
Abstract
Objective
There is some controversy about the beneficial effects of occupational physical activity (OPA) on cardiovascular risk (CVR)
Methods
This cross-sectional study included data from 2516 couriers living in Spain, delivering either by motorbike or foot, and practicing LTPA never, occasionally, or regularly. Couriers were classified into six categories according to LTPA and OPA; body composition was assessed by Bioelectrical Impedance, and CVR by the Framingham equation. General linear models were performed to explore the association between different categories with each outcome (CVR and body composition) and the possible role of VAT as a mediator between PA and CVR.
Results
Compared with the most sedentary group (motorbike couriers that never practice PA), walking couriers who practice regular PA presented the lowest CVR [β −1.58 (95% CI −2.31; −0.85)] and the lowest VAT [β −2.86 (95% CI −3.74; −1.98) followed by the motorbike couriers who practiced regular PA [β −0.51 (95% CI −1.00; −0.03) for CVR and β −2.33 (95% CI −2.91; −1.75) for VAT]. The association between PA and CVR was partially mediated by VAT.
Conclusion
The present results indicated that both OPA and LTPA are protective factors for CVR and play an important role on VAT accumulation.
Keywords
Introduction
Regular physical activity (PA) has significant health benefits linked with the reduction of cardiovascular disease (CVD) and mortality (Kraus et al., 2019; Zhao et al., 2020) along with the amelioration of a variety of other chronic conditions (Colberg et al., 2016). The potential health effect of PA may depend on the domain (Hall et al., 2019; Wanner et al., 2019) and frequency (Södergren et al., 2008). Regular leisure-time physical activity (LTPA), which includes sports and all forms of aerobic and resistance-training exercises performed during free time (Howley, 2001), has been shown to significantly improve cardiovascular health (Lin et al., 2015; Piercy et al., 2018). In addition, occasional LTPA, has also shown some beneficial effects (O’Donovan et al., 2017). However, there is some controversy about the effect of different intensities of occupational physical activity (OPA), which relates to the PA performed as part of a job during working hours (Howley, 2001), on cardiovascular risk (CVR; Hu et al., 2007), as well as a lack of evidence over the possible role of OPA in combination with regular or occasional LTPA, on CVR and mortality, and body composition.
Moderate to high levels of OPA have been found to be either beneficial (Hu et al., 2007), detrimental (Harari et al., 2015), or have unclear effects (Richard et al., 2015) on cardiovascular health. In a large prospective Finnish study, moderate (standing and walking) to heavy (walking and lifting or heavy manual labor) OPA was associated with a reduced risk of coronary heart disease (Hu et al., 2007). However, the CORDIS study, which compared men performing moderate-high OPA with men performing none-mild OPA, showed that those in the first category had a higher incidence rate of all-cause and CVD mortality (Harari et al., 2015). High OPA has also been observed to increase ambulatory blood pressure as compared to low OPA (Clays et al., 2012). In a recent systematic review with meta-analysis, no association was found between OPA and CVD mortality, although a 15% statistically non-significant increase in ischemic heart disease was observed at higher levels of OPA (Cillekens et al., 2021).
Concerning the combination of OPA and LTPA, workers performing no LTPA and high OPA were those with the highest all-cause mortality and CV risk as opposed to those performing sedentary jobs and regular LTPA, who had the lowest risk (Harari et al., 2015). The increased risk of CVD of sedentary occupations (Hermansen et al., 2019) could be ameliorated when combined with regular LTPA (Clays et al., 2014; Harari et al., 2015; Hermansen et al., 2019; Richard et al., 2015). However, this is not always the case, as it is argued that sedentarism is a risk factor for CVD independently of performed LTPA (Katzmarzyk et al., 2009). Visceral adipose tissue (VAT), more than total body fat, is another known risk factor for CVD and all-cause mortality (Després, 2012; Kuk et al., 2006), and is strongly influenced by sedentary habits and physical inactivity (Galmes-Panades et al., 2021). While regular practice of moderate-to-vigorous LTPA has been shown to significantly reduce total and visceral fat and increase muscle mass (Galmes-Panades et al., 2021), very little evidence exists on the effect of OPA at different intensities. Studies mainly focus on waist circumference or body mass index (BMI), and it seems that more intensive OPA is associated with a lower waist circumference (Steeves et al., 2012) and a lower BMI (Yuan et al., 2021), even in subjects who perform little or no LTPA (Steeves et al., 2012); however, it is unknown if this translates into improved cardiometabolic health. Therefore, the aim of this study was to evaluate the combination of different frequencies of LTPA and two types of OPA on body composition and CVR, and whether and to which extend the effect of PA on CVR is mediated by VAT.
Methods
Study Design and Participants
The present cross-sectional study included postal service workers from 83 postal offices working in the Spanish areas of Valencia, Castilla La-Mancha, Balearic Islands, and Madrid. Postal service workers were working full-time on different employment sites of the communities. Screening and inclusion were carried out between January 2008 and December 2010 during yearly voluntary routine occupational health visits. Health visits for occupational risk prevention are established as mandatory at governmental level and integrated in the Occupational Risk Prevention Plan of the company. Employees underwent a standardized health assessment which included medical history, current medications, and health monitoring (blood and urine sample collection, blood pressure measurements, anthropometric measurements); a structured interview regarding socio-demographic and health behavior characteristics such as smoking habits and exercise frequency during leisure time; and a job profile diagram to collect data on OPA (specifically the mean of kilometers covered in a day of work). During the clinical visit, workers were given information about the study and asked to participate by sharing their health assessment data for research purposes. The study protocol was in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Clinical Research of the Balearic Islands (CEI-IB) with reference number 1887.
