
Abstract
Purpose:
To evaluate, through the in vivo confocal microscopy, the pathological changes of each corneal layer in eyes affected by pseudoexfoliation syndrome.
Methods:
We studied 40 eyes of 40 patients with diagnosis of unilateral senile cataract associated with pseudoexfoliation syndrome and 40 eyes of 40 control subjects with senile cataract without pseudoexfoliation syndrome. All patients underwent a complete ophthalmic examination including best corrected visual acuity, slit-lamp examination, corneal sensitivity measurement using a Cochet-Bonnet nylon thread esthesiometer, and anterior segment optical coherence tomography (Visante OCT, Carl Zeiss Meditec AG, Germany); in vivo confocal microscopy of corneal sections (endothelium, stroma, sub-basal nerve plexus, and superficial and basal epithelium) was performed with the ConfoScan 4.0 (Nidek, Japan).
Results:
In pseudoexfoliation syndrome group, the mean corneal sensitivity was 44.1 ± 1.3 mm and in the control group was 55.6 ± 4.7 mm. The corneas of the eyes with pseudoexfoliation syndrome were significantly less sensitive than those of control group eyes (p < 0.001). Pseudoexfoliation syndrome eyes had a lower nerve density and less nerve beadings and a higher degree of tortuosity in sub-basal plexus compared to the control group. The cell density of epithelial and endothelial layers was significantly lower in pseudoexfoliation syndrome eyes than controls. In 80% of pseudoexfoliation syndrome eyes, we found activated keratocytes and inflammatory cells in the anterior stroma.
Conclusion:
Our study demonstrates the morpho-structural corneal alterations in eyes affected by pseudoexfoliation syndrome, using corneal in vivo confocal microscopy as a non-invasive and high-reproducible technique to evaluate pathophysiology of each corneal layer; the sub-basal nerve plexus alterations are correlated with the lower corneal sensitivity.
Introduction
Pseudoexfoliation syndrome (PEX) is an age-related disorder characterized by the deposition of abnormal extracellular fibrillar material in ocular tissues. It is now well established that this disorder does not affect only the eye, as immunohistochemical studies and electron microscopy revealed the presence of such deposits also in non-ocular tissues, such as the heart, blood vessels, kidneys, liver, lung, gall bladder, and cerebral meninges. 1 Nevertheless, the real impact of these changes on the organ dysfunction has not yet been demonstrated. 2 In this context, one of the most frequently described associations is the sensorineural hearing loss, 3 whose most intimate mechanisms, however, are not yet well established. In the eye, the PEX is responsible for a wide range of issues, including cataract, phacodonesis and zonulopathy, angle closure, keratopathy, and blood–aqueous barrier dysfunction that can lead to pseudo-uveitis and retinal venous occlusive diseases. 4 The deposition of a whitish material on the front surface of the lens or at the pupil edge is the classic ophthalmoscopic marker of this disorder. Although this syndrome is now well described, there is still much to understand about the exact mechanisms underlying the pathogenesis, evolution, and development of PEX-related eye disorders; in this context, in vivo confocal microscopy (IVCM) is proposed as a non-invasive imaging technique able to analyze the structures of the anterior segment of the eye and has recently been used in several studies to identify corneal changes related to PEX. 5
Our purpose is to analyze, relying on this technique, corneal abnormalities of eyes affected by PEX syndrome in order to document how this disorder involves all corneal layers and how this method can be useful in the evaluation of the anterior segment before ocular surgery.
Subjects and methods
Subjects
We studied 40 eyes of 40 patients with diagnosis of senile cataract associated with PEX (PEX group) and 40 eyes of 40 control subjects with senile cataract without PEX (control group).
This study was conducted between October 2015 and September 2016, at the Eye Clinic, Department of Surgery and Translational Medicine, University of Florence, Florence, Italy. Informed consent was acquired from subjects after a description of possible consequences of the procedures. The study adhered to the tenets of the Declaration of Helsinki and was approved by the local ethics committee.
