
Abstract
Purpose:
To compare the optic nerve head morphology among primary open-angle glaucoma, non-arteritic anterior ischemic optic neuropathy eyes, their fellow healthy eyes and control eyes, using spectral-domain optical coherence tomography with enhanced depth imaging.
Methods:
Observational cross-sectional study including 88 eyes of 68 patients. In this study, 23 non-arteritic anterior ischemic optic neuropathy eyes, 17 fellow unaffected eyes, 25 primary open-angle glaucoma eyes, and 23 age-matched control eyes were included. Peripapillary retinal nerve fiber layer thickness and optic disk area were evaluated. Bruch’s membrane opening diameter, optic cup depth, anterior lamina cribrosa depth, and prelaminar tissue thickness were assessed.
Results:
Non-arteritic anterior ischemic optic neuropathy and primary open-angle glaucoma eyes had similar visual field mean deviation and peripapillary retinal nerve fiber layer thickness (P = 0.6 and P = 0.56, respectively). Bruch’s membrane opening diameter was significantly larger in primary open-angle glaucoma eyes than in control eyes (P = 0.02). Lamina cribrosa and disk cup were deeper in eyes with primary open-angle glaucoma than both control and non-arteritic anterior ischemic optic neuropathy eyes (P < 0.001). Prelaminar tissue thickness was significantly thinner in primary open-angle glaucoma eyes than in non-arteritic anterior ischemic optic neuropathy eyes (P < 0.001). Lamina cribrosa was shallower in both non-arteritic anterior ischemic optic neuropathy and unaffected fellow eyes compared to healthy eyes (P < 0.001 and P = 0.04, respectively). No differences were found in the optic disk area.
Conclusion:
A forward lamina cribrosa placement and not a smaller disk could be involved in the pathogenesis of non-arteritic anterior ischemic optic neuropathy. A significantly larger Bruch’s membrane opening diameter was found in primary open-angle glaucoma eyes compared with control eyes. This issue has clinical implications because Bruch’s membrane opening has been considered a stable reference for disk-related measures.
Keywords
Introduction
Glaucoma is a multifactorial optic neuropathy with an acquired and progressive loss of retinal ganglion cells (RGCs). Lamina cribrosa (LC) has been considered as the primary site for axonal damage.1–6 It provides both structural and functional support to the RGC axons working as a natural barrier between high intraocular pressure and low retrobulbar pressure 7 so that its deformation could lead to axonal damage through various mechanisms.8–10
Non-arteritic anterior ischemic optic neuropathies (NAIONs), characterized by acute clinical presentation due to acute ischemic damage to the optic nerve, leads like primary open-angle glaucoma (POAG), that is, a chronic progressive optic neuropathy, to an irreversible loss of RGC. Furthermore, NAION and POAG show other clinical, morphological, and histopathological differences.11,12
Spectral domain optical coherence tomography (SD-OCT) with enhanced depth imaging (EDI), by increasing penetrance and axial resolution provides better visualization of the LC and its surroundings.13–17 Using this technique, several studies have reported a backward LC displacement in patients with POAG compared to healthy subjects and have evaluated its impact on visual field progression.18–21 However, information regarding LC position in other non-glaucomatous optic neuropathies is scarce.22,23 Some authors have reported that eyes with POAG 22 or normal tension glaucoma (NTG) 23 had a deeper LC than NAION eyes.
The purpose of this study was to compare the optic nerve head (ONH) morphological features among eyes with POAG, NAION eyes and their healthy unaffected fellow eyes, and healthy control eyes. As there are some clinical similarities between glaucomatous and ischemic optic neuropathies, studies in both conditions could help us recognize ONH morphological differences, improve diagnosis, and identify the mechanism of optic nerve damage with the goal of protecting RGCs.
Methods
Subjects
This cross-sectional study included eyes with POAG, eyes with NAION matched for visual field (VF) mean deviation (MD), and age-matched control eyes. Unaffected fellow eyes of NAION were also included.
The study was approved by Hospital Ramón y Cajal Review Board. All participants provided written informed consent according to the Declaration of Helsinki.
Inclusion criteria for NAION were optic disk atrophy with a documented history of painless visual loss in one eye and optic disk swelling at least 6 months prior to the study. The mean time lapsed from the acute episode of NAION was 2.54 ± 2.33 years. The exclusion criteria for NAION patients were a suspicion of glaucoma and/or a baseline intraocular pressure (IOP) >21 mmHg and any ocular or neurologic disease other than NAION, especially arteritic anterior ischemic optic neuropathies (AION).
