
Abstract
Purpose:
To assess the effectiveness of autologous platelet-rich plasma for the treatment of dormant corneal ulcers secondary to corneal surgery and unresponsive to conventional treatment.
Setting:
VISSUM, Ophthalmology Institute of Alicante, Alicante, Spain.
Design:
Prospective nonrandomized, observational consecutive study.
Methods:
A total of 44 eyes of 28 patients with dormant corneal ulcers secondary to corneal surgery were included in a prospective study and treated with autologous platelet-rich plasma during 6 weeks. Wilcoxon signed-rank test was used to compare the effect of the treatment.
Results:
In all, 28 patients (65.1%) improved their visual acuity at least one line in Snellen chart, 26 (59.09%) had a decrease in the size of the ulcer or even a total closure, and 40 (90.9%) experienced an improvement in their symptoms. The results are also provided for the four groups of patients (keratoplasty, refractive surgery, cross-linking, and chronic postsurgical corneal edema).
Conclusion:
Platelet-rich plasma eye drops shows to be a good option for the treatment of dormant corneal ulcers secondary to corneal surgery.
Keywords
Introduction
Following corneal surgery, dormant corneal ulcers may appear as epithelial defects associated to Bowman’s layer disruption with associated damage and partial variable loss of superficial corneal stroma larger than 2 mm in diameter that persist more than 2 weeks even treated with conventional therapies. 1 They are located usually at the central cornea and may develop following a diversity of corneal surgeries and are a relevant complication that may affect very negatively the outcome of any corneal surgery.
Surgical procedures may damage the corneal nerves, which have an important role over the corneal epithelial proliferation. 2 Neurotrophic keratitis (NK) is, for instance, a degenerative corneal disease caused by partial or total impairment of trigeminal innervation leading to a reduction or even absence of corneal sensitivity.3,4 NK affects mainly to corneal epithelium, limiting its natural healing responses. It can produce a wide range of corneal signs. In mild cases, NK produces punctate keratopathy and stromal scarring, but in severe cases, it can lead to corneal ulcers, melting, and even perforation.3,4
Corneal hypesthesia or anesthesia can be caused by a variety of causes, such as infections (herpes simplex or zoster), corneal dystrophies, systemic polyneuropathies, topical or systemic treatments, chemical burns, or surgical procedures.2–5
There is a great variety of treatments for dormant corneal ulcers. The main medical approaches aim to avoid the use of eye drops with preservatives that can induce local toxicity and contribute to the chronicity of the disease and the use of the ocular surface lubrication with adequately selected artificial tears. Topical anti-inflammatory therapies, 6 collagenase inhibitors, 7 or procedures that to reduce the exposure of the ocular surface to the outside environment such as bandage contact lenses or tarsorrhaphy are also used.4,5,8 Amniotic membrane transplant has also been proposed as it may provide corneal tectonic protection and bio-stimulation, even than its use is not free from biological risks. 9
Autologous serum drops were the first autologous blood-derived product used for ocular surface diseases.10–13 Platelets are the main reservoirs of growth factors in blood. 14 Platelet-rich plasma (PRP) and plasma rich in growth factors (PRGF) contain platelets or platelet derivatives, which provide more growth factors than autologous serum without any disadvantages. PRP has been used previously by our group and others in small series of patients to treat several ocular surface problems with good results.1,15–17
Surgically related chronic epithelial defects and ulcers are frequently difficult to manage. PRP has previously shown to be effective in the treatment of ulcerative corneal disorders.1,18,19 The aim of this study is to assess the efficiency of PRP for the treatment of dormant corneal ulcers secondary to corneal surgery and unresponsive to conventional treatment.
Patients and methods
The study was designed to evaluate the efficacy of treatment for 6 weeks with autologous PRP eye drops of dormant corneal ulcers related to surgical procedures. For this purpose, a prospective non-comparative observational consecutive study was designed and performed, including patients with central dormant corneal ulcers related to previous eye surgical procedures who had not responded showing any improvement to previous conventional treatments for at least 15 days before.
