
Abstract
Introduction
More than half of transplanted kidneys do not last. Within 10 years after kidney transplant (KT) surgery, most kidney grafts from both deceased donors (46.4%) and living donors (30.4%) stop functioning (Hariharan et al., 2021). For those who experience failing kidney grafts, repeat KT is the preferred treatment option because it is still linked to superior health outcomes in comparison to renal replacement therapy (Sandal et al., 2023). However, patients must undergo a rigorous screening process because they are classified in the high-risk category with regard to the aim of graft success and patient survival after KT, and transplant programs often hesitate to perform kidney transplantation on these patients with numerous comorbidities and immunological risk due to the potential risks of being flagged for underperformance (Abecassis et al., 2009). In particular, increasing age and a greater burden of comorbidities in the setting of long-term immunosuppressant use superimposed on chronic kidney disease from grafts place these patients at risk of physical deterioration (De Smet & Van Craenenbroeck, 2021). This impaired physical condition resulting in a reduced ability to resist health stressors, leading to heightened vulnerability to negative health outcomes is defined as frailty (Fried, 2016).
Out of every 10 patients with end stage kidney disease, 7 suffer from frailty (Chowdhury et al., 2017), which ultimately lead to prolonged hospitalization (McAdams-DeMarco et al., 2017), readmission (McAdams-DeMarco et al., 2013), falls (Chu et al., 2020), or death (McAdams-DeMarco et al., 2015) after KT. One out of six patients referred for KT are considered to be frail (Haugen, Agoons, et al., 2020), and patients with impaired physical function are more likely to lose their eligibility for KT before being added to the waiting list (Haugen, Thomas, et al., 2020). The KT community has made an effort to objectively assess frailty (McAdams-DeMarco et al., 2023) and intervene (McAdams-DeMarco et al., 2019) on behalf of patients seeking an initial KT.
However, patients who fail kidney grafts and need dialysis are primarily managed by local kidney providers, resulting in reduced rigorous and regular follow-up by transplant programs and limiting the availability of information regarding their frailty. Data from the national transplant registry record physical function, defined by the ability to carry out the physical challenges encountered in daily activities, with Karnofsky scores for transplant recipients ranging from zero to 100. These scores are used by the Organ Procurement and Transplantation Network (OPTN) for all adult recipients as a surrogate measure of frailty. In light of these circumstances, the aim of the present study was to determine the impact of physical function on access to repeat KT by analyzing the dataset from the national registry.
Materials and Methods
Design and Sample
We examined data from kidney only transplant patients (N = 28,884) who were ≥18 years old and experienced failure of kidney grafts after undergoing KT from a deceased-donor or living-donor January 1, 2000, and August 31, 2015. Transplant recipients who had received multiple organs, such as also receiving a liver, heart, or pancreas, were excluded because the complexity of their health conditions is different from those of recipients of a kidney only. Additionally, we precluded those who died after the primary KT without undergoing a repeat KT, regardless of the cause of death or graft function at the time of death (e.g., death unrelated to graft function or death with a functional graft).
Measurements
The independent variables in this study included demographics (such as age, gender, race) and clinical information (including primary diagnoses of kidney failure, panel reactive antibodies, and physical function assessed by Karnofsky scores). The dependent variables comprised (1) access to the waiting list for second KT and (2) the time (in days) it takes for a patient to be re-listed after kidney graft failure.
Initially designed to measure the performance level of individuals with cancer (Karnofsky & Burchenal, 1948), Karnofsky scores are assigned by health-care providers’ in-person evaluation conducted in clinical environments and range from zero (death) to 100 (fully active without assistance). These scores predicted patient survival of 1–3 years after deceased-donor KT (Bui et al., 2019). For the present study, the physical function status measured by Karnofsky score was classified into three categories: zero to 40 (total assistance), 50 to 70 (some assistance), and 80 to 100 (no assistance) (Yoo et al., 2020).
Analysis
To summarize the patients’ clinical and demographic profiles, we indicated the continuous variables using the median and interquartile range (IQR) and sorted them into categories by creating another variable. Multivariate logistic regression analysis estimated the effect of individual covariates on access to the waiting list for repeat KT. We used Multivariate Cox proportional hazard regression to analyze whether there was the statistically significant difference in recipients’ duration to wait-listing post kidney allograft failure, based on covariates by calculating the proportional hazards. We conducted all analyses using R statistical software (R Core Team, 2023).
