
Abstract
Preterm infants experience frequent stressors that activate the hypothalamic-pituitary-adrenal (HPA) axis. Cortisol can be readily quantified in saliva samples, but sufficient saliva volumes are difficult to collect from preterm infants. We report the development and validation of a novel method to collect saliva using flocked polyester swabs and the application of this method in a study of preterm infants. Saliva samples, collected from adult participants (N = 24), were divided and processed as “standard” aliquots and aliquots absorbed by and extracted from flocked polyester swabs. Cortisol levels in “standard” and “swab” aliquots were compared. We then collected saliva samples from preterm infants (N = 31) using flocked polyester swabs to measure HPA responses to routine, clustered nursing care. Saliva samples were collected from each infant prior to caregiving, 30-min after caregiving, and 60-min after caregiving. Aliquots from the same adult were highly correlated. Sufficient volumes of saliva were extracted from 91 of 93 infant swabs (98%). Changes in cortisol levels from baseline to 30-min and 60-min after caregiving were negatively associated with acute procedural stress, quantified using the Neonatal Infant Stressor Scale. The change in cortisol level from baseline to 60-min after caregiving was negatively associated with caregiving duration. Further research is needed to understand the relationship between caregiving stress exposure and HPA axis responses in preterm infants and to identify the myriad factors that may influence this association. Flocked polyester swabs offer a viable option for the collection of sufficient volumes of saliva to support this research.
Introduction
Preterm infants born <32 weeks gestational age (GA) experience repeated, frequent stress exposure during lengthy hospitalizations in the neonatal intensive care unit (NICU). This stress occurs during a sensitive period of brain development and can result in abnormal programming of the stress response systems (Lavanga et al., 2020; McLean et al., 2023), altered brain structure and function (Boggini et al., 2021; Lavanga et al., 2020), and poor neurodevelopmental outcomes (Coviello et al., 2018; Valeri et al., 2015). Although stress exposure in the NICU is most commonly operationalized as counts of invasive or skin-breaking procedures (van Dokkum et al., 2021), the seemingly benign caregiving activities included in routine nursing care, which occurs frequently (Cameron et al., 2007; Cong et al., 2017), also elicit physiologic stress responses in preterm infants (Cistone et al., 2024; Griffiths et al., 2021). Routine nursing care includes activities of daily living (e.g., diaper change, bathing, feeding), general monitoring (e.g., assessment of vital signs), and activities addressing clinical needs (e.g., suctioning, feeding tube insertion, blood collection), some of which are highly invasive procedures (e.g., heel lance, endotracheal suctioning). Routine nursing care is often provided as “clustered” care, a caregiving episode that includes multiple activities administered on a predefined schedule and typically occurring every 3-4 hours during hospitalization (Holsti et al., 2006). While any routine caregiving activity can be stressful, clustered care may elicit a more intense stress response (Allinson et al., 2017; Brashear et al., 2023). Thus, understanding how routine, “clustered” nursing care affects physiological stress responses in preterm infants is important foundational knowledge for future interventions to improve outcomes.
Stressors disrupt homeostasis, resulting in activation of the hypothalamic-pituitary-adrenal (HPA) axis and release of cortisol (Johnson et al., 1992). Although most cortisol found in blood is bound in its inactive state to corticosteroid-binding globulin or albumins, unbound cortisol is physiologically active and is critical in maintaining the energy requirements of a time-limited stress response (Bozovic et al., 2013; Johnson et al., 1992). Inconsistent HPA responses to stressors have been observed in preterm infants and may depend on contextual factors (Cañadas et al., 2021; Morelius et al., 2016), the infant’s gestational age at birth (D’Agata et al., 2019; Howland et al., 2017), prior exposures to endogenous or exogenous glucocorticoids during the fetal and/or neonatal periods (Finken et al., 2016; Howland et al., 2017), and HPA axis immaturity that causes relative adrenocortical insufficiency (Finken et al., 2016). Further research is needed to more fully understand HPA axis responses in preterm infants.
Unbound serum cortisol passes by simple diffusion into saliva, which can be noninvasively collected and quantified (Bozovic et al., 2013), making salivary cortisol an attractive way to assess HPA axis activity following NICU stress exposures (Morelius et al., 2016). However, collecting sufficient volumes of saliva from preterm infants can be difficult even with extended collection periods (5–10 minutes), resulting in missing samples (Morelius et al., 2016; Neu et al., 2007) and, potentially, biased results. Thus, novel methods of saliva collection requiring short collection periods and minimal processing are needed.
Commercially available flocked polyester swabs designed to absorb and release samples are ideal for buccal cell, forensic, DNA, and other specimen collections (Thermo Fisher Scientific, Inc., 2025). In a study comparing the efficiency of various swab materials for environmental monitoring, flocked polyester swabs exhibited superior performance to foam, cotton, and flocked nylon swabs (Kumarajith et al., 2024). However, flocked polyester swabs are untested for saliva collection from preterm infants. Moreover, the ability to recover absorbed saliva and potential interference of the swab with analysis of cortisol are unknown.