At the moment of inclusion, all the subjects had a complete ophthalmic examination, including best-corrected visual acuity (VA) measurements and biomicroscopy with careful evaluation of the ocular surface as it will be mentioned later including corneal fluorescein staining. An evaluation of the patient’s symptoms was also performed. All the examinations were repeated on weekly basis. The condition of the patient at the end of the sixth week of treatment was taken as the endpoint for the purpose of this investigation.
The patients were classified into four different groups according to the type of surgery performed previously for the development the corneal ulcer: “keratoplasty” (including only penetrating keratoplasty and deep anterior lamellar keratoplasty (DALK)), “refractive surgery” (including laser in situ keratomileusis (LASIK) and photorefractive keratectomy (PRK)), “cross-linking” (with or without implanted intracorneal rings segments), and “chronic postsurgical corneal edema” (CPCE) caused by cataract surgery affected by a variety of intraoperative complications.
All the patients who had transmissible blood infections such as hepatitis B or C or HIV were excluded in order to guarantee the safety of the personnel that manipulate the blood samples. Patients with corneal dormant ulcers without previous corneal surgical procedures were excluded.
To be included in this investigation, all patients had to be able to understand and agree to sign a specific informed consent. The study was designed following the Declaration of Helsinki 20 and was previously approved by the Ethical Committee of VISSUM Alicante, Spain.
Main outcome measures
The studied outcomes were the evolution of subjective symptoms, improvement in VA, and the decrease of ocular surface inflammation and fluorescein staining after 6 weeks of treatment. Other medical treatments were not used during the investigational period. All the patients included in this clinical study were using a bandage contact lens at the moment of their inclusion in this study. Such contact lens was removed prior the beginning of the eye-platelet-rich plasma (E-PRP) treatment for 48 h.
The outcomes reported here are those found after 6 weeks or topical PRP monotherapy. Prior to start the PRP treatment, all topical treatments were stopped for a minimum of 48 h. The day of the beginning of the therapy, the eyes were then reevaluated according to the study protocol designed for the purpose of this investigation. Then, PRP treatment was started as one drop every 4 h on continuous basis for the following 6 weeks. Furthermore, frequent use of the E-PRP drops was allowed if the patient was feeling dryness or foreign body sensation. The same type of bandage contact lens was used in all cases from the beginning of the PRP therapy (Balafilcon A, PureVision®; Bausch & Lomb, Rochester, NY, USA). The only one associated therapy to E-PRP that was allowed was the use of a topical antibiotic (Ofloxacine, Oftacilox; Alcon Cusi, Barcelona, Spain) one drop every 12 h to prevent any infectious contamination. A bandage contact lens was used in all cases along the treatment period.
The patients were followed up on weekly basis by the same experienced ophthalmologist. The outcomes here reported correspond to the sixth week of treatment.
VA evaluation
Best-corrected visual acuity (BCVA) was measured before and after the treatment with PRP with a Snellen chart on a conventional projecting screen. For this purpose, counting fingers at 6 m was converted to Snellen range of 0.1, counting fingers at 60 cm to 0.01, hand motion at 6 m to 0.01, and hand motion at 60 cm to 0.001. Patients with light perception or worst were not included in the analysis. BCVA were analyzed on a logarithm of minimal angle of resolution (logMAR) scale. 21
The percentages of eyes which gained 1 or more lines lose 1 or more lines or remain stable in BCVA in the Snellen chart after the treatment was also studied.
Corneal surface evaluation
Corneal surface integrity was measured with fluorescein staining before and after the treatment. Particular attention was paid to ulcer diameter (vertical and horizontal), conjunctival appearance (edematous and non-edematous), conjunctival or ciliary hyperemia (intensive, medium, low, or absent), and discharge.
The evolution of ocular surface was categorized always by the same ophthalmologist and in all visits from the initial one as “worse”, “no change,” or “improved”.
