
Abstract
Background:
The aim of this study was to assess the expression of cytokines/chemokines in tears from patients with non-advanced primary open-angle glaucoma and patients with non-severe dry eye disease versus healthy controls.
Methods:
This prospective, observational cohort study enrolled patients with confirmed or suspected non-advanced primary open-angle glaucoma who received any prostaglandin analogue monotherapy for longer than 6 months, patients with non-severe dry eye disease, and healthy controls. Expression of interleukin-1β, interleukin-2, interleukin-4, interleukin-5, interleukin-6, interleukin-8, interleukin-10, and interleukin-12; tumor necrosis factor α; vascular endothelial growth factor; granulocyte-macrophage colony-stimulating factor; and interferon γ was assessed.
Results:
107 participants were enrolled (primary open-angle glaucoma, n = 41; dry eye disease, n = 30; and healthy controls, n = 36). Compared with healthy controls, interleukin-6 was significantly higher (p = 0.0001) in patients with primary open-angle glaucoma and interleukin-1β (p = 0.0144), interleukin-6 (p < 0.0001), and interleukin-10 (p = 0.0392) were higher in patients with dry eye disease. Compared with patients with dry eye disease, patients with primary open-angle glaucoma had significantly lower levels of interleukin-4 (21.79 vs 20.18 pg/mL; p = 0.0012) and significantly higher levels of vascular endothelial growth factor (367.75 vs 609.28 pg/mL; p = 0.0058), tumor necrosis factor α (14.27 vs 17.93 pg/mL; p = 0.0048), and interleukin-6 (17.95 vs 27.48 pg/mL; p = 0.0145). In patients with primary open-angle glaucoma, interleukin-1β expression (p = 0.0011) was lower than in those who received intraocular pressure–lowering eye drops without preservatives compared with those who received eye drops with preservatives.
Conclusion:
Different cytokine/chemokine expression profiles in tears of patients with primary open-angle glaucoma and dry eye disease strongly suggest the involvement of a variety of signaling pathways in the pathogenesis of these ophthalmic processes.
Introduction
The term “glaucoma” encompasses different diseases characterized by progressive visual field defect secondary to retinal ganglion cell (RGC) loss. 1 The most prevalent type is primary open-angle glaucoma (POAG), which accounts for almost 80% of all cases.2,3 Glaucoma is the second leading cause of irreversible blindness worldwide.2,4 Because intraocular pressure (IOP) is considered the main risk factor in POAG, the first line of treatment is typically IOP-lowering eye drops, generally containing preservatives.
Dry eye disease (DED) is a complicated pathological condition affecting the ocular surface. 5 DED usually affects people over 60 years old and may be caused by internal or external injury including topical or systemic medications.5,6 DED could be classified into tear deficient and evaporative types but usually are combinations of the two forms seen in clinical practice.6,7 DEDs are also classified according to severity: mild, moderate, or severe.
Both diseases, glaucoma and DED, are associated with age. It is not uncommon to see clinical manifestations of DED in patients chronically treated with IOP-lowering eye drops. It has been shown in some studies that 66% of patients with severe DED also have glaucoma, 8 and around 60% of patients with glaucoma receiving topical therapy report DED symptoms9,10 that appear at the initiation of medical treatment. 11 These side effects may be triggered by the active compound, by the preservatives included in the formulation, or both. 12
Inflammation and immune response (IIR) processes in eyes are continuously stimulated with the intention of preventing and healing internal and external injuries. The main intermediaries of IIR processes include leukocytes, T-, B-, and natural killer lymphocytes and interconnections between these cells are modulated by cytokines, chemokines, and other molecules. 13 The idea that an abnormal activity of the immune system is involved in both anterior and posterior ocular segment disorders is supported by the altered levels of a wide spectrum of IIR mediators found in the blood, aqueous humor, vitreous body, and eye tissues.14–17 DED could be considered an immune-mediated ocular surface disorder. 15 Multiplexed flow cytometry assays, as an advance in biotechnology, could help us to understand the pathogenesis of eye diseases,18,19 and especially the ocular surface morbidities such as DED and glaucoma.