SRTR and IRB Statement
This study used data from the Scientific Registry of Transplant Recipients (SRTR). The SRTR data system includes data on all donor, wait-listed candidates, and transplant recipients in the US, submitted by the members of the Organ Procurement and Transplantation Network (OPTN). The Health Resources and Services Administration (HRSA), U.S. Department of Health and Human Services provides oversight to the activities of the OPTN and SRTR contractors.
Given that the study is retrospective and uses de-identified data from the national registry, it was determined that this research involved little to no risk and was approved as non-human research by the institutional review board (IRB) of the author’s affiliated institution.
The data reported here have been supplied by the Hennepin Healthcare Research Institute (HHRI) as the contractor for the Scientific Registry of Transplant Recipients (SRTR). The interpretation and reporting of these data are the responsibility of the author(s) and in no way should be seen as an official policy of or interpretation by the SRTR or the U.S. Government.
Results
Baseline Characteristics
Demographic and Clinical Characteristics and Adjusted Odds for Being Re-isted for Repeat KT.
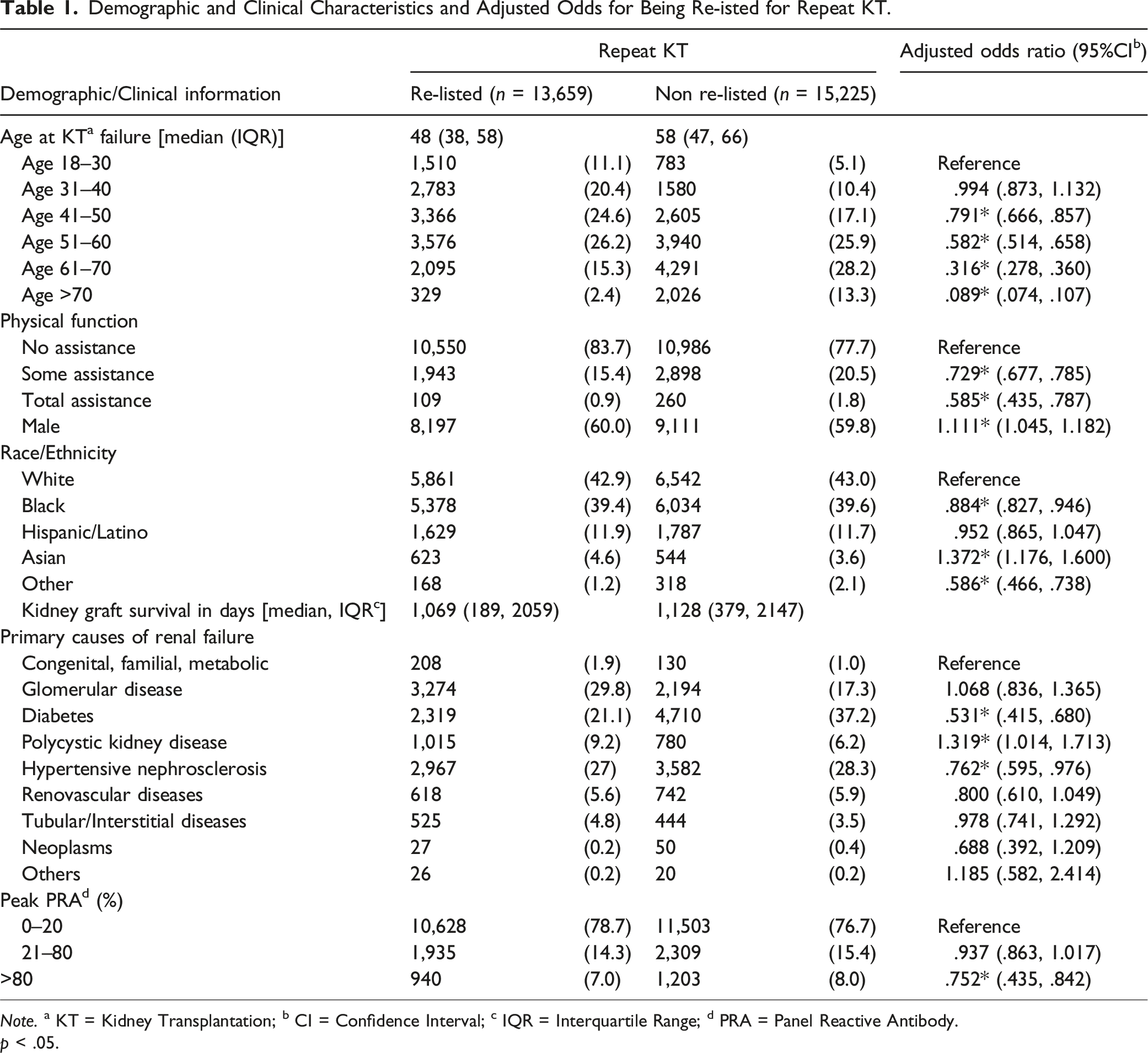
Note. a KT = Kidney Transplantation; b CI = Confidence Interval; c IQR = Interquartile Range; d PRA = Panel Reactive Antibody.
p < .05.