POAG was defined by the presence of a typical glaucomatous optic disk appearance, open-angle on gonioscopy and glaucomatous VF defects defined as: Glaucoma Hemifield Test outside normal limits on at least two consecutive VF tests, and/or the presence of at least three contiguous test points within the same hemifield on the pattern deviation plot at P < 0.01, with at least one point at P < 0.05. The mean follow-up time in our Glaucoma Department before recruitment was 3.52 ± 1.51 years.
Healthy controls, selected from the relatives of patients were age-matched subjects with best-corrected visual acuity (VA) of ⩾20/30, IOP of ⩽21 mmHg, normal optic disk appearance, and no VF or peripapillary retinal nerve fiber layer (pRNFL) damage.
In all groups, eyes with a refractive error greater than 5.0 diopters (D) of spherical equivalent or 3.0 D of astigmatism, prior ocular surgery other than uneventful cataract extraction, history of ocular or neurologic disease other than POAG or NAION were excluded.
All patients were evaluated by one of the authors (A.P.S.) and underwent a complete ophthalmic examination, including best-corrected logMAR VA, Goldmann tonometry and anterior segment, and funduscopic examinations. The axial length (AL) was obtained using IOLMaster (Carl Zeiss Meditec, Jena, Germany). Perimetry was performed with the standard Swedish Interactive Thresholding Algorithm (SITA) using the 24-2 pattern on the Humphrey Field Analyzer (Carl Zeiss Meditec, Dublin, CA, USA).
Spectralis OCT imaging
All subjects underwent pRNFL measurement using the new Glaucoma Module Premium (GMP) Edition and ONH scanning using the EDI technique provided by Spectralis (Heidelberg Engineering GmbH, Heidelberg, Germany). Images with segmentation errors, poor centration, or poor quality were excluded from analysis.
The new GMP Edition includes 24 radial and 3 circular scans. We registered the data provided by the inner circle scan (3.5 mm, standard). Bruch’s membrane opening (BMO)-based minimum rim width (MRW) is measured from radial B-scans automatically centered at the ONH. Retinal nerve fiber layer (RNFL) thickness measurements of each individual eye are normalized for anatomic orientation of the fovea-to-BMO-center axis to ensure accurate and consistent positioning of the pRNFL thickness profile across eyes. The optic disk area was also registered.
ONH scanning was performed using the EDI technique. The OCT device was set to image a 15 × 10° vertical rectangle centered on the optic disk. The closest vertical scan to the ONH center where the visibility of the anterior LC surface was complete (without including main vessels) was selected.
A reference line connecting the two ends of the BMO was defined as the BMO diameter. Three equidistant points (inferior, middle, and superior), corresponding to one-half and one-third of the reference, were highlighted and connected from this reference line to the anterior face of the prelaminar tissue (PT) and the anterior surface of the LC. 24
Optic disk cup excavation was defined as the distance between the reference line and the anterior surface of the PT, and prelaminar tissue thickness (PTT) as the distance between the anterior surfaces of the PT and LC. Lamina cribrosa depth (LCD) was defined as the distance from the reference line to the anterior surface of the LC. All these parameters were measured by the same observer (A.P.S) using the manual caliper tool at the above-mentioned three points, and the arithmetic mean of the three measurements was registered as the average.
Data analysis
Demographic characteristics of the patients were compared by independent samples two-tailed t-test and chi-square test. A comparison among NAION, unaffected fellow eyes, POAG and control eyes was performed using analysis of variance (ANOVA) test with Bonferroni post hoc analysis for continuous variables and chi-square test for categorical variables. Pearson’s test was used to evaluate the association among several ONH parameters, as well as with the IOP.
To evaluate intraobserver and interobserver reproducibility of ONH measurements, 10 randomly selected EDI-OCT scans were remeasured by the same and by a second observer (V.D.J), and the intraclass correlation coefficients were calculated. Statistical analyses were performed using SPSS software version 17 (SPSS, Inc, Chicago, IL, USA). A probability value of P < 0.05 was considered statistically significant.
Results
Initially, a total of 100 eyes of 74 patients were included in this study. Six patients with NAION had to be excluded, four due to poor quality of the images of the LC, and two because of poor collaboration when performing the EDI test.