The main objective of the present study was to assess and compare the expression of IIR molecules in the tears of patients with POAG receiving IOP-lowering eye drops and patients with non-severe DED versus healthy controls. The expression of IIR molecules in the tears of patients with POAG receiving IOP-lowering eye drops with and without preservatives was also assessed.
Methods
Study design
This prospective observational cohort study enrolled suitable patients with POAG receiving IOP-lowering eye drops, patients with DED, and healthy controls who visited one of the study centers (Hospital of Jerez, Jerez de la Frontera, Cadiz, Spain; University and Ophthalmic Research Unit Santiago Grisolia, Valencia, Spain) for an ophthalmologic appointment.
The study protocol was approved by the ethics and clinical research committee of the Hospital del SAS de Jerez de la Frontera, Cádiz, Spain (CEI/11), and all procedures involving human participants complied with the 1964 Declaration of Helsinki, as revised in 2008. All patients provided written informed consent.
Patients were included in the study if they were aged >25 and <80 years and were deemed capable of following the study procedures. For inclusion in the POAG patient group: (1) patients had to have a non-advanced POAG with mild-to-moderate visual field defects 20 or be suspected of having POAG with normal visual field and (2) had to receive topical antiglaucoma treatment for at least 6 months. POAG treatment consisted of any topical prostaglandin (PG) analogue treatment regimen available at the time, including benzalkonium chloride (BAK)-preserved latanoprost 0.005% ophthalmic solution once daily, BAK-preserved bimatoprost 0.03% ophthalmic solution once daily, polyquaternium 1-preserved travoprost 0.004% ophthalmic solution once daily, and tafluprost 0.0015% ophthalmic solution once daily. For inclusion in the DED patient group, patients had to have mild-to-moderate disease according to the Ocular Surface Disease Index questionnaire 21 for more than 1 year. The control group consisted of healthy individuals.
Patients were excluded from the study if they wore contact lenses or had atopy or an allergic disorder; a history of refractive surgery; any systemic diseases and general treatments that may alter ocular surface, eyelid anomalies, severe blepharitis, meibomitis, or punctal occlusion; any other distinct ocular disorders, or if they received eye drops other than preservative-containing artificial tears or a PG analogue; or had a previous diagnosis of concomitant POAG and DEDs.
Prior to the first study visit, participants were required to discontinue, for at least 1 month, the use of nutritional supplements, systemic antihistamines, and treatments for DED (or meibomian gland disorder) such as antibiotics, nonsteroidal anti-inflammatory drugs, and corticosteroids, as well as artificial tears containing vitamins.
Study visits and tear sampling
During the first study visit, participants attended the ophthalmic clinic between 9 a.m. and 12 p.m. All patients underwent an ophthalmological examination, including Schirmer’s test (Type I), slit lamp examination of the anterior and posterior eye segment and the eye adnexa, and measurement of tear breakup time (BUT) with fluorescein. The following day, reflex tear samples were obtained using a gentle rubbing method by means of a capillary tube (Pasteur micropipette, 60 µL) from the inferior tear meniscus of both eyes. The collected tear samples were placed into cryotubes and stored at −80°C until processing. In cases of decreased tear production, the sampling maneuvers were repeated until an acceptable volume was obtained (approximately 30 µL). The tear sampling procedures have yet been published elsewhere.22,23
The level of expression of a number of cytokines and chemokines was assessed in the tear samples using the Luminex R-200 multiplex system (Luminex, Austin, TX, USA). As described by the manufacturer, this tool was designed to simultaneously multiplexing up to 100 analytes in a single well of a microtiter plate. Basically, the Luminex is a flow cytometry–based analyzer capable to perform immunodetection with a minimum amount of fluids (20 µL). Proper identification of the assayed molecules depends on bead color and fluorescence. This technique works using fluorescently labeled reporters associated with each target protein. Quantitation of unknown cytokine and chemokine expression levels were carried out by the Bio-Plex Manager software, using a standard curve that was generated with data from a recombinant cytokine sample. Optimizing the quantification of molecules present at the low tear sampling used herein, cytokine and chemokine levels were corrected for the initial total protein concentration of each sample during analysis. The molecules present in the human cytokine/chemokine bead-based panel were the following: interleukin (IL)-1β, IL-2, IL-4, IL-5, IL-6, IL-8, IL-10, and IL-12; vascular endothelial growth factor (VEGF); tumor necrosis factor α (TNF-α); granulocyte-macrophage colony-stimulating factor (GM-CSF); and interferon γ (IF-γ).