Table 1 indicates the patients’ clinical and demographic characteristics. And it also presented the adjusted odds ratios indicating the probability of being re-listed based on that patient profiles. Those patients re-listed lost their kidney grafts at a younger age compared to those not on the waiting list (48 years vs. 58 years; IQR = 38, 58 years). The median kidney graft survival duration was 3.1 years for patients not re-listed (IQR = 1.0, 5.9 years) and 2.9 years for those re-listed (IQR = 0.5, 5.6 years).
Most individuals in the two groups were White (42.9% [re-listed] vs. 43.0% [not re-listed]) or Black (39.4% [re-listed] vs. 39.6% [not re-listed]). The proportions of male patients were comparable between the two groups (60.0% [re-listed] vs. 59.8% [not re-listed]). For re-listed patients, glomerular disease was the leading cause of kidney failure (29.8%), followed by hypertension (27%). In contrast, diabetes was the primary reason for kidney failure among those who were not re-listed (37.2%). Peak panel reactive antibody (PRA) levels, indicating sensitivity, exceeded 80% in 940 re-listed patients and 1,203 non-re-listed patients.
Out of the entire sample (N = 28,884), Karnofsky scores were documented for 26,746 individuals before KT. Among re-listed candidates, 83.7% (n = 10,550) were fully independent, 15.4% (n = 1,943) required some assistance, and 0.9% (n = 109) needed complete assistance. For non-listed individuals, 77.7% (n = 10,986) were fully independent, 20.5% (n = 2,898) required some assistance, and 1.8% (n = 260) needed complete assistance.
Impacts of Physical Function on Access to the Waiting List
Probability of Being Re-listed
After adjusting for the covariates of age at kidney transplant (KT) failure, gender, race/ethnicity, primary diseases, and panel reactive antibody (PRA), the odds of being re-listed after kidney graft failure were higher for patients who were physically independent (Figure 1; Table 1). The data appeared to fit the logistic regression model well, according to the Hosmer–Lemeshow goodness-of-fit test (11.347, df = 8, p = 0.183). Effects of Clinical Characteristics on Access to Repeat Kidney Transplantation. Note. PRA indicated panel reactive antibody (peak level): a = PRA 0%–20%; b = PRA 21%–80%; c = PRA >80%.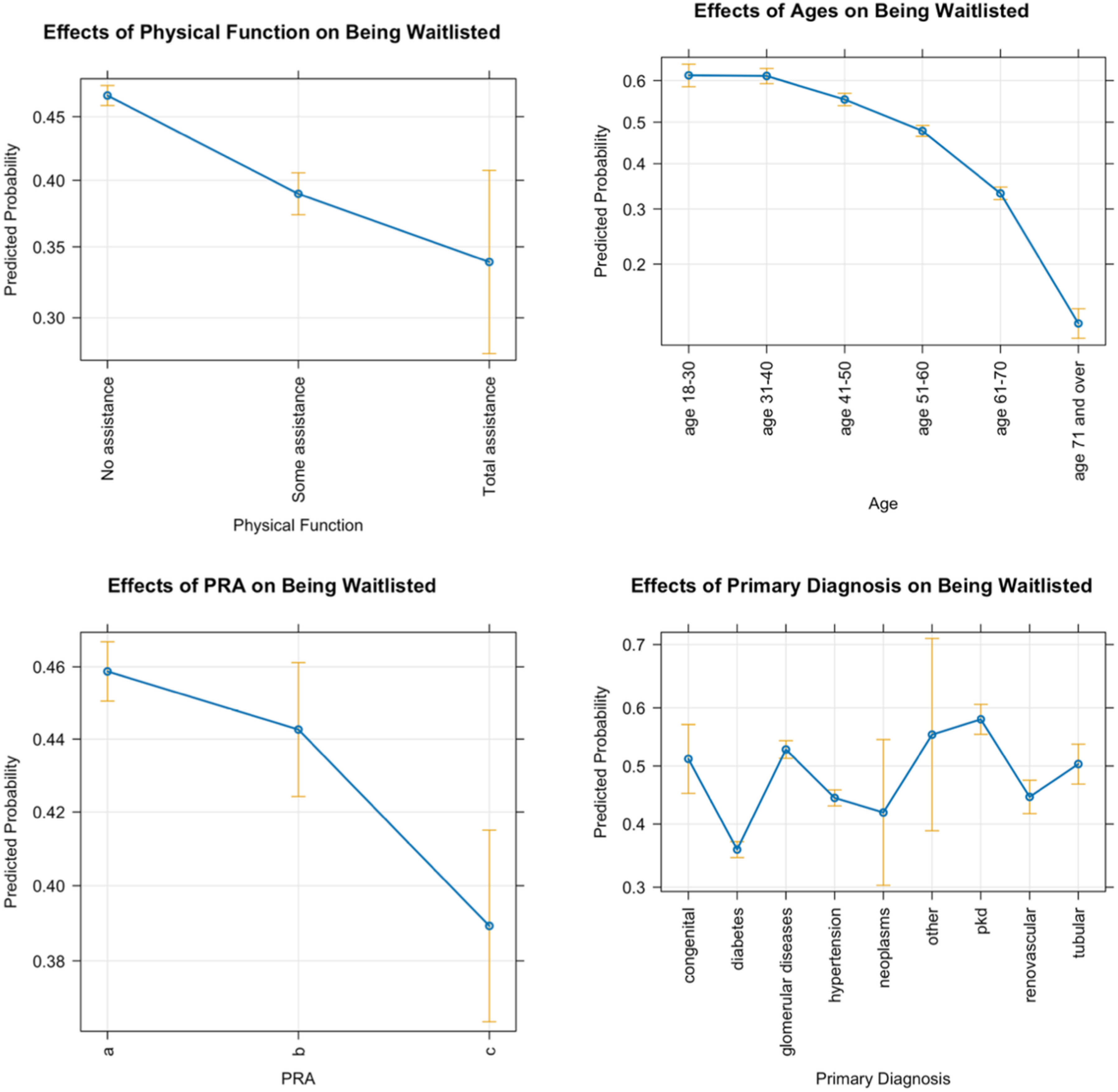