Diagnosis of senile cataract associated with PEX was based on the presence of a classic exfoliation deposition pattern on the anterior lens capsule as a central gray disk, mid-peripheral clear ring, and peripheral gray rim. In all eyes, exfoliation material was observed by slit-lamp microscopy at the pupillary border and/or on the anterior lens capsule.
Exclusion criteria included the presence of systemic diseases, lymphoma, sarcoidosis, diabetes mellitus, systemic therapy with drugs that have known corneal toxicity; congenital, metabolic, or traumatic cataract; previous ocular surgery or ocular trauma; corneal edema, cornea guttata, corneal precipitates, corneal dystrophy, and ocular inflammation; glaucoma, ocular hypertension, and treatment with topical anti-glaucoma drugs, steroids, or non-steroidal anti-inflammatory drugs (NSAIDs); use of contact lenses; Stevens–Johnson syndrome; and other ophthalmic diseases.
All patients underwent a complete ophthalmic examination including best corrected visual acuity (BCVA), corneal sensitivity measurements, un-dilated and dilated slit-lamp examination, gonioscopy, ocular Goldmann applanation tonometry, and fundus examination.
Corneal sensitivity measurements
Central corneal mechanical sensitivity (CCMS) was tested using a Cochet-Bonnet nylon thread esthesiometer: the exam was carried out using a 60 mm length of nylon thread at the beginning, applied it perpendicularly to the central cornea, and reducing in subsequent tests the length of the wire by 5 mm each time, up to which the subject has perceived the contact. Each measurement was taken twice with a between-test interval of at least 5 min; the average of two measurements was used for the statistical analyses. 6
IVCM
IVCM of corneal sections was performed with the ConfoScan 4.0 (Nidek, Japan) connected to an immersion lens (Achroplan 40x/0.75 W; Carl Zeiss Meditec AG, Germany).
The cornea was anesthetized with oxybuprocaine chloride 0.4% (Novesina; Novartis Farma, Italy), then viscotears was administered (Carbomer 0.2%; CIBA Vision Europe Ltd, UK). The cornea was scanned with a probe 40X with magnification 500, acquiring 350 images in 25 s/exam.
The resulting two-dimensional images consisted of 768 × 576 pixels and covered an area of 460 μm × 345 μm. The lateral resolution was 0.62 μm/pixel, the optical resolution was ±5 μm, and the working distance was 1.98 mm, as stated by the manufacturer.7,8 The central cornea images were acquired in all subjects. Endothelium, stroma, sub-basal nerve plexus, and superficial and basal epithelium scans were selected for the analysis.
Cell density of the epithelium, stroma, and endothelium corneal study
Using the software provided by ConfoScan 4.0, the cell density in each layer was determined by a manual cell counting method, within default area called “Boundary box” with fixed resolution (200 μm × 300 μm) and an area of 0.084 mm2, located in the center of the image.
This technique was used to quantify the surface and basal epithelial cells, endothelial cells, and keratocytes. The superficial epithelial cells (50 μm) were identified as polygonal cells with clearly visible edges, bright cytoplasm, and dark nuclei.
The basal epithelial cells were identified as a compact layer, where the cells are smaller, with bright edges, uniform shape, and non-homogeneous cytoplasm. The keratocyte density was measured in the anterior stroma (from 0 to 100 μm posterior with respect to basal epithelium), in the intermediate stroma (between anterior and posterior stroma), and in the posterior stroma (from 0 to 100 μm anterior with respect to endothelium). 9
The corneal endothelium (30 μm) was identified as hexagonal cells, arranged regularly, with dark borders and with the reflective bright cytoplasm. The structural characteristics and the density in the various layers of the cornea were evaluated and compared, between eyes affected by PEX and eyes of the control group. All measures were presented as mean of three images, and results were expressed in cells per mm2.
