
Abstract
Background
Autonomic dysfunction is an important propagator of cardiometabolic disease and can be measured using multiple metrics such as heart rate variability (HRV) and heart rate recovery (HRR). The relationships between HRV and HRR have not been fully examined, nor have the relationships between HRV, HRR, and other physiological measures linked to cardiometabolic disease (e.g., blood pressure recovery). Evaluation of these additional relationships may provide new insights into the association between autonomic function and cardiometabolic disease especially among high-risk groups like firefighters.
Methods
92 firefighters (96% male, 81% white) without overt cardiovascular disease underwent exercise testing with continuous heart rate (HR) and blood pressure (BP) monitoring. HRR was the difference between maximal HR and HR 1-minute post-exercise; BP recovery (BPR) was the difference between maximal BP and BP 2-minute post-exercise. Afterwards, participants underwent 24-hour electrocardiographic monitoring to measure HRV. Unadjusted Spearman correlations and adjusted partial Spearman correlations were computed. Between group analyses were also conducted with Kruskal–Wallis test.
Results
Associations between HRV and HRR poorly converged (RMSSD and HRR, unadjusted = 0.235; adjusted = 0.144). SDNN Index exhibited the strongest association with parasympathetic tone exhibited by overall lower HRs (unadjusted = −0.600; adjusted = −0.631). HRR demonstrated stronger associations with systolic and diastolic BP responses during exercise (SBP Recovery unadjusted = 0.267; adjusted = 0.297; DBP Recovery unadjusted = −0.276; adjusted = −0.232).
Conclusions
Overall, while HRV metrics converged and were associated with lower resting heart rates, HRV and HRR poorly converged. Interestingly, HRR was related with measures of hemodynamics indicating a potential relationship with vascular function during both maximal exercise and exercise recovery.
Introduction
Measures of autonomic function such as heart rate variability (HRV) and heart rate recovery (HRR) index the contribution of the parasympathetic nervous system on cardiac and vascular regulation; consequently, autonomic dysfunction has been linked to number of cardiometabolic diseases (Laborde et al., 2017; Thayer et al., 2010). HRV refers to a variety of different measurements derived from changes in the time interval between successive regular heartbeats; whereas HRR is the difference in heart rate at maximal and post-exertion (Camm et al., 1996; Cole et al., 1999). Both HRV and HRR are increasingly being used in practice and research as measures of cardiometabolic risk because they have been validated in previous studies, easy to record, non-invasive, inexpensive, and pain free (Laborde et al., 2017, 2018).
The convergence between HRV and HRR has not been extensively investigated nor has the convergence of HRV and HRR with other physiological measures linked to cardiometabolic disease such as blood pressure recovery (BPR), heart rate reserve, and exercise performance (Laborde et al., 2018; Tanindi et al., 2015). Evaluating the relationships between HRV, HRR, BPR, heart rate reserve, and exercise performance is necessary to establish HRV and HRR as valid measures of autonomic function as well as to further investigate the associations linking autonomic dysfunction and cardiometabolic disease especially among groups with high cardiometabolic risk.
Firefighters are a high-risk group for cardiometabolic disease and sudden cardiac death, yet, due to their occupation, are an active workforce. Firefighters are expected to have endurance and strength as a part of their job making them a suitable population to investigate the associations between HRV, HRR, BPR, heart rate reserve, and exercise performance. Of note, nearly half exhibit autonomic dysfunction and harbor multiple cardiometabolic risk factors yet, as a part of their profession, are required to perform intensive exercise. From our previous studies, 55% of firefighters demonstrated autonomic dysfunction with sympathetic dominance, 48% were obese, 52% exhibited fasting hyperglycemia, and 53% were hypertensive (Al-Zaiti & Carey, 2015; Carey et al., 2011). Yet, firefighting is physically demanding with firefighters wearing heavy gear weighing up to 36 kg and performing exercises such as pulling and running often in environments which may reach 815°C (Fyock-Martin et al., 2020). The combination of underlying autonomic dysfunction, multiple cardiometabolic risk factors, and extreme physical exertion exacerbate the progression of cardiometabolic disease and even sudden death; approximately 1-in-3 deaths occur during fire suppression, although only 1% of occupational time was spent performing this duty (Ebersole et al., 2020; Smith et al., 2019). In summary, studying firefighters provides a unique opportunity to investigate the associations between HRV, HRR, BPR, heart rate reserve, and exercise performance necessary to understand the dynamic relationships between autonomic function and cardiometabolic disease.
In this analysis, we evaluated the relationships between HRV, HRR, BPR, heart rate reserve and exercise performance to understand the linkage between autonomic function and cardiometabolic disease. As measures of autonomic function, we hypothesized that HRV and HRR would be positively correlated, and that HRV and HRR would also be positively correlated with exercise performance and resting 24-hour hear rate reflecting strong parasympathetic dominance. Additionally, we hypothesized HRV and HRR would positively correlate with BPR and exercise performance such that greater parasympathetic influence would correspond to faster vascular recovery and improved overall fitness; and, that HRV and HRR would be positively correlated with heart rate reserve given parasympathetic withdrawal during acute exercise.