From a total population of 2795 delivery workers, 2516 voluntarily agreed to participate (90%) and signed the written informed consent. Inclusion criteria were age between 18 and 65 years and being gainfully employed; exclusion criteria were current treatment with systemic steroids, active cancer or a history of malignancy in the previous 5 years, or pregnancy.
Exposure Assessment
Occupational physical activity was defined depending on the mean of transportation couriers used for delivery: couriers delivering by foot (i.e., postal service) were classified as “walking couriers” (WC), and those delivering by motorbike as “motorbike couriers” (MC). WC walk between 8 and 10 km on a typical day at work, while MC are required to get off their motorbikes and walk to the door to deliver the package/mail. Frequency of LTPA practice was classified as “never” (N; mostly inactive, with LTPA performed either never or almost never), “occasional” (O; if performed few times a month but less than once a week), and “regular” (R; if performed every week). Finally, according to the possible combination of LTPA and OPA, couriers were further categorized into the following six groups: MC-N, MC-O, MC-R, WC-N, WC-O, and WC-R.
Outcome Assessment
Risk of developing coronary heart disease (fatal and non-fatal) at 10-years was assessed by the Framingham and REGICOR risk equations, while fatal CVD at 10-years was estimated using the SCORE risk model. The variables used in the Framingham equation are sex, age (years), smoking (at least one cigarette a day on average over the past year), systolic blood pressure (mmHg), treatment with antihypertensive medications, diabetes (fasting plasma glucose >125 mg/dL or treatment with glucose lowering medications), total-cholesterol (mg/dL) and HDL-cholesterol (mg/dL; D’Agostino et al., 2008). The risk is expressed as percentage (%) and categorized as low (<10%); moderately high (10–20%); and high (>20%). The REGICOR equation uses the same variables as the Framingham’s; however, results are adapted to the characteristics of the Spanish population through previous calibration and validation processes (Marrugat et al., 2007; Marrugat, D’Agostino, et al., 2003; Marrugat, Solanas, et al., 2003; Ramos et al., 2003). The risk is expressed as percentage (%) and categorized as low (<5%); medium (5–9.9%); high (10–14.9%); and very high (≥15%). The SCORE algorithm is based on categories of age (years), sex, smoking status, total-cholesterol (mmol/L) and systolic blood pressure (mmHg). The 10-year risk is expressed as percentage (%) and categorized as low (<1%), moderate (1–4.9%), high (5–9.9%), and very high (≥10%; Conroy, et al., 2003).
Measures
Information on sociodemographic, health history, medication use, and smoking status (current, former, never) were recorded at participant’s entrance to the study. Specifically, data on occupation and social class were collected in accordance with the Spanish National Classification of Occupations (Domingo-Salvany et al., 2000), smoking status was self-reported and determined according to the World Health Organization (WHO) diagnostic criteria. Information on LTPA was collected by asking participants how often they practiced any sports or any form of aerobic and resistance-training exercises during free time and responding either (1) never or almost never, (2) few times a month but less than once a week or (3) every week.
Anthropometric measurements were recorded according to the International Standards for Anthropometric Assessment (ISAK) recommendations (Marfell-Jones et al., 2012) and by using the same brand of equipment in all centers involved. Height was measured to the nearest 0.5 cm using a scale mounted telescopic stadiometer (Seca 220, Seca GmbH, Hamburg, Germany), with the participant’s head maintained in the Frankfort Horizontal Plane. Body weight to the nearest 0.1 kg, total body fat (%), muscle mass (kg), and VAT (expressed on a range from 1 to 59) were measured by Bioelectrical Impedance Analysis (BIA) (Tanita BC-418, Tanita, Tokyo, Japan) (Kelly & Metcalfe, 2012), with participants wearing light clothing and standing on the metal contact with no shoes. Body mass index (BMI) was calculated by standard formula (weight in kg divided by squared height in m, kg/m2). Blood pressure was measured after a resting period of 10 minutes in supine position, using an automatic and calibrated sphygmomanometer (OMRON M3, OMRON Healthcare Europe, Spain). Measurements were taken 3 times with a one-minute gap in between; the average value was used for analysis.
Venous blood samples were taken from the antecubital vein in suitable vacutainers following a 12 hours overnight fast. Samples were then centrifuged to obtain serum (15 min, 1000 g, 4°C), which was stored at −20°C and analysed for fasting plasma glucose (FPG), total cholesterol (T-Chol), HDL-cholesterol (HDL-C) and triglycerides (TG) within 3 days in a centralized laboratory by standard procedures using an autoanalyzer (SYNCHRON CX®9 PRO, Beckman Coulter, Brea, CA, USA). Using the American Diabetes Association criteria, subjects were classified as normoglycemic (FPG <100 mg/dL), prediabetics (FPG ≥100 ≤125 mg/dL) and with type 2 diabetes mellitus (FPG ≥126 mg/d or use of antidiabetic drugs) (American Diabetes Association, 2012).
Statistical Analyses
Continuous variables were presented as means and standard deviations (SD), and categorical variables as absolute numbers and percentages (%). Independent samples t-tests and Chi-Square tests were used to compare means and frequencies of participants’ characteristics between the WC and MC groups. When more than two groups of frequencies were compared, the Bonferroni post-hoc test was performed. One-way analysis of variance (ANOVA) and Chi-Square test with Bonferroni post-hoc test was used to compare means of participants’ characteristics between the six categories derived from the combination of LTPA and OPA.