Sub-basal nerve plexus study
Images of the sub-epithelial plexus containing the greatest number of nerve fibers were chosen. Our assessment based on four parameters:
Beadings density is defined as the number of hyper-reflective dots in 100 of a nerve fiber.
Tortuosity is defined as a less regular and straight trend of the nerve fibers: five degrees were considered, from grade 0 (nearly straight) to grade 4 (extremely tortuous).
Nerve fibers number is defined as the sum of the logs of the main nerves and their branches in the same images.
Density of length of the nerve fibers in each image is calculated as the total length of the nerves (μm) divided by the image size (0.084 mm2).
These evaluations were carried out using software for nerve analyses, provided by the ConfoScan 4.0.
Anterior segment optical coherence tomography analyses
Pachymetry of the central cornea was performed using Visante OCT (Carl Zeiss Meditec AG, Germany), high-resolution cornea mode. Central corneal thickness (CCT) was measured by the software-embedded caliper on three different scans, and the mean value was then calculated and recorded.
Statistical analyses
Results were analyzed with the Excel statistical software (version 8.0 for Windows 7) and SAS software version 9.1.3 (SAS Inc., USA). All results were expressed as mean ± SD, according to the assumption of normal distribution. The Student’s t-test was performed to compare two groups. The correlation index r, for Spearman’s ranks, was used to determine correlation between corneal sensitivity and sub-basal nerve plexus density. A value of p < 0.05 was considered statistically significant.
Results