Methods
This study was a secondary data analysis from the study of Surveying and Assessing Firefighters Fitness and Electrocardiogram (SAFFE). SAFFE was a cross-sectional study to evaluate the prevalence of electrocardiographic and socio-psychological risk factors among on-duty firefighters. To improve the ecological fidelity of this study, all data were collected in the firehouse. Seven different firehouses belonging to the same fire department in upstate New York were included. The study’s primary results have been reported previously (Al-Zaiti & Carey, 2015). For the protection of human subjects for research, the institutional review board at the State University of New York approved this study. All firefighters were eligible to participate in the SAFFE study, but for this analysis some were excluded including: those with diagnosed cardiometabolic disease; those on medications (i.e., beta-blockers) that influence heart rate and blood pressure; and those unwilling or unable to exercise. Consent and enrollment occurred in a quiet and private bunkroom where participants could ask questions regarding the study. During enrollment, participants self-reported demographics (i.e., age, sex, history of currently smoking), and a registered nurse collected weight using a calibrated bathroom scale, as well as height and waist circumference using a tape measure. Body mass index (kg/m2) was computed and organized based on recommended classifications (Calle et al., 2003). Blood pressure (BP) was measured using a manual sphygmomanometer over the brachial artery in a resting position. Two recordings were taken 5-minutes apart from each other and averaged together. Hypertension was categorized in accordance with the 2017 American Heart Association Hypertension Guidelines (Whelton et al., 2017).
Exercise Stress Test Protocol
All participants underwent an exercise test based on the Bruce protocol with continuous BP and electrocardiography (ECG) monitoring in accordance to published guidelines (Bruce, 1974; Fletcher et al., 2013). Participants were asked to abstain from consuming stimulants, and to avoid smoking for at least 12 hours prior to exercise. The protocol included seven incremental stages. Each stage took 3 minutes with an incremental increase in speed and incline of the treadmill. When the participant achieved 80%–85% of the predicted maximal heart rate, calculated as 220–age (years), the nurse turned the treadmill into a recovery mode and allowed for 5 minutes of recovery. Participants remained standing during the recovery phase. For the safety of participants, the nurse monitored the entire exercise test, and terminated the protocol if participants complained of discomfort such as chest pain or dyspnea. In case of an emergency, nurses had basic life support training and an automatic external defibrillator. No complications occurred. Measures of exercise performance included maximum speed achieved (miles per hour, mph), maximum incline achieved (% incline), and metabolic equivalent of task (METs).
Exercise Measures of Interest
Cardiovascular Measures, Operational Definitions and Clinical Significance.
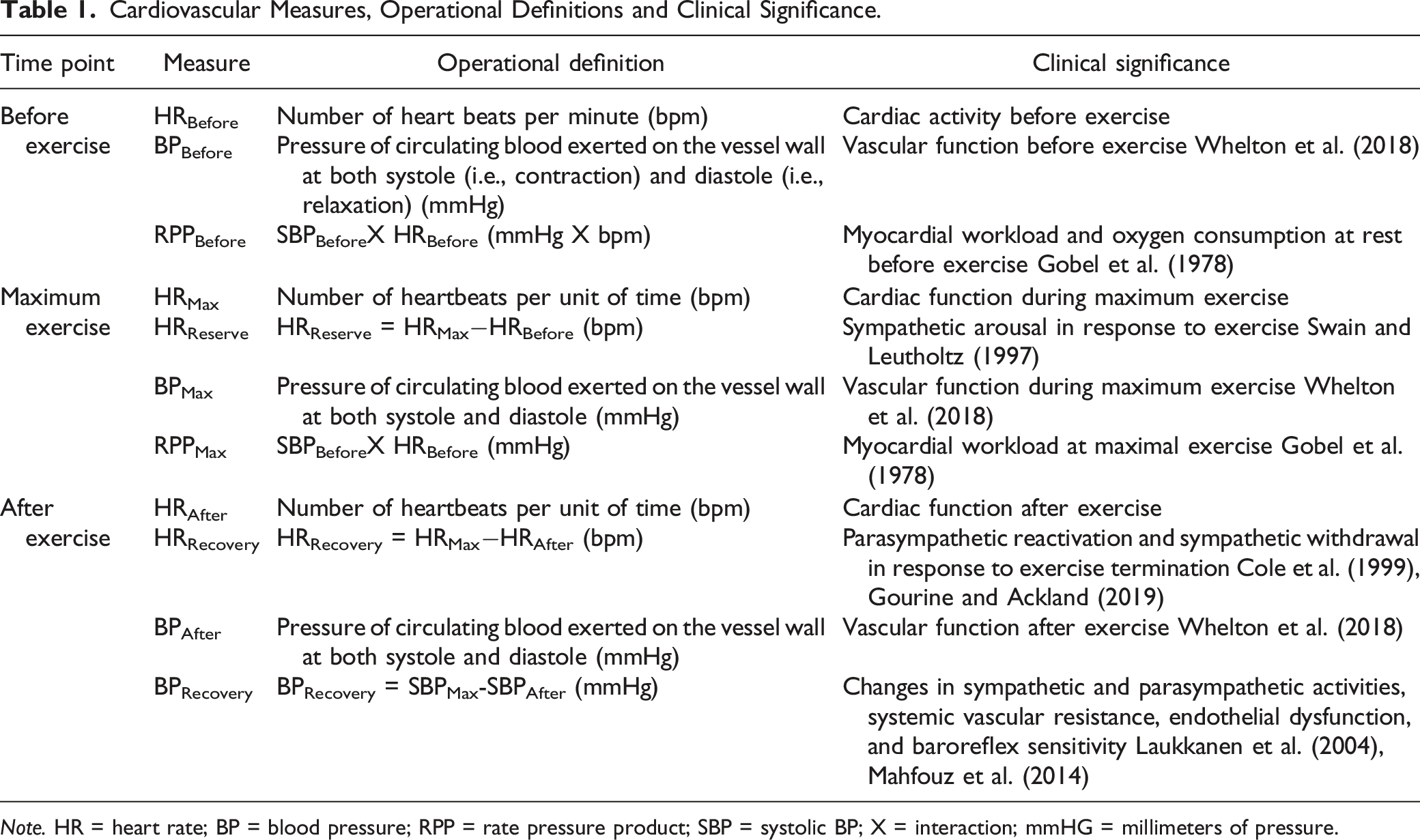