Statistical analysis
Data were recorded in Excel spreadsheets (Microsoft Corporation, Redmond, WA, USA) and analyzed with the SPSS 20.0 program (IBM Corp., SPSS Statistics for Windows, version 20.0, Armonk, NY, USA). Group sample size was calculated by power analysis. Demographic and clinical characteristics were studied with Chi-squared test for categorical variables and standard parametric tests for non-categorical variables. Cytokine/chemokine concentrations were expressed in picograms per milliliter (pg/mL), and mean and standard deviations (SD) were calculated for all analyses. Most cytokine and chemokine concentrations detected followed a non-homogeneous distribution (D’Agostino-Pearson test for normal distribution), so a non-parametric Mann–Whitney U test was selected to compare two independent sample groups, and Kruskal–Wallis test and the post hoc Tukey’s honestly significant difference (HSD) test were selected to compare three independent sample groups. All results were statistically analyzed to detect differences between groups, and p < 0.05 was considered statistically significant.
Results
Participants
A total of 116 participants were enrolled in the study; however, three patients in the POAG group and six patients in the DED group were not included in the main analysis as the tear samples obtained from these patients were not sufficiently large for analysis: in 92.2% of study participants the volume of tear samples obtained guaranteed detection.
After these exclusions, the overall study population consisted of 107 participants: POAG, n = 41; DED, n = 30; and healthy controls, n = 36 (total 214 eyes). No statistically significant differences between groups in baseline demographics were observed (Table 1); however, significant differences in clinical characteristics (Schirmer’s test scores and fluorescein tear BUT) were noted (Table 1).
Demographic and clinical characteristics of the study population.
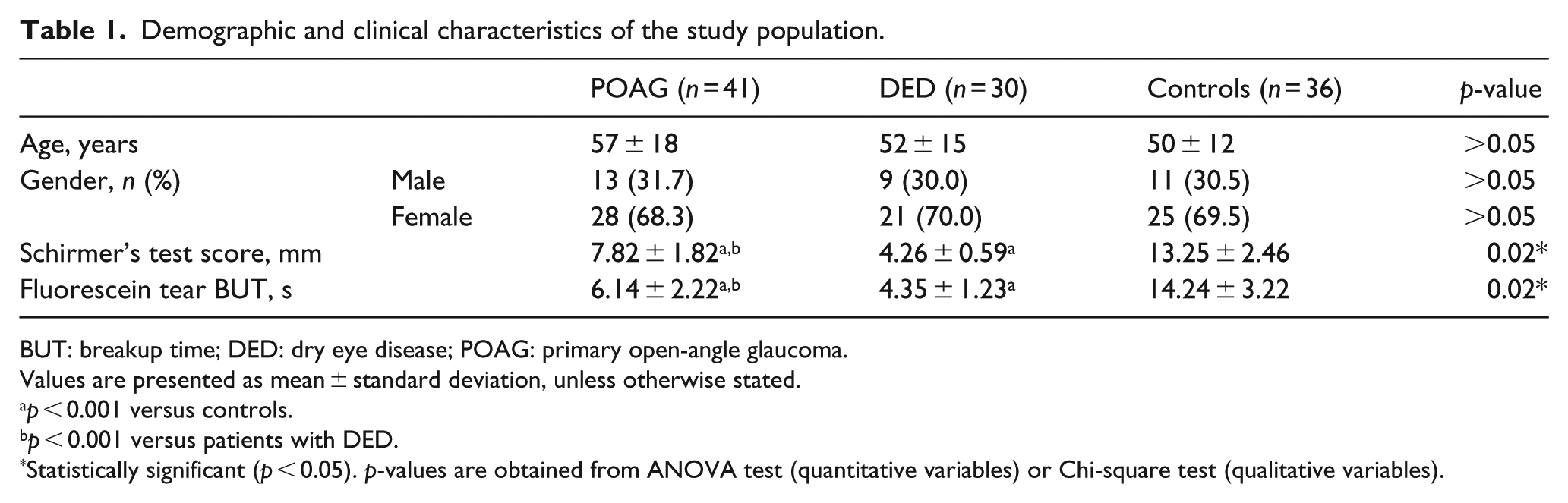
BUT: breakup time; DED: dry eye disease; POAG: primary open-angle glaucoma.
