
Abstract
Introduction
Chronic diseases are the biggest emerging threat to global health (Lozano et al., 2016). Chronic obstructive pulmonary disease (COPD) ranks the third leading cause of death currently worldwide and is a multi-factorial progressive chronic lung disease, defining features include persistent airflow obstruction and chronic airflow limitation because of airway and/or alveolar abnormalities (López-Campos et al., 2016). Most patients with COPD may experience lower exercise tolerance, enhanced dyspnea, as well as reduced quality of life (Decramer et al., 2012; Gu et al., 2021). Increased COPD symptoms provoke anxiety and depression, which inevitably lead to further breathlessness and exacerbation of panic. This causes a vicious circle whereby any activities that involve physical exertion are avoided, thereby leading to accelerated disease progression and increased mortality (Bourbeau & Nault, 2007; Martí et al., 2020; Ngai et al., 2016). In addition, COPD, as an incurable condition, carries a huge and growing economic and social burden (Barbosa et al., 2020). Therefore, it is imperative to explore effective therapy to help patients manage their symptoms to improve exercise capacity, lung function as well as other health-related functions.
The current treatment options for COPD include pharmacological, non-pharmacological (e.g., smoking cessation, exercise, oxygen therapy and pulmonary rehabilitation), and surgical treatment (e.g., lung transplantation; Mulhall & Criner, 2016; Vogelmeier et al., 2020). While pharmaceuticals have been studied extensively and utilized, their disease-modifying effects are limited or even uncertain (Mulhall & Criner, 2016; Ngai et al., 2016). Invasive surgical treatments have known postoperative complications (Decramer et al., 2012). Tai chi is a type of fitness exercise combining psychological treatment and physical exercise with no special equipment and attracts the attention and interest of the world (Polkey et al., 2018). Tai chi is characterized by slow, controlled graceful movements of different body parts, which integrates mental concentration and deep breathing (Chan et al., 2011; Wang et al., 2022). The potential benefits of tai chi have been well established by promoting circulation of ‘‘Qi’’ (vital energy) in the meridians, regulating functions of the internal organs, and improving psychological condition without risks of surgery and adverse drug reactions (Chan et al., 2011; Wang et al., 2022; Zhang et al., 2019).
The health benefits of tai chi have been observed in many chronic conditions, such as osteoarthritis, chronic pain, and Parkinson’s disease (Cai et al., 2022; Deuel & Seeberger, 2020; Hu, X. et al., 2020b; Urits et al., 2021; Zhang et al., 2021). However, whether tai chi is beneficial in improving lung function and health-related outcomes in COPD patients is presently inconclusive. A Cochrane systematic review explored the effects of tai chi for symptom improvement in COPD and found better effects on pulmonary function, but not on dyspnea level and quality of life (QoL; Ngai et al., 2016). A randomized controlled trial (RCT) including 120 patients conducted by Polkey et al. (2018) revealed a significant difference for QoL and 6-min walk distance (6MWD), but not for FEV1. A recently published RCT also evaluated the benefits of tai chi for COPD, and significant effects on mood, social support, and functional capacity were observed (Kraemer et al., 2021). Currently, no consensus has been reached about the benefits of tai chi (Zhang et al., 2019). With a plethora of original studies recently published, it is possible to explore a comprehensive picture of the potential benefits of tai chi for patients with COPD in terms of lung function and health-related outcomes (Kraemer et al., 2021; Zhu et al., 2018). Hence, this systematic review aims to evaluate the effects of tai chi on lung function, exercise capacity, and psychosocial outcomes in patients with COPD.
Methods and Search Strategy
This systematic search followed an international prospectively registered protocol (PROSPERO CRD42023389695). PubMed, Cochrane Central Register of Controlled Trials (CENTRAL), Embase, Chinese National Knowledge Infrastructure (CNKI), Wanfang, and China Science and Technology Journal (VIP) databases were searched to identify RCTs related to this topic from inception to January 5, 2023. Reference lists of related system reviews and meta-analyses were also manually searched to expand our search scope and identify more eligible RCTs. RCTs published in English and Chinese were included. The specific search strategy is shown in the supplementary material.
Inclusion Criteria
Study Selection and Data Extraction
Two reviewers independently read titles and abstracts identified by the search and then screened the full manuscripts of potentially relevant RCTs. The same two reviewers also independently extracted the data of eligible studies and recorded these on a Microsoft Excel spreadsheet, including author, year, participant characteristics, study location, details of intervention and control, time point as well as outcomes. Any disagreements were resolved through discussion with the third researcher.
Quality Appraisal
Two reviewers independently evaluated the quality of the eligible RCTs with the risk of bias tool from the Cochrane Collaboration (version 5.1.0), focusing on sequence generation, allocation concealment, blinding, attrition bias, completeness of outcome data, and other sources of bias (Higgins et al., 2019). The risk of bias for each item was adjudicated as ‘yes’ (low bias), ‘no’ (high bias), or ‘unclear’ (lack of relevant information or uncertainty of bias). Any discrepancies were also settled by a discussion with a third researcher.