In total, 88 eyes of 68 patients were evaluated in this study. Both eyes of three patients with sequential NAION were included in the NAION group. When both eyes of patients with POAG or healthy subjects were valid for the study, only one eye was chosen at random. Table 1 shows the main demographic and clinical characteristics of the patients included in the study. There were no statistically significant differences in age, gender, and AL among groups.
Demographics and clinical features of all included eyes.
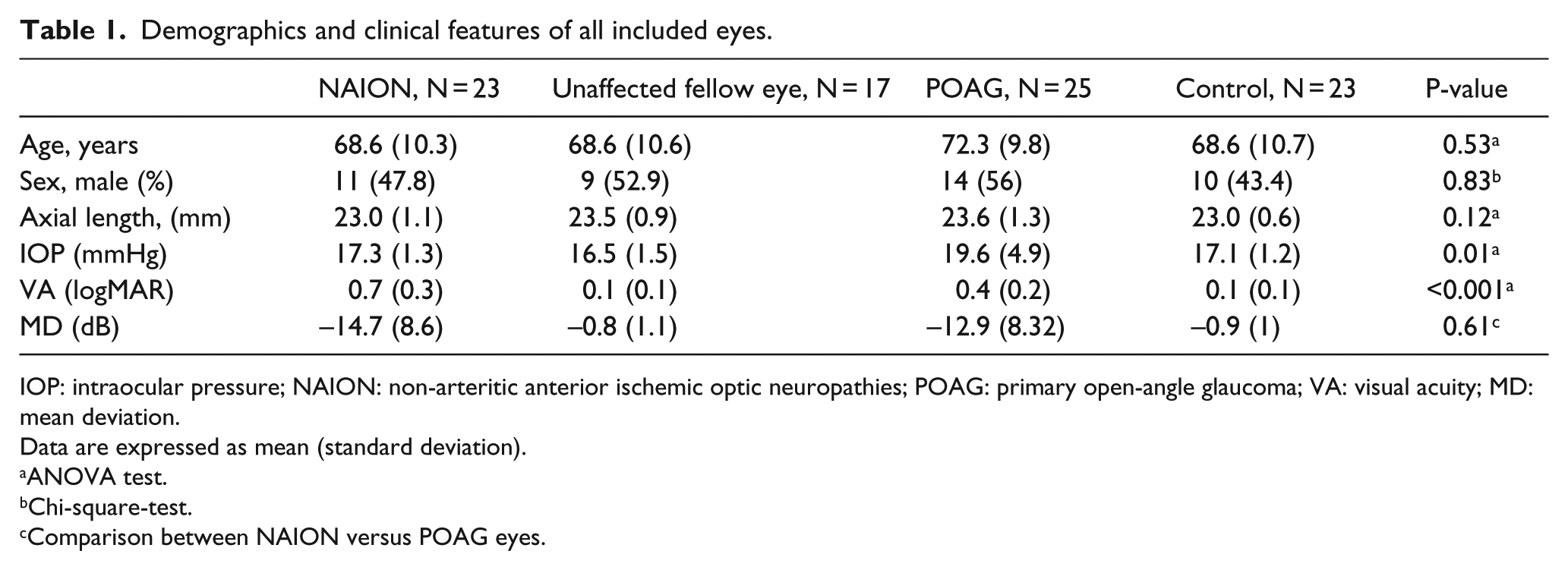
IOP: intraocular pressure; NAION: non-arteritic anterior ischemic optic neuropathies; POAG: primary open-angle glaucoma; VA: visual acuity; MD: mean deviation.
Data are expressed as mean (standard deviation).
ANOVA test.
Chi-square-test.
Comparison between NAION versus POAG eyes.
The mean IOP was higher in the POAG eyes than in NAION, unaffected fellow, and control eyes (P = 0.01), but no differences were found between NAION and control eyes (P = 0.89).
There was no significant difference in VF MD between NAION and glaucoma groups (P = 0.61).
There was no significant difference in average pRNFL between the NAION and POAG groups (P = 0.56), but both groups showed thinner pRNFL when compared to control and unaffected fellow eyes (P < 0.001).
All ONH measurements showed an excellent intraobserver and interobserver reproducibility, Interclass Coefficient Correlation (ICC) ranging from 0.974 to 0.999 (Table 2).
Interclass Coefficient Correlation (ICC) for optic nerve head measurements.