General lineal models (GLM) were performed for each outcome (CVR and mortality risk, and body composition) to evaluate their association with the six categories of combined leisure and occupational PA. Specifically, the Framingham, REGICOR, and SCORE equations were separately used as outcomes for CVD and CV mortality risk, and adjusted for age, sex and BMI. For body composition, VAT, total body fat (%) and total body muscle mass (kg) were separately used as outcomes and adjusted for age and sex. Finally, a GLM was carried out to test the mediating role of VAT in the association of PA with CVR and mortality risk. An initial model included LTPA (no/yes) and OPA (motorbike/walking) as potential predictors of CVR and mortality risk (again separately assessed by the Framingham, REGICOR, and SCORE risk equations); in the second model the predictors were further adjusted for VAT. To create the dichotomous variable LTPA (yes/no), the variables LTPA-R and LTPA-O were put together to form the variable LTPA “yes”, and the variable LTPA-N corresponded to LTPA “no”. Analyses were conducted with Stata v13.0 and SPSS v24.0 statistical software packages. All p values <.05 were deemed statistically significant.
Results
Characteristics of the Study Population as a Whole and by Occupational Physical Activity.
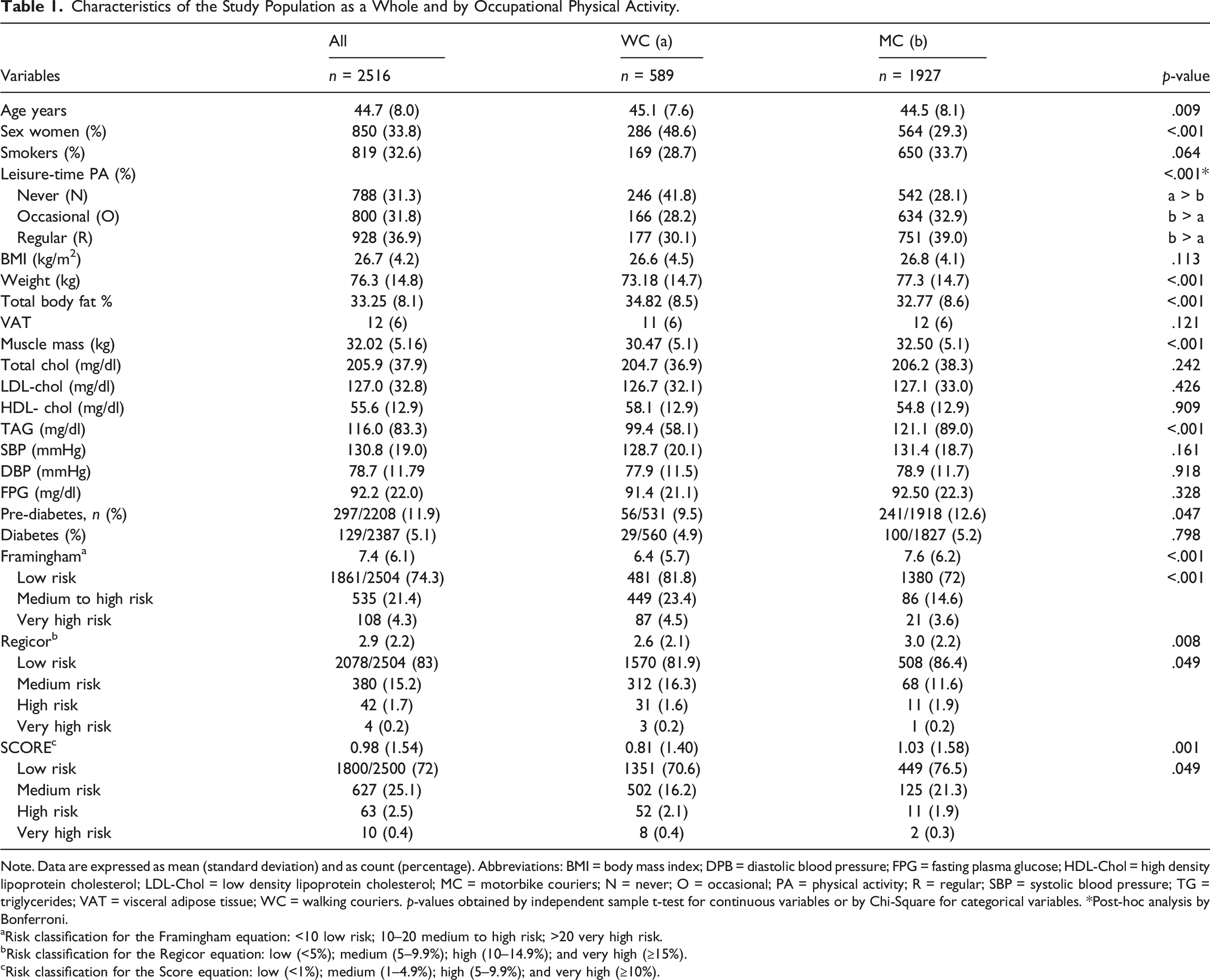
Note. Data are expressed as mean (standard deviation) and as count (percentage). Abbreviations: BMI = body mass index; DPB = diastolic blood pressure; FPG = fasting plasma glucose; HDL-Chol = high density lipoprotein cholesterol; LDL-Chol = low density lipoprotein cholesterol; MC = motorbike couriers; N = never; O = occasional; PA = physical activity; R = regular; SBP = systolic blood pressure; TG = triglycerides; VAT = visceral adipose tissue; WC = walking couriers. p-values obtained by independent sample t-test for continuous variables or by Chi-Square for categorical variables. *Post-hoc analysis by Bonferroni.
aRisk classification for the Framingham equation: <10 low risk; 10–20 medium to high risk; >20 very high risk.
bRisk classification for the Regicor equation: low (<5%); medium (5–9.9%); high (10–14.9%); and very high (≥15%).
cRisk classification for the Score equation: low (<1%); medium (1–4.9%); high (5–9.9%); and very high (≥10%).