Note. HR = heart rate; BP = blood pressure; RPP = rate pressure product; SBP = systolic BP; X = interaction; mmHG = millimeters of pressure.
24 Hour ECG Holter Recording and Heart Rate Variability
Afterwards, the 24-hour monitor remained on the firefighter to capture HRV metrics. In order to optimize the quality of the electrode signal and reduce artifact, the nurse cleaned and removed any skin oil with alcohol pads and shaved the firefighter’s chest hair if needed. After making sure the skin was well-prepared, 10 electrodes were placed in the Mason-Likar position (Mason & Likar, 1966). The nurse verified that all electrodes were firmly attached to the torso and that the Holter monitor (Mortara Instrument) functioned normally by verifying the ECG signal on the display. To ensure data was accurately recorded, the nurse regularly monitored the Holter display and replaced electrodes as needed. The participant was instructed to wear the Holter monitor continuously for 24 hours. Afterwards, a research nurse retrieved the monitor for offline analysis.
Heart Rate Variability
Once the 24-hour session was completed, ECG recordings were downloaded to a laptop computer equipped with H-Scribe 4 software (Mortara Instrument) for ECG analysis. All ECGs were reviewed and manually annotated by a PhD-prepared cardiovascular nurse (PhD, Acute Care Nurse Practitioner, RN) blinded to the study and verified by a second PhD-prepared cardiovascular nurse and principal investigator of the study (PhD, RN). This inter-rater agreement was especially important with HRV measures which can be artificially elevated due to underlying arrhythmias such as atrial fibrillation (Camm et al., 1996). For the purpose of this study, four time-domain measures of HRV were included: SDNN (standard deviation of all normal R-R (NN) intervals, reported in milliseconds (ms)), SDNN Index (the average standard deviation of the NN intervals for each 5 minutes segment of a 24 hours HRV recording, reported in ms), NN50 (percentage of differences between adjacent NN intervals >50 ms, reported as a percent %), and RMSSD (root mean square of successive RR interval differences, reported in ms) (Camm et al., 1996; Shaffer & Ginsberg, 2017). We focused on time domain metrics of HRV because (1) we used 24-hour recordings, the gold standard for time domain measurements and (2) these are the most commonly reported in medical literature (Shaffer & Ginsberg, 2017). Furthermore, these measures are becoming increasingly accessible to consumers and scientists through wearable technology (Laborde et al., 2017). After data cleaning, the computer software automatically computed the necessary HRV metrics and exported them for analysis.
Covariates
Given the observational nature of this data, covariate adjustments were necessary. For this study, significant covariates included age (years) (Shaffer & Ginsberg, 2017), sex (male/female) (Shaffer & Ginsberg, 2017), race (white/non-white) (Hill et al., 2015), and BMI (kg/m2) (Thayer et al., 2010).
Additional Measures
In this manuscript, we also report measures of depressive symptoms and sleep quality, which also influence autonomic function (Liao et al., 2014; Tobaldini et al., 2013).