Data Synthesis and Analysis
RevMan 5.30 was used for data synthesis and analysis. The standard mean difference (SMD) or mean difference (MD) with a 95% confidence interval (CI) was used to calculate the pooled effect size. Effect sizes were classified as small (SMD < 0.40), moderate (SMD = 0.40), or large (SMD > 0.70; Higgins et al., 2019). Statistical heterogeneity was assessed using the Cochran Q test and the Higgins I 2 statistical test. A fixed-effect model was used when no significant heterogeneity was observed (p > .05 and I 2 < 50%); otherwise, a random-effect model was applied. Sensitivity analysis was performed by removing each included RCT at a time to compare the effect sizes and CIs of the remaining RCTs. Potential publication bias was assessed with Egger’s test.
Results
Study Selection and Characteristics
A total of 582 records were identified. After removing duplicates, 366 articles were excluded after the title and abstract screen. After reviewing the full text, 20 finally fulfilled the inclusion criteria and were included for further analysis. The flow chart of study selection and screen is presented in Figure 1. Flow chart for the selection process.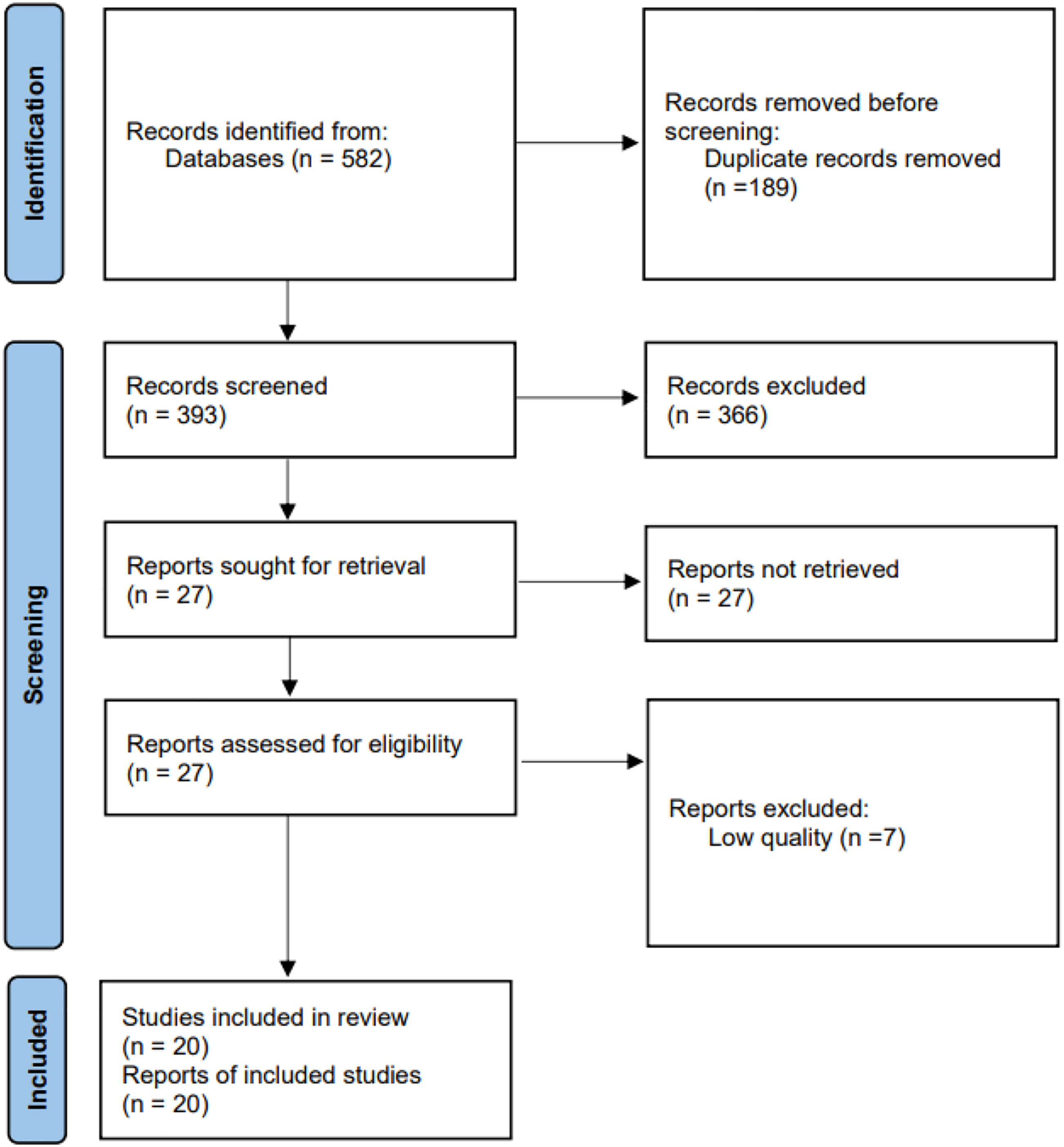
Study Characteristics.