Time to Being Re-listed
The multivariate Cox proportional hazard model included physical function along with other risk factors (i.e., age at kidney transplant failure, gender, race/ethnicity, primary diseases, and PRA). Provided they remained in the work-up process, patients requiring total assistance were more likely to have a shorter time to re-listing for repeat KT compared to those needing no assistance (HR 1.54, 95% CI 1.19–2.00, p < 0.001), independent of all other factors (Figure 2). The hazard ratio for being re-listed was 1.11 (95% CI 1.05–1.18, p < 0.001) for those needing some assistance, indicating a 52% probability of being listed sooner if the patients continued in the evaluation process long enough. Forest Plot for the Multivariate Cox Proportional Hazards Model for Re-listing. Note. The plot illustrates hazard ratios and associated confidence intervals for re-listing, contingent upon remaining in the work-up process. It indicates the time until re-listing associated with covariates. Gender: F = female; M = Male. PRA = Panel Reactive Antibody. a = PRA 0%–20%; b = PRA 21%–80%; c = PRA >80%. Reason for Kidney Failure: PKD = polycystic kidney disease. *p < .05.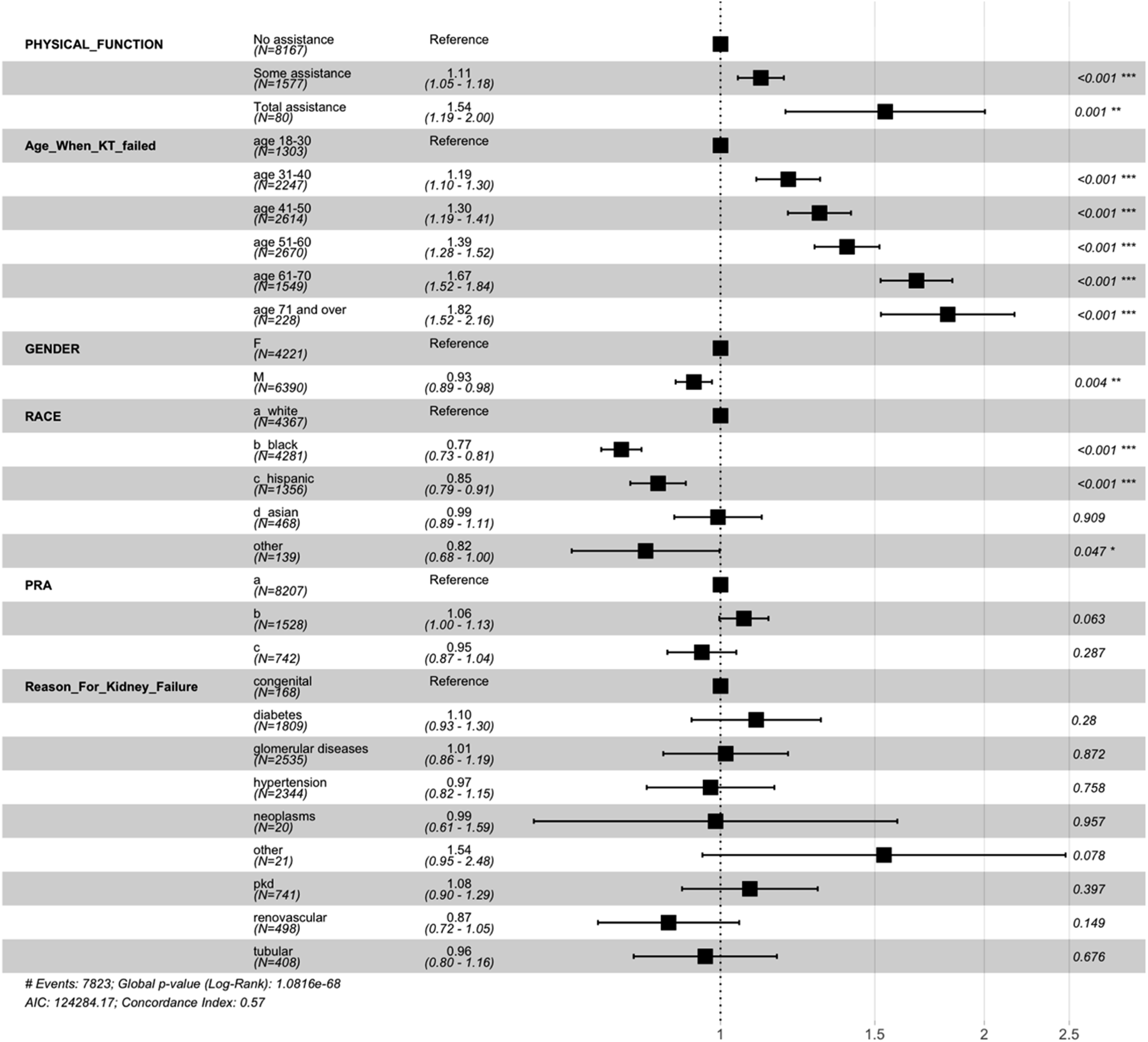
Discussion
In this study, we investigated whether the physical function of KT recipients impacts their access to repeat KT upon kidney graft failure. Our results show that only half of the patients were re-listed after kidney graft failure, and the odds of being listed were 41.5% lower for patients who needed total assistance than for those who did not need any assistance. The patients in need of some type of assistance had a 27% lower likelihood of being listed for repeat KT.