In this paper, we describe (1) an initial validation study of flocked polyester swabs to collect saliva and analyze extracted cortisol and (2) a research application of the saliva collection protocol to quantify salivary cortisol in preterm infants. The aim of the validation study was to determine the correlation of cortisol obtained by standard saliva collection (i.e., passive drool or spit) and that absorbed by and extracted from flocked polyester swabs. The aim of the application study was to examine the relationship between stress exposure during routine nursing care and salivary cortisol responses in preterm infants.
Materials and Methods
Validation Study–Flocked Polyester Swabs
Study Design and Sample
Validation testing of the flocked polyester swabs was conducted using a cross-sectional, correlational study design with adult participants recruited by convenience sampling. Adult volunteers provided a saliva sample by drooling or spitting (i.e., standard collection procedures) into a laboratory tube. We quantified cortisol concentrations in two aliquots derived from each saliva sample. One aliquot was used to test the flocked polyester swabs, mimicking the collection procedure for preterm infants. The other aliquot was not subjected to further processing and, thus, represented the standard collection procedure. Participants were included if they were at least 18 years old and able to provide verbal consent for their own participation. There were no exclusions.
Measures
We quantified cortisol in undiluted saliva samples using Salimetrics Expanded Range High Sensitivity Salivary Cortisol Enzyme Immunoassay (ELISA) kit (1-3002, Salimetrics, LLC., Carlsbad, CA). Salimetrics’ cortisol ELISA quantifies salivary cortisol within a range of 0.012-3000 µg/dl and sensitivity <0.007 µg/dl (Salimetrics, 2025). High and low controls provided by the manufacturer were included for quality control, and samples were analyzed in duplicate according to the manufacturer’s instructions. Plates were read at 450-nm with a 490-nm correction filter using a BioTek Synergy LX microplate reader (BioSPX, Brussels, Belgium). The intra-assay coefficients of variation (CV) for the two plates used to quantify cortisol were 7.1% and 7.2%. The R2 values for standard curves were .997 and .9998.
Procedure
We recruited participants in the lobby of a local college building in March 2024. Consenting participants provided a 1-2 ml drool or spit saliva sample behind a privacy screen. After collection, samples were immediately placed on ice until all samples were collected and processed.
On the same day that samples were collected, they were divided into “standard collection” and “swab” aliquots in the lab. After briefly vortexing, the volume of each sample was measured using a serological pipette. One-half the volume was dispensed into a clean 2-ml microcentrifuge tube using a serological pipet. These aliquots were labeled as “standard collection”. The remaining half of each saliva sample was dispensed back into its original collection tube. We inserted one Puritan HydraFlock Swab (22029660, Fisher Scientific, Waltham, MA) into each collection tube until the swab was fully saturated with saliva. Using a 24ga needle, we punctured a hole in the bottoms of 0.6-ml snap cap microcentrifuge tubes. Each saturated swab tip was cut and placed in a punctured tube that was then capped