Evaluation of subjective symptoms
Patient symptoms were evaluated by the ophthalmologist at the first and sixth visits through a subjective questionnaire. We ask questions about their condition and feelings previously and after the treatment with PRP. Red eyes, foreign body sensation itching, dryness, and pain were evaluated. To have an objective measure of the improvement, a 5-point scale was used for this purpose, where 0 = no change, 1 = slight improvement, 2 = moderate improvement, 3 = very good, and 4 = excellent.
Autologous topical E-PRP preparation
PRP preparation was carried out under strict sterile conditions using sterile and disposable materials and operating inside a laminar flow hood. Whole patient’s blood was extracted aseptically using 3.8% sodium citrate as anticoagulant. After centrifugation (10 min at 1600 r/min), three layers were obtained. Platelet-poor plasma (PPP) on the top, PRP below, and at the bottom separated white and red cells. PRP was aspired and 3–4 mL aliquots are transferred into 10 mL new sterilized amber glass bottles with eye drop applicators. The bottle in use should be kept in the refrigerator at +4ºC for 1 week and the remaining bottles were kept in the freezer at −20ºC. 19 There were no dilutions of the PRP. The substance so created was termed as E-PRP.
Statistical analysis
After normality test assessment was performed, non-parametric test was used (Wilcoxon) to compare the response to the treatment. Dataset and statistical analysis were performed with STATA v.13® (STATA Corp., College Station, TX, USA).
Results
In all, 44 eyes were included in this prospective investigation (23 males and 21 females). There were 29 eyes with NK post-keratoplasty, six patients post refractive surgery, three patients with cross-linking with epithelium removal technique, and six patients with CPCE. The mean age of all the patients was 48.77 ± 3.4 years.
VA evolution
The mean BCVA was 1.36 ± 0.17 logMAR (0.04 ± 0.17 lines in Snellen decimal scale 21 previous to treatment with E-PRP and 0.97± 0.15 logMAR (0.10 ± 0.15 lines in Snellen decimal scale) after it. The p value for this change was 0.0009 (p < 0.05 in Wilcoxon paired test).