Characteristics of the Study Population: Differences Between the six Categories of Leisure-Time Physical Activity and Occupational Physical Activity Combined.
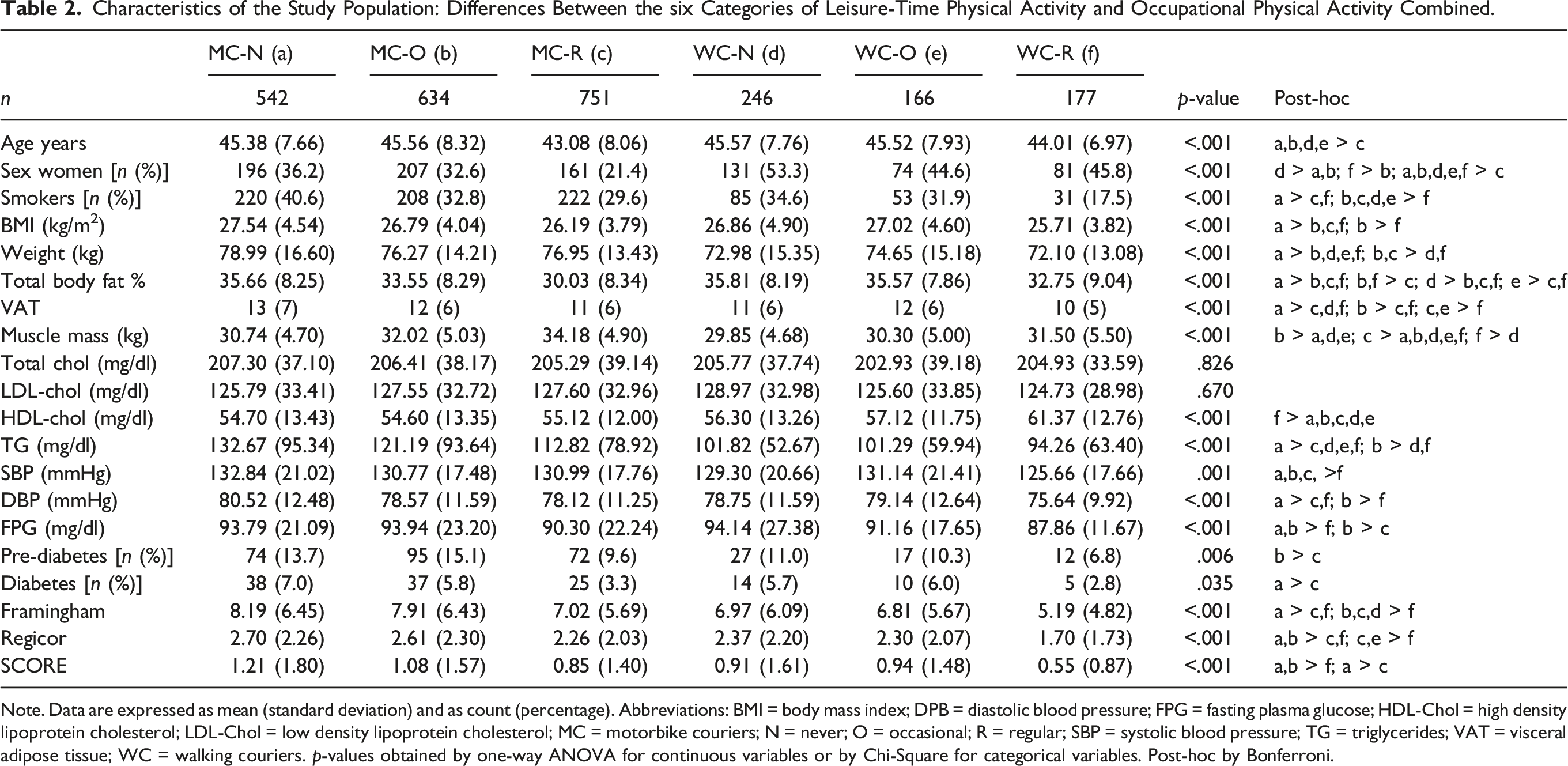
Note. Data are expressed as mean (standard deviation) and as count (percentage). Abbreviations: BMI = body mass index; DPB = diastolic blood pressure; FPG = fasting plasma glucose; HDL-Chol = high density lipoprotein cholesterol; LDL-Chol = low density lipoprotein cholesterol; MC = motorbike couriers; N = never; O = occasional; R = regular; SBP = systolic blood pressure; TG = triglycerides; VAT = visceral adipose tissue; WC = walking couriers. p-values obtained by one-way ANOVA for continuous variables or by Chi-Square for categorical variables. Post-hoc by Bonferroni.
Multivariate Linear Regression Analysis of the Association Between the six Categories of Leisure-Time Physical Activity and Occupational Physical Activity and the Risk of Developing Fatal and Non-Fatal Cardiovascular Disease Assessed by the Framingham, REGICOR and SCORE Risk Equations.
