
Abstract
Purpose:
To evaluate light and electron microscopic changes of the anterior capsule and its epithelium after clear lens extraction of vitrectomized myopic eyes with silicone oil tamponade.
Methods:
This prospective, controlled, non-randomized, interventional study included 20 anterior lens capsular specimens that were excised during combined clear lens extraction and silicone oil removal from previously vitrectomized highly myopic patients with silicone oil tamponade for previous retinal detachment surgeries. The specimens were examined via light microscopy and electron microscopy and compared with 20 anterior capsule specimens removed during clear lens extraction of non-vitrectomized highly myopic eyes.
Results:
Light microscopic examination of clear lens anterior capsule specimens of vitrectomized myopic eyes filled with silicone oil showed relatively more flat cells with irregular outline of lens’ epithelial cells with wide intercellular spaces, deeply stained nuclei, and multiple intracytoplasmic vacuoles. Scanning electron microscopy revealed collagenous surfaces filled with multiple pits, depressions, and abnormal deposits. Transmission electron microscopy revealed lens epithelial cells with apoptotic changes, many cytoplasmic vacuoles, and filopodia-like protrusions between lens epithelial cells and the capsule. Epithelial proliferation and multilayering were also observed.
Conclusion:
silicone oil may play a role in the development of apoptotic and histopathological changes in clear lens epithelial cells. Clarity of the lens at the time of silicone oil removal does not indicate an absence of cataractous changes. We found justification of combined clear lens extraction and silicone oil removal or combined phacovitrectomy when silicone oil injection is planned, but further long-term studies with larger patient groups are required.
Introduction
Vitreoretinal surgeons have used silicone oil tamponade in retinal detachment surgeries for over 50 years. 1 However, many postoperative complications following silicone oil injection have been reported, including cataractous changes, resistant glaucoma, and corneal complications. 2 Cataract is the most common complication associated with the injection of silicone oil after retinal detachment surgery. 3 Casswell and Gregor 4 reported that 60% of lenses that were clear at the time of silicone removal developed clinically significant cataract after 6 months of follow-up. Researchers have studied the ultrastructural effects of silicone oil tamponade on the anterior lens capsule and its epithelium in cataractous lenses.5–9
The aims of this study were to investigate the clinically unseen cataractogenic effects of silicone oil via light and electron microscopy of clear lens anterior capsules and their epithelium in highly myopic vitrectomized eyes with silicone oil tamponade and to compare those capsules with anterior lens capsules obtained by refractive clear lens extraction (RLE) in highly myopic eyes.
Methods
The study included 20 patients who had presented with highly myopic vitrectomized eyes with silicone oil tamponade for 8–12 weeks (group A) at the Ophthalmology Department of Assiut University Hospital, Egypt, between May 2015 and June 2016. No silicone oil emulsified droplets were seen in the anterior chamber or the angle of the cases studied. A total of 20 non-vitrectomized highly myopic eyes were included as a control group (group B). The capsule specimens of group A were examined via light microscopy, scanning electron microscopy, and transmission electron microscopy and compared with 20 anterior capsule specimens removed from non-vitrectomized highly myopic eyes during RLE (group B). In both groups, we excluded cases with any clinically visible cataractous changes and cases with a previous history of ocular trauma or chronic uveitis. We also excluded cases with silicone oil emulsifications in the anterior chamber or its angle. The Ethics Committee of the Faculty of Medicine at Assiut University approved the study, and it was conducted in accordance with the Declaration of Helsinki II. All study subjects provided informed consent prior to participation.
The study was a prospective, controlled, non-randomized, interventional study. In both group A and group B, we performed preoperative examinations including uncorrected visual acuity (UCVA), best-corrected visual acuity (BCVA), applanation tonometry, B-scan ultrasonography, and fundus assessment with examination of the retinal periphery. Optical biometry was performed using an AL-Scan Optical Biometer (Nidek, Fremont, CA, USA).