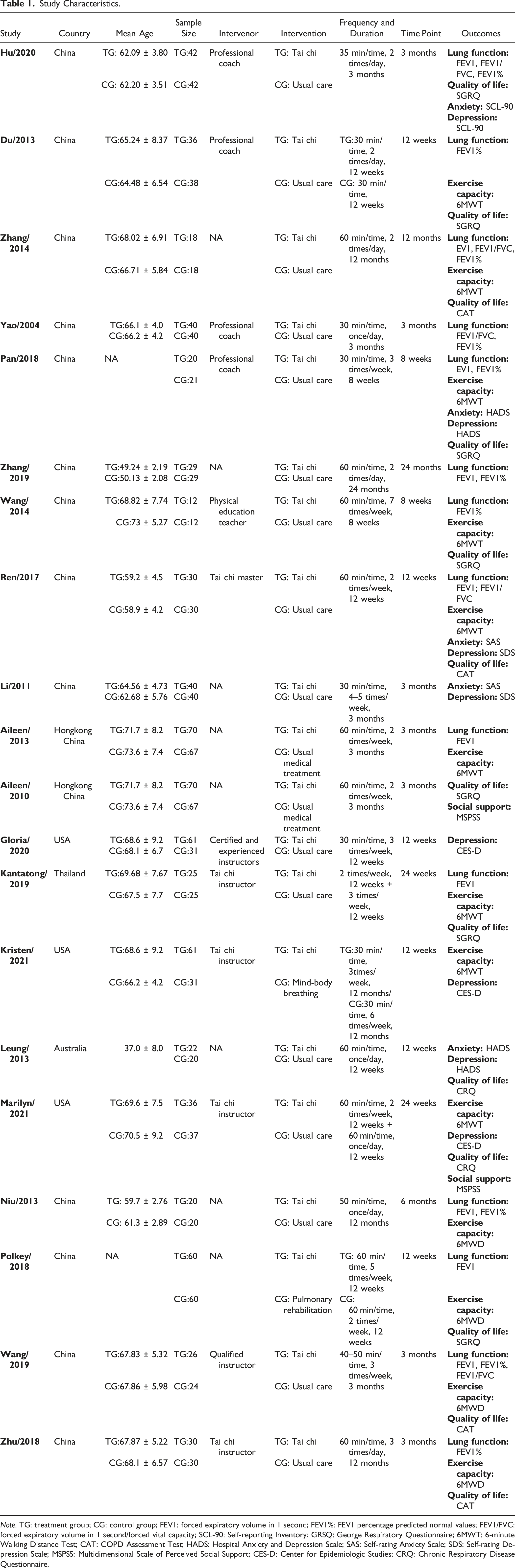
Note. TG: treatment group; CG: control group; FEV1: forced expiratory volume in 1 second; FEV1%: FEV1 percentage predicted normal values; FEV1/FVC: forced expiratory volume in 1 second/forced vital capacity; SCL-90: Self-reporting Inventory; GRSQ: George Respiratory Questionnaire; 6MWT: 6-minute Walking Distance Test; CAT: COPD Assessment Test; HADS: Hospital Anxiety and Depression Scale; SAS: Self-rating Anxiety Scale; SDS: Self-rating Depression Scale; MSPSS: Multidimensional Scale of Perceived Social Support; CES-D: Center for Epidemiologic Studies; CRQ: Chronic Respiratory Disease Questionnaire.
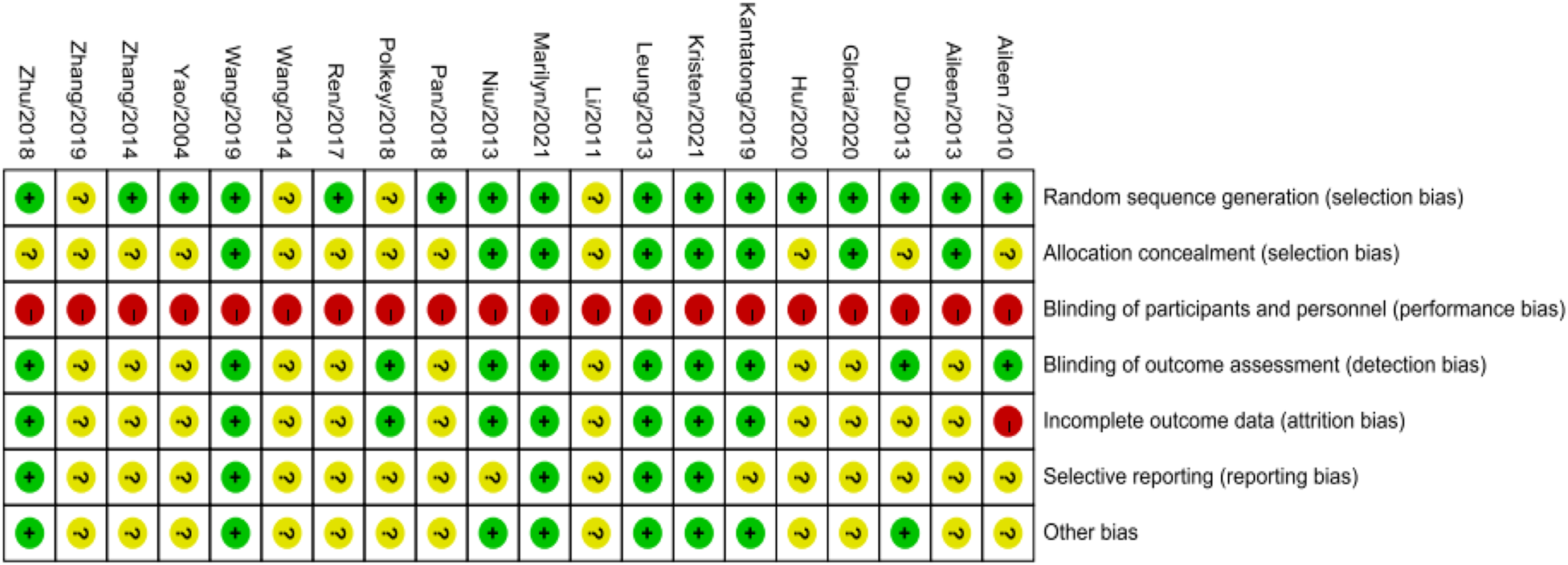
Risk of bias assessment.