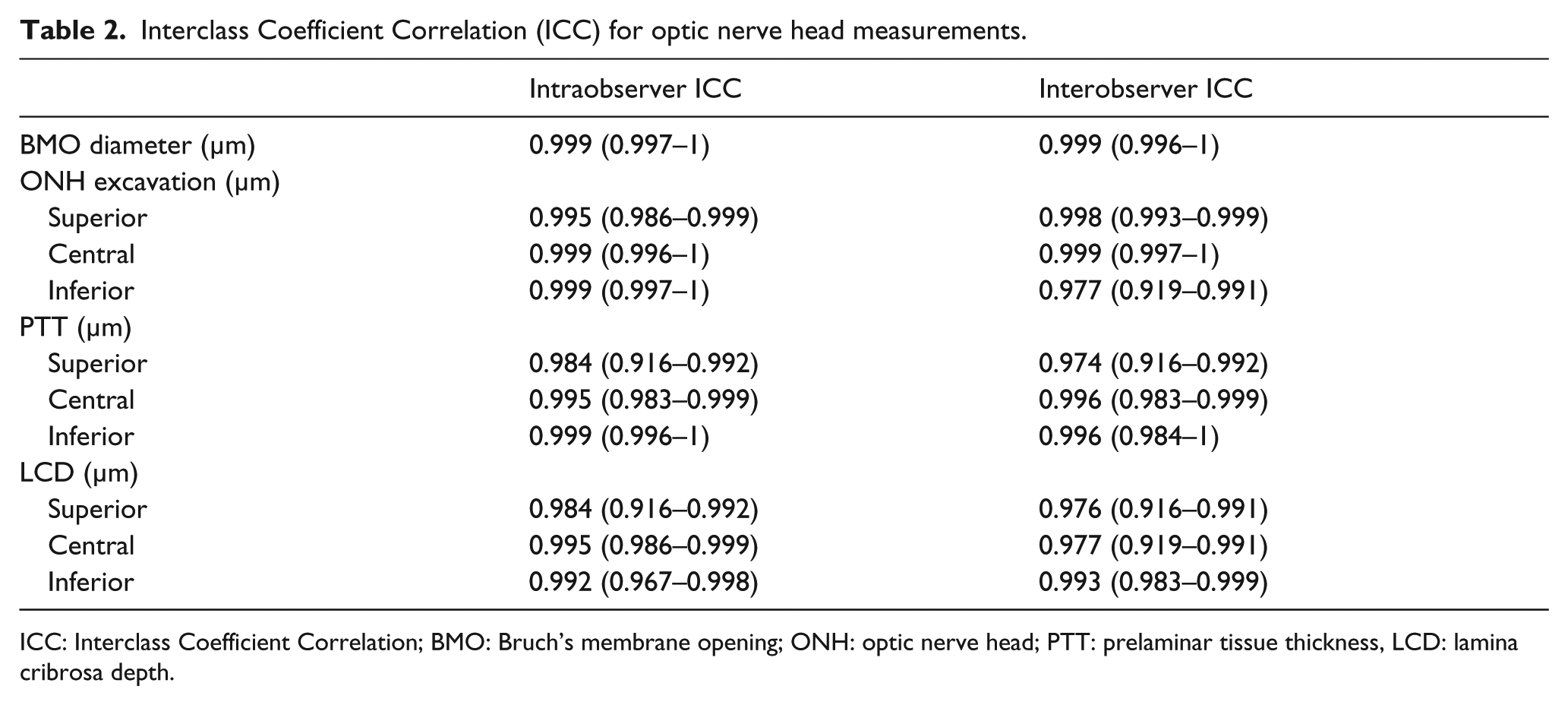
ICC: Interclass Coefficient Correlation; BMO: Bruch’s membrane opening; ONH: optic nerve head; PTT: prelaminar tissue thickness, LCD: lamina cribrosa depth.
Overall, significant differences were found in BMO diameter, ONH excavation, PTT, and LCD among the four groups (P < 0.01). Data are shown in Table 3.
Comparison of optic nerve head and lamina cribrosa parameters among the groups.