Patient evaluation and assessment
Group A
Patients in group A underwent combined silicone oil removal and phacoemulsification performed by the same surgeon, and the anterior capsule specimens were obtained via capsulorhexis (5 mm) and preserved immediately in 2.5% glutaraldehyde solution in 0.1 M cacodylate buffer (pH 7.4) for 24 h. Prophylactic argon laser treatment (532 nm green; Ellex, SA, Australia) was performed in any suspicious retinal areas 2 weeks before surgery. We included patients with myopia >–14 diopters, aged >40 years, with a clear crystalline lens at the time of silicone oil removal and a logarithm of the minimum angle of resolution (logMAR) BCVA of at least 1.00 (Snellen equivalent 20/200), and with no recurrent retinal detachment during silicone oil removal. Clear lens extraction was done at the time of silicone oil removal for refractive purposes as previously described by Fathalla et al. 10 We performed clear lens extraction before silicone oil removal. Silicone oil was extracted after making two sclerotomies 3.5 mm from the limbus. After inserting an infusion cannula into one sclerotomy, silicone oil was actively suctioned from the other sclerotomy. We then checked retinal status. All patients in group A had silicone oil tamponade 2000 cSt (Siluron; Fluoron, Neu-Ulm, Germany).
Group B
Patients in group B underwent RLE for refractive purposes. Phacoemulsification was performed by the same surgeon and the anterior capsular specimen was obtained via capsulorrhexis (5 mm) and then preserved immediately in 2.5% glutaraldehyde solution in 0.1 M cacodylate buffer (pH 7.4) for 24 h. Patients were seeking RLE because they did not wish to wear glasses. We included patients with myopia >–14 diopters, aged >40 years, with logMAR BCVA of at least 1.00 (Snellen equivalent 20/200). We included patients who were not candidates for laser-assisted in situ keratomileusis (LASIK). We performed prophylactic argon laser photocoagulation (532 nm green; Ellex, Adelaide, SA, Australia) in the retinal periphery 2 weeks before RLE.
All specimens from each group were divided into two parts. One part was prepared for scanning electron microscopy (JEM 100 CXII; JEOL, Tokyo, Japan) via fixation in 1% osmium tetroxide in phosphate buffer for 2 h, dehydration in increasing concentrations of acetone, air drying, mounting on metal stubs with a double-sided adhesive band, and then sputtering with a 100-Å-thick layer of gold. The other part was prepared for light microscopy (Olympus, Japan) and transmission electron microscopy.
Results
The study included 40 eyes of 40 patients. Mean age in group A was 40.46 ± 4.74 years (range = 40–49 years; 8 females and 12 males), and in group B it was 41.32 ± 3.52 years (range = 41–47 years; 9 females and 11 males). In group A, myopia ranged from −14 to −20 diopters (mean −15.3 ± 4.1 diopters), and in group B, it ranged from −14 to −19 diopters (mean −14.3 ± 5.2 diopters). There were no statistically significant differences in age or refraction between groups A and B (p > 0.05). Silicone oil removed between 8 and 12 weeks after retinal detachment surgery (mean 8.71 ± 2.75 weeks). Mean preoperative logMAR BCVA was 1.32 ± 0.04 (mean Snellen equivalent 20/390) in group A, and in group B, it was 0.70 ± 0.05 (mean Snellen equivalent 20/100). Mean preoperative intraocular pressures were 14.45 ± 1.70 mmHg in group A and 13.27 ± 1.80 mmHg in group B. No intraoperative complications were reported in either group.
Light microscopy examination of lens capsules from group B showed regularly arranged cuboidal epithelial cells with a large central nucleus (Figure 1(a)). The lens capsules in group A showed relatively flat cells, irregular outline of lens epithelial cells with wide intercellular spaces, deeply stained nuclei, and multiple intracytoplasmic vacuoles (Figure 1(b) and (c)).