These study findings on patients wishing to undergo repeat KT are consistent with previous reports showing limited access to the waiting list among patients with suboptimal physical function wishing to undergo primary KT. Given the inferior transplant outcomes (e.g., prolonged hospital stays, graft dysfunctions, and death) arising due to compromised physical function (Quint et al., 2021), more than half of the transplant programs in the United States have implemented screening processes for physical function as a guide for determining transplant candidacy (McAdams-DeMarco et al., 2020). Accordingly, Haugen, Agoons, et al. (2020) found that patients with impaired physical function, as measured by the Short Physical Performance Battery, had a 30% lower possibility of being wait-listed compared to non-impaired patients. The authors also found that even when successfully wait-listed, patients with limited physical function had a 1.6-fold higher mortality while waiting for a KT. This finding was consistent with a report that KT candidates with low physical function, as defined by the Short Form Health Survey, were put inactive status on the waiting list and ineligible for KT (Reese et al., 2015). Thus, although patients might satisfy the criteria at their initial transplant evaluations and get wait-listed, they could become inactive on the waiting list or delisted from it if their physical conditions deteriorate while awaiting KT (Haugen, Thomas, et al., 2020; Reese et al., 2015). The association observed in the present study between physical function and the likelihood of access to KT after kidney graft failure could therefore reflect the fact that transplant programs, to avoid underperformance and scrutinization by the government, have increasingly hesitated to proceed with transplant surgeries for candidates deemed high-risk (Abecassis et al., 2009). Therefore, our study findings highlight the need to implement strategies to enhance and maintain optimal physical function throughout the kidney transplant journey to improve transplant outcomes and access to repeat transplantation.