and inserted into a clean 2-ml microcentrifuge tube. Because the 2-ml tube caps would not close over the inserted 0.6-ml tubes and to prevent breakage in the centrifuge, we cut the tops off the 2-ml tubes (Figure 1). After all samples were similarly processed (∼30 minutes), the tubes were centrifuged at 18,000 x g for 10 minutes at room temperature to extract saliva from the swabs. Following centrifugation, the 0.6-ml tubes and swab tips were removed and discarded. Extracted saliva was transferred to clean microcentrifuge tubes and labeled as “swab” aliquots. The “standard collection” and “swab” aliquots were stored at −20°C until analysis. “Standard collection” and “swab” aliquots were analyzed simultaneously on two ELISA plates. Aliquots from the same participant (i.e., same original saliva sample) were analyzed on the same plate. Procedure for extracting saliva from swabs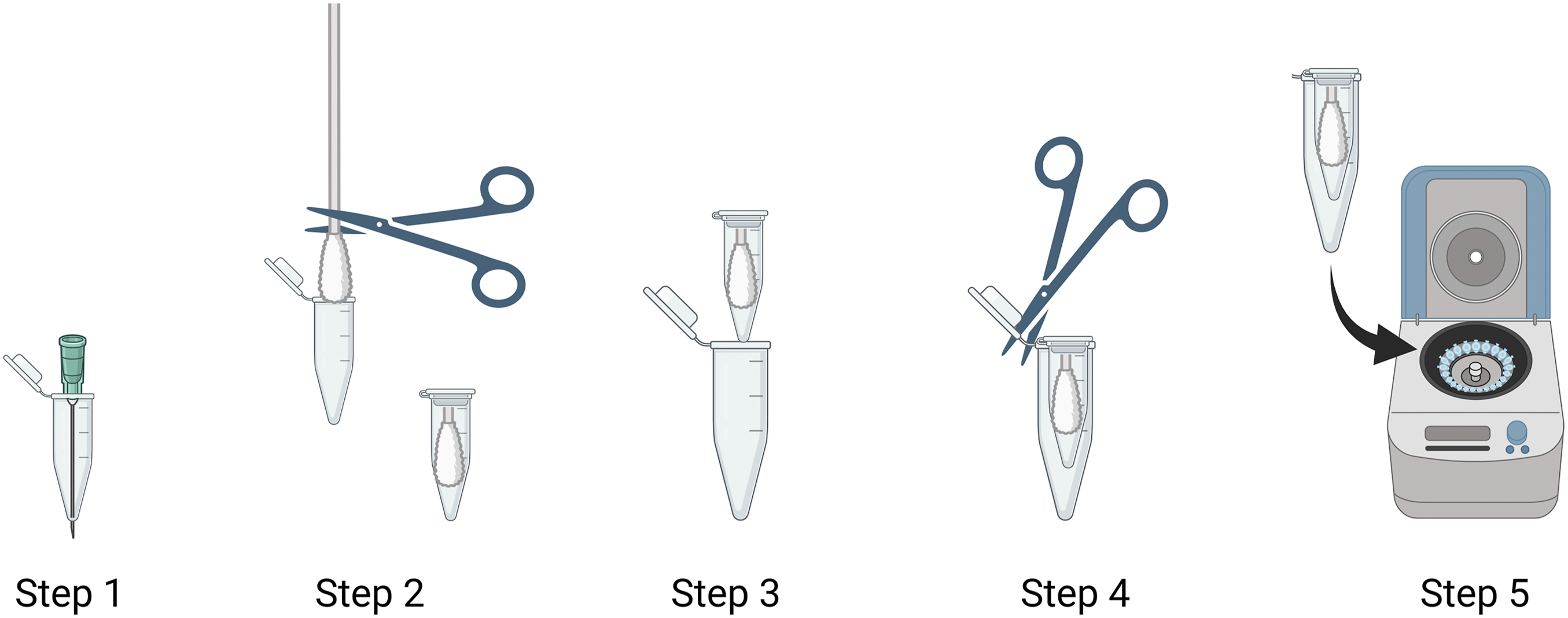
Ethical Considerations
The university’s institutional review board (IRB) approved the protocol under expedited review. Because other identifying information was not collected from participants and the consent form would be the only participant identifier, the IRB waived the requirement for written documentation of consent. A member of the study team read a script outlining the study procedures, risks, and benefits, and participants provided verbal consent before providing saliva samples.
Statistical Analysis
We examined the agreement between cortisol analyzed from “standard collection” samples and cortisol analyzed from “swab” samples using a Bland-Altman plot with the 95% limits of agreement and with the estimated intraclass correlation coefficient (ICC) (Ranganathan et al., 2017). Statistical analyses were conducted using Stata (version 18.5).
Application Study–Salivary Cortisol Responses in Preterm Infants
Study Design and Sample
The saliva collection procedure was applied in a non-experimental, cohort study of preterm infants in the NICU. Stress exposure was operationalized as (1) acute procedural stress, and (2) caregiving duration. Stress responses were operationalized as changes in salivary cortisol from baseline to post-caregiving (30-min after caregiving) and following a recovery period (60-min after caregiving) in accordance with the most common collection times in preterm infants to account for the delay in HPA axis responses to stressors (Morelius et al., 2016).
Infants born 27–31 weeks GA were recruited during their first week of life from a neonatal network in a large Midwest city. We included infants born within this narrow age range to limit variance in cortisol attributable to gestational age. Infants were eligible for the study if they had an English-speaking parent who was able to provide informed consent. Infants were excluded if they required inotropic therapy for cardiovascular instability; had congenital or chromosomal anomalies affecting sensory or motor functioning (i.e., neural tube defects, trisomy); had neurologic injuries (i.e., grade III or IV intraventricular hemorrhage, periventricular leukomalacia, hypoxic ischemic encephalopathy); or were administered steroids, sedatives, muscle relaxants, or narcotic analgesics within 48 hours of data collection. We sought to enroll 30 preterm infants to detect a moderate correlation (0.5) between stress exposure and salivary cortisol with 80% power and p < .05.