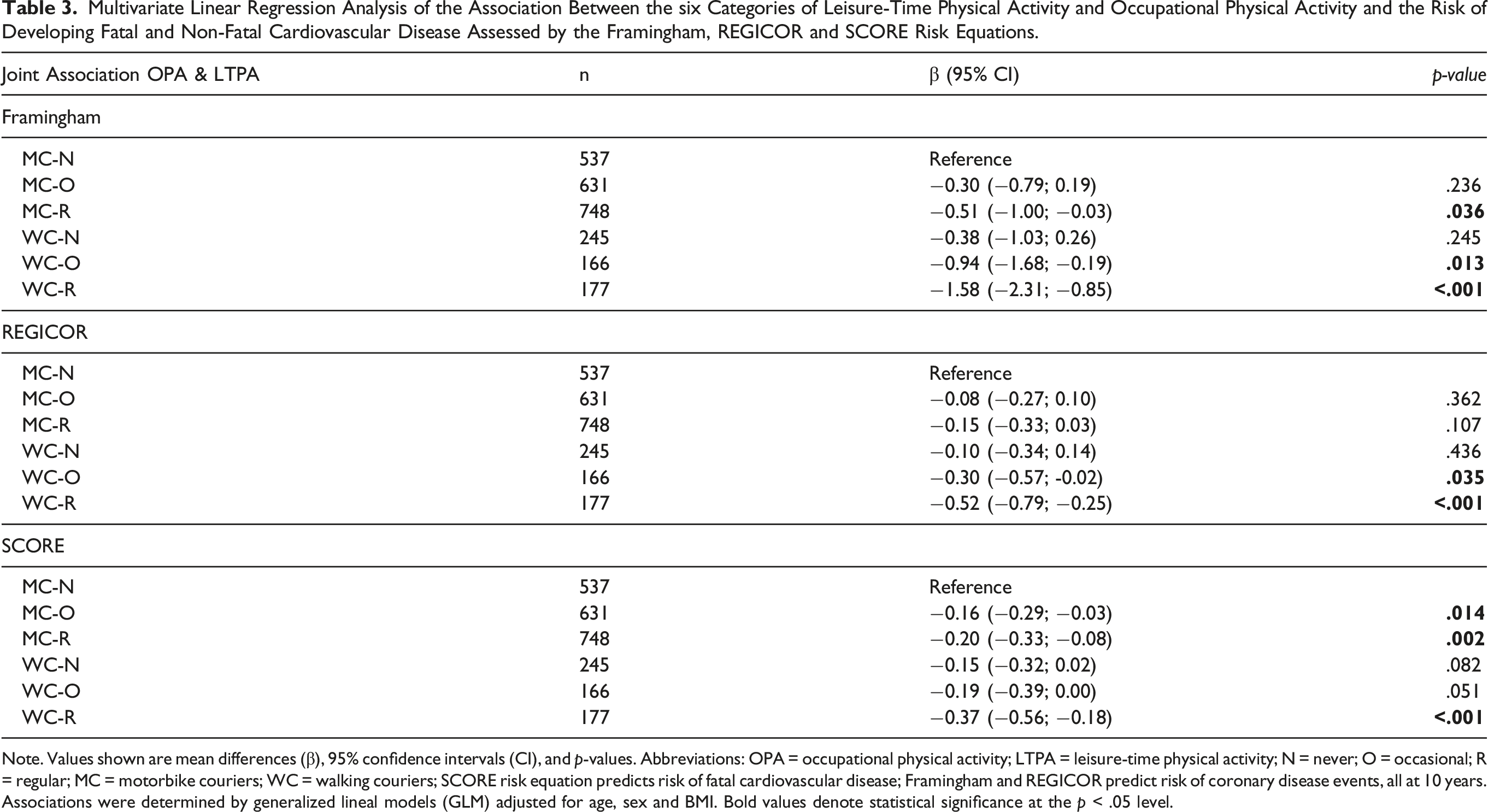
Note. Values shown are mean differences (β), 95% confidence intervals (CI), and p-values. Abbreviations: OPA = occupational physical activity; LTPA = leisure-time physical activity; N = never; O = occasional; R = regular; MC = motorbike couriers; WC = walking couriers; SCORE risk equation predicts risk of fatal cardiovascular disease; Framingham and REGICOR predict risk of coronary disease events, all at 10 years. Associations were determined by generalized lineal models (GLM) adjusted for age, sex and BMI. Bold values denote statistical significance at the p < .05 level.
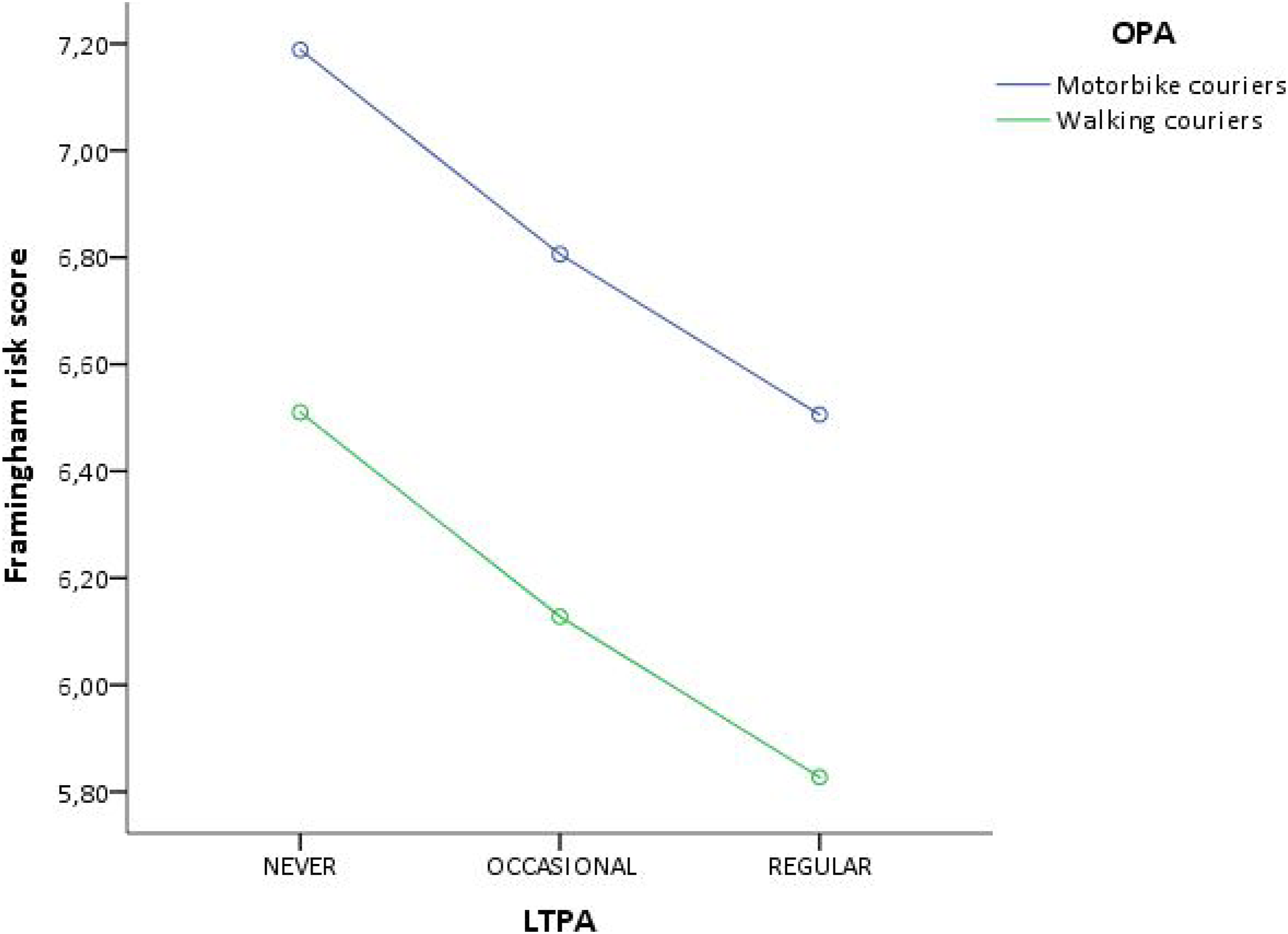