This study involves 40 eyes of 40 patients with diagnosis of unilateral senile cataract associated with PEX (15 women, 25 men; mean age of 76.5 ± 8.2 years; age range of 52–86 years) and 40 eyes of 40 control subjects with senile cataract without PEX (17 women, 23 men; mean age of 77.7 ± 8.7 years; age range of 59–85 years). The difference between the mean age of the two groups was not statistically significant (p = 0.425) (see Table 1).
Results of confocal microscopy analysis.
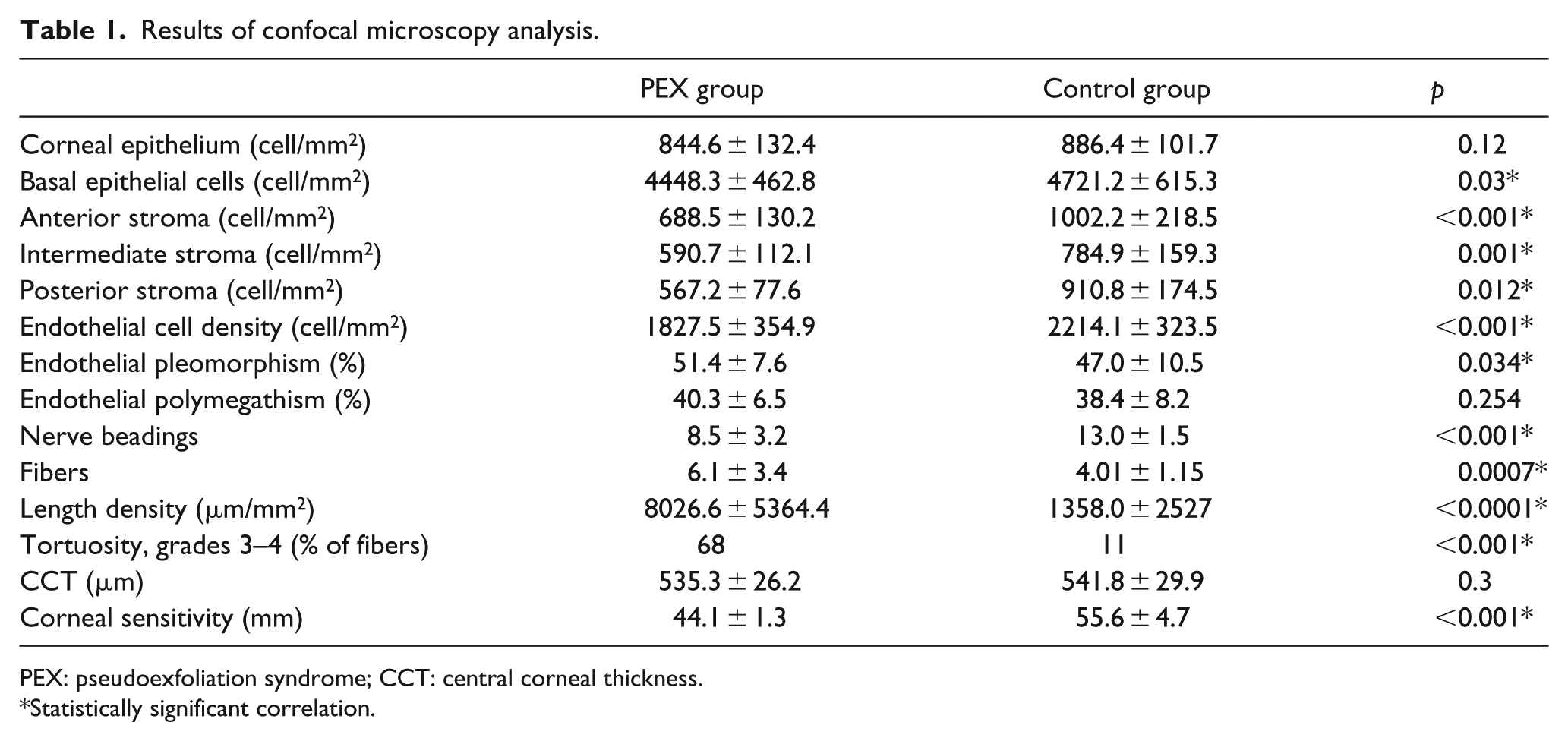
PEX: pseudoexfoliation syndrome; CCT: central corneal thickness.
Statistically significant correlation.
Corneal sensitivity
In PEX group, the mean corneal sensitivity was 44.1 ± 1.3 mm and in the control group was 55.6 ± 4.7 mm. The corneas of the eyes with PEX were significantly less sensitive than those of control group’s eyes (p < 0.001).
Cell densities
Corneal epithelium
In PEX group, the density of the superficial corneal epithelial cells was 844.6 ± 132.4 cells/mm2 and of the basal epithelial cells was 4448.3 ± 462.8 cells/mm2. The density of the corresponding layers of the control group was 886.4 ± 101.7 and 4721.2 ± 615.3 cells/mm2. The density of the basal epithelial cells was significantly lower in PEX eyes than control eyes (p = 0.03). However, there was no significant difference (p = 0.117) between the density of the superficial corneal epithelial cells of the two experimental groups.
Corneal stroma
The density of the cells in the anterior stroma was 688.5 ± 130.2 and 1002.2 ± 218.5 cell/mm2 in PEX and control groups, respectively. PEX group showed a significant decrease in the stromal cell density both in intermediate and posterior layers (590.7 ± 112.1 and 567.2 ± 77.6 cell/mm2) compared to control group (784.9 ± 159.3 and 910.3 ± 174.1 cell/mm2, respectively, Figure 1).