Depressive Symptoms
The Beck Depression Index- II (BDI-II) was used to measure depressive symptoms (Beck et al., 1988). The BDI-II is a 21-question multiple-choice survey, and one of the most widely used self-report inventories to screen for depressive symptoms among adults. The 5-minute inventory includes items related to symptoms of depression including hopelessness, irritability, mood, and fatigue. The validity and reliability of BDI-II has been extensively studied. The internal consistency has been reported to be 0.89 and the test–retest reliability has been reported to be 0.75 in a recent comprehensive meta-analysis of varying studies using this instrument (Erford et al., 2016). Additionally, convergent comparisons were robust across 43 depression instruments (Erford et al., 2016). For screening purposes, participants scoring ≥14 points (possible range 0–63) on the BDI-II were considered to be at least mild-to-moderately depressed. Our lab has previously reported that decreased HRV was associated with depressive symptoms among firefighters (Liao et al., 2014). The Cronbach’s alpha for the BDI-II survey in the sample was 0.86.
Sleep Quality
The well-validated Pittsburgh Sleep Quality Index (PSQI) was used to subjectively evaluate sleep quality (Buysse et al., 1989). Previous studies report that sleep is modulated by autonomic function (Tobaldini et al., 2013). The PSQI contains 19 self-rate questions divided into the following components: sleep quality, sleep latency, sleep duration, habitual sleep efficiency, and sleep disturbances, use of sleeping medication, and daytime dysfunction. Each of the seven components scored from 0 indicating no difficulties to three indicating severe difficulty. The seven component scores are summed for a global score ranging from 0 to 21 with 0 indicating no difficulty sleeping and 21 indicating severe difficulties with sleeping. For this study, a PSQI score ≥5 was considered for poor sleep quality which has been reported to have a diagnostic sensitivity of 98.7% and specificity of 84.4% to distinguish between “poor” sleepers from “good” sleepers and had high test-retest reliability (Backhaus et al., 2002). The Cronbach’s alpha for the PSQI has been reported to be 0.83 (Buysse et al., 1989) and in the sample was 0.88.
Secondary Data Power Analysis
To ensure computational adequacy of the data to achieve the proposed research aims, a power analysis was computed. Using GPower 3.1 (Faul et al., 2007) and assuming a small effect size (d = 0.3), a type I error rate of 0.05, and a total sample size of 92, power was calculated to be 0.84 using a correlational bivariate model. This was considered adequate power to answer the research aims of this secondary analysis.
Statistical Analysis
All statistical analyses were performed using SPSS (version 25.0). All analyses were 2-tailed, and statistical significance was set at 0.05. Continuous variables were evaluated for normality of distribution by visual inspection of the histogram, and the Shapiro-Wilk test. All of measures of autonomic function (e.g., SDNN, SDNN Index, HRR) were not normally distributed which is consistent with past studies (Shaffer & Ginsberg, 2017). Based on prior publications, we choose not to use a natural logarithm transformation in order to preserve the ability to easily interpret data (Shaffer & Ginsberg, 2017). Consequently, most of the statistics used in this analysis were non-parametric. The mean (± standard deviation, SD) for normally distributed variables and the median (interquartile range, IQR) for non-normally distributed variables are reported. Spearman correlations with bootstrapping of 10,000 samples was computed. Due to a number of potential confounding variables identified from past studies, partial Spearman correlations were adjusted for age, BMI, sex (male; female), and race (white; non-white) (Shaffer & Ginsberg, 2017). We used the SPSS Syntax Editor to write the following code: NONPAR CORR/MISSING = LISTWISE/MATRIX OUT(*) RECODE rowtype_ (‘RHO’ = ‘CORR’) PARTIAL CORR/significance = twotail/MISSING = LISTWISE/MATRIX IN(*).To add robustness to this analysis, between group analyses using Kruskal-Wallis non-parametric tests were conducted using median values based on age (< 45; ≥ 45 years of age), BMI (< 28.0; ≥ 28.0 kg/m2), sex (male; female), race (white; non-white), depression (BDI-II ≥ 14), and sleep quality (PSQI ≥ 5) with cutoffs being determined based on median values or on published literature (Liao et al., 2014; Tobaldini et al., 2013).
Results
Demographics
After excluding 21 firefighters who were receiving treatment for a cardiorespiratory condition or had known cardiovascular disease, 91 firefighters were included in this analysis. All participants were in normal sinus rhythm for the entirety of the Holter recording. The majority were male (96%, n = 87), white (81%, n = 74), non-Hispanic (81%, n = 74), overweight (47%, n = 43) or obese (41%, n = 38), and hypertensive (70%, n = 64). In this sample, 11% (n = 10) had a positive BDI-II screening for depressive symptoms and 56% (n = 51) were poor sleepers. The mean age of a firefighter in this sample was 43 (±7.9) years, and mean length of employment of a firefighter was 15 (±7.1) years. Only 12.0% (n = 11) were currently tobacco smokers with an average of one pack/day (±0.6 packs), 3.3% (n = 3) self-reported a diagnosis of sleep apnea, and 1.1% (n = 1) self-reported pre-diabetes.