Although a few studies have indicated that KT itself could improve functionality initially (Ali et al., 2021; Broers et al., 2019), its long-term influence on physical function remains controversial (Takahashi et al., 2018; Tsarpali et al., 2022). KT clearly improves quality of life (Tucker et al., 2019) and prolongs the life expectancy of patients with kidney failure (Chaudhry et al., 2022; Strohmaier et al., 2022). Nevertheless, enhancing physical function throughout the post-transplantation period has often been neglected or underemphasized (Berben et al., 2019) for several possible reasons. One is that nerve damage caused by the self-retaining retractors used in the operation may cause lower extremity weakness immediately after surgery (Yamada et al., 2020). Neuropathic disorders that lead to weakness may also arise due to perinephritic hematoma, hypotension during transplant surgery, cold exposure caused by ice in the iliac fossa area, and prolonged iliac artery occlusion (Li et al., 2010). Another reason is that immunosuppression-related drugs, such as calcineurin inhibitors, can also have neurotoxic effects that can cause functional disorders (e.g., tremor, neuralgia, and peripheral neuropathy) and result in patient dependence on caregivers (Farouk & Rein, 2020). Similarly, the long-term use of immunosuppressive steroids is known to cause functional disorders associated with osteoporosis and bone fractures (Batteux et al., 2020; Vangala et al., 2018). Other factors can include gastrointestinal symptoms, such as nausea, vomiting, or diarrhea, which are also common during the post-transplantation period (Davies et al., 2007) and can cause dehydration, weakness, and overall diminished physical function. Similarly, acute or chronic anemia post-KT can cause fatigue and general body weakness and can lead to a high ratio of graft failure and death (Schechter et al., 2019). Furthermore, underlying chronic kidney disease from a renal graft is related to bone weakness and muscle atrophy (Kasiske et al., 2011), while post-KT depression could also be related to chronic fatigue and create a lack of motivation for physical activity (Bossola et al., 2021; Srifuengfung et al., 2017).
Therefore, to prevent physical function deterioration after KT, we recommend that the transplant community employ a few simple strategies. As a first approach, during the post-transplantation course, transplant providers and nurses should share realistic outcomes, particularly regarding the life expectancy of transplanted kidneys. This approach can help patients avoid discouragement when informed of the potential need for repeat KT; instead, they can be prepared for it as they age, especially since evidence supports the benefits and satisfactory outcomes of KTs in elderly patients. For example, previous studies have shown improved quality of life (de Boer et al., 2024), a one-year graft survival rate of up to 92.6% (Mehta et al., 2023), and a reduction in mortality to as low as 41% (Rao et al., 2007) in elderly patients post-KT. Furthermore, patients aged ≥65 years who underwent repeat KT have had comparable graft survival when compared with the same age group of patients receiving their first KT (Heldal et al., 2017). Most importantly, survival rates were better for KT patients than for patients who remained on dialysis treatment.
As a second step, the KT community should continue to emphasize and implement strategies that enforce physical function in post-KT patients. Immediately after kidney transplant surgery, patients may misguidedly limit their physical activity due to the fear of harming their kidney grafts (Suet-Ching Luk, 2004). Also, a survey conducted after transplant surgery indicated that 76% of kidney transplant recipients lead sedentary lifestyles (Gordon et al., 2010), and one study of kidney recipients found that 48.4% (n = 2,933) reported being physically inactive during long-term follow-ups extending up to ten years (Masiero et al., 2020).
According to a review by Takahashi et al. (2018), exercise programs are likely to be effective in improving overall cardiorespiratory fitness indicators and quality of life among KT recipients. Another study reported that KT patients who performed aerobic exercise and physical therapy immediately after KT showed improved 6-min walking distance and knee extensor strength without injuring their kidney grafts (Yamamoto et al., 2020). Yamaguchi et al. (2024) reported significant increases in the Short Physical Performance Battery score and knee extensor strength throughout a one-year rehabilitation period. Despite the relatively small sample sizes of these studies, their findings all underscore that the transplant community should emphasize the need for interventions to increase physical activities and physical function in patients who undergo KT.