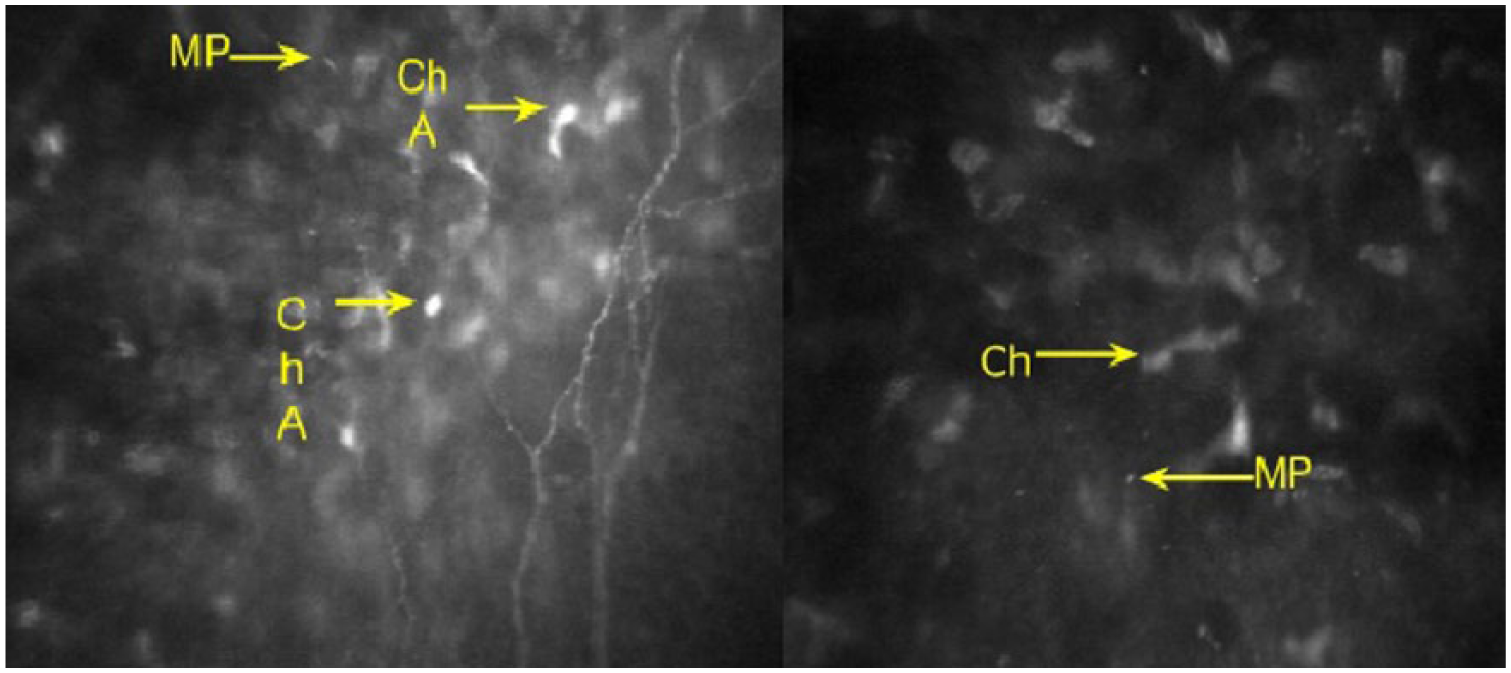
IVCM of corneal stroma in PEX patient shows activated cheratocytes (ChA) and PEX material (PM). Sub-basal plexus nerves show high degree of tortuosity and reduced number of branches.
Corneal endothelium
The density of the endothelial cells in PEX group was 1827.5 ± 354.9 and 2214.1 ± 323.5 cells/mm2 in the control group. The difference was significant (p < 0.001) between eyes with PEX and control groups.
There was a higher degree of pleomorphism in PEX group (51.4% ± 7.6%), in comparison with the control group’s eyes (47.0% ± 10.5%) (p = 0.034). The polymegathism was not significantly different—in patients with PEX was 40.3% ± 6.5% and in the control group was 38.4% ± 8.2% (p = 0.254, Figure 2).