Results of Meta-Analysis
The final values were used in our final efficacy analysis. The results of our analysis of each outcome were described below.
Lung Function
Ten trials including 665 patients evaluated the effects of tai chi on lung function using FEV1 (Chan, A. W. K. et al., 2013; Hu et al., 2020a; Kantatong et al., 2019; Niu et al., 2014; Pan et al., 2018; Polkey et al., 2018; Ren et al., 2017; Wang et al., 2018; Zhang et al., 2014; Zhang & Liu, 2019). The results indicated a significant difference between the tai chi and the control groups (MD = 0.12, 95% CI = 0.01 to 0.23, p = .03; I
2
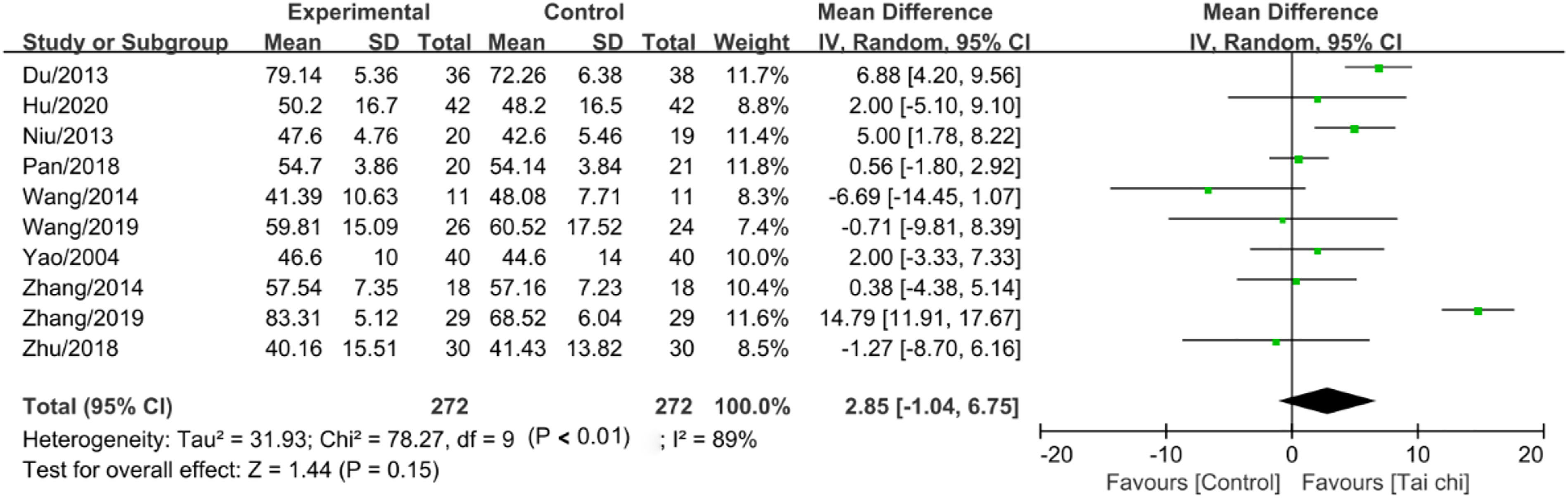
= 85%, p < .01) with a random-effects model (Figure 3). However, the different trends were observed about the FEV1 predicted value from 10 RCTs (Du et al., 2013; Hu et al., 2020b; Niu et al., 2014; Pan et al., 2018; Wang et al., 2014; Wang et al., 2019; Yao, 2004; Zhang et al., 2014; Zhang & Liu, 2019; Zhu et al., 2018) (MD = 2.85, 95% CI = −1.04 to 6.75, p = .15; I
2
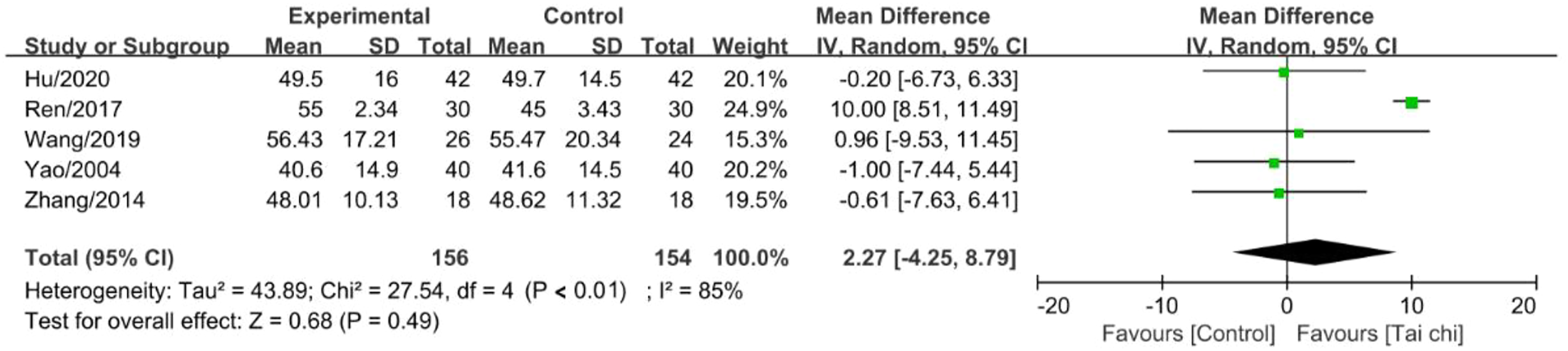
= 89%, p < .01) (Figure 4), and FEV1/FVC reported in five articles (Hu et al., 2020b; Ren et al., 2017; Wang et al., 2019; Yao, 2004; Zhang et al., 2014) (MD = 2.27, 95% CI = −4.25 to 8.79, p = .49; I
2