Measures
Neonatal Infant Stressor Scale (NISS)
Neonatal Infant Stressor Scale (NISS) Acute Stress Items Experienced by Preterm Infants (N = 30) and Item Intensity Weights
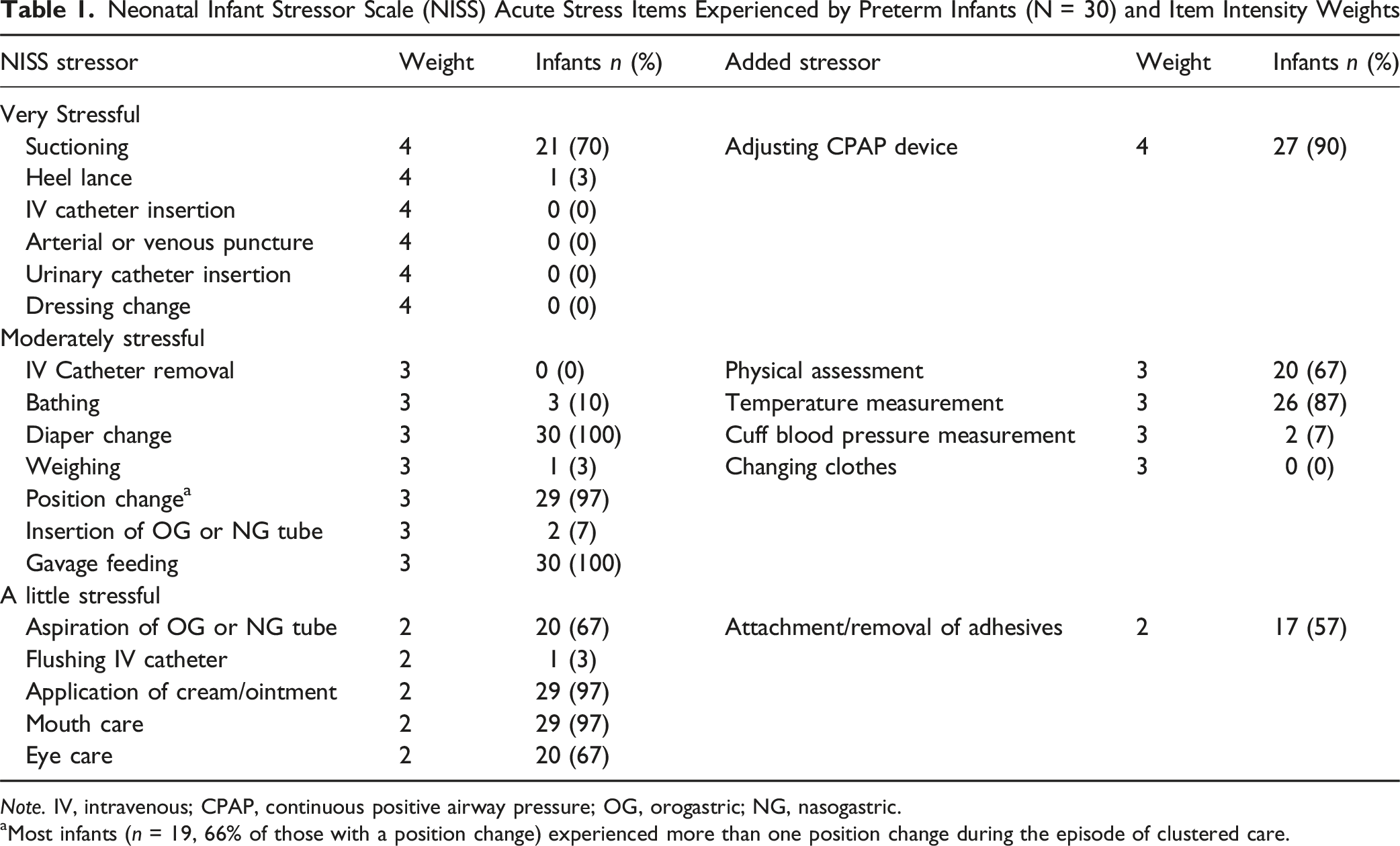
Note. IV, intravenous; CPAP, continuous positive airway pressure; OG, orogastric; NG, nasogastric.
aMost infants (n = 19, 66% of those with a position change) experienced more than one position change during the episode of clustered care.
Caregiving Duration
Caregiving duration (in minutes) was also used as a measure of stress exposure and was determined using a stopwatch. The stopwatch was started with the bedside nurse’s first direct touch of the caregiving episode and was stopped after the bedside nurse’s last direct touch of the caregiving episode. Direct touch was defined as physical contact between the bedside nurse and infant or direct physical contact between an object (e.g., stethoscope) and the infant.
Salivary Cortisol
Saliva was collected using Puritan HydraFlock Swabs (22029660, Fisher Scientific, Waltham, MA) Swab tips were immediately cut after saliva collection and placed into 2-ml microcentrifuge tubes. These tubes were kept on ice until they were returned to the lab for further processing. Immediately after data collection for each infant, samples were returned to the lab where they were centrifuged to extract saliva as described above. Saliva samples extracted from swabs were stored at −80°C until analysis. Cortisol levels in centrifuged saliva samples remain stable for up to one year at −80°C (Garde & Hansen, 2005). Within nine months of collection, we quantified cortisol in the saliva samples using Salimetrics’ Expanded Range High Sensitivity Salivary Cortisol ELISA (1-3002, Salimetrics, LLC., Carlsbad, CA) according to the manufacturer’s protocol and using manufacturer-provided controls. Saliva samples were diluted 1:2 using Salimetrics assay buffer and analyzed in duplicate on three ELISA plates. For samples of insufficient volume, sample dilutions of 1:3 were used. Intra-assay coefficients of variation were 9.5%, 12.6%, and 16.2%.
Procedure
Data collection occurred during each enrolled infant’s second week of life as part of a scheduled episode of clustered caregiving. We chose the second week of life for data collection to limit variance in cortisol attributable to chronological age. At the time of data collection, infants were admitted to one of four Level III/IV NICUs. The Level IV NICU is located in an all-referral academic children’s hospital where infants are primarily housed in single-family private rooms with an area of open bays for more clinically stable infants. All Level III NICUs are located in adult medical centers that provide maternity services. Two Level III NICUs house infants in single-family private rooms. A few double rooms are available and are typically reserved for twins. One Level III NICU houses infants primarily in open bays with a few private rooms reserved for very small or sick infants or infants requiring special isolation.
