
Abstract
Purpose:
To evaluate the efficacy and safety of bimanual, low-energy femtosecond laser-assisted cataract surgery with 1.4-mm microincisions compared to standard bimanual phacoemulsification (bimanual microincision cataract surgery).
Design:
Prospective, non-randomized comparative case series.
Methods:
Bimanual femtosecond laser-assisted cataract surgery with microincisions was performed on 80 eyes (Group A) with the low-energy Ziemer LDV Z8; a matched case–control series of 80 eyes performed with standard bimanual microincision cataract surgery technique was selected for comparison (Group B). All interventions were performed by the same experienced surgeon. Intraoperative parameters were recorded as well as intra- and postoperative complications. Best corrected visual acuity, surgically induced astigmatism, central corneal thickness and endothelial cell count were evaluated before surgery and at 1 and 3 months post intervention.
Results:
The mean effective phaco times were 3.79 ± 2.19 s (Group A) and 4.49 ± 1.84 s (Group B) (p = 0.041). No major intra- or postoperative complications occurred. An overall significant mean best corrected visual acuity improvement was noted at 3 months, but was not statistically different between the groups. No significant changes were observed for surgically induced astigmatism or corneal pachymetry. A significant loss of endothelial cell count in both groups was detected at 3 months, with Group A reporting a significantly lower endothelial cell count loss compared to Group B (p = 0.009).
Conclusion:
Bimanual, low-energy femtosecond laser-assisted cataract surgery with 1.4-mm microincisions by an expert surgeon was proven to be safe and effective in this study. This technique has advantages compared with standard bimanual microincision cataract surgery in terms of endothelial preservation.
Keywords
Introduction
The femtosecond laser was introduced in ophthalmology more than 7 years ago to assist in precision cataract surgery. 1 Although femtosecond laser-assisted cataract surgery (FLACS) does not seem to show any significant difference with respect to refractive and visual outcomes as compared to standard phacoemulsification, this new technique offers advantages in terms of reproducibility and precision by helping the surgeon for the creation of microincisions, capsulotomies and nucleus fragmentation.2–4
Bimanual microincision cataract surgery (B-MICS) is a minimally invasive variant of coaxial phacoemulsification which enables microincisions of 1.4 mm. 5 This technique is characterized by increased stability of the anterior chamber with the separation of the aspiration and the infusion probe. Moreover, the small instruments give greater visibility of the surgical field.5–8 Because of the requirement of precision and small openings, the use a femtosecond laser is well suited for minimally invasive bimanual surgery.
The femtosecond laser LDV Z8 (Ziemer Ophthalmic Systems AG, Port, Switzerland) is a mobile femtosecond laser system used in cataract surgery and characterized by high frequency and low energy. 9 Through the use of a non-applantating liquid patient interface, the structural anatomy of the cornea during the procedure remains intact and free of posterior corneal folds. 10 The Z8 also employs the use of an integrated high-definition ocular coherence tomography (OCT) which allows a clear visualization of the structures inside the anterior segment. 11 Furthermore, its complete mobility and small dimensions allow surgeons to carry out the whole surgical operation in the same operating room without the need to complete the surgery in another adjacent operating room. 12
Recent studies have underlined a faster visual recovery and reduced phacoemulsification time in FLACS technique compared to standard technique12–14 and bimanual FLACS has been proven to be surgically and statistically more efficient than coaxial FLACS.15,16 We recently investigated the learning curve for bimanual FLACS with intraocular lens (IOL) implantation through a 1.4-mm incision and we found that this technique, although it simplifies certain critical steps of cataract surgery, requires a learning curve. 17
The purpose of this study was to evaluate the safety and efficacy of bimanual FLACS with a low-energy femtosecond laser in terms of intraoperative parameters and 3-month follow-up outcomes compared to the standard B-MICS technique. Postoperative outcomes included visual acuity, astigmatism, corneal thickness and endothelial cell count (ECC).
Methods
This prospective study was performed in a single centre at the Institute of Ophthalmology, University of Modena and Reggio Emilia, Italy. The study protocol was approved by the local ethics committee (prot no. 202/15) and was conducted in compliance with the Declaration of Helsinki. All patients gave written informed consent.