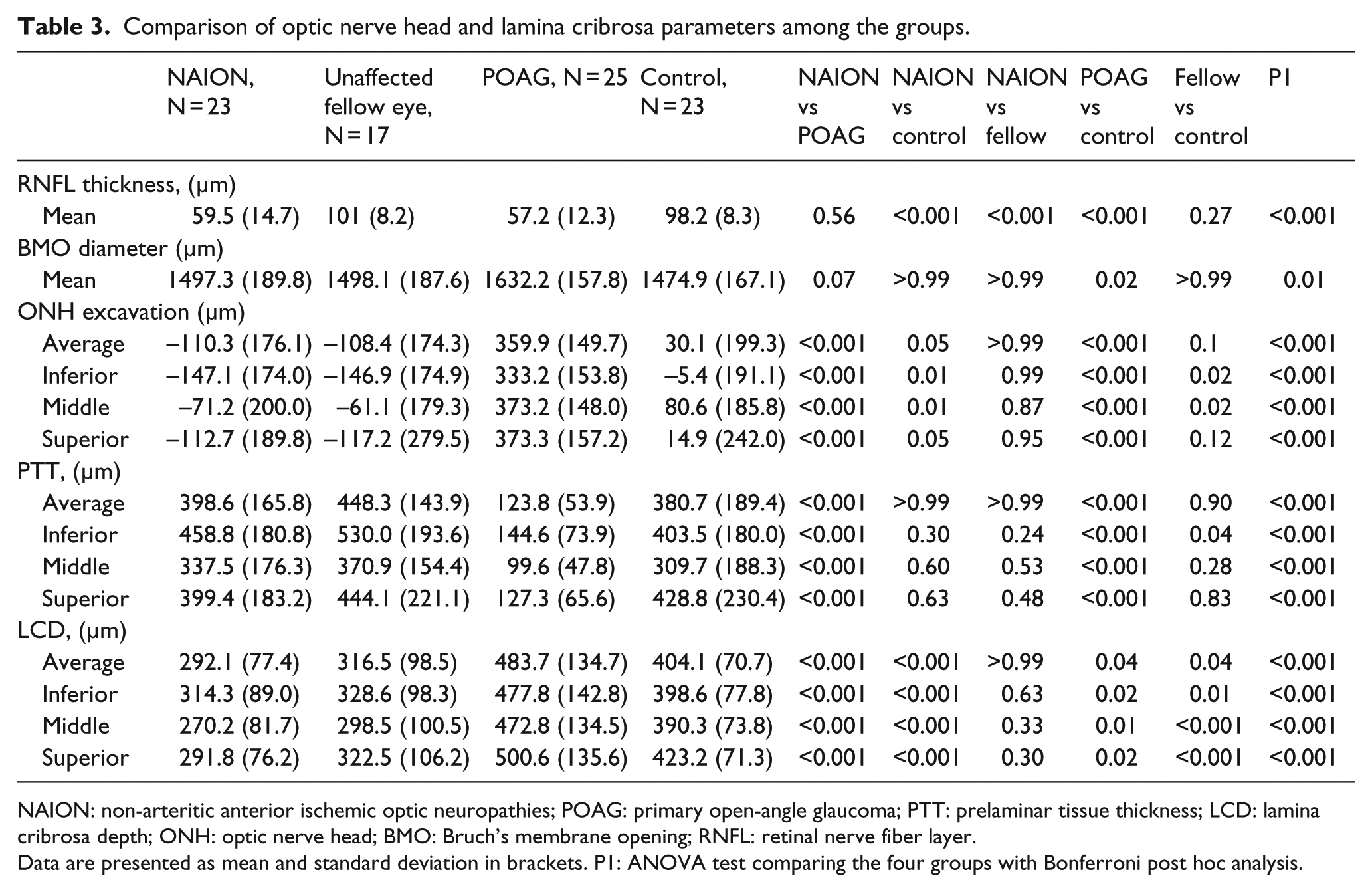
NAION: non-arteritic anterior ischemic optic neuropathies; POAG: primary open-angle glaucoma; PTT: prelaminar tissue thickness; LCD: lamina cribrosa depth; ONH: optic nerve head; BMO: Bruch’s membrane opening; RNFL: retinal nerve fiber layer.
Data are presented as mean and standard deviation in brackets. P1: ANOVA test comparing the four groups with Bonferroni post hoc analysis.
The BMO diameter was 10.7% greater in POAG than in control eyes (1632.2 µm vs 1474.9 µm, respectively, P = 0.02).
A significantly deeper excavation was observed in POAG eyes when compared to both control and NAION eyes (P < 0.001). Similar significant differences were found at the three points of measurement (P < 0.001; Table 3).
The average mean PTT was thinner in POAG eyes compared to control eyes (123.8 µm vs 380.7 µm, respectively, P < 0.001) and NAION eyes (123.8 µm vs 398.6 µm, respectively, P < 0.001). There was marked PT thinning at the inferior, middle, and superior points in POAG eyes compared to control and NAION eyes (P < 0.001). There were no statistically significant differences between NAION and control groups (Table 3).