Immediately prior to the observed caregiving episode, a member of the study team collected a saliva sample from the enrolled infant by gently introducing a HydraFlock swab into the infant’s mouth and holding it in place for a maximum of 4 minutes to allow for swab saturation. After the baseline saliva collection, bedside nurses provided care based on standard practice and the infant’s specific clinical needs. During caregiving, we recorded the acute NISS procedures that occurred (e.g., gavage feeding, diaper change). Thirty minutes and 60 minutes after the last direct touch of the caregiving episode, saliva samples were again collected from the infant in the same manner to quantify HPA axis responses to caregiving (30 minutes) and following a recovery period (60 minutes). Saliva swabs were returned and processed in the lab immediately after the recovery period (∼2 hours after collection of baseline samples).
Ethical Considerations
The hospital’s IRB approved the study under expedited review. Following a thorough review of the study procedures, risks, and benefits, a parent or legal guardian provided written informed consent for infant participation in the study.
Statistical Analyses
We used measures of central tendency and variance to describe NISS scores and cortisol levels at baseline, 30-min after caregiving, and 60-min after caregiving. We calculated cortisol change scores from (1) baseline to 30-min after caregiving, (2) baseline to 60-min after caregiving, and (3) 30 to 60-min after caregiving. We regressed cortisol change scores on NISS scores and used robust standard errors to account for the possible misspecification of variance (Freedman, 2006). We repeated the analysis by regressing cortisol change scores on durations of caregiving. All analyses were conducted using STATA (version 18.5) with statistical significance at p <. 05.