Convergent Validity Between Measures of Autonomic Activity
Correlations Between HRV, HRR, and Heart Rate Dynamics (n = 91).
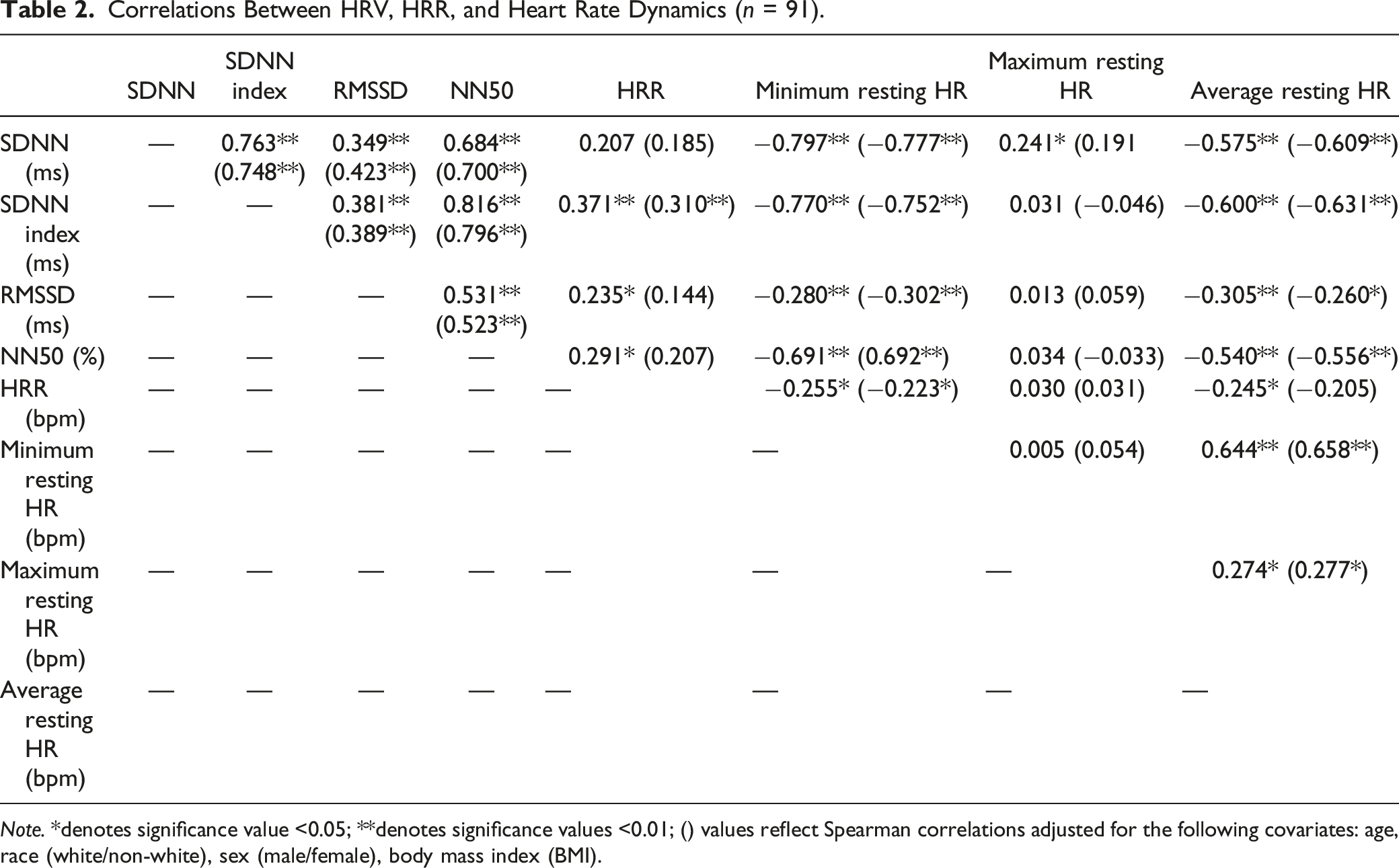
Note. *denotes significance value <0.05; **denotes significance values <0.01; () values reflect Spearman correlations adjusted for the following covariates: age, race (white/non-white), sex (male/female), body mass index (BMI).
Autonomic Function and Exercise Performance
Correlations Between HRV, HRR, and Exercise Performance (n = 91).