Consecutive patients with nuclear sclerosis grade 2 (NS2) and 3 (NS3) in the Lens Opacities Classification System III (LOCS III), 18 and in line for cataract surgery on the day in which the femtosecond laser was available, were treated with the FLACS technique by the same experienced surgeon and enrolled into this study, between November 2016 and May 2017 (Group A). The experienced surgeon had performed a total of 100 FLACS procedures before including patients for this study and his learning curve was surpassed. A control series was selected based on nuclear sclerosis grade, treated by the same surgeon with B-MICS between April 2015 and October 2015, and used for comparison (Group B). Exclusion criteria included eyes with previous surgery, complicated cataracts (e.g. hard cataracts, traumatic cataract, pseudoexfoliation syndrome), insufficient mydriasis (<4 mm), concomitant eye pathologies (uveitis, glaucoma, corneal opacities, diabetic retinopathy), low ECC (<1500 cells/mm2) and monocular patients.
A detailed clinical history was collected for all patients and a full preoperative ophthalmic evaluation, including anterior segment biomicroscopy, fundus examinations, axial length and biometry, best corrected visual acuity (BCVA), corneal astigmatism, central corneal thickness (CCT) and ECC, was carried out. Biomicroscopy and fundus examinations were performed at slit lamp, axial length and biometry were performed with IOL Master (Carl Zeiss Meditec, Jena, Germany), BCVA was measured with Snellen visual acuity charts with the logMAR methodology, corneal astigmatism was obtained with a CT-1000 topographer (Shin Nippon, Tokyo, Japan), CCT with corneal pachymetry IOPac (Heidelberg Engineering, Heidelberg, Germany) and ECC was measured using corneal microscopy Noncon Robo-CA (Konan Medical Inc., Hyogo, Japan). All surgeries in both groups were performed using the same phaco machine (Faros; Oertli Instruments AG, Berneck, Switzerland).
Intraoperative parameters were recorded and included the total surgery time, effective phacoemulsification time (EPT) and balanced salt solution (BSS) usage. The total surgical time for Group A was calculated from the interface application to hydrosuture, subtracting the time between the end of the liquid interface removal to the opening of the first corneal incision; for Group B, it was calculated from the first corneal incision to hydrosuture. EPT data were registered from the phacoemulsification machine at the end of each intervention; BSS usage was calculated by subtracting the residual volume at the end of surgery from the initial volume in the infusion bottle.
Potential intraoperative complications included suction break, conjunctival redness or haemorrhage, capsule tags and bridges, anterior capsule tear, miosis, endothelial damage, capsule blockage and posterior capsule tear. Postoperative complications (within 3 months of follow-up) were considered corneal oedema, inflammatory complications (uveitis), IOL dislocation, rise of IOP and cystoid macular oedema. 19
Surgical technique
Preoperatively, all patients were prescribed non-steroidal anti-inflammatory drug (NSAID) eye drops three times a day for 3 days prior to surgery. Prophylactic strategies to prevent infection in all patients included the application of topical antibiotic eye drops and 5% povidone iodine drops to the conjunctival cul-de-sac and 10% povidone iodine on the periocular skin in the surgical suite prior to surgery, and intracameral antibiotic was applied along with topical antibiotics in the conjunctival cul-de-sac at the end of surgery.
Intraoperatively, consistent mydriasis was achieved with the instillation of 10% phenylephrine and 1% cyclopentolate in all patients; peribulbar block was performed to obtain local anaesthesia (1.5 mL of lidocaine 2% and 1.5 mL of bupivacaine 0.5%).
FLACS technique
A disposable suction ring was carefully applied to the eye and centred over the limbus; a liquid interface was created by filling the suction ring with a BSS and then the mobile arm of the laser system was placed over the corneal apex. Integrated optical coherence tomography (OCT) illustrated the ocular structures. Treatment parameters were determined in a customized manner using the laser platform Wizard setting: for capsulotomy 90% laser power, 0.6 mm resection height, 5.2 mm diameter; for lens fragmentation 95%–100% laser power, 16 segments; and for controlled cortical impacts and for clear corneal incisions (CCIs) 120%–130% laser