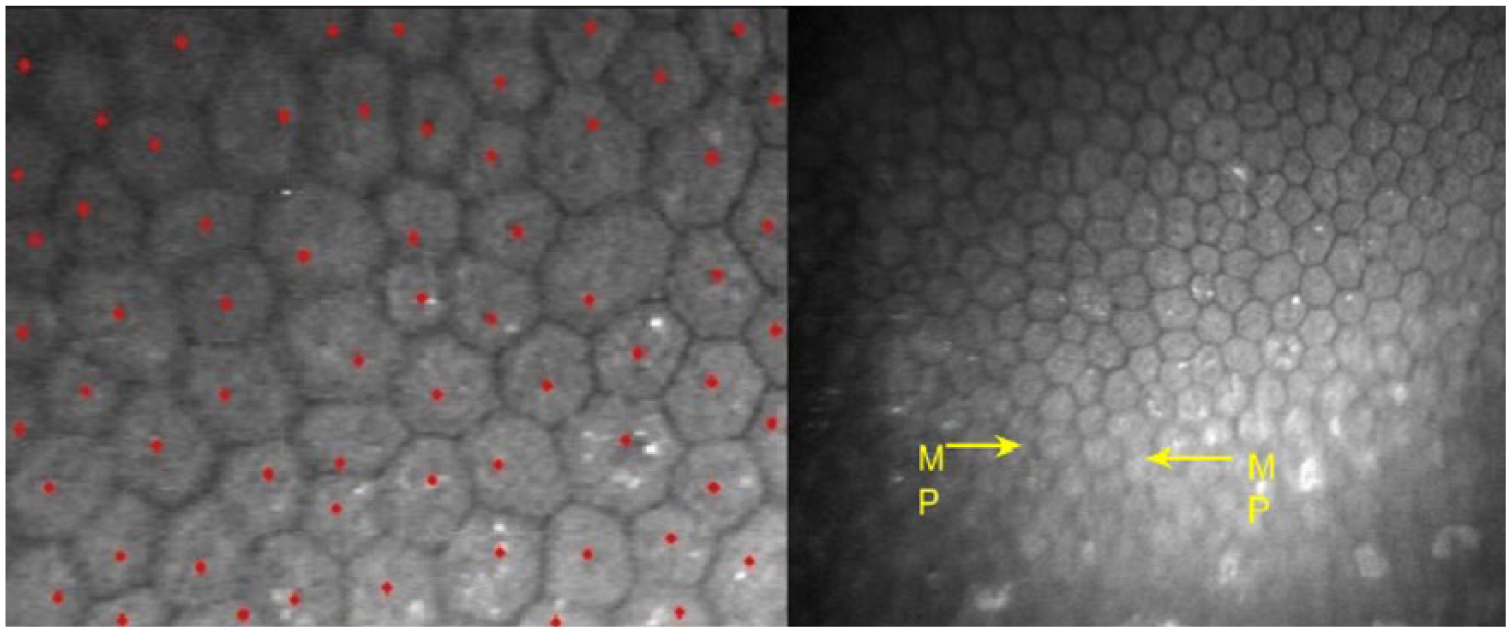
IVCM of corneal endothelium in PEX patient shows the presence of PEX material deposits. On the left, the technique of manual counting of endothelial cells.
Sub-basal nerve plexus: correlation between corneal sensitivity and density of nerves in the sub-basal nerve plexus
The study showed that patients with PEX had a lower density and a reduced number of fibers, lower number of “nerve beadings,” and higher degree of tortuosity of nerve fibers in the sub-basal plexus compared to the control group (Figure 1).
The analysis of Spearman’s correlation showed that there was significant positive correlation between CCMS and the density of long nerve fibers in sub-basal nerve plexus (r = 0.624; p < 0.001). The correlations between CCMS and the other sub-basal nerve plexus parameters were not statistically significant (p > 0.05).
Corneal thickness
The CCT measured with Visante OCT was 535.3 ± 26.2 μm in the PEX group and 541.8 ± 29.9 μm in the control group; the difference was not statistically significant (p = 0.3).
Confocal microscopy ultra-structural analysis
The IVCM demonstrated the presence of hyper-reflective material, probably pseudoexfoliation material (PEM), in all layers including the anterior stroma of the cornea. This alteration was not detected in control group. In 80% of patients with PEX-activated keratocytes and inflammatory cells (dendritic cells) were detected in the anterior stroma. Moreover, in 30% of patients with PEX, stromal nerve plexus was thickened with the presence of adjacent inflammatory cells.