Values are presented as mean ± standard deviation, unless otherwise stated.
p < 0.001 versus controls.
p < 0.001 versus patients with DED.
Statistically significant (p < 0.05). p-values are obtained from ANOVA test (quantitative variables) or Chi-square test (qualitative variables).
Cytokine/chemokine levels
There were a number of differences in cytokine and chemokine expression between the patient groups and the healthy controls. Compared with the healthy controls, patients in the POAG patients had significantly higher levels of expression of IL-6 (p = 0.0001), while patients in the DED group had higher levels of IL-1β (p = 0.0144), IL-6 (p < 0.0001), and IL-10 (p = 0.0392) and lower levels of VEGF (p = 0.0042; Table 2).
Cytokine and chemokine profile in tears from overall study population.
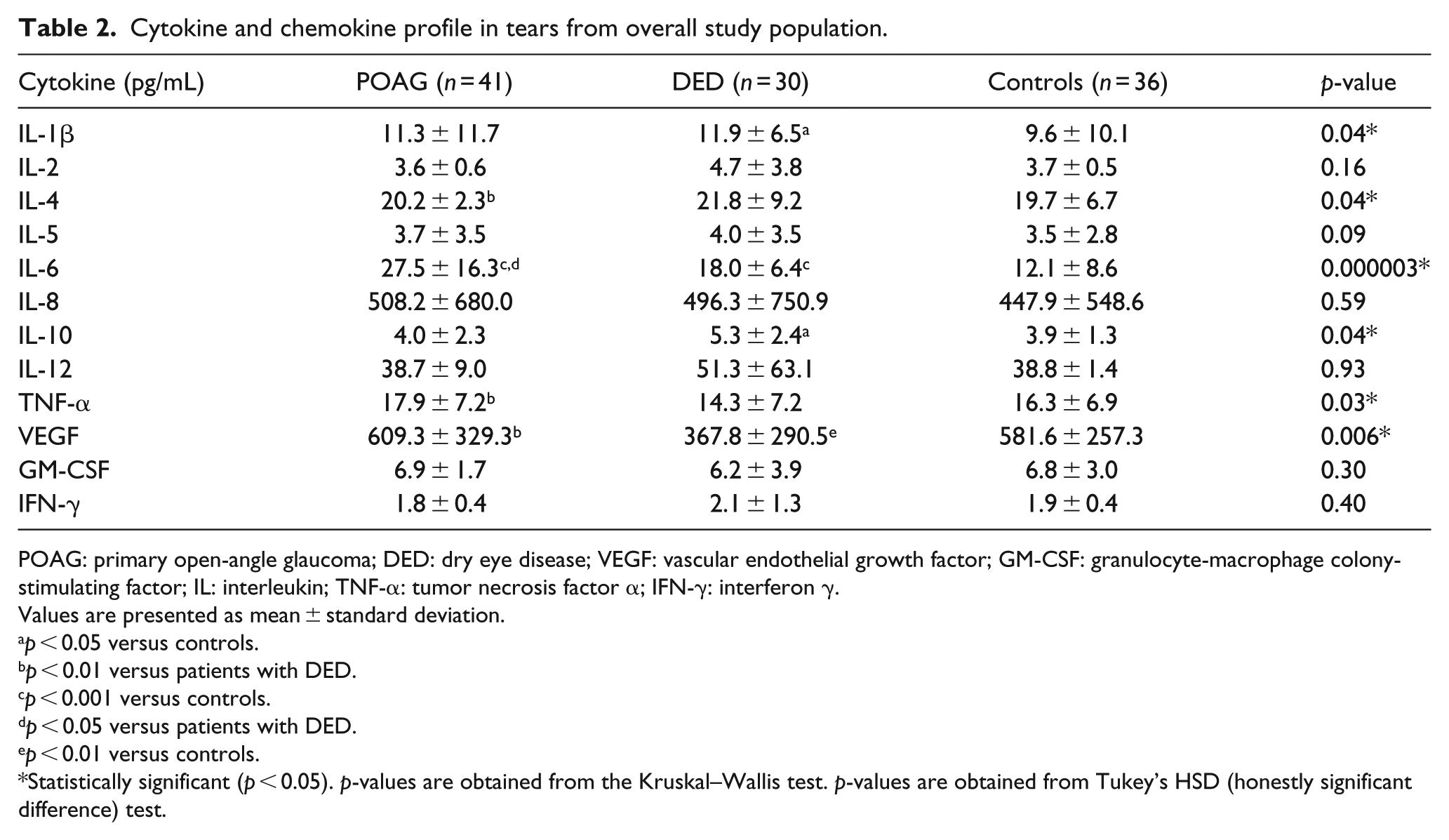
POAG: primary open-angle glaucoma; DED: dry eye disease; VEGF: vascular endothelial growth factor; GM-CSF: granulocyte-macrophage colony-stimulating factor; IL: interleukin; TNF-α: tumor necrosis factor α; IFN-γ: interferon γ.
Values are presented as mean ± standard deviation.
p < 0.05 versus controls.
p < 0.01 versus patients with DED.
p < 0.001 versus controls.
p < 0.05 versus patients with DED.
p < 0.01 versus controls.
Statistically significant (p < 0.05). p-values are obtained from the Kruskal–Wallis test. p-values are obtained from Tukey’s HSD (honestly significant difference) test.
There were also significant differences in cytokine and chemokine expression between the patient groups. IL-6 (p = 0.0145), TNF-α (p = 0.0048), and VEGF (p = 0.0058) levels were significantly higher in the POAG group, while IL-4 (p = 0.0012) levels were higher in the DED group (Table 2).
In the POAG group, patients who were receiving treatment with PG analogue eye drops without preservatives (n = 11) had significantly lower expression of IL-1β (p = 0.0011) than patients who were receiving treatment with PG analogue eye drops with preservatives (n = 30). There were no statistically significant differences in treatment duration between these subgroups (p = 0.2002; Table 3).
Cytokine and chemokine profile of tears and duration of treatment in patients with primary open-angle glaucoma receiving intraocular pressure-lowering eye drops with and without preservatives.