= 85%, p < .01) (Figure 5). The effect of tai chi intervention on FEV1. The effect of tai chi intervention on FEV1%. The effect of tai chi intervention on FEV1/FVC.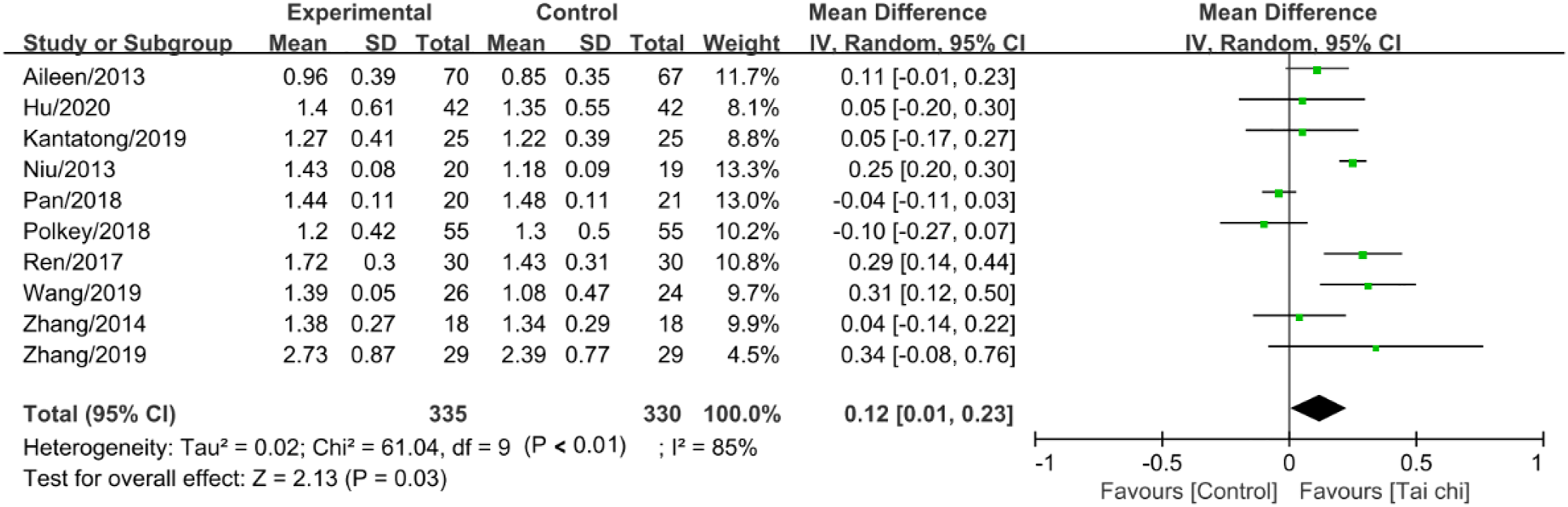
Exercise Capacity
Thirteen studies (Chan et al., 2013; Du et al., 2013; Kantatong et al., 2019; Kraemer et al., 2021; Moy et al., 2021; Niu et al., 2014; Pan et al., 2018; Polkey et al., 2018; Ren et al., 2017; Wang et al., 2014; Wang et al., 2019; Zhang et al., 2014; Zhu et al., 2018), involving 825 participants, assessed the benefits for exercise capacity measured by 6MWD. Because of inter-study heterogeneity (I
2
= 88%, p < .01), a random-effect model was performed. The data pooling revealed that tai chi can significantly increase the distance covered on the 6MWD compared to the control (MD = 34.6, 95% CI = 17.45 to 51.75, p < .01; I
2
= 88%, p < .01) (Figure 6). The effect of Tai chi intervention on 6MWD.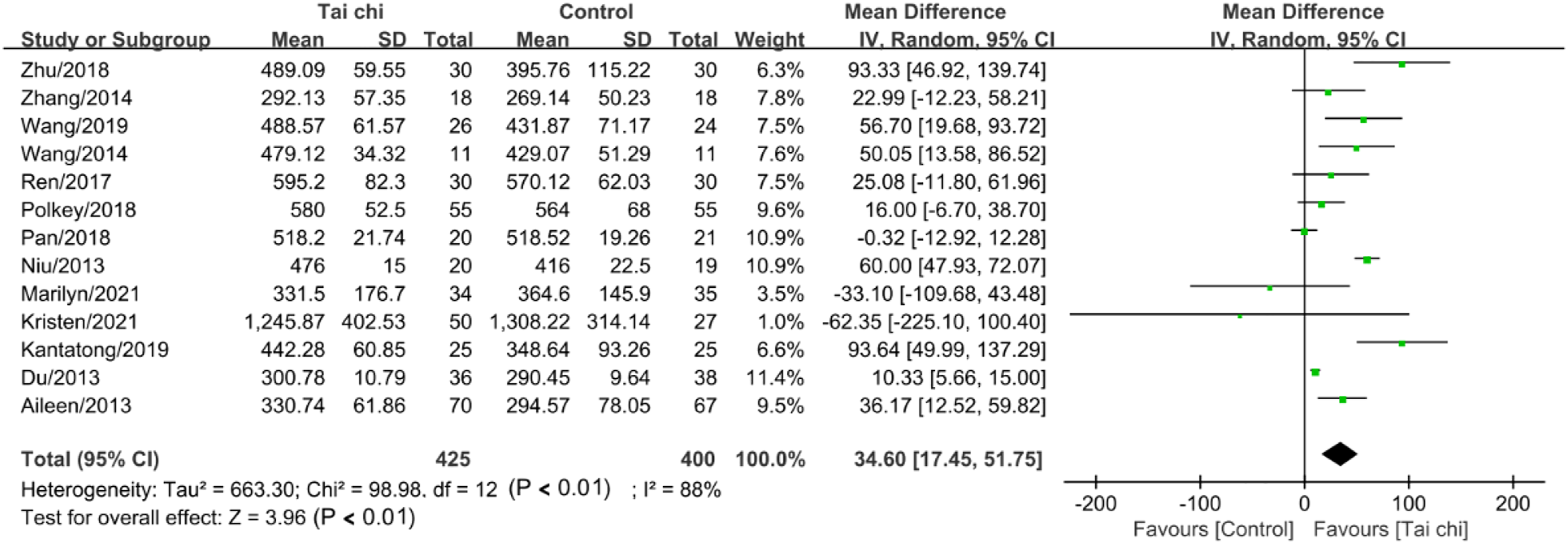
Anxiety
Five trials (Hu et al., 2020b; Leung et al., 2013; Li, 2011; Pan et al., 2018; Ren et al., 2017), including 303 participants, evaluated the effects on anxiety, measured by the Self-reporting Inventory (SCL-90), the Hospital Anxiety and Depression Scale (HADS), and the Self-rating Anxiety Scale (SAS). With a random-effects model, a significant difference in anxiety was observed (SMD = −0.69, 95% CI = −1.15 to −0.22, p < .01; I 2 = 73%, p < .01) (Supplementary material 2).