(a) Semi thin sections of lens capsules stained by toluidine blue in the clear lens extraction group (group B) showing regularly arranged cuboidal epithelial cells (ep) with a large central nucleus (N). (b) The silicone-filled eyes group (group A) showing irregular outline of epithelial cells with wide intercellular spaces (*). (c) Lens epithelia of group A showing deeply stained nuclei (N) and multiple intracytoplasmic vacuoles (v).
Transmission electron microscopy examination of group B lens capsule specimens showed normal looking epithelial cells with a healthy basement membrane and a cytoplasm filled with organelles (Figure 2). Conversely, transmission electron microscopy examination of group A lens capsules showed lens epithelial cells with apoptotic changes, including electron-dense nuclei with irregular contours and chromatin margination (Figure 3(a)). Many vacuoles were observed among accumulations of Golgi bodies in the cytoplasm that contained engulfed silicon oil droplets (Figure 3(b)). Contact between lens epithelial cells and the capsule was altered, with filopodia-like protrusions creating a gap beneath the capsule (Figure 3(c)). Some specimens showed epithelial proliferation and multilayering (Figure 3(d)).
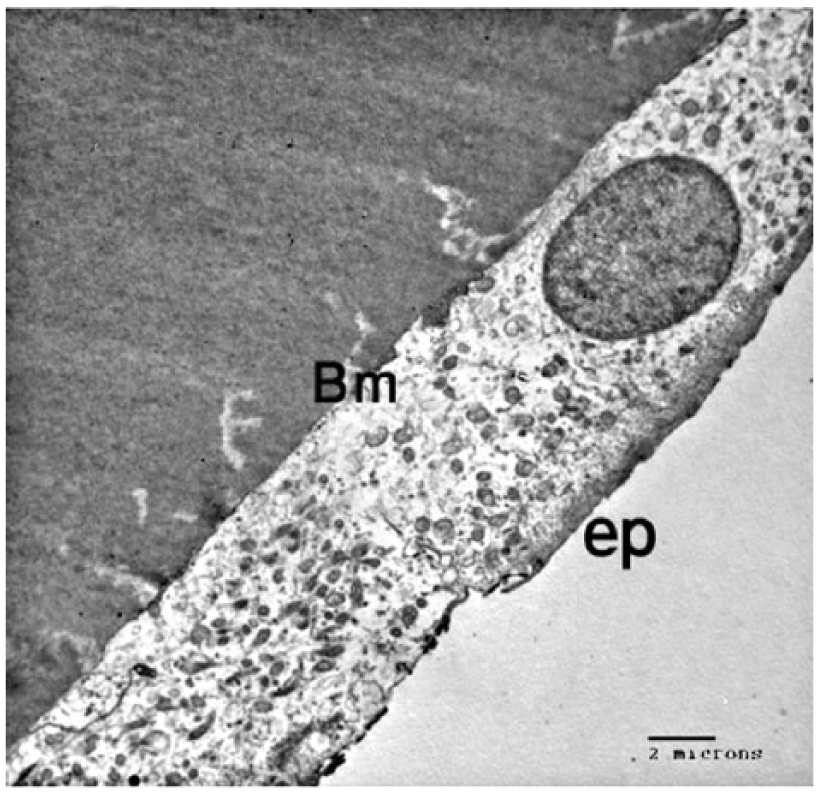
Transmission electron micrograph of group B lens capsule shows normal looking epithelial cells (ep) with a healthy basement membrane (Bm), and the cytoplasm is filled with organelles.