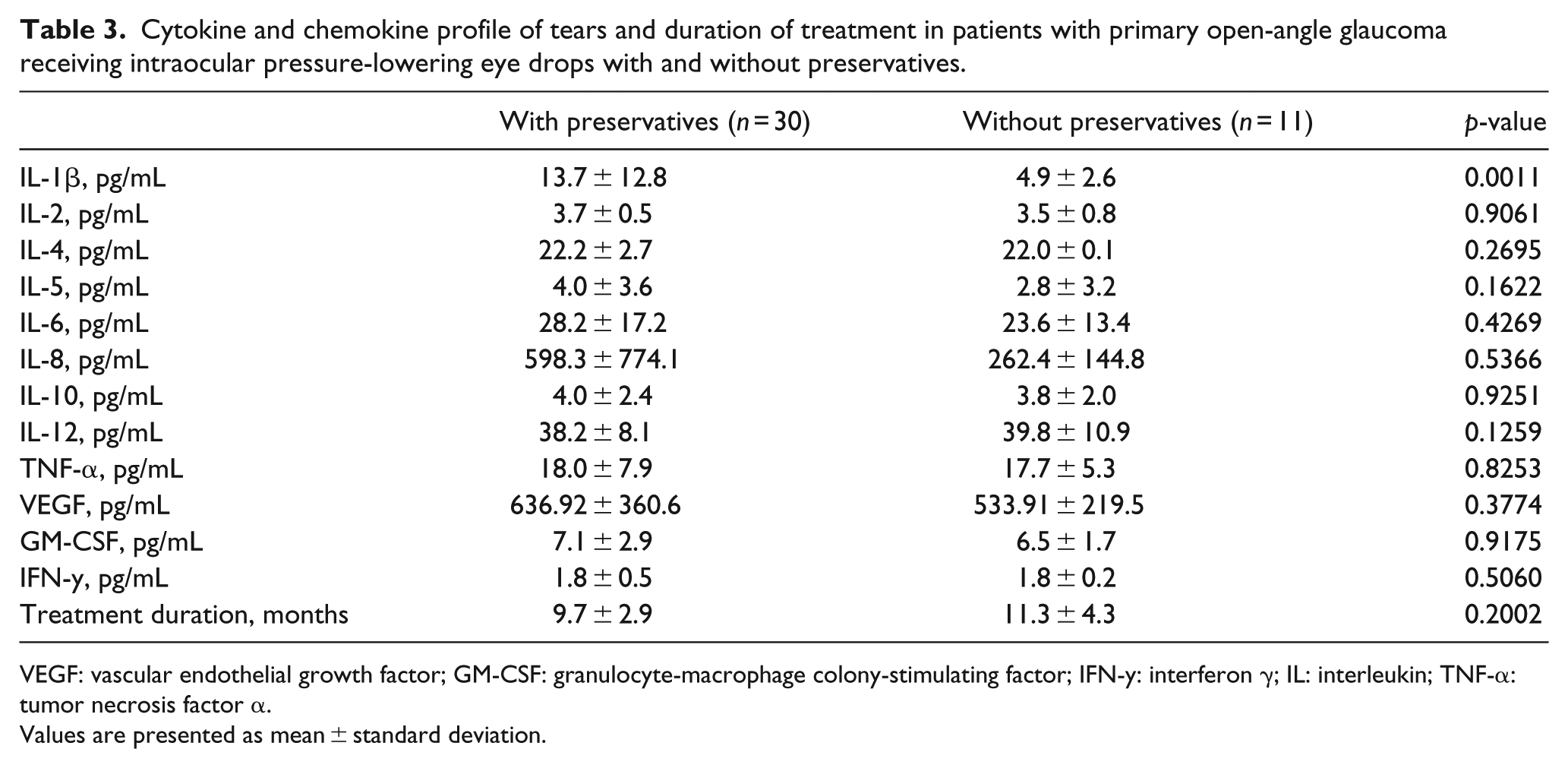
VEGF: vascular endothelial growth factor; GM-CSF: granulocyte-macrophage colony-stimulating factor; IFN-y: interferon γ; IL: interleukin; TNF-α: tumor necrosis factor α.
Values are presented as mean ± standard deviation.
Discussion
The aim of this study was to assess and analyze changes in the expression of IIR mediators in the tears of patients with, or those suspected of having, POAG and receiving IOP-lowering eye drops, as well as in patients with non-severe DED, versus healthy controls. This was done using a machine capable of simultaneously measuring several molecules in a single microplate well using small sample volumes. The method used in this study for collecting tears is noninvasive and relatively simple.