Eyes with POAG had a deeper LC than healthy (483.7 µm vs 404.1 µm, respectively, P = 0.04) and NAION eyes (483.7 µm vs 292.1 µm, respectively, P < 0.001). Deepening of LC was significant at the inferior, middle, and superior measurements in POAG compared to healthy (P < 0.03) and compared to NAION eyes (P < 0.001). By contrast, average, superior, middle, and inferior LCD were lower in NAION eyes compared to control eyes (P < 0.001) and in unaffected fellow eyes compared to control eyes (P < 0.05; Table 3).
No differences were found in BMO disk area between NAION, unaffected fellow eyes and control eyes (1.74 ± 0.37 vs 1.74 ± 0.38 vs 1.70 ± 0.39 mm2, respectively, P = 0.95).
Overall, there was a significant correlation between IOP and both, average ONH excavation and average LCD (0.31, P < 0.001, and 0.31, P < 0.001, respectively). On the contrary, we found an inverse correlation between IOP and average PTT (–0.23, P = 0.25). Average ONH excavation was directly correlated with the mean LCD and BMO diameter (0.69, P < 0.001, and 0.45, P < 0.001, respectively) but inversely correlated with average PTT (–0.88, P < 0.001). The pRNFL thickness was directly correlated with the mean PTT (0.33, P < 0.001) and inversely with the optic disk excavation (–0.27, P = 0.01).
The mean AL was directly correlated with the mean optic disk excavation (0.21, P = 0.03) and inversely with the mean PTT (–0.23, P = 0.03).
In the univariate analysis, we found a significant association between the mean age and the LCD only in POAG eyes (–0.511; P = 0.00), but it was not significant in the multivariate analysis (P = 0.83).
Discussion
RGC loss takes place in several optic neuropathies. In this study we have compared the ONH structures between NAION and POAG.
Histological, experimental, and clinical studies have shown morphological changes in the ONH after artificial induction of IOP elevation, including an increase in ONH excavation, a decrease in PTT, and a backward LC displacement, suggesting that the ONH has viscoelastic properties.24–29 In contrast, a forward LC displacement and PT thickening have been observed following medical or surgical reduction of IOP.30–32
Unsurprisingly, we found a significantly deeper cup and LCD at all points of measurement in POAG group in comparison to both healthy and NAION groups. It has been reported that a thick PT can impair LC visualization and create a selection bias against healthy eyes. Furthermore, scans with a thicker PT had a low signal intensity. 33 In this study, although PT was significantly thicker in control and NAION eyes compared to POAG eyes (P<0.001), the anterior LC boundary was well delineated in all eyes. Apart from that, the mean signal intensity score was not significant different among groups (25.5, 24.7, 25.2, and 26.5 in NAION eyes, contralateral NAION eyes, POAG eyes, and healthy eyes, respectively, P = 0.81).
Despite a similar VF damage and pRNFL loss in both groups, the PT was thicker in NAION than in POAG eyes (P < 0.001). Our results are in line with those reported by Fard et al. 22 who found that eyes with POAG had greater LCD than control eyes and NAION eyes in all regions of the ONH and that the PT was thicker in NAION eyes than in POAG eyes, at similar levels of pRNFL thinning. Similarly, Lee et al. 23 found a greater LCD in NTG patients, followed by NAION patients, while PTT was thinner in NTG patients than in NAION patients (P < 0.001). These findings could be explained by the chronic effect of an increased IOP on the PT in the POAG group resulting in its mechanical compression that is not present in NAION eyes (19.6 vs 16.5 mmHg, P = 0.01). The PT is not only affected by axonal loss but also undergoes structural changes in response to IOP fluctuations. It is well known that a higher IOP can influence ONH conformation showing apart from a posterior LC displacement a significant thinning of the PT and the MRW, while the RNFL thickness is less affected by the IOP. 34 Danesh-Meyer et al., 35 using Heidelberg retina tomography, reported that glaucoma disks had significantly less disk rim tissue and a remarkable deeper cup than NAION, suggesting that glaucoma affects the LC connective tissues much more than NAION.