The mean lines of VA in Snellen chart were 3.33 ± 0.49 before the treatment and 4.48 ± 0.59 after it. The p value for this change was 0.0006 (p < 0.05 in Wilcoxon paired test).
Of the eyes, 29 (65.9%) had an improvement of at least 1 line of VA in Snellen chart, 9 eyes (20.5%) remain stable, and 6 (13.6%) suffered a decrease in their vision. The patients who decreased their vision were from the penetrating keratoplasty group.
The improvement in BCVA and in lines in Snellen chart had significant changes (p < 0.05 in Wilcoxon paired test) only in the post-keratoplasty grow, but is close to be significant in refractive and CPCE groups (Table 1).
BCVA and lines in Snellen chart by groups.
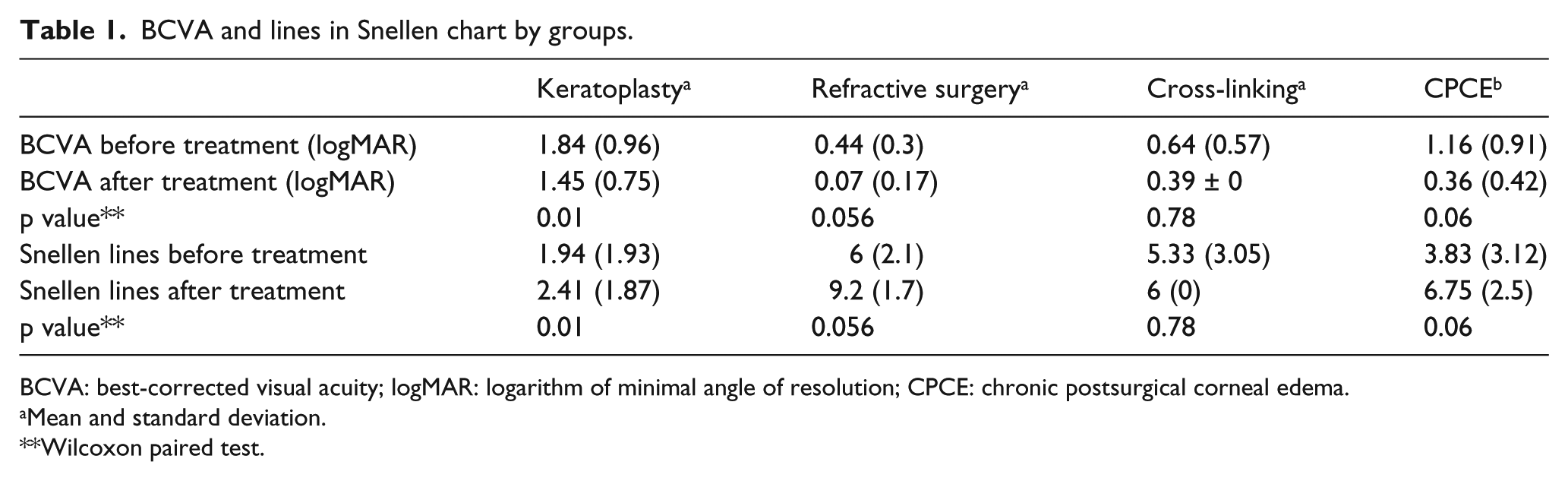
BCVA: best-corrected visual acuity; logMAR: logarithm of minimal angle of resolution; CPCE: chronic postsurgical corneal edema.
Mean and standard deviation.
Wilcoxon paired test.
Corneal surface evolution
The vertical and horizontal dimensions of the fluorescein-stained area at the corneal surface were used to assess the response of ocular surface to the treatment of E-PRP. Overall, 26 eyes (59.1%) had a decrease in the fluorescein-stained area, 15 remained stable (34.1%), and 3 got worst after the treatment (6.8%; Table 2). The corneal evolution of one patient is shown in Figure 1.
Corneal surface integrity by groups.

CPCE: chronic postsurgical corneal edema.
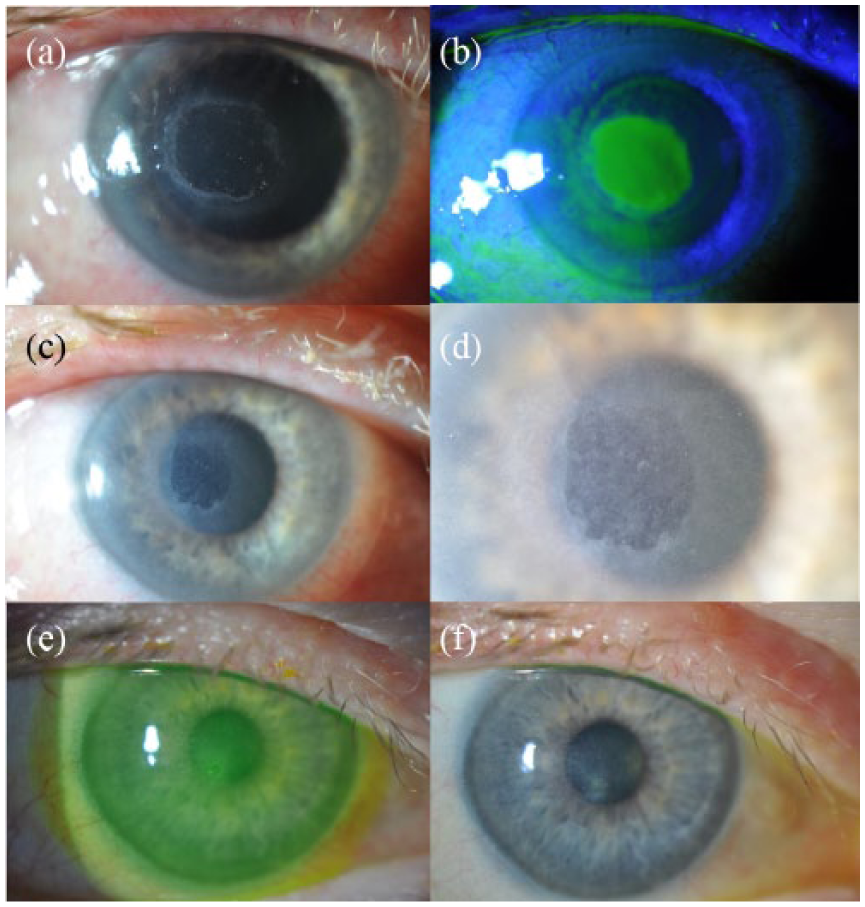
Different pictures of the right eye of a patient taken with a slit lamp that underwent a photorefractive keratectomy and showed an ulcer after the surgery. (a) Slit-lamp picture showing the ulcer of the patient before the treatment with E-PRP. (b) The same ulcer but with fluorescein. (c) The ulcer 3 days after treatment with E-PRP, and there is a minimal improvement compared to the ulcer without treatment. (d) Similar to (c), but with a higher magnification. (e) The ulcer with fluorescein 15 days after the treatment with E-PRP. (f) Slit lamp shows the ulcer 1 month after the treatment which shows that the ulcer has nearly disappeared.