Glaucoma is a common ocular disease that remains the second leading cause of blindness worldwide. 4 DED is among the most common conditions observed in ophthalmological practice and has the highest prevalence rates worldwide. 6 The symptoms of DED include ocular discomfort, unstable vision, and impairment of daily activities.5–7 Furthermore, for reasons previously discussed, DED and glaucoma could be considered concomitant diseases.
In this study, patients with POAG and DED had significant changes in basic clinical DED tests. Schirmer’s test scores were significantly lower in patients with POAG and DED (both p < 0.0001) compared with the healthy controls, reflecting a low tear secretion in both patient groups. Furthermore, the fluorescein tear BUT was much shorter in the patients with POAG and DED (both p < 0.0001) compared with healthy controls, which reflects the unstable tear film in patients with POAG and DED compared with healthy controls.
A wide variety of cytokines and chemokines can be found in human tears to maintain the morphology and function of the ocular surface.24–26 An underlying cytokine/chemokine-mediated inflammatory disorder should be expected in all ocular surface alterations, regardless of etiology. However, some cytokines/chemokines are more important for enhancing the innate immune response and directing adaptive immunity toward a Th1- or Th2-dependent response. 27 In this sense, proinflammatory cytokines IL-1β and IL-6 are essential for the synthesis of proteins in the acute phase and occur in large quantities in response to infections and any type of stress. IL-10 is an anti-inflammatory cytokine synthesized by Th2 cells, monocytes, and B-lymphocytes, which inhibits production of proinflammatory cytokines.
In this study, tears collected from patients with POAG had a different expression profile of the analyzed cytokines and chemokines compared with healthy controls. Specifically, the concentration of IL-6 was significantly higher (p = 0.0001) in patients with POAG respect to the control individuals. As previously suggested, this proinflammatory cytokine is probably the underlying cause of most clinical manifestations of the ocular surface alterations in patients with POAG receiving medical treatment. 28 Higher levels of IL-6 (in addition to IL-8 and IL-10) in POAG patients undergoing hypotensive eye drops therapy compared with normal patients have been reported, 29 while monocyte chemoattractant protein-1 has been found to be the predominant cytokine elevated in tears of Asian patients with glaucoma receiving topical treatment. 30 This study also found a higher level of IL-6 in the POAG patients, although the increase was not statistically significant. Nevertheless, these results are not entirely comparable to the results of this study as the patient groups differed with regard to types of glaucoma and topical treatments received.29,30
In this study, patients with DED had highly variable etiology and included patients with any three of the known clinical types (aqueous deficient, evaporative, or combined form). Tear samples collected from these patients displayed significantly increased levels of IL-1β (p = 0.0144), IL-6 (p < 0.0001), and IL-10 (p = 0.0392) compared with the tear samples from the controls. The presence of these three molecules in tears of patients with DED confirms the activation of IIR processes in affected eyes. In fact, the results of this study are in agreement with previous reports,24–26,31–33 despite the differences in tear sampling and processing. IL-6 has been described as one of the key molecules in DED.25,34 It has been associated with a number of clinical characteristics in patients with severe DED 35 and could be used as a biomarker of severity. It raises a small controversy the significantly lower VEGF expression (p < 0.01) found in our patients with DED as compared to the healthy controls. Most of the studies stated that VEGF levels were increased in tear samples from non-severe DED patients, 15 particularly in those with evaporative-type DED. 24 But, VEGF could be the prototypic example of the crosstalk between nerves and vessels, 36 and it is likely that our DED patients suffered from a mild neurotrophic epitheliopathy 37 that caused a reduced expression of the VEGF. Anyway, this finding will require further research.