Interventions are also needed to protect patients from worsening frailty after a return to dialysis and while on the waiting list for a repeat KT. Prehabilitation has been highlighted for its potential effectiveness in increasing the physical activity levels of patients on the waiting list and reducing the length of hospital stay after KT surgery (McAdams-DeMarco et al., 2019). However, a center-based exercise program, such as the one demonstrated in the present pilot study, might not be flexible enough to accommodate the diverse dialysis modalities (e.g., hemodialysis/peritoneal dialysis, treatment schedule, and treatment duration) of all patients, and could lead to lower participation and sustainability. In contrast, a home-based exercise regimen that includes both aerobic walking and resistance training, together with ongoing feedback from health care providers, could be a flexible and alternative option that would mitigate or prevent frailty in patients diagnosed with end-stage renal disease who are seeking a new KT (Yoo et al., 2022).
One concern raised by our secondary findings was that patients who were younger, male, Asian, or diagnosed with polycystic kidney disease were more likely to be wait-listed for a repeat KT, whereas Black patients or individuals with diabetes were less likely to receive a repeat KT. These results align with a previous study by Schold et al. (2020), who documented lower rates of preemptive re-listing or transplantation among the elderly, Black patients, or individuals with diabetes. Although the primary goal of the transplant community is to achieve equitable access to KT and transparency in the transplant process (Kizer et al., 2022), evidence continues to highlight disparities in KT access among historically marginalized populations, such as Black and female patients. Despite their higher susceptibility to kidney failure, Black patients are less likely to undergo kidney transplantation (Purnell et al., 2018). Recent updates to kidney function calculation have removed race coefficients and now aim to expand eligibility for KT among Black patients (Zelnick et al., 2021). However, barriers such as social determinants of health (e.g., neighborhood, knowledge, financial constraints) (Li et al., 2024) and mistrust persist (Boulware et al., 2021; Harding et al., 2017). Community outreach to promote living donor KT (Boulware et al., 2013) or a transplant program designed for improving racial equity (Taber et al., 2023) to build trust can potentially reduce this disparity in access to KT.
Women also face challenges in receiving repeat KT, a finding that contrasts with research published by Schold et al. (2020), who assessed outcomes in a distinct study cohort focusing on preemptive relisting and different time frames. Factors such as serving as primary caregivers, lower incomes leading to lower socioeconomic status, and limited health literacy (Salter et al., 2014) likely contribute to this gender disparity. Kidney providers can play a crucial role by offering tailored education and advocating for financial support for women with kidney failure (Natale et al., 2023). While addressing equitable access to KT falls beyond the scope of our present study, future research should explore whether these populations face greater disadvantages for getting a repeat KT due to limited physical functions that may lead to exclusion from transplant eligibility.
Our findings also showed that individuals with diabetes are less likely to be put on a transplant waiting list for a repeat KT, whereas individuals with polycystic kidney disease (PCKD) often have a higher probability of being wait-listed. This discrepancy may stem from the higher rates of complications, such as peripheral or cardiovascular diseases, experienced by patients with diabetes (Dolla et al., 2020). Conversely, those diagnosed with PCKD may exhibit relatively better physical resilience due to their lower rates of comorbidities (Bhutani et al., 2020), and may therefore benefit from increased access to repeat KT.
One surprising finding from our study was that patients requiring total assistance had a shorter duration before being re-listed compared to those requiring no assistance, provided that they remained in the evaluation phase long enough. Additionally, the hazard ratios for being listed increased with increasing patient age; for instance, patients aged 71 years or older had an HR of 1.82 (95% CI 1.52–2.16). One potential explanation for this observation is that transplant programs may expedite evaluations to determine candidacy earlier and prevent deterioration of physical function, particularly in patients deemed potential candidates who require repeat KT. Evidence indicates that implementing a specialized waiting list management program, such as the Transplant Readiness Assessment Clinic, can expedite access to KT by activating patients on the waiting list through comprehensive evaluations, including psychological and physical assessments, together with patient education (Cheng et al., 2018). This proactive approach, which aims to expedite wait-listing and the activation of wait-listed patients, can particularly benefit those awaiting repeat KT who are at risk of frailty. This approach could significantly benefit elderly individuals (aged ≥65 years), who are projected to constitute 61% of patients diagnosed with end-stage renal disease by 2030 (McCullough et al., 2019).