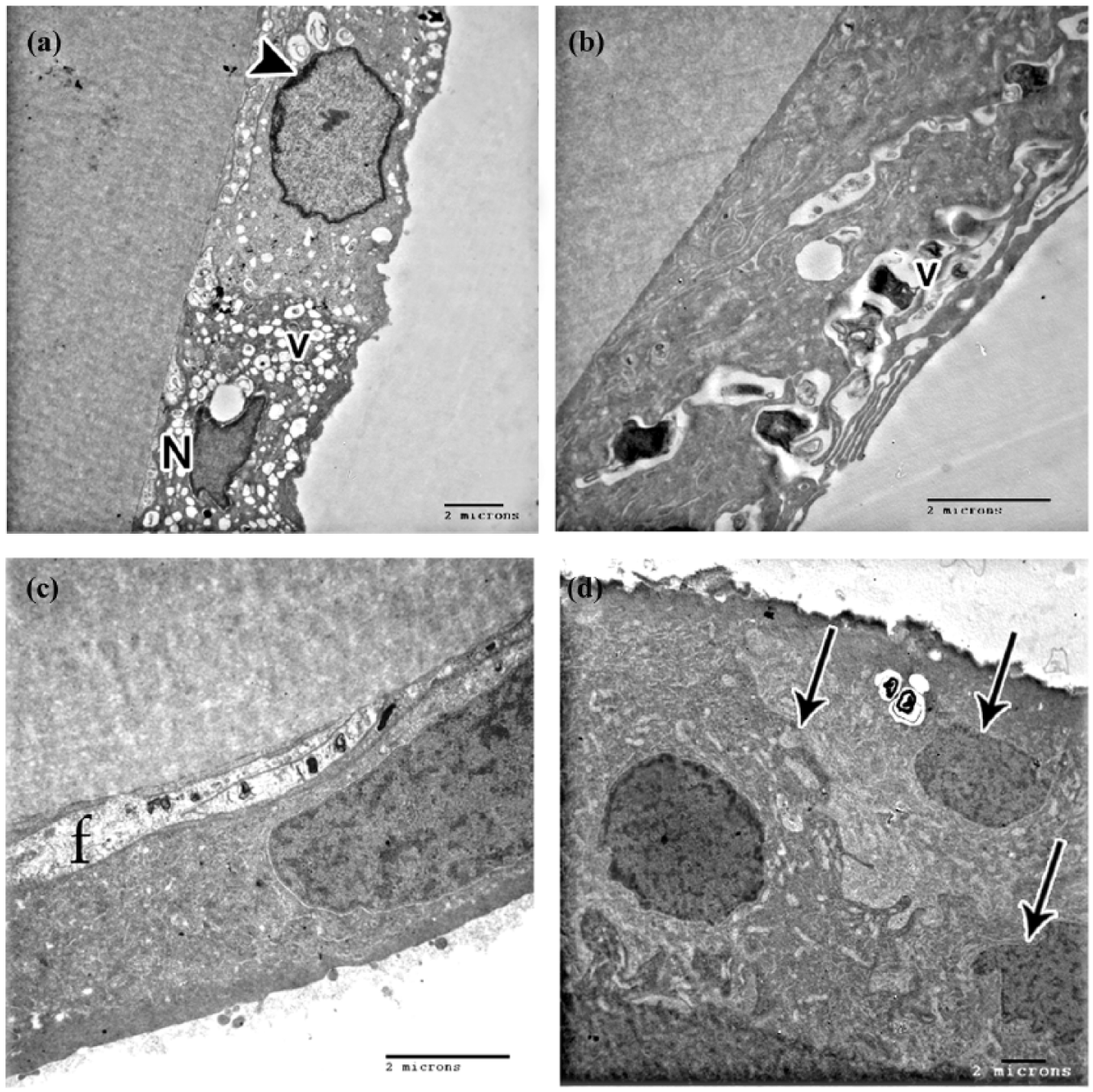
Transmission electron micrographs of group A lens capsules: (a) lens epithelial cells with irregular electron-dense nuclei (N) and chromatin margination (arrow head). The cytoplasm shows many vacuoles (v). (b) Many vacuoles accumulate among Golgi bodies in the cytoplasm that contain engulfed silicon oil droplets (v). (c) Contact between lens epithelial cells and the capsule was altered where (f) filopodia-like protrusions created a gap beneath the capsule. (d) One specimen exhibited epithelial proliferation and multilayering (arrow).