Depression
Eight trials (Hu et al., 2020b; Kraemer et al., 2021; Leung et al., 2013; Li, 2011; Moy et al., 2021; Pan et al., 2018; Ren et al., 2017; Yeh et al., 2020) with data from 530 participants assessed the effects on depression measured by SCL, HADS, SAS and the Center for Epidemiologic Studies (CES-D). With a random-effects model, pooled results in depression after tai chi intervention revealed no significant difference between groups (SMD = −0.57, 95% CI = −1.21 to 0.06, p = .08; I 2 = 92%, p < .01) (Supplementary material 2).
QoL
For QoL, three questionnaires were used to evaluate program effectiveness, including George Respiratory Questionnaire (SGRQ), Chronic Respiratory Disease Questionnaire (CRQ), and COPD Assessment Test (CAT). The collated differences from 13 RCTs (Chan, A. W. K. et al., 2013; Du et al., 2013; Hu et al., 2020b; Kantatong et al., 2019; Leung et al., 2013; Moy et al., 2021; Pan et al., 2018; Polkey et al., 2018; Ren et al., 2017; Wang et al., 2014; Wang et al., 2019; Zhang et al., 2014; Zhu et al., 2018) with 831 patients revealed significant difference between groups (SMD = −0.78, 95% CI = −1.20 to −0.37, p < .01; I 2 = 87%, p < .01), based on a random-effects model (Supplementary material 2).