Although theoretically the BMO could enlarge or expand with IOP increase, 15 to the best of our knowledge, this is the first study to find a greater BMO diameter in patients with POAG than in control eyes. In the study by Fard et al., 22 this parameter was also greater in POAG eyes than in control eyes (1576 µm vs 1519 µm), but the difference was not significant. Differences in the severity of glaucoma damage could explain these differences. Fard et al. enrolled only patients with moderate to severe defects (MD: –16.28 ± 9.98 dB), whereas in this study, eyes with a mild defect were also included (MD: –12.9 ± 8.32 dB). It has been reported that posterior LC displacement occurs mostly in the preperimetric and mild-moderate glaucoma stages. 16 If the BMO behavior is related to glaucoma stage, as does the LCD is unanswered.
On the other hand, BMO expansion has been demonstrated immediately after intravitreal aflibercept injection 24 and in NAION eyes at onset that reversed with the follow-up. 36 ONH deformation by means of an IOP increase or optic nerve swelling can be explained by two mechanisms or forces; one pushing LC backwards and compressing the PT and other related to the hoop stress (inner circumferential pressure supported by the peripapillary sclera) which results in the sclera and BMO expansion. 7 Apart from the BMO enlargement during acute NAION, Rebolleda et al. 36 observed a significant posterior LC displacement that returned to normal in the atrophic stage, with no significant differences in LCD with the fellow unaffected eye. The above-mentioned mechanisms are present in both POAG and NAION eyes, but changes seem to be permanent just in glaucoma patients.
Contrary to previously published by Fard et al. 22 and Lee et al. 23 who did not find significant differences in the LC position between NAION and control eyes. In this study, we found a more anteriorly placed LC in both NAION and unaffected fellow eyes compared to control eyes (P < 0.001, P = 0.04, respectively). These differences could be explained by the shorter time lapsed since the NAION onset and inclusion in the study by Fard et al. 22 (3 vs 6 months). Apart from that Lee et al. 23 selected for LCD evaluation just the ONH sector affected by the disease.
Fard et al. 22 reported that the PT was thicker in NAION eyes than in control eyes. In contrast, we did not find any significant differences (P = 0.99). This discrepancy can be explained by the shorter time lapsed since NAION onset in their study.
A small optic disk has been considered a risk factor for NAION, but data regarding this issue are conflicting. Some authors have found that the disk area is significantly smaller in eyes of patients with NAION than in control eyes,37–39 while others did not confirm this finding.40–43 In our study no differences were found in BMO disk area between groups. These results suggest that NAION eyes have a shallower LC, and not a smaller optic disk as previously believed.37–39 A minor LCD observed in NAION and unaffected fellow eyes could act as a predisposing risk factor for NAION (Figure 1).