Scanning electron microscopy examination of group B lens capsules showed a relatively homogeneous collagenous surface of the anterior capsule (Figure 4(a)) with regular arrangement of normal looking epithelial cells that exhibited bulging of nuclei and interlacing intercellular junctions (Figure 4(b)). Group A lens capsule specimens exhibited a collagenous surface filled with multiple pits and depressions (Figure 4(c)), and the epithelial side showed irregularly arranged, relatively flattened cells with abnormal intercellular junctions (Figure 4(d)).
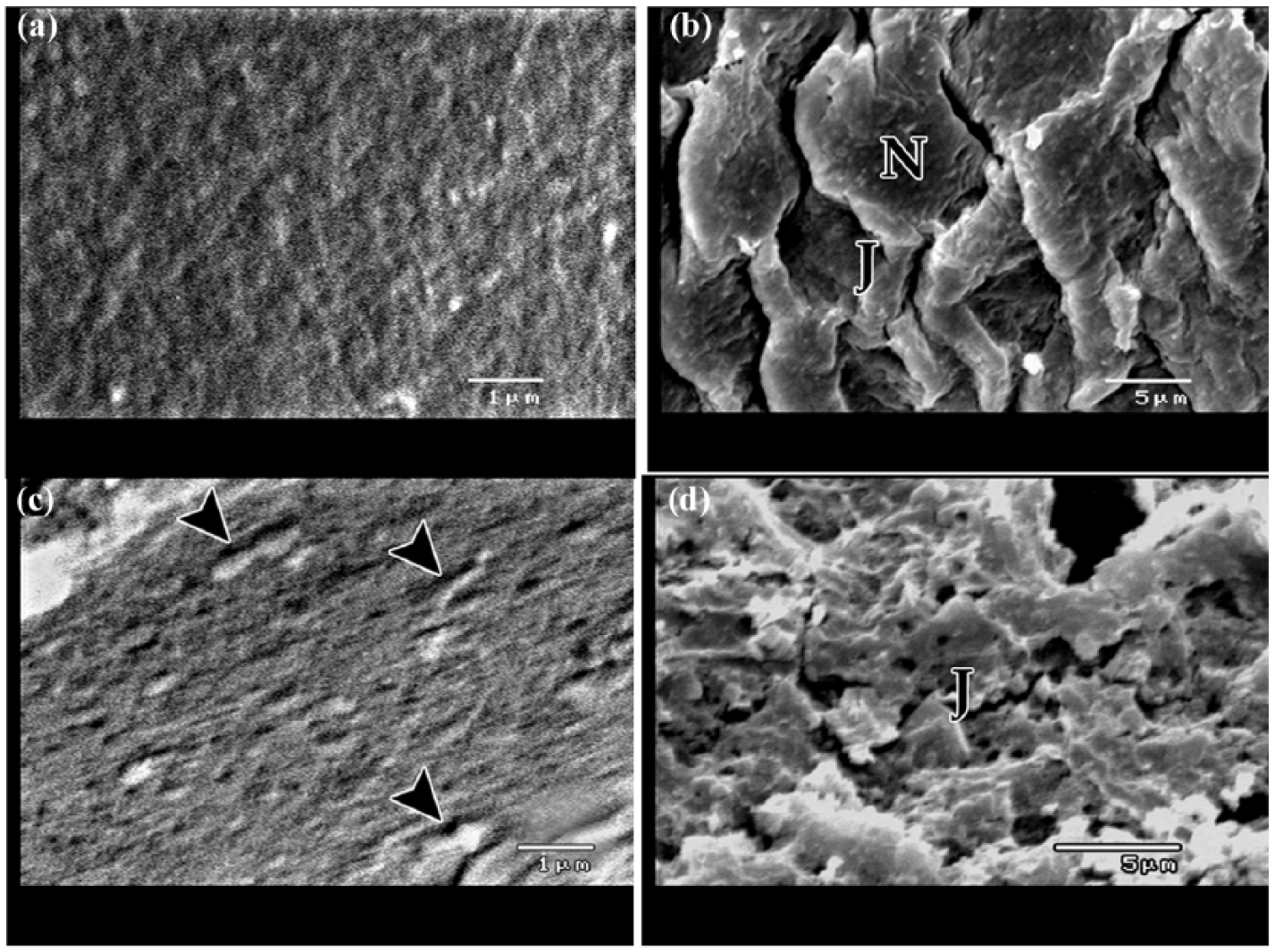
Scanning electron micrographs of (a and b) group B and (c and d) group A lens capsules: (a) a relatively homogeneous collagenous surface of the anterior capsule. (b) Regular arrangement of lens epithelial cells exhibiting central bulging of nuclei (N) and normal interlacing intercellular junctions (J). (c) Lens capsule exhibits a collagenous surface filled with multiple pits and depressions (arrow head). (d) Epithelial side shows irregularly arranged relatively flattened cells with abnormal intercellular adhesions (J).
Discussion
The timing of lens extraction after vitrectomy and silicone oil tamponade for rhegmatogenous retinal detachment is controversial. Cataractous change is the most common complication of silicone oil injection after vitrectomy. 3 Casswell and Gregor 4 reported that 60% of lenses that were clear at the time of silicone removal developed clinically significant cataract after 6 months of follow-up, and Gonvers 11 reported an even higher percentage of cataract after silicone oil removal (78%). Casswell and Gregor 4 reported that 100% of patients developed lens opacities if the silicone remained in the eye for more than 10 weeks.
In this study, the mean time of silicone oil tamponade was nearly 9 weeks, and we detected apoptotic changes including electron-dense nuclei with irregular contours, chromatin margination, and degenerated nucleoli in the epithelial cells of clear lenses at the time of silicone oil removal. This may partly explain why lenses that are clear at the time of silicone oil removal can become cataractous within 6 months postoperatively. Without increasing redetachment rates, clear lens extraction in combination with silicone oil removal was justified socially and scientifically for myopic patients in a study by Fathalla et al. 10 due to the associated increase in postoperative BCVA compared to the predetachment BCVA. In this study, there was also another scientific justification for removing the clear lens in combination with silicone oil removal because of the unseen cataractogenic effect of silicone oil tamponade. Our findings suggested that there were apoptotic changes in the lens epithelium of the clear crystalline lens that may explain the post-silicone oil removal development of cataract. Many possible explanations for the cataractogenic effect of silicone oil tamponade after detachment surgery have been suggested. Some relate to the disturbance of normal oxygen exchange and the exchange of other nutrients at the interface between the silicone oil and lens tissues.3,12