Evolution of the symptoms
All the patients were asked for the change of their symptoms. Patients reported the improvement of their symptoms as “great improvement” after the treatment in 16 (36.4%), as “moderate improvement” in 17 (38.6%), as “slight improvement” in 7 (15.9%), and as “no changes or worsen” in 4 (9.1%). Overall, 40 patients (90.9%) showed an improvement of their symptoms, and most of them were “great” or “moderate improvement”. The subjective response to the treatment of E-PRP for each group is shown in Table 3.
Changes on symptoms by groups of pathologies.
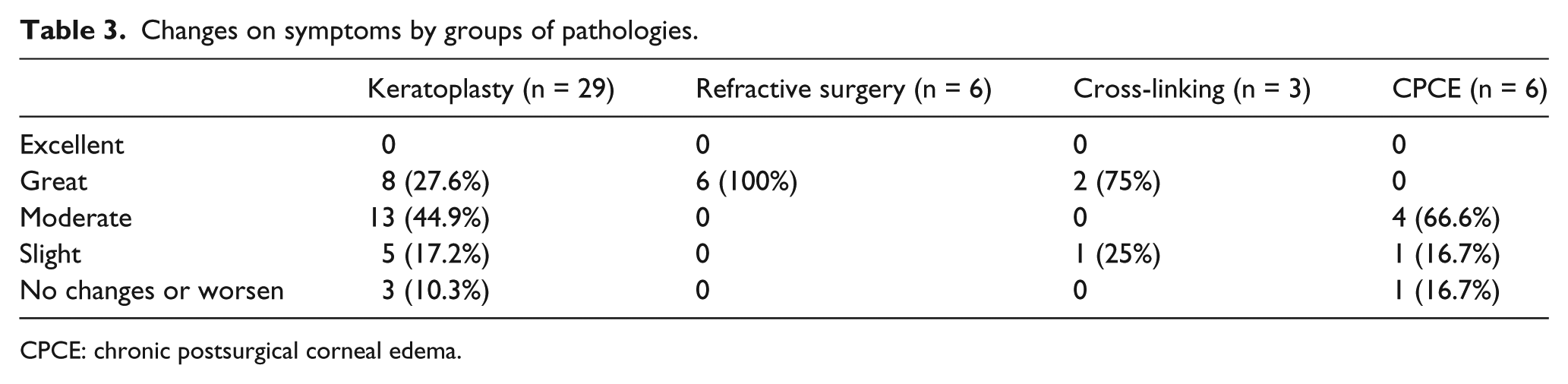
CPCE: chronic postsurgical corneal edema.