Discussion
The purpose of our study was to observe, through the confocal microscopy (IVCM), the pathological changes of each corneal layer in eyes affected by PEX, trying to correlate such obtained data with the current knowledge about the disease.
Our results demonstrate a lower cell density in the corneal epithelial basal layer, as reported by previous studies,10,11 and statistically significant decrease in the density of corneal stromal cells, both in the anterior portion and in the deeper layers; we also detected the presence of hyper-reflective aggregates (PEM) both in the stroma and in the endothelial layer. As suggested in previous studies, 10 the lower density of stromal keratocytes may be related to increased apoptosis due to deposition of these exfoliative clumps. In this context, the deposition of hyper-reflective material (PEM) both in stromal and endothelial layers could represent, with poorly known mechanisms, an important direct causative factor for corneal damage; moreover, it might induce a state of sub-clinical inflammation by the release of soluble factors such as cytokines and chemokines. This hypothesis is further supported by our IVCM findings of inflammatory dendritic cells and activated keratocytes in the anterior corneal stroma of PEX eyes.
Corneal endotheliopathy in PEX eyes has been shown in several previous studies.5,8,10 According to the literature, we found a considerable decrease in the endothelial cell density and an increased cell pleomorphism, although there was not a statistically significant increase in the polymegathism compared to control group. It was supposed 11 that endotheliopathy in PEX could be linked to deposition of exfoliative material on the endothelium, leading to sub-clinical inflammation via increased transforming growth factor beta (TGF-β) release and clusterin deficiency.12,13
Corneal endotheliopathy could also lead to changes in CCT, as supposed by several authors in the literature. 14 In agreement with current knowledge,15,16 the conflicting results about the changes of CCT in eyes affected by PEX could be interpreted either as the consequence of reduced corneal cell density and morphological changes due to hypesthesia or as the expression of corneal swelling due to endothelial dysfunction. In our study, however, we did not find any significant changes in CCT between the two study groups, so the relationship between presence of PEM and stromal/endothelium alterations is not yet currently clear.
Particular attention is paid to corneal sensitivity, which is significantly lower in the PEX group than control. Although this alteration had already been demonstrated in previous studies and correlated with the changes in the tear film,17,18 our study demonstrates that CCMS measured by Cochet-Bonnet nylon thread esthesiometer is statistically correlated to the anatomical alterations suffered by the corneal nerve plexus. With the use of the IVCM, we have demonstrated, in accordance with what is reported in recent studies,10,11 that there is a major alteration of the sub-basal corneal nerve plexus structure in terms of length, density, tortuosity, and number of nerve branches in PEX eyes. It is our opinion, supported by statistical data, that these nerve alterations may represent the anatomical-structural base underlying corneal hypesthesia, in addition to alterations in the tear film and the ocular surface already described in the literature. Whether sub-basal nerve plexus alterations are primary changes or due to other underlying mechanisms must still be determined.
As supposed in the literature, 10 pseudoexfoliative material found in basal epithelial layer and stroma could suggest that several extracellular materials, such as basement membrane components, may contribute to PEM formation, in addition to elastic microfibrils already studied. 19 Presence of dendritic cells in stroma and near the sub-basal nerve plexus fibers suggests that there is an inflammatory mechanism underlying the plexus degeneration and neuropathy.
Although previous study showed lower CCMS in fellow eye of PEX group and hypothesized that it could possibly reflect the systemic nature of the disease, and Zheng et al. 10 found these nerve alterations in contralateral PEX eyes too, as different degrees of a bilateral disease expression, further studies are needed in order to assess if this alteration can be predictive of subsequent clinical development of the disease and to define the exact mechanisms underlying this pathology.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.