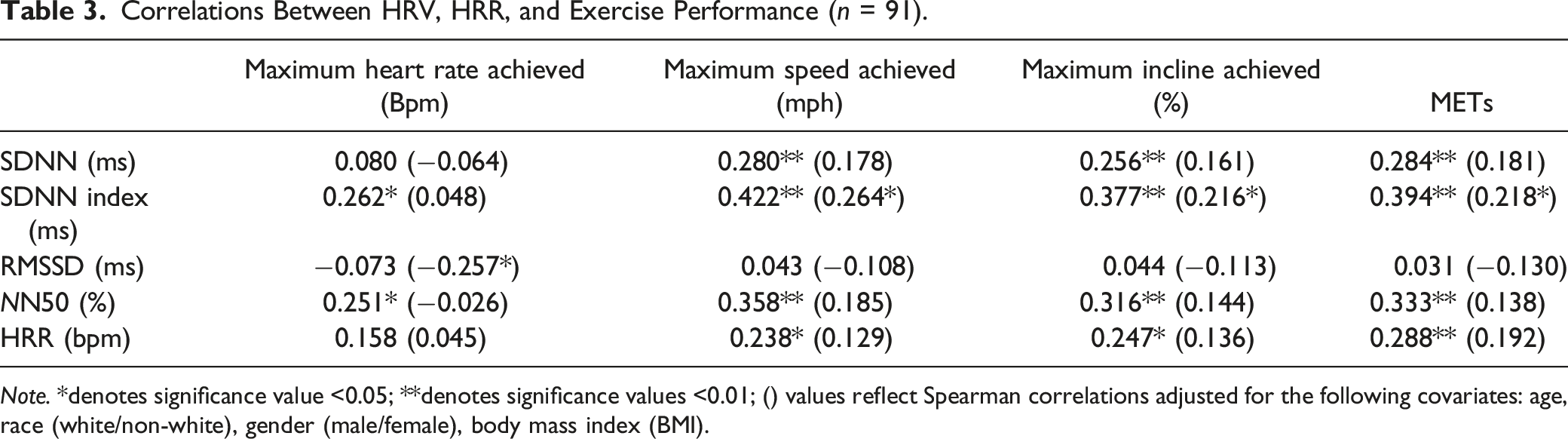
Note. *denotes significance value <0.05; **denotes significance values <0.01; () values reflect Spearman correlations adjusted for the following covariates: age, race (white/non-white), gender (male/female), body mass index (BMI).
Autonomic Activity and Cardiac Hemodynamics During Exercise
Correlations Between Metrics of HRV, HRR, and Blood Pressure During Exercise (n = 91).
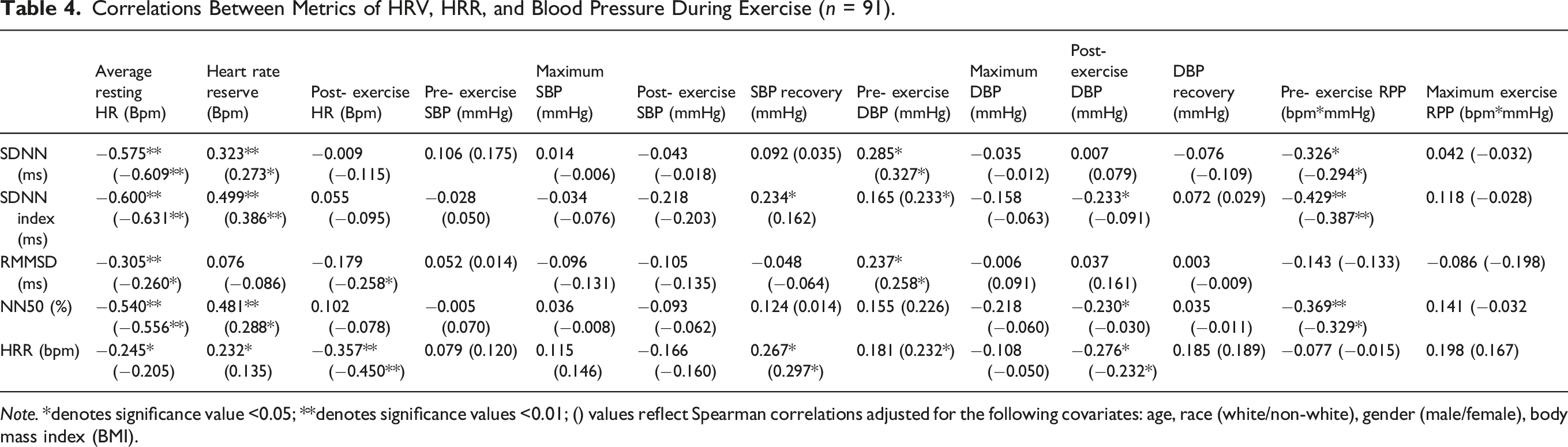
Note. *denotes significance value <0.05; **denotes significance values <0.01; () values reflect Spearman correlations adjusted for the following covariates: age, race (white/non-white), gender (male/female), body mass index (BMI).
Between Group Analyses
Between Group Analyses Based on Demographics Depressive Symptoms, and Sleep Quality.