Silicone oil particles were detected inside the cytoplasm of the lens epithelial cells in this study, and this is concordant with Ohira et al. 13 who reported that silicone oil injected into rabbits’ eyes was detected in the retinal layers 1 week later. A study by Citirik et al. 5 suggested that silicone oil led to changes in the molecular charge of the lens capsule that could increase the permeability of the lens capsule and enable the ingress of silicone oil particles into epithelial lens cells. This may explain the presence of silicone particles inside the clear crystalline lens cells detected in this study. The expression of biochemical apoptotic markers such as B-cell lymphoma 2-associated X protein (BAX) and caspase-3 increased in the epithelial cells of cataractous lenses due to silicone oil tamponade in a study by Zhu et al., 9 and this is concordant with the apoptotic changes in clear crystalline lens epithelial cells detected in this study. Although emulsified silicone was not found in our study, we detected apoptotic changes in lens epithelial cells. Thus, silicone oil can still exert cataractogenic effects in the absence of emulsification. This was also confirmed in a study in which there was no correlation between silicone emulsification and increased apoptotic marker expression in patients with complicated cataract due to silicone oil tampnade. 9
While previous studies have investigated changes in capsule and lens epithelial cells in cataractous lenses after silicone oil tamponade,7,14 our study investigated such changes in clear lenses at the time of silicone oil removal. Miyamoto et al. 14 studied ultrastructural changes in the posterior surface of the anterior capsule following lensectomy and vitrectomy with or without silicone oil tamponade in rabbits and reported the presence of many vacuoles on the capsular surface, suggesting the deposition of emulsified silicone oil droplets. This was also apparent in this study, wherein we detected many vacuoles among accumulated Golgi bodies in the cytoplasm that contained engulfed silicon oil droplets. We also observed evidence of epithelial cell proliferation and multilayering of lens epithelium cells, as has been described previously by Koch et al. 6 who investigated anterior capsulorrhexis in vitrectomized eyes filled with silicone oil. Rossi et al. 15 showed that the presence of filopodia-like extensions in lens anterior capsule was due to altered structure of the capsule in addition to defective adhesions between cells that were stimulated to send extensions. Our study supported this view as we found surface alterations in the capsule and intercellular junctions on scanning electron microscopic examination of group A specimens.