Social Support
MSPSS (Multidimensional Scale of Perceived Social Support) was used to evaluate the level of social support in the included two articles (Chan et al., 2013; Moy et al., 2021). Significant effects were found from 206 data between groups (MD = −0.02, 95% CI = −0.51 to 0.48, p = .94; I 2 = 0%, p = .56), based on a fixed-effects model (Supplementary material 2).
Publication Bias and Sensitivity Analyses
Egger’s test was performed to determine publication bias from all the literature. The p value from the Egger is 0.77, which showed no publication bias exists in included trials. Sensitivity analysis was carried out by excluding individual trials one by one. Except for FEV1, no substantial modification for other outcomes in this review. Hence, the effects on FEV1 should be interpreted with caution. (Figure 7). Egger’s test of publication bias.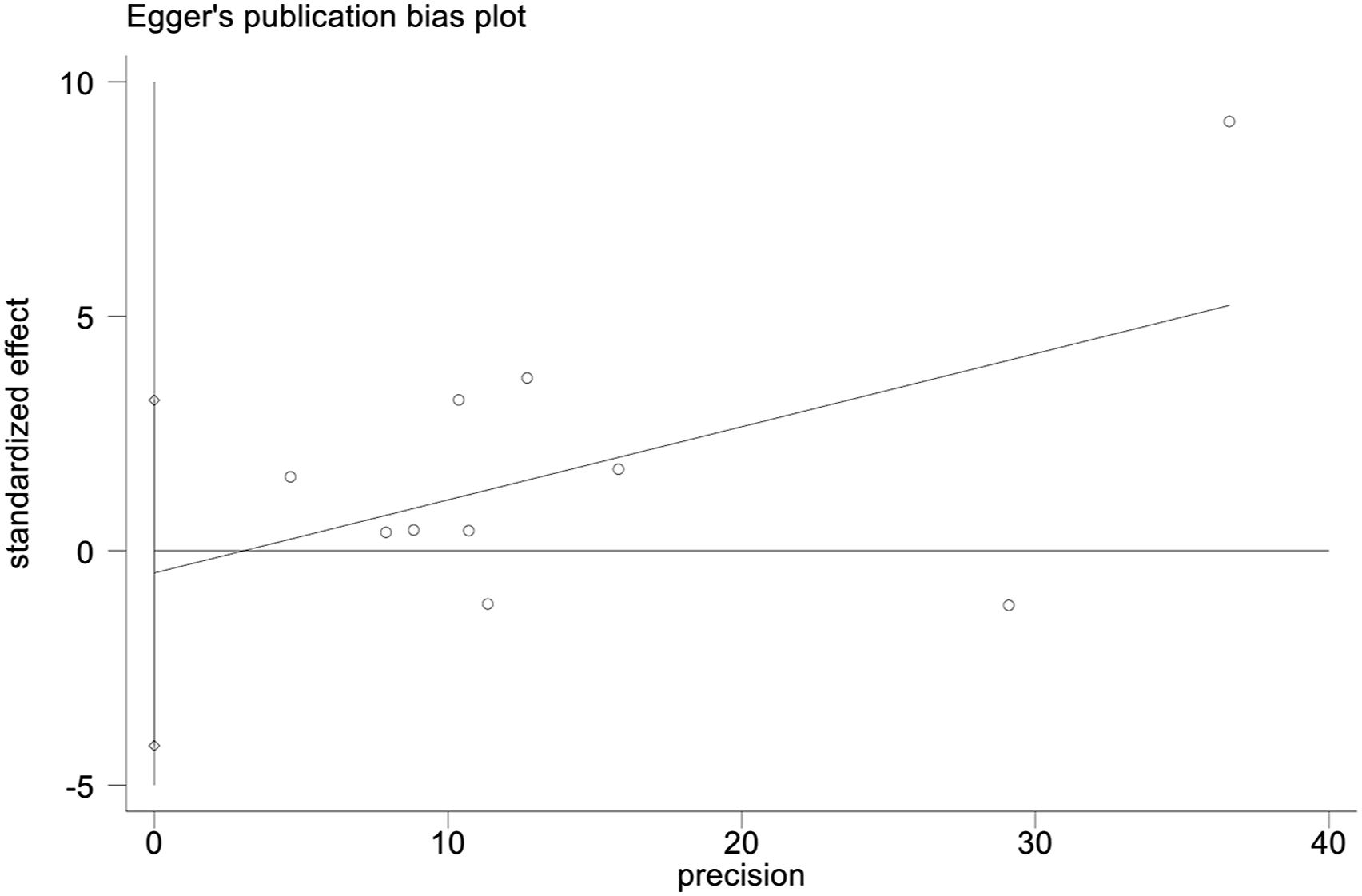
Discussion
This systematic review and meta−analysis aimed to analyze the RCTs on tai chi about its influence on lung function, exercise capacity, and psychosocial outcomes in patients with COPD. This systematic review involved 20 RCTs. In these, 1430 participants were randomly allocated to a tai chi group or a control group for minimum training of 8 weeks to maximum training of 24 months. By analyzing eligible studies, our pooled effect sizes showed that tai chi is a potential therapy for FEV1, 6WMD, anxiety, and QoL in patients with COPD. Healthcare staff could combine tai chi with usual medical care to optimize the management of COPD.