Our study has limitations that should be noted. First, we excluded KT recipients who expired following their initial transplantation without undergoing subsequent re-transplantation, regardless of the cause of death or graft function at the time of death (e.g., death unrelated to graft function or death with a functional graft). Consequently, we may possibly have inadvertently omitted individuals who were ultimately not re-listed due to their frailty and subsequent death. Second, the SRTR dataset is missing a significant amount of information. For example, among the total 28,884 patients, 2,138 (7.4%) had missing Karnofsky scores. We treated any missing information as randomly missing data and used a listwise deletion method. This study had a large sample size; therefore, we believe that we did not lose the ability to examine associations between the independent and dependent variables. However, given the transplant community’s advantage of nationwide information about all donors, candidates, and recipients collected on predetermined forms and entered by the staff of transplant teams, the accuracy of data analyses would benefit from diligent and more rigorous data entry to ensure inclusion of complete information.
A third limitation is that the OPTN required transplant programs to record Karnofsky scores for all adult KT candidates and recipients. The Karnofsky measure has therefore become a surrogate marker for assessing frailty and physical function in organ transplant candidates and recipients (Cheng et al., 2019; Shamseddeen et al., 2021). However, its reliability and validity, specifically for KT patients, have been subject to debate. Originally developed in 1949 for oncology patients, the Karnofsky score evaluates an individual’s ability to participate in normal activities and their dependence on assistance from others (Karnofsky et al., 1948). An important point to note, however, is that functional status is a broad concept that is affected not only by physical function but also by cognitive impairment (Martin et al., 2015), psychological conditions such as depression or anxiety (Mahlaq et al., 2023), and the severity of pain (Lin et al., 2003). Patients with chronic kidney disease and end-stage renal disease commonly experience both cognitive dysfunction and emotional stress (Kim et al., 2022; Tuna et al., 2021), which can result in a low functional status despite intact physical function.
Most importantly, physical function is only one dimension of frailty. Frailty is a syndrome that consists of multiple dimensions: physical/cognitive function, and psychosocial aspects (Chen et al., 2014). The measurement of physical function is relatively easy and clinically practical, and it has therefore become a surrogate measure of frailty (O’Hoski et al., 2020). However, a few studies have warned that Karnofsky scores are not an accurate measurement of frailty (Parala-Metz et al., 2023; Stedman et al., 2021). Therefore, a pressing need remains to develop and identify an accurate tool for measuring frailty that is agreed on by the transplant community (Kobashigawa et al., 2019; McAdams-DeMarco et al., 2023). Furthermore, Karnofsky scores are provider-driven scales; consequently, the inter-rater reliability is significantly low (Stedman et al., 2021). In addition, the recorded Karnofsky scores may not accurately reflect the latest physical function right before transplant surgery, as they are usually documented during transplant evaluation and subsequent follow-up appointments.
A further limitation was that although we controlled for primary demographic and clinical characteristics, we might have overlooked other confounding factors in this study. For example, patients with strong support systems (such as family or community) may overcome limitations and become more suitable candidates (Ladin et al., 2019). Given this study’s retrospective design, we cannot establish causal relationship between physical function and access to repeat KT. Furthermore, we might have underestimated the sample size as some patients may have received a repeat KT from the living donors without being listed.
In conclusion, this study underscores the influences of physical function on both the likelihood of being re-listed for a repeat KT and the time it takes for a patient to be re-listed after experiencing kidney graft failure. Almost half of KT recipients experience kidney graft failure and require repeat KT if they want to avoid dialysis therapy, especially given that the health benefits of repeat KT are superior to a return to dialysis. Therefore, kidney transplant providers and nurses should encourage and foster physical activities throughout the kidney transplant process to enhance physical function and access to repeat KT, with the ultimate goal of improving health outcomes for our kidney transplant community.
Footnotes
Author Contributions
Yoo, J contributed to conception and design contributed to acquisition drafted manuscript critically revised manuscript gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent Statements
On 5/6/2024, Rush University IRB acknowledged that this study does not meet the definition of human subject research therefore, informed consent was not necessary. Data Use Agreement was approved by Scientific Registry of Transplant Recipient on 5/24/2024. The manuscript was reviewed and approved on behalf of the Health Resources and Services Administration representative on 5/30/2024.
Data Availability Statement
The data reported in this study are available upon reasonable request to the corresponding author.