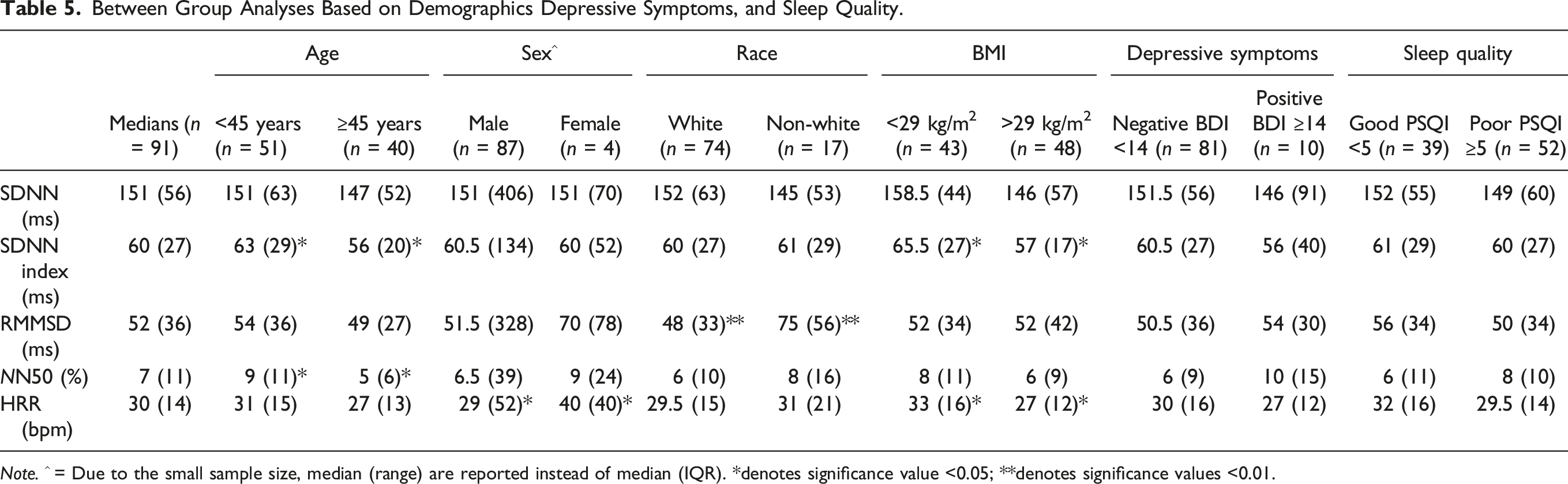
Note. ^ = Due to the small sample size, median (range) are reported instead of median (IQR). *denotes significance value <0.05; **denotes significance values <0.01.
Discussion
In this secondary data analysis, we report (1) a weak relationship between HRV and HRR; and (2) weak-to-moderate correlations with measures of cardiac hemodynamics during physical exertion with HRR having higher associations to vascular measures compared to HRV. Additionally, between-group analyses showed sizeable differences across well documented factors which influence autonomic function, age, sex, race, and BMI (Hill et al., 2015; Shaffer & Ginsberg, 2017; Thayer et al., 2010). Overall, these findings can be interpreted such that there is poor convergence between HRV and HRR despite the same underlying physiological understanding (Laborde et al., 2018; Gourine & Ackland, 2019). Based on these data, we hypothesize HRV provides excellent measurement of parasympathetic influence on the heart itself, whereas HRR may be a more holistic marker of parasympathetic and sympathetic leading to unforeseen relationships with vascular measures.