FEV1, FEV1%, and FEV1/FVC were used to reflect the lung function. The pooled results found that tai chi was beneficial for improving EFV1 in adults with COPD. This is in accordance with the conclusions of the previous Cochrane meta-analysis results conducted by Ngai et al., (2016). Nagi’s review including 4 studies with 570 patients also showed a significant improvement in FEV1 (p = 0.01) in patients with COPD after receiving tai chi. A possible explanation is that tai chi is a low-intensity, noncompetitive, and nonimpact exercise incorporating deep breathing into a body movement (Zhang et al., 2019). Repetitive deep breathing training draws the breath down into the lower tension (the main energy center of the body), increasing lung capacity and benefiting cardiorespiratory function (Chan, A. W. et al., 2013; Wang et al., 2019). However, no effects were observed on FEV1% and FEV1/FVC. As we only evaluated the effects on the post-intervention point, the improvement of lung function due to the pathophysiological process of COPD might not be demonstrable in short duration (Wu et al., 2018). Additionally, the limited number of RCTs included and differences in the characteristics of interventions could also affect the effects of intervention. Hence, it was still unclear whether improvements gained in lung function after tai chi intervention due to the variation of duration and doses of intervention. More RCTs are needed to reinforce the evidence of effects on lung function (Wu et al., 2018).
The 6MWT is a simple and valid evaluation parameter for assessing exercise capacity that measures the maximum distance covered in 6 min and is widely used in patients with COPD (Guyatt et al., 1985; Holland & Nici, 2013). In this meta-analysis, a statistically significant increase in 6MWD was observed in participants receiving tai chi compared with the control. This result was consistent with previously published reviews showing improvements in exercise capacity in patients with COPD (Wu et al., 2014). Tai chi should be in a semi-squatting position, and this may promote muscle endurance and further prolong exercise tolerance as reflected by longer distance capacity in 6MWT (Ngai et al., 2016).
Psychosocial outcomes are also a significant domain of disease management for patients with COPD (Yeh & Horwitz, 2017). This review showed significant effects of tai chi on anxiety and QoL. This is in line with research suggesting that tai chi may confer psychosocial benefits for patients with respiratory diseases (Philip et al., 2019; Wu et al., 2018). Previous evidence showed that patients with COPD found tai chi to be enjoyable, promoted exercise self-efficacy, removed psychosocial barriers to exercise (e.g., anxiety), and enhanced motion regulation processes (Yeh et al., 2010). Hence, an individual’s QoL is improved by removing negative emotions such as anxiety. A previous study also clarified that tai chi emphasizes the overall adjustment in patients with physical, mental, and psychological status, thereby contributing to further improvement in QoL for patients (Huston & Mcfarlane, 2016). However, there was also no significant improvement found in our review regarding depression and social support compared with the control group. Several factors such as insufficient required sample size, a small number of eligible RCTs, different styles and numbers of forms of tai chi adopted may partly explain the lack of significant findings.
Strengths and Limitations
Our study followed the guidelines for performing rigorous systematic reviews. Moreover, all included studies were RCTs, which reinforces the evidence of our results. We also proposed a rigorous screening and search strategy to identify the most comprehensive literature. Consequently, the results of our review are widespread belief. However, some limitations should also be mentioned in our review. First, grey literature and Google Scholar were not searched due to limited access to the website, leading to publication bias in our review. Second, tai chi intervention duration, frequency, and intensity were different between the intervention and control groups, affecting the reliability of the results. Third, we included articles published only in English and Chinese, leading to inclusion criteria bias. Fourth, since we only considered the immediate effects after tai chi intervention, the sustainability of intervention effects was not explored in our review. Therefore, pooled results in our review should be interpreted with caution given these limitations.
Conclusion
This meta-analysis further strengthened the support for the positive effects of tai chi on lung function, exercise capacity, and psychosocial outcomes in patients with COPD. Although existing included studies were limited, this review demonstrated the potential effects of tai chi on FEV1, 6WMD, anxiety, and QoL in patients with COPD, but not on FEV1%, FEVI/FVC, depression, and social support. More scientific and reasonable RCTs are warranted to confirm such positive effects of tai chi in COPD patients.
Supplemental Material
Supplemental Material - Effects of Tai Chi on Lung Function, Exercise Capacity and Psychosocial Outcomes in Patients With Chronic Obstructive Pulmonary Disease: Systematic Review and Meta-analysis of Randomized Controlled Trials
Supplemental Material for Effects of Tai Chi on Lung Function, Exercise Capacity and Psychosocial Outcomes in Patients With Chronic Obstructive Pulmonary Disease: Systematic Review and Meta-analysis of Randomized Controlled Trials by Ying Yang, Li Yang, Xuejin Yang, and Yuqi Tian in Biological Research For Nursing.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability
The protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO) network (PROSPERO CRD42023389695).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.