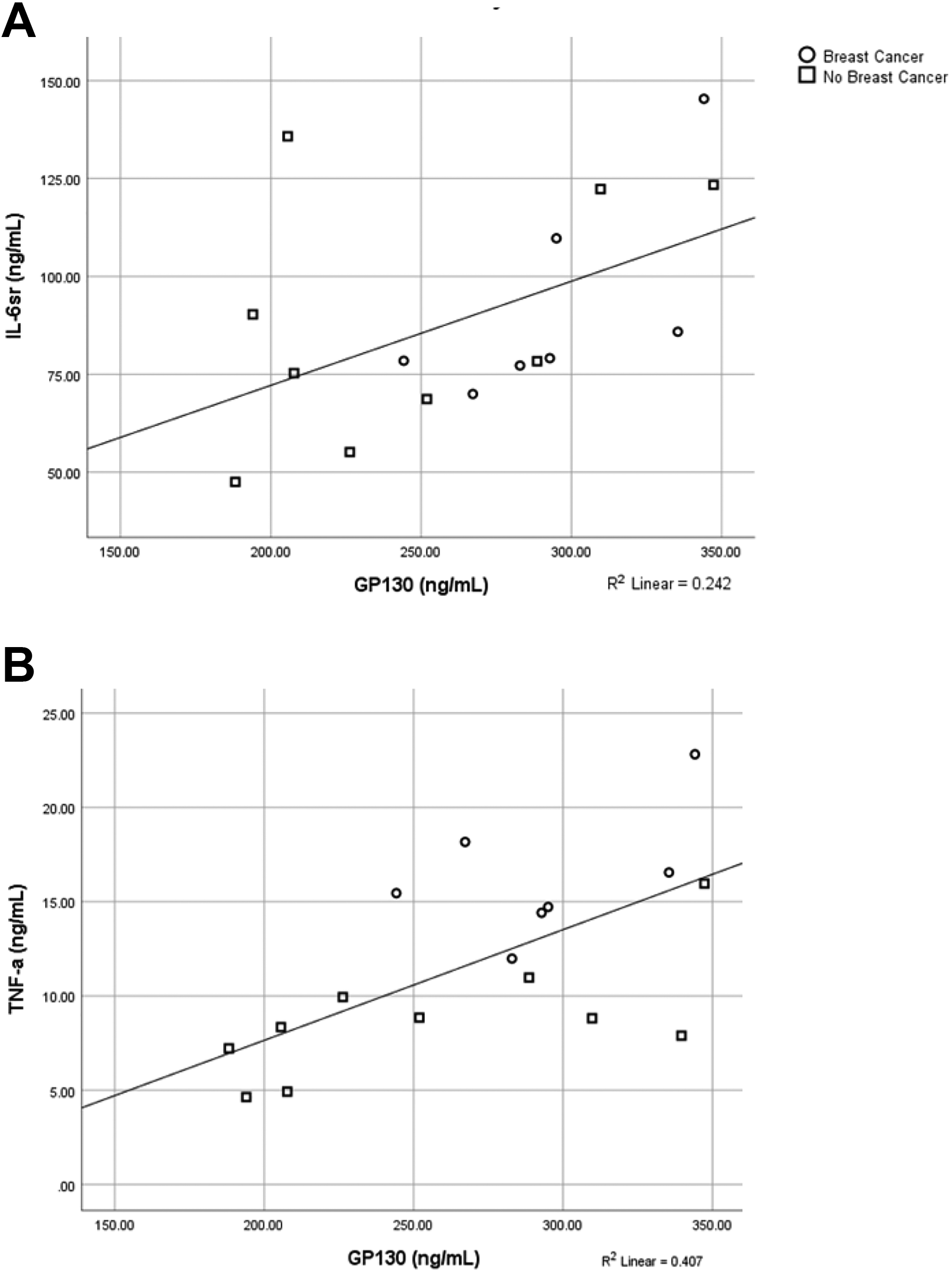
(A) Relationship between GP130 and IL6sr. (B) Relationship between GP130 and TNF-α.