Framingham risk score across leisure-time physical activity for occupational physical activity categories.
Multivariate Linear Regression Analysis of the Association Between the six Categories of Leisure-Time Physical Activity and Occupational Physical Activity and Body Composition.
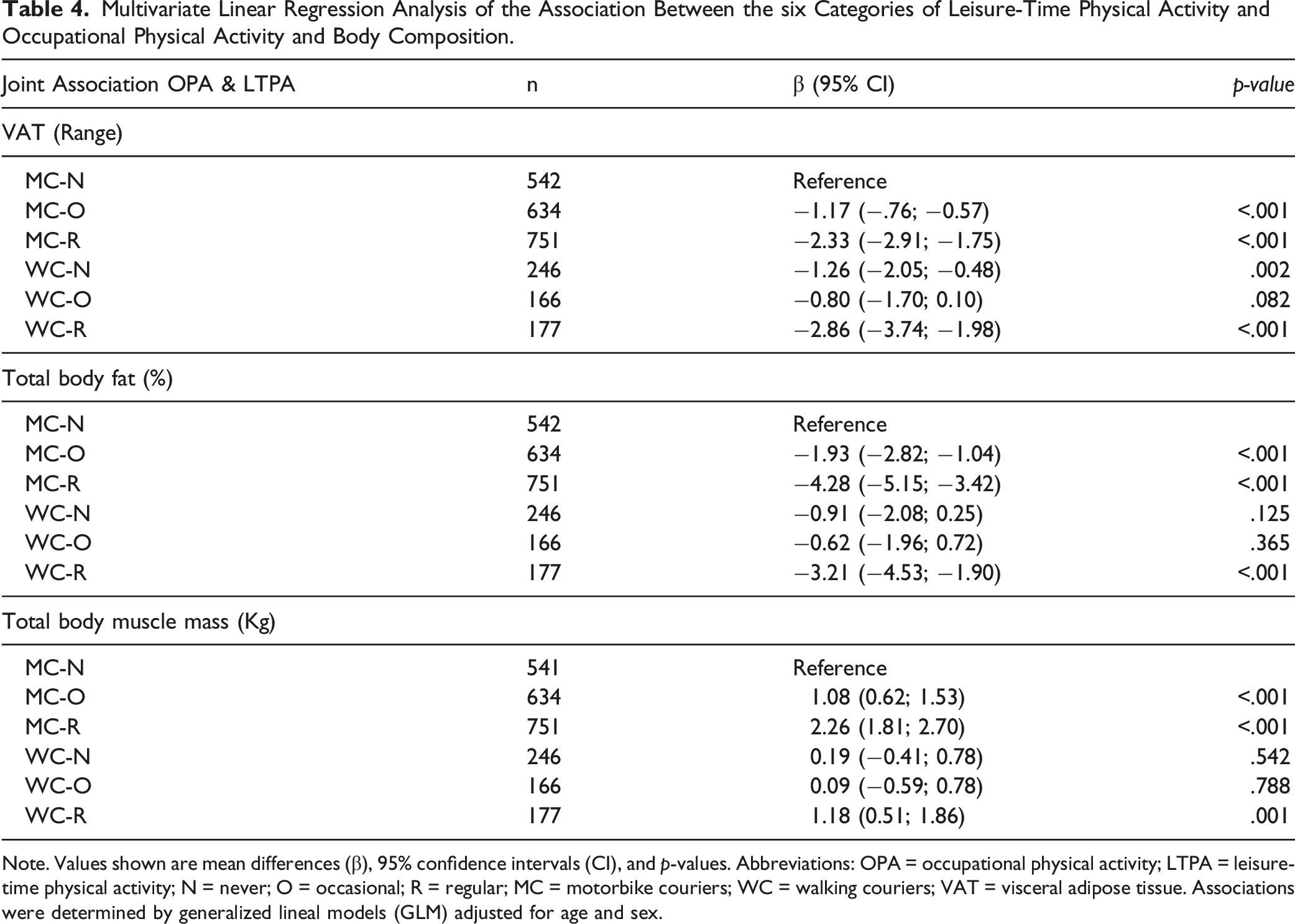
Note. Values shown are mean differences (β), 95% confidence intervals (CI), and p-values. Abbreviations: OPA = occupational physical activity; LTPA = leisure-time physical activity; N = never; O = occasional; R = regular; MC = motorbike couriers; WC = walking couriers; VAT = visceral adipose tissue. Associations were determined by generalized lineal models (GLM) adjusted for age and sex.