Results
Validation Study–Flocked Polyester Swabs
Validation Study Cortisol Levels (µg/dl) in Aliquots Collected by Standard Methods and Extracted From Swabs (N = 23)

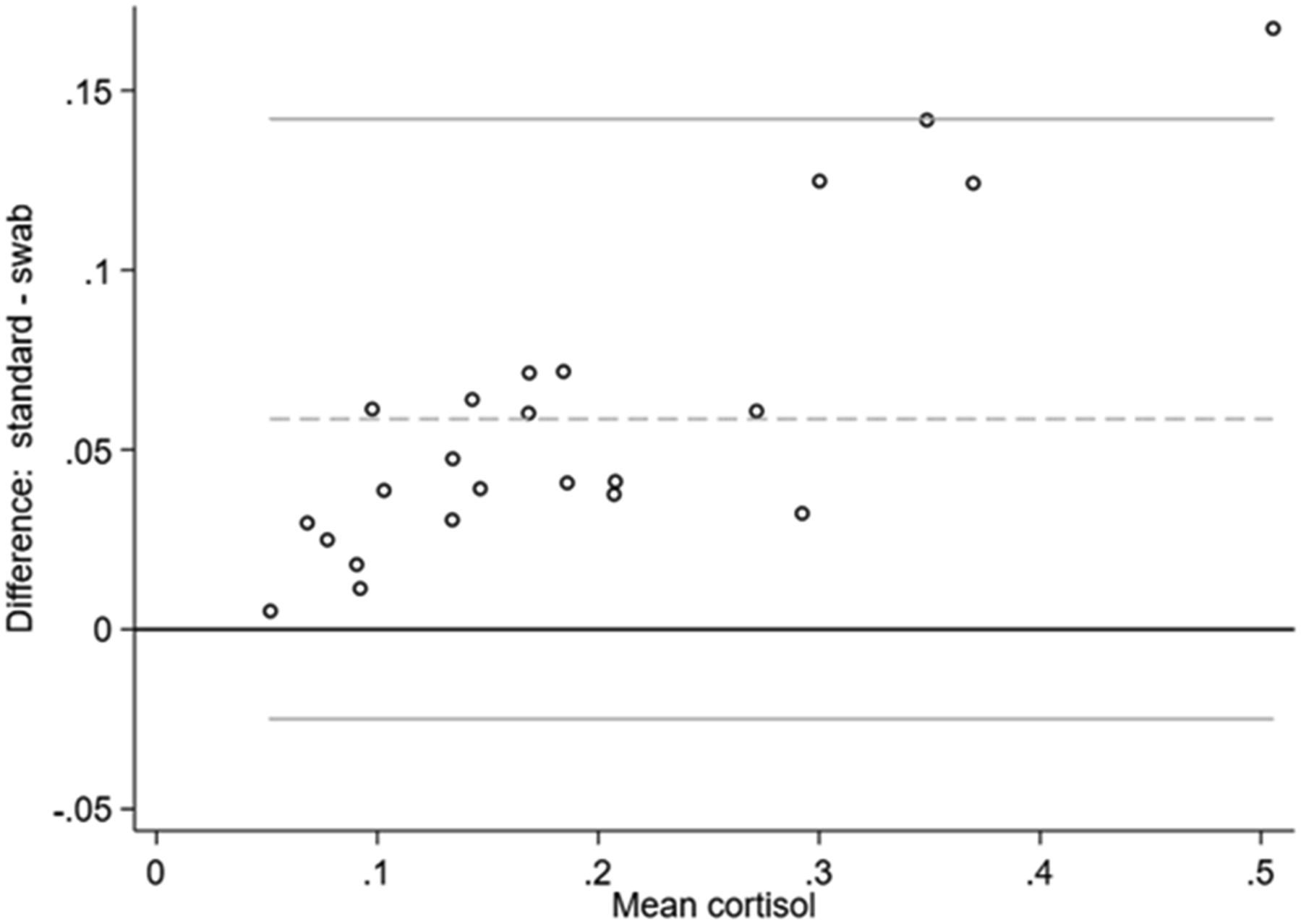
Bland-Altman plot
Application Study–Salivary Cortisol Responses in Preterm Infants
Participant Characteristics
Preterm Infant Characteristics (N = 31)
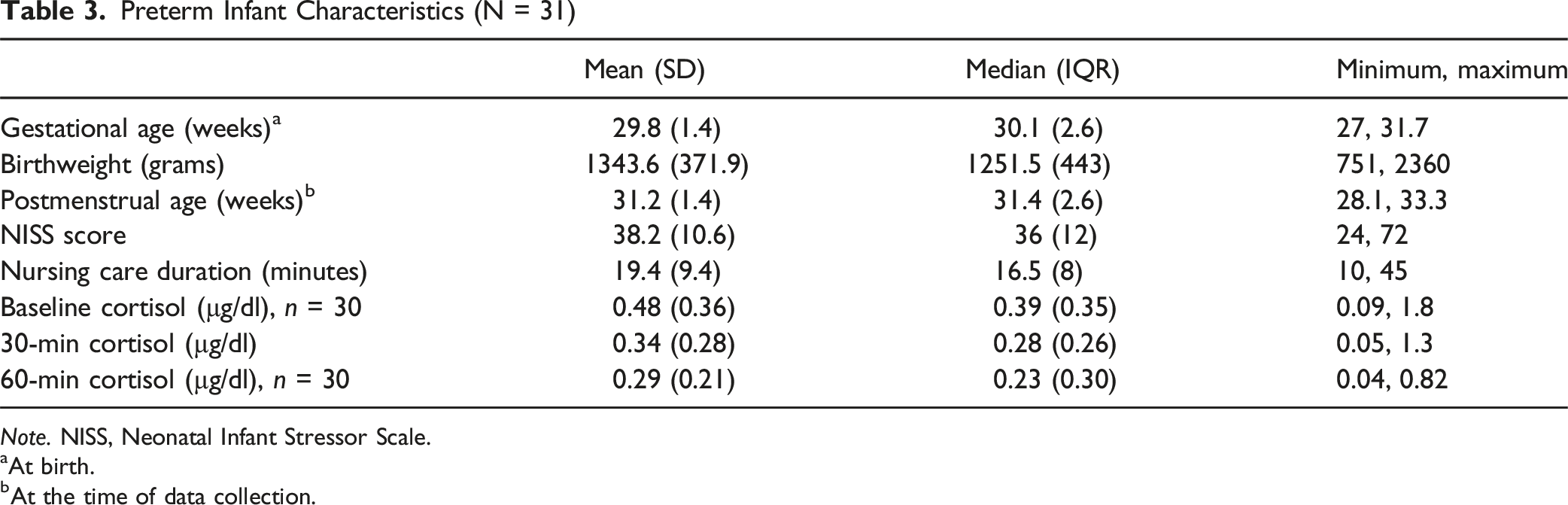
Note. NISS, Neonatal Infant Stressor Scale.
aAt birth.
bAt the time of data collection.
Ninety-three saliva samples were collected via swabs from the 31 enrolled infants. Following centrifugation, sufficient volumes for analysis were obtained from 91 of 93 swabs (98%). We were unable to extract sufficient volumes of saliva from the two swabs collected during baseline and at 60-min after caregiving from the first enrolled infant. Six of the 91 analyzed samples (7%), all collected from three infants, were diluted 1:3 prior to analysis to increase the total volume. Mean cortisol levels at baseline, 30-min after caregiving, and 60-min after caregiving were 0.48 µg/dl (SD = 0.36), 0.34 µg/dl (SD = 0.28), and 0.29 µg/dl (SD = 0.21), respectively. Most infants (n = 22, 76%) exhibited a decrease in cortisol from baseline to 30-min after caregiving. One infant exhibited no change between these timepoints. Similarly, 23 infants (77%) exhibited a decrease in cortisol from baseline to 60-min after caregiving, and 18 infants (62%) exhibited a decrease in cortisol from 30-min after caregiving to 60-min after caregiving. One infant exhibited no change in cortisol from 30-min to 60-min after caregiving.