Discussion
IL-6 and its soluble receptors are of particular interest to evaluate in the setting of BC because IL-6 is commonly found in BC tissue; furthermore, IL-6 levels are relatively higher in African Americans compared to Caucasians and positively associated with both percentage of body fat and BC-related complications. Comparison of the IL-6 complex in a sample of overweight and obese African American subjects with and without a BC history provided an opportunity to discern not only how individual IL-6 complex components differ between groups but also how they are related to TNF-α. We included TNF-α in our analysis because TNF-α and IL-6 are drivers of acute phase protein production initiation, which results in inflammation. In the setting of obesity, white adipose tissue includes a large number of inflammatory molecules, including TNF-α and IL-6, which may have systemic effects on a number of physiologic processes. Our sample of BMI similar groups allowed us to compare inflammation between them while mitigating the influence of obesity on IL-6 and TNF-α levels. Our results indicate significantly higher TNF-α levels in the BC group and a strong correlation between GP130 and TNF-α, suggesting the presence of IL-6 initiated TNF-α production. Thus, higher TNF-α values in the BC group may have been driven by increased activity of the IL-6 complex.
The direct effect of IL-6 on estrogen receptor positive/progesterone receptor positive (ER/PR+) BC cell growth is not well understood, with some findings demonstrating inhibitory effects on BC cell growth and proliferation (Badache & Hynes, 2001) and others documenting BC cell growth promoting effects (Jiang et al., 2011). ER/PR- cell types have received less attention, but to date IL-6 has been found to have no effect on ER/PR- BC proliferation (Johnston et al., 1992). Current interpretation of the data indicates that the effect of IL-6 depends upon the activation of the Jak/Stat3 pathway. IL-6 is a principal activator of Stat3 in BC cell lines (Liao et al., 2011); Stat3 is active in at least half of BC, and therefore inhibition of IL-6/Jak/Stat3 signaling presents an important opportunity to interrupt tumorigenesis.
GP130 levels, although not significantly different between BC history groups, tended to be higher in the BC group. Soluble GP130 inhibits IL-6 responses that rely on IL6sr (Jostock et al., 2001) and thus has therapeutic potential through blocking the IL6sr transsignaling response (Heo et al., 2016). Promising work in mice using a small-molecule target that binds directly with GP130 reduced the IL-6/IL6sr complex as well as IL-6-induced TNF-α production in addition to pancreatitis-associated inflammation (Hong et al., 2015). Currently, several GP130 targeting agents are under consideration for human testing in BC prevention and treatment (Heo et al., 2016).
Raloxifene, a selective ER modulator (SERM), reduces risk of BC in women at risk for estrogen receptor positive BC (Barrett-Connor et al., 2006) through its blocking of estrogen’s effect on breast tissue. Reduced expression of both IL-6 by 50% and TNF-α by 30% was observed in post-menopausal women after 6 months of raloxifine treatment (Gianni et al., 2004), demonstrating its ability to modulate circulating cytokine levels. More recently, raloxifene demonstrated inhibition of the interaction between IL-6 and GP130 (Li et al., 2014), suggesting a potential for raloxifine and other SERMS to reduce the IL-6/GP130/STAT3 cancer signaling pathway that is implicated in progression of several cancer types, including breast cancer (Deng et al., 2007).
Our work demonstrates a trend of higher GP130 levels in African American women with BC compared to those without a BC history, which underscores the need for continued investigation of pharmacological inhibition of GP130, the common signaling subunit of receptors used in the IL-6 cytokine complex. The possibility of survival bias is present in all studies of cancer survivors and represents a loss of key data which could threaten accuracy of findings. Yet, there was a wide range of time from diagnosis in our study participants that reduces potential survival bias. Systematic recruitment of survivors across specific times from diagnosis in future, larger studies will allow inclusion of this potential confounder in multivariable models and reduce survival bias. Our study limitations of small sample size, lack of direct measures of body fat, limited scope of inflammatory markers, are balanced by novel findings in this group of obese women. Mechanistic studies of weight loss designed to evaluate IL-6 complex changes in overweight and obese African American women with a BC history would provide further insight; effective reduction of IL-6 complex components may result in reduced BC-specific recurrence and mortality. Other studies of the effect of IL-6 targeting agents on BC are also indicated in this understudied population, given the growing evidence of correspondence between IL-6 levels and promotion of ER/PR+ BC.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Griffith—KCA126849A NCI-Greenebaum Cancer Center K12; Ryan—VA RR&D Senior Research Career Scientist, National Institutes of Health RO1-AG-19310, P30-AG-028747 and P30-DK-072488, Baltimore Veterans Affairs Medical Research Service, and Baltimore Geriatrics Research Education and Clinical Center (GRECC).
Statement of Data Availability
Data are available upon reasonable written request.