Discussion
Leisure-time PA performed either regularly or occasionally has consistently shown cardioprotective effects (Kraus et al., 2019; Zhao et al., 2020) as well as reduced VAT accumulation (Galmes-Panades et al., 2021), a known risk factor for CVD (Després, 2012). Evidence is inconclusive over the possible role of different intensities of OPA alone or in combination with regular or occasional LTPA, on CVR and mortality, and body composition.
The present cross-sectional study evaluated the association between the combination of two different types of OPA (motorbiking or walking) with regular, occasional, and no practice of LTPA on CVR and body composition, including VAT, in a sample of Spanish couriers. Results showed that delivering by foot and regular practice of LTPA were strongly and independently associated with both a lower CVR and healthier body composition parameters, especially reduced VAT. The combination of walking as OPA and regular LTPA showed the most cardio-protection and the lowest VAT accumulation. Regular LTPA in couriers delivering by motorbike was also associated with a diminished CVR and reduced VAT, although to a lesser extent. Moreover, despite having less total body fat % and more muscle mass than any other group, motorbike couriers practicing regular LTPA presented a blood lipid, metabolic and blood pressure profiles, and VAT, comparable with those of walking couriers practicing LTPA either never or occasionally and were more likely to suffer from prediabetes than couriers delivering by foot, independent of LTPA frequency. Furthermore, it was observed that in the nested GLM models, after adjusting for VAT, the magnitude of the association between OPA and practicing regular LTPA with CVR was diminished, showing a partial role of VAT as a mediator.
Independently of OPA, the beneficial effects of LTPA on CVD, CV mortality risk, and body composition including VAT observed in the present study are consistent with the vast body of evidence (Ekelund et al., 2016; Galmes-Panades et al., 2021; Kraus et al., 2019; Lee et al., 2012; Stamatakis et al., 2019; Zhao et al., 2020), which strongly back-up public health recommendations on the practice of PA and the reduction of sedentary behavior for health maintenance and disease prevention (Bull et al., 2020). On the other hand, our observations on the association between OPA alone or in combination with LTPA on CV health and body composition provide new insights on an issue which has not yet been fully addressed, and that so far has generated controversial results (Holtermann, Hansen et al., 2021; Hu et al., 2007; Wanner et al., 2019). In a recent systematic review and metanalysis (Cillekens et al., 2021), it was concluded that higher OPA was not associated with overall CVD mortality but was positively, although non-significantly associated with ischemic heart disease mortality risk. According to our observations however, in the case of walking as OPA compared with motorbike transport, and independently of LTPA frequency, CVR was significantly lower, indicating that occupational walking could be associated with better cardiovascular health (Cillekens et al., 2021). There is only one previous study available on the association of OPA with CVR in walking/delivery workers, which also showed that, when compared with office workers, occupational walking was associated with improved cardiometabolic health and a lower CVR (Tigbe et al., 2017). Generally, walking is a highly recommended practice because it presents a low risk of injury, provides cardiovascular protection (Murtagh et al., 2010), and reduces abdominal obesity (Hong et al., 2014; Miyatake et al., 2002). Therefore, it is not surprising that employees who do a lot of walking during their working hours exhibit increased cardiovascular protection. Our observations also demonstrate that when LTPA is regularly practiced on top of walking, the health benefits are even greater.
Some previous evidence also showed that OPA greatly influence CV health and body composition. Generally, when OPA involves repetitive or heavy lifting and strenuous manual work, it is associated with increased CVD risk (Hu et al., 2007; Sjögren et al., 2003; Wanner et al., 2019) and mortality (Hermansen et al., 2019;Holtermann, Burr et al., 2012), similar to that observed with sedentarism and sedentary jobs (Hermansen et al., 2019; Holtermann, Schnohr et al., 2012; Hu et al., 2007); however, when OPA involves walking or light aerobic chores, it associates with a reduced risk of myocardial infarction, ischemic heart disease (Hu et al., 2007), and all-cause mortality (Hermansen et al., 2019).
However, some studies showed that high OPA may increase CVR and be deleterious to health (Harari et al., 2015), or not have any influence on health risks (Richard et al., 2015). Such controversy could be explained by methodological differences including how OPA is defined (e.g., heavy and/or repetitive lifting, strenuous manual work, aerobic), categorized (light, moderate/mild, heavy), grouped and compared (e.g., low vs. high; none-to-mild vs. moderate-to-hard), and whether it is self-reported or objectively measured. Such differences in data collection and analysis could influence the interpretation of the results on the association between OPA and CVR and lead to assumptions that OPA and LTPA have opposite effects on CVD health and mortality (Hermansen et al., 2019). Accordingly, a recent metanalysis on OPA and CVD mortality suggests that the high probability of non-differential exposure misclassification of OPA as well as the healthy worker effect most likely led to an underestimation of the possible effects of high OPA (Cillekens et al., 2021).