The lack of a strong relationship between HRV and HRR reflects poor convergent validity. Similar findings have been published by Esco et al. (2010) which demonstrated HRV may not be related to the HRR among a small sample of college aged men (Esco et al., 2010). Of note, this study measured HRV using 5 minutes compared to 24 hours in the present manuscript (Esco et al., 2010). Similarly, among a sample of 31 healthy physically active men, Molina et al. (2016) reported a lack of significant correlations of absolute HRR and percent change HRR at the first minute post-exercise with HRV parameters in supine and standing postural positions (Molina et al., 2016). Despite similar theoretical underpinnings, differences in HRV and HRR pose a potential measurement threat as they are assumed to be related to the same physiological mechanisms (Laborde et al., 2017; Thayer et al., 2010; Gourine & Ackland, 2010). In our data, HRV variables demonstrated high intra-correlation suggesting convergence onto the same construct of heart rate regulation by the parasympathetic nervous system and had strong positive correlations with resting 24-hour heart rate and minimum 24-hour heart rate which further supports this convergence. In summary, our findings align with previous investigations, and suggest HRV reflects parasympathetic influence of the heart itself were as HRR may be more reflective of parasympathetic and sympathetic influence. Specifically, HRR was negatively correlated with post-exercise systolic and diastolic BP and was positively correlated with systolic and diastolic BPR, and these associations are consistent with the underlying understanding that after exercise sympathetic withdrawal and parasympathetic reactivation dramatically decrease HR and BP (Cole et al., 1999; Laborde et al., 2018; Laukkanen et al., 2004; Tanindi et al., 2015). This dynamic flux in sympathetic and parasympathetic activity is responsible for a number of hemodynamic changes including a drop in total peripheral resistance and cardiac output (Gourine & Ackland, 2019; Laukkanen et al., 2004; Mahfouz et al., 2014; Tanindi et al., 2015). Given that the sympathetic nervous system directly innervates vessel walls, this may partially explain the association between HRR and hemodynamics. Mahfouz et al. (2014) reported abnormal HRR and poor systolic BPR were significantly correlated with impaired endothelial function and diastolic dysfunction among a sample of prediabetic patients (Mahfouz et al., 2014). Also, given the cohort of professional firefighters was largely hypertensive and overweight, it is reasonable to assume there may have undiagnosed cardiometabolic conditions. Interestingly, Alihanoglu et al. (2015) reported that metabolic syndrome and not the individual components of metabolic syndrome were independently associated with impaired systolic BPR and HRR. In a more robust trial, Kim et al. (2019) reported HRR at the first minute and poor systolic BPR were associated with microvascular angina, a phenomenon with overt chest pain caused by abnormalities of the coronary arteries and hypothesized this due to poor vessel dilation due to poor parasympathetic response (Kim et al., 2019). To summarize, HRR may measure the dynamic interplay between the sympathetic and parasympathetic nervous system during recovery from exercise representing not just heart function but also endothelial function and vascular activity.
Lastly, this analysis reinforces the well-documented relationships between HRV and HRR, and heart rate reserve and exercise performance. Previous longitudinal studies performed among athletes and patients demonstrates that repeated aerobic exercise training improves both autonomic function and exercise performance and produces a mortality and morbidity benefit (Pearson & Smart, 2018). Although we cannot provide evidence of long-term benefits, this study reported moderate strength correlations with HRV and heart rate reserve indicating overall between autonomic function, and moderate-to-weak positive correlations between HRV and HRR with maximum speed achieved, maximum incline achieved, and MET achieved. Of note, after adjustment for age, BMI, sex, and race the strength of associations was significantly weaker so these additional factors may infringe on the benefits of exercise performance. Based on our prior results, other occupational-related risk factors such as career length may be more pertinent than traditional covariates like age (Dzikowicz & Carey, 2021). Further work is necessary to investigate the neurophysiological mechanisms underlying the plasticity of autonomic function and, given our findings regarding the relationship between HRR and BPR, we emphasize future research should investigate the mechanisms between autonomic function on both the heart, endothelial function, and vasculature.
Our study provides correlational evidence that HRV and HRR reflect unique measures of autonomic function and overall fitness which may help screen firefighters for progression of cardiometabolic disease and sudden death. Given that cardiometabolic disease and sudden cardiac death rely on inputs from cardiac vagal tone, vasculature, and the heart itself, HRV and HRR may be used as during screening measures to index autonomic function under fire simulations to mimic when the risk of sudden death is highest (Ebersole et al., 2020; Smith et al., 2019). This study adds to our previous analyses which have investigated the affects of cardiometabolic disease among the firefighter population (Al-Zaiti & Carey, 2015; Carey et al., 2011; Dzikowicz & Carey, 2019a, 2019b; Dzikowicz & Carey, 2020, 2021). Moreover, both measures could be used to index autonomic function after aerobic rehabilitation among firefighters with autonomic dysfunction who at greatest risk for cardiometabolic disease and sudden death (Fyock-Martin et al., 2020).
Given the correlational design of this study, several limitations may impact the study results. Confounding effects by other moderator variables not measured in this study such as physical activity, muscle mass, and the number of fire calls may confound results. HRR and BPR were measured at two different time intervals, potentially impacting the interpretation of the results though these time cutoffs were identified from previous studies (Cole et al., 1999; Laukkanen et al., 2004). Only one stress test was completed which does not reflect the daily fluctuations of the sympathetic and parasympathetic nervous system. Lastly, we did not include other measures of vasculature function such as inflammatory biomarkers or pulse wave analysis which would strengthen our argument regarding the relationship between HRR and BPR. In conclusion, this manuscript reports poor convergent validity between HRV and HRR and novel relationships between HRR and BPR which potentially describe the interplay between sympathetic and parasympathetic influence on vascular function among high-risk population, that is, firefighters.
Footnotes
Acknowledgements
We thank the firefighters who participated in this research.
Author Contributions
D.J.D. contributed to conception and design contributed to analysis and interpretation drafted manuscript critically revised manuscript gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy. M.G.C contributed to acquisition, analysis, and interpretation critically revised manuscript gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the National Institutes of Health, Mary G Carey R21 NR-011077.