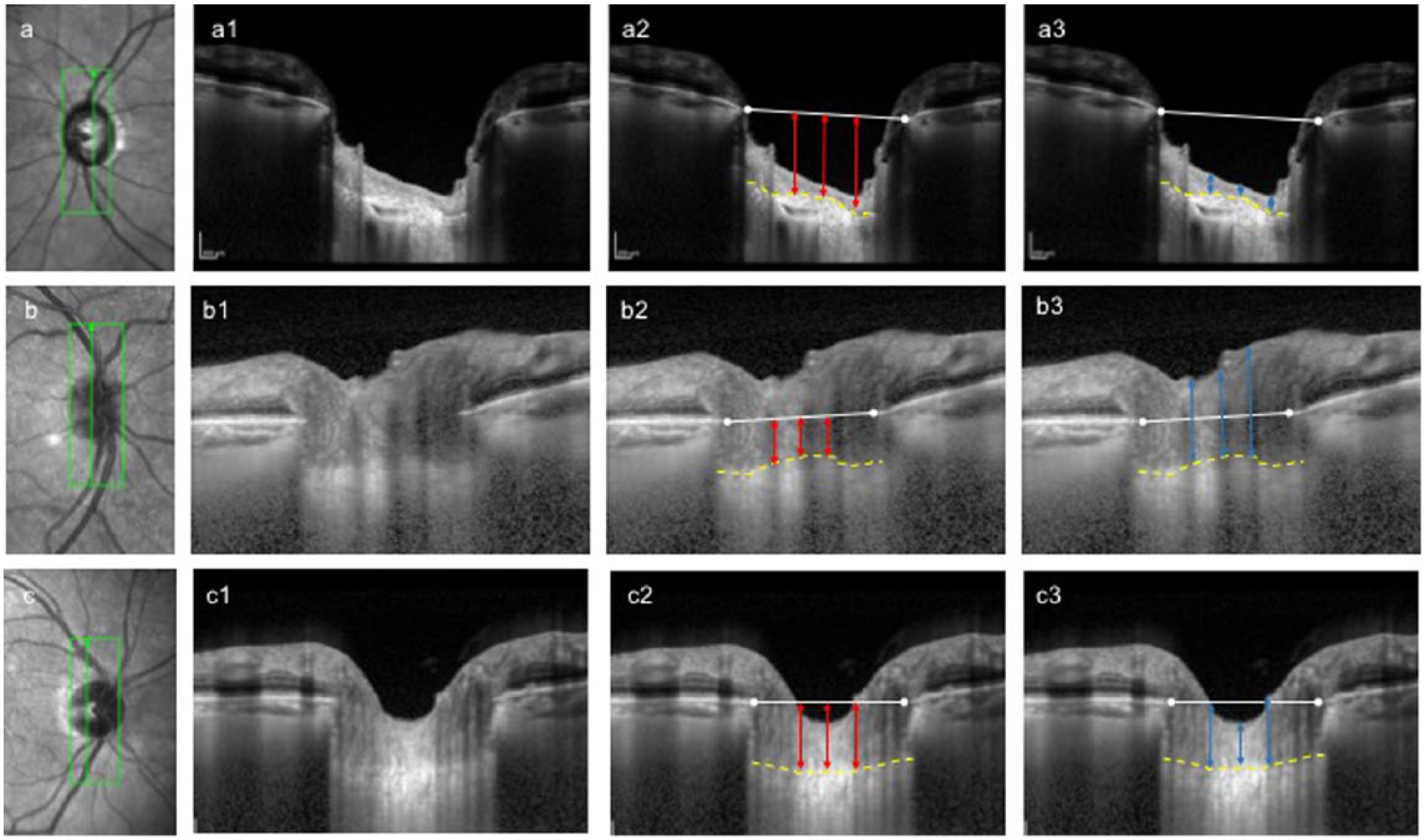
Infrared fundus images showing morphological differences in ONH deep structures among representative cases of (a) POAG, (b) NAION, and (c) healthy eyes. Images obtained at the vertical scan (green line) in an eye with POAG (a1), a prior NAION (b1), and a healthy eye (c1). White glyphs: BM termination points; horizontal white lines: reference lines indicating the level of BMO; yellow glyphs: anterior border of the LC. Same images as a2, b2, and c2, respectively, with labels (red lines) for LCD measurements at three locations (inferior, middle, and superior points); and same images as a3, b3, and c3, respectively, with labels (blue lines) for PTT at three locations. POAG eye is characterized by a deeper LC and thinner PTT. In contrast, NAION eye shows a thicker PTT and a more anteriorly placed LC.
Measuring LCD from the BMO reference plane includes the peripapillary choroidal thickness (PCT), which is known to be variable among individuals and influenced by several factors.44,45 PCT has been reported to be significantly thicker in NAION and unaffected fellow eyes than healthy eyes, using both manual37,42 and automated measurements; 43 therefore, in those eyes with a thick choroid, the LCD as measured from the BMO reference would be overestimated. Despite this confounding factor, in this study, the LCD was lower in NAION eyes than in control eyes, reinforcing this finding.
Our study has some limitations. First, it was limited by the relative small sample size. Besides that, three patients with sequential NAION were included in the statistical analysis, but it was powerful enough to reach statistical significance in all the parameters studied. Second, one single vertical scan was analyzed. However, only the highest-quality image and most centered vertical temporal scan without retinal vasculature was evaluated. Furthermore, NAION may cause segmental optic disk changes. Whereas, full information is not collected, we believe that the selected B-scan can be representative of the structural changes. In addition, all ONH measurements showed an excellent intraobserver and interobserver reproducibility supporting the reliability of our data. Third, to establish the temporary relationship between the observed morphological changes and the disease, a longitudinal prospective study is necessary. Finally, all eyes included in the study were Caucasian, and we excluded high ametropias. Therefore, our data cannot be extrapolated to other ethnicities or large refractive defects.
In summary, there were significant differences in ONH morphologic features among POAG, NAION, and healthy eyes using EDI SD-OCT. We found a shallower LC depth and not a smaller BMO-based optic disk area in NAION eyes compared to healthy controls, as well as greater BMO diameter and posterior LC placement in POAG eyes. These morphological differences may be helpful to clarify and better understand the differences between ischemic and glaucomatous optic nerve damage. Further longitudinal studies are necessary to confirm these findings.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.