Associations With Acute Procedural Stress
We found significant negative associations between NISS scores and changes in cortisol from baseline to 30-min after caregiving (Figure 3(A)) and from baseline to 60-min after caregiving (Figure 3(B)). On average, for each one-point increase in NISS score, the change in cortisol from baseline to 30-min after caregiving decreased (or became more negative) by 0.014 µg/dl (95% CI [0.0019, 0.026], p = .025). Similarly, for each one-point increase in NISS score, the change in cortisol from baseline to 60-min after caregiving decreased (or became more negative) by 0.016 µg/dl (95% CI [0.0034, 0.028], p = .014). NISS scores were not strongly associated with the change in cortisol from 30- to 60-min after caregiving (−0.0018 µg/dl, 95% CI [−0.007, 0.003], p = .46; Figure 3(C)). Associations between caregiving stressors and change in cortisol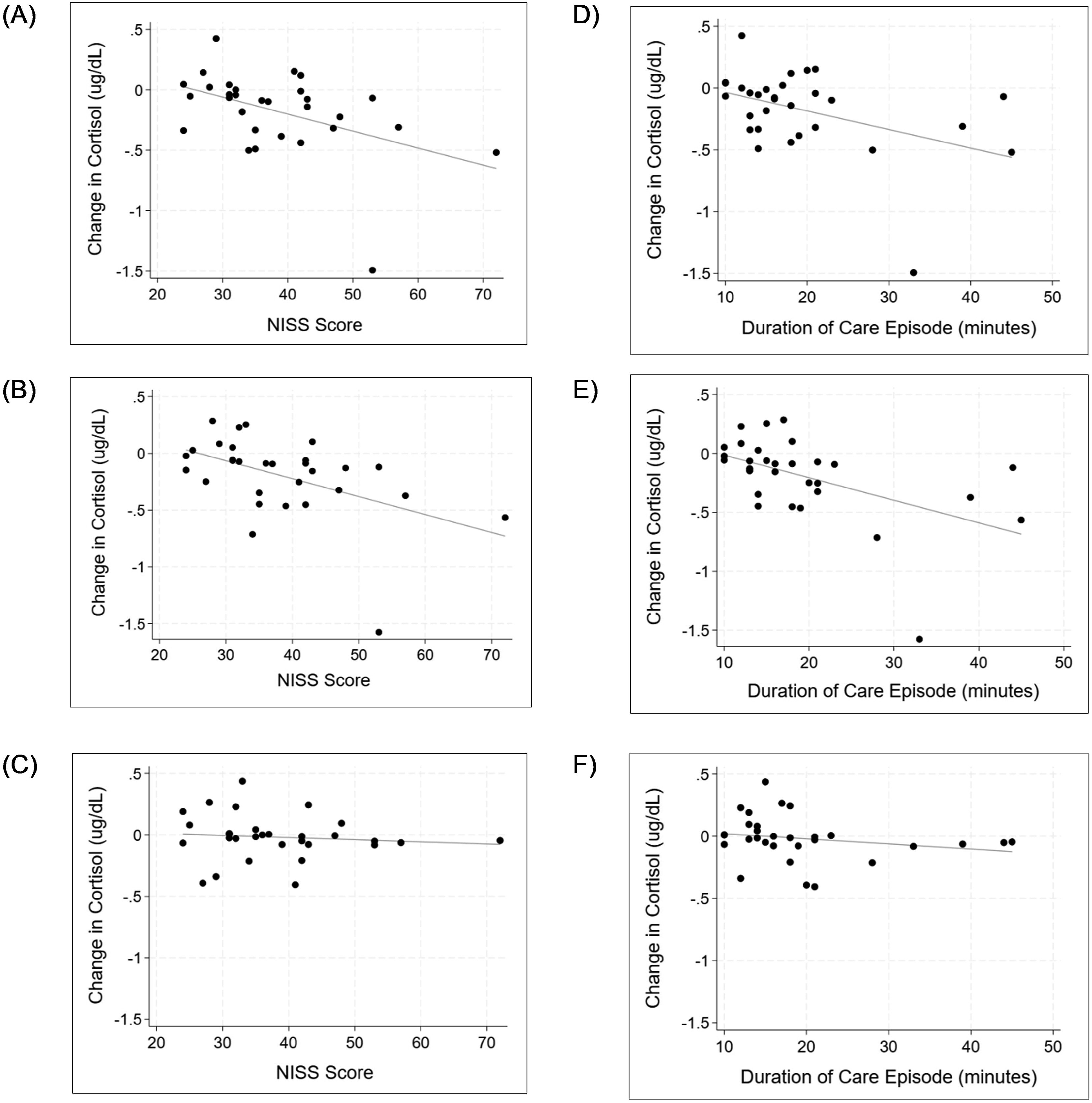
The duration of caregiving was negatively associated with the change in cortisol from baseline (Figure 3D–(F)), although this association was only statistically significant when considering the change from baseline to 60-min after caregiving (Figure 3(E)). For each 1-min increase in caregiving, the change in cortisol from baseline to 60-min after caregiving decreased (or became more negative) by 0.019 µg/dl (95% CI [0.0015, 0.037], p = .034). A similar association was observed between duration of caregiving and change from baseline to 30-min after caregiving, although this association did not reach statistical significance (−0.015, 95% CI [-0.032, 0.0015], p = .07; Figure 3(D)). The association between duration of caregiving and the change in cortisol from 30- to 60-min after caregiving was also not significant (−0.0041, 95% CI [−0.0083, 0.00006], p = .053; Figure 3(F)).