Discussion
Postoperative corneal dormant ulcers may be caused by several factors; being the neurotrophic origin due to corneal nerves damage the most common. Other causes are the toxicity of topical drugs and preservatives used in topical medication postoperatively, 22 and the reactivation of herpetic previously latent infection. 23
Direct surgical damage of the corneal nerves is a common pathogenic mechanism of damage in many of these diseases.3–5 The direct cut by accidental trauma or corneal surgery produces a tissue denervation, leading to epithelial and stromal corneal damage. The re-innervation of the damaged tissue depends on the deepness, the direction, and the location of the corneal cut. 2 Stromal re-innervation is slight and limited to the corneal periphery in penetrating keratoplasty surgery, but is almost complete after LASIK or cross-linking procedures. 2 Topical drugs may have detrimental effects on ocular surface and corneal epithelium, and they may compromise the recovery of any surgical treatment. All topical drugs have toxic effects; however, it is greater in long-term use of drops of timolol, betaxolol, prostaglandin analogs, and preservatives.3,24
There are several treatments for corneal dormant ulcers, and the use of growth factors has shown to have an important potential role. 2 Modulators of corneal nerve and epithelium growth are present in platelets and they can be supplied by the adequate blood derivatives. 2 As an example, autologous serum (AS) has nerve growth factor (NGF), epidermal growth factor (EGF), insulin-like growth factor 1 (IGF-1) and vascular endothelial growth factor (VEGF) among others. 2 Autologous serum drops were first used for the treatment of dry eye with Sjögren’s syndrome.10,12,25 Since then, it has been the preferred blood-derived topical preparation in the treatment of ocular surface diseases. It is effective for persistent epithelial defects, 13 neurotrophic ulcers, 11 superior limbic keratoconjunctivitis, 26 and dry eye due to graft versus host disease 27 or LASIK. 28
Platelets are the main growth factor reservoirs in blood. Their alpha granules contain more than 30 bioactive proteins which promote tissue repair. 14 In light of this evidence, concentrated platelet preparations have been used in multiple clinical situations where fast healing and tissue regeneration are needed.29,30 E-PRP drops have been used previously to treat corneal ulcers caused by different etiologies.1,15,18,31 In this report, we have studied the response to this treatment shown by dormant corneal ulcers related to previous corneal surgery.
Overall, we have found a significant improvement in BCVA and gain in lines on Snellen chart after 6 weeks of treatment. Analyzing each group of surgery, only the group operated with keratoplasty had significant gains of BCVA and lines on Snellen chart. However, refractive and CPCE cases were closed to be significant in the visual improvement. The absence of improvement in cross-linking group may be explained by the low number of patients (three patients).
In all, 26 patients (59.09%) of the whole sample improved the corneal integrity, and most of the patients of each group had an improvement of corneal surface. However, our previous results in a pilot study 1 and other similar studies 16 showed greater improvements close to 90%. This may be explained because of sampling differences. Dormant corneal ulcers developed following corneal surgical procedures may have greater severity than herpetic disease or dry eye, diseases which form the most of the patients of those samples.1,16
A total of 40 patients (90.9%) improved their symptoms, although there were no patients reporting levels of “excellent” recovery. Symptomatic improvements must be analyzed carefully. A very important factor to consider in the evaluation of the symptoms is that patients with a neurotrophic component may not feel significant pain or discomfort because of their corneal hypesthesia. This might have a confounding influence in the patient’s symptoms, as if an anatomical improvement is promoted, when tissue heals, the corneal sensitivity returns and the patients might fell more pain or foreign body sensation than before the treatment. 11
Our study analyzed the largest series of surgically induced dormant corneal ulcers treated with PRP. This novel treatment has shown in this study positive outcomes in the treatment of dormant corneal ulcers due to corneal surgery. These encouraging results should promote further prospective studies to compare E-PRP with other blood derivatives to ascertain the relative role that each derivative may have in the treatment of dormant corneal ulcers.
Footnotes
Acknowledgements
The authors warrant that the manuscript represents original, unpublished material not under editorial consideration elsewhere and that ethical guidelines were followed in the conduct of the research. Pablo De Arriba is now affiliated with Research, Development and Innovation Department, VISSUM, Alicante, Spain.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication has been carried out in the framework of the Red Temática de Investigación Cooperativa en Salud (RETICS), reference number RD16/0008/0012, financed by the Instituto Carlos III – General Subdirection of Networks and Cooperative Investigation Centers (R&D&I National Plan 2008-2011) and the European Regional Development Fund (Fondo europeo de desarrollo regional FEDER).