This study also assessed whether there were any differences in the expression of IIR mediators in the tears of patients with non-severe DED and patients with POAG receiving treatment with IOP-lowering eye drops. Significant differences in the levels of TNF-α (p = 0.0048), IL-4 (p = 0.0012), IL-6 (p = 0.0145), and VEGF (p = 0.0058) were found between these groups. The different molecules identified in the ocular surface of these two clinically similar alterations may indicate a common inflammatory basis, but with the intervention of distinct signaling pathways. Interestingly, similar conclusions were reached before in a study that compared tear protein expression patterns between the two groups using principal component analysis. 38 Another study suggested that these molecules could be used to design new treatments for patients with ocular surface dysfunction. 39
The role of preservatives with detergent activity in the concurrence of ocular surface disease in patients with POAG receiving IOP-lowering therapies is well established.40–42 In this study, 30 patients in the POAG group received topical treatment with a PG analogue formulation that contained a preservative, while 11 patients in the POAG group received a PG analogue formulation that did not (tafluprost 0.0015%). Compared with patients who received the PG analogue formulation without preservatives, patients who received the formulation with preservatives had higher values of IL-1β (p = 0.0011). IL-1β and IL-6 molecules are considered relevant markers of DED. 43 Nevertheless, similar results have been found when comparing patients using preserved versus non-preserved latanoprost. 44 In this particular study, unlike ours, patients were treated only with latanoprost and for a longer period of time when evaluated. 44 In any case, these results could be explained on the basis of an inflammatory activity related to the toxic effect of preservative-containing formulations. Interestingly, Jee et al. 45 described decreased levels of IL-1β and TNF-α in tears from patients with preexisting DED who were treated with preservative-free sodium hyaluronate and preservative-free fluorometholone eye drops after surgery for cataracts. Findings of these studies highlight the need for further research with larger patient samples to elucidate the specific roles of preservatives and other components of eye drops in the IIRs of patients with POAG receiving medical treatment.
This study had several limitations. First, the majority of the IIR molecules were expressed in tears by showing an abnormal distribution. While non-parametric tests were performed to enable comparison between groups, the abnormal distribution could reduce the power of the study. Second, the small sample size could limit the reliability of the analysis of the POAG patients. It is also plausible that the tear collecting technique could influence the type of molecules detected, as suggested before. 46 This should be taken into account when designing new studies in this area. Another limitation is the fact that this study was conducted in Caucasian patients with suspected or early-to-moderate stage POAG and mild-to-moderate DED. Due to these limitations, caution is recommended when extrapolating the results to other populations.
In conclusion, increased levels of IL-6 were found in patients with POAG or those suspected of having POAG, who were receiving treatment with IOP-lowering eye drops. Furthermore, in patients with mild-to-moderate DED, increased levels of IL-1β, IL-6, and IL-10 were also detected. Significant differences in the expression of IIR mediators were found between the tears of patients with non-severe DED and patients with POAG. The elevated IL-6 levels in tears from the POAG patients and the increased levels of IL-1β and IL-6 in tears from the DED patients may be contributing to the clinical manifestations of these diseases. In this scenario, the molecular basis of POAG and/or DED, and the use of tear sampling, may offer ophthalmologists and researchers new strategies for further investigation on the role of presumptive biomarkers for POAG/DED diagnosis and therapy. Larger trials with a greater number of participants may help to devise guidelines for the diagnosis and treatment of these common diseases.
Footnotes
Acknowledgements
The authors thank Gemma Odena, PhD, on behalf of Springer Healthcare Communications, who provided editorial assistance in the drafting of this manuscript. Georgii Filatov, Springer Healthcare Communications, performed English edit of the text and prepared the manuscript for submission. This assistance was funded by Santen Pharmaceutical. Santen Pharmaceutical had no role in the content of the manuscript, which was entirely the authors’ responsibility. All authors have approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in this study were approved by the Ethics and Clinical Research Committee of the Hospital del SAS de Jerez de la Frontera. The study was conducted in accordance with the ethical standards of the 1964 Declaration of Helsinki, as revised in 2008.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financed by a research grant (SAS/11202) from the Junta de Andalucía, Servicio Andaluz de Salud, Sevilla, Spain (PI: Javier Benitez-del-Castillo, 2011–2012).
Informed consent
Informed consent was obtained from all individual participants included in the study.