Discussion
We found that flocked polyester swabs can be used to collect saliva samples and do not interfere with the ELISA commonly used to quantify salivary cortisol. Although “standard” collection and “swab” collection produced aliquots with a high level of agreement in cortisol values, “swab” aliquots were consistently lower than “standard” collection aliquots. This difference may be caused by proteins binding to the swab fibers or incomplete saliva extraction from swabs. Thus, the same collection strategy must be used for all participants in a study, and cortisol levels across studies using different collection strategies will be difficult to compare. This limitation exists for most absorptive products used to collect saliva for the measurement of salivary cortisol (Harmon et al., 2007). Incomplete recovery of saliva from cotton and hydrocellulose products have been similarly demonstrated (Harmon et al., 2007). However, the use of an absorptive collection product is necessary to collect saliva from preterm infants, who are unable to provide samples by standard methods. We have shown that differences in cortisol levels in samples collected by standard methods and those collected using flocked polyester swabs do not appear to be random, allowing the substitution of swabs when standard collection methods cannot be used.
We also demonstrated that sufficient quantities of saliva for cortisol analysis can be collected from most preterm infants using flocked polyester swabs. A number of saliva collection strategies have been tested in infants, including syringe aspiration and absorption using filter paper, hydrocellulose microsponges, and commercially available saliva swabs; however, each of these strategies presents challenges (Tryphonopoulos et al., 2014). Specifically, syringe aspiration can cause mucosal damage in infants and, similar to cotton ropes, is only useful in infants who produce sufficient quantities of saliva (Tryphonopoulos et al., 2014). While filter paper absorption of saliva appears promising, this method requires an accurate estimation of the volume of saliva absorbed so that the correct amount of buffer is subsequently used to extract cortisol (Neu et al., 2007; Tryphonopoulos et al., 2014). Such estimations may be difficult in the clinical setting. Even highly absorbent materials, such as hydrocellulose, often fail to collect sufficient volumes for analysis (Araújo et al., 2018) and may require extended collection periods (Janevski et al., 2016) or saliva stimulants to obtain sufficient volumes (Zwimpfer et al., 2022). In addition to preterm infants, the collection of saliva with flocked polyester swabs may be useful for research with other populations such as those with cognitive impairment who may be unable to follow instructions for standard collection methods or older adults who often experience hyposalivation (Pina et al., 2020).
The infant study revealed a negative association between salivary cortisol levels and caregiving stressors, operationalized as acute NISS scores and caregiving duration. Although we might expect an increase in salivary cortisol from baseline levels following caregiving, cortisol responses can be highly variable in preterm infants (Janevski et al., 2016; Zwimpfer et al., 2022) and may depend on factors such as infant GA (D’Agata et al., 2019; Howland et al., 2017) and exposure to antenatal steroids (Finken et al., 2016; Howland et al., 2017). While all infants in our study were exposed to antenatal steroids, we did not have data on the time between steroid exposure and salivary cortisol measurement or the dose of antenatal steroids. Cortisol responses in preterm infants may be unpredictable due to the developmental immaturity of the HPA axis and variable programming effects related to maternal cortisol (Howland et al., 2017). Such factors make cortisol levels in preterm infants difficult to interpret, as there are no established normal ranges for cortisol in this population and levels may be influenced by prenatal and postnatal environmental exposures, maternal cortisol levels, and medical interventions.
Limitations
There are several limitations of this study. First, we were unable to conduct the initial validation study using preterm infants. Thus, cortisol levels reported for the adult volunteers may be very different from preterm infant levels. However, adult volunteers were necessary for the validation study so that sufficient volumes could be collected to compare cortisol levels from swabs and standard collection methods in the same saliva sample. Second, we did not have a sufficient sample size to conduct more complex statistical analyses for the application study. Variables such as GA may moderate infant responses to caregiving stressors and should be examined in larger studies. However, the primary purpose of the application study was to test feasibility of the saliva collection method in preterm infants. In addition, we limited enrollment within a narrow GA range (27–31 weeks) and collected data during each infant’s second week of life to control for chronological age. Finally, some caregiving activities such as suctioning and mouth care, which were routinely performed as part of clustered nursing care, may affect the post-caregiving cortisol levels. Future studies with large sample sizes should identify differences in cortisol between infants who experience these activities and infants who do not.
Conclusion
Although results of the infant study need to be considered with caution due to small sample size, the ability to collect adequate samples using the method is promising for future research that, to date, has been difficult due to high numbers of unusable samples. Additionally, because the results may be different from what may have been expected, it is important to further study the relationship between caregiving and acute stress responses and to consider how routine caregiving, a frequently repeated stressful event, might influence long-term health and programming of stress responses over time. Moreover, the manner in which care is provided may moderate the relationship between caregiving and infant responses and is an important area for study to improve outcomes. The timing and pacing of caregiving as well as the number of caregiving activities, provision of developmental interventions, and involvement of parents in infant caregiving may also influence infant responses and outcomes and should be considered for future study.
Footnotes
Ethical Considerations
The validation and application studies were approved by the Institutional Review Boards of The Ohio State University (2024H0063) and Nationwide Children’s Hospital (STUDY00003231), respectively.
Consent to Participate
Participants in the validation study provided verbal informed consent. The requirement for written informed consent was waived by the IRB, as this documentation would be the only identifiable link to study participants. Parents of infants in the application study provided written informed consent for their infant’s participation. Consent for public sharing was not obtained from participants.
Author Contribution
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute of Nursing Research of the National Institutes of Health under award number F31NR020849 (Cistone, PI). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available from the corresponding author following reasonable request.