Lens epithelial cell flattening was evident in this study, but the pathological findings did not extend to fibrous pseudometaplasia (spindle-shaped cells with collagen production), which was reported by Spraul et al. 16 in a study examining surgically excised posterior lens capsules of eyes with posterior subcapsular cataract that were filled with silicone oil. The flattening of epithelial cells observed in this study may represent a pathological stage before the development of spindle-shaped cells that migrate and form fibrous pseudometaplasia and posterior subcapsular cataract reported by Spraul et al. 16 In a study by Citirik et al., 5 they reported the presence of surface irregularities, pits, and depressions in the anterior lens capsule, and these were also clearly apparent in this study.
We propose that our findings in clear lens anterior capsules represent the first steps in a transformation to spindle-shaped cells, collagen production (fibrous pseudometaplasia), and migration to the posterior capsule, which lead to the clinically observable posterior subcapsular cataract which is a complication of silicone oil tamponade.5,16
There is high incidence of cataract formation after vitrectomy operation itself. Many explanations have been suggested to explain the development of post-vitrectomy cataracts, including either the damage of barrier role of the vitreous or the change of lens permeability, in addition to lens touch during surgery, lens toxicity, intravitreal steroids, or postoperative onset of uveitis.17–20 There is also high rate of cataract formation after vitrectomy for macular hole surgery with gas tamponade. 21 These findings may indicate that either vitrectomy itself or silicone oil or gas tamponade may have a role in the pathogenesis of postoperative cataract formation. These studies also may justify the procedure of combined phacovitrectomy done by many retina surgeons. 22
Our study only included patients who had been exposed to silicone oil for a minimum of 8 weeks, and further studies including eyes exposed to silicone oil tamponade for shorter durations should be performed to investigate the timing of the initiation of lens epithelial cell changes after silicone oil injection. In addition, this study may contribute to solving the issues associated with the timing of removal of the lens after retinal detachment vitrectomy surgery with silicone oil tamponade and could also justify combined phacovitrectomy procedures in cases with planned intraoperative silicone oil injection.
In conclusion, silicone oil may play a role in the development of apoptotic and histopathological changes in clear lens epithelial cells. Clarity of the lens at the time of silicone oil removal does not indicate an absence of cataractous changes. We found justification of combined clear lens extraction and silicone oil removal or combined phacovitrectomy when silicone oil injection is planned, but further long-term studies with larger patient groups are required. Our findings may reduce the burden associated with undergoing multiple surgeries after retinal detachment surgery.
Footnotes
Acknowledgements
W.S. performed the surgeries, M.S. and K.A. did the analysis, and D.E. and A.N. made the histopathology and electron microscopic work. All authors wrote the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.