In addition to investigating LTPA and OPA independently, their synergistic relationship in combination must also be analysed. Generally, performing strenuous OPA makes it less likely to engage in LTPA (Petermann-Rocha et al., 2019; van Dommelen et al., 2016), especially at moderate to vigorous intensities, which is the most recommended intensity (World Health Organization, 2020). The present results are in line with this pattern, where 39% of MC practice LTPA regularly in front of 30.1% of WC.
We also observed that those workers with a lower CVR, according to the Framingham equation, were those who combined regular LTPA with high OPA (WC); that is, those who combined more total PA time, independently of whether they perform a high OPA or more LTPA, followed by those who combined occasionally LTPA with high OPA, and thirdly, by workers who performed low OPA (MC) combined with regular LTPA. As opposed, MC who did not perform any LTPA were those with a worse cardiometabolic profile. The results obtained with other CVR factors and CV mortality risk equations were consistent. In fact, combining regular LTPA practice with high OPA was cardioprotective. Similarly, another study conducted on a large sample observed that higher LTPA and OPA combined was associated with a lower risk of mortality and CVD in individuals from countries with different incomes (Lear et al., 2017). In addition, another study suggests that both OPA and LTPA are associated with the lower presence of type 2 diabetes and hypertension (Petermann-Rocha et al., 2019).
When evaluating body composition, WC who performed LTPA regularly, had the lowest VAT, while MC engaging in regular LTPA presented the lowest body fat % and the highest muscle mass accumulation; however, their VAT was significantly higher than WC performing LTPA regularly. Plenty of evidence exists on the effect of LTPA on VAT, but little is known on the effect of OPA on VAT. A more intensive OPA is associated with a lower waist (Steeves et al., 2012) and a lower BMI (Yuan et al., 2021), even in subjects who perform little or no LTPA (Steeves et al., 2012). Interestingly, the MC-R group also presented a higher proportion of subjects suffering from prediabetes and diabetes than any other WC group, possibly reflecting the effect of VAT on metabolic health (Levelt et al., 2016). Aerobic exercise combined with resistance training seems to be the most effective method to maintain healthy body composition and cardiometabolic health (Lear et al., 2017; Levelt et al., 2016). Unfortunately, in our study we did not explore what type of PA couriers were performing during their leisure-time.
The main strength of this study was the use of a large sample of men and women, belonging to the same social class and with very similar incomes. Body composition was measured with an objective and validated technique, and CVR and mortality risk were determined with widely validated equations. This reduces potential bias or measurement errors and increases the opportunity for comparison across the literature. In terms of limitations, the cross-sectional design prevents the assessment of causality. Given that exposure and outcome variables were measured simultaneously, we cannot rule out reverse causation. Moreover, the lack of important information such as the type of PA performed during leisure-time, the intensity of OPA measured objectively, and dietary patterns, limits the accuracy of the results. These limitations were nevertheless overcome by using several analyses to assess the complex inter-relationships between different types of PA in relation to CVR and mortality and body composition.
Conclusion
Results from this cross-sectional study show beneficial and independent effects of both leisure and occupational physical activity on cardiovascular risk and body composition. Workers who combined more total PA time, independently of whether they perform a high OPA or more LTPA, had a lower CVR. Based on the present results and the available literature, OPA may play an important role in the association between PA and cardiovascular health and body composition. Some factors that are part of the conditions in which the OPA is carried out, such as physical and mental stress, repetitive movements and heavy lifting, should be considered when evaluating the effect of OPA on workers’ health. In addition, it is important to highlight the importance of LTPA in maintaining CV health, with the lowest risk indicators being found in those who performed LTPA regularly, independently of OPA. Moreover, the OPA performed could not be sufficient, and added LTPA could further benefit CV health. Future intervention studies are needed to confirm causality, with standardized and well-defined methodologies to define OPA.
Supplemental Material
Supplemental Material - Occupational and Leisure Physical Activity on Cardiovascular Risk and Body Composition Among Courier Workers
Supplementary Material for Occupational and Leisure Physical Activity on Cardiovascular Risk and Body Composition Among Courier Workers by Aina Maria Galmes-Panades, Manuela Abbate, Miquel Bennasar-Veny, Angel Arturo López-González, María Teófila Vicente-Herrero, Carla Busquets-Cortés, Alfonso Leiva, and Aina María Yañez in Biological Research For Nursing.
Footnotes
Acknowledgments
The authors are grateful to the field staff and participants of this study.
Author Contributions
Conception: Galmes-Panades, A.M., Abbate, M, Bennasar-Veny, M., López-González, A.A, Vicente-Herrero, M.T., Yañez, A.M.; design: Galmes-Panades, A.M., Abbate, M, Bennasar-Veny, M., Leiva, A., Yañez, A.M.; data analysis: Galmes-Panades, A.M., Abbate, M, Bennasar-Veny, M., Leiva, A., Yañez, A.M.; interpretation: Galmes-Panades, A.M., Abbate, M, López-González, A.A, Vicente-Herrero, M.T., Busquets-Cortes, C., Yañez, A.M.; data acquisition: López-González, A.A, Vicente-Herrero, M.T., Busquets-Cortes, C.; drafted manuscript: Galmes-Panades, A.M., Abbate, M, Bennasar-Veny, M., Yañez, A.M.; critically revised manuscript: López-González, A.A, Vicente-Herrero, M.T., Busquets-Cortes, C., Leiva, A. All authors gave final approval and agrees to be held accountable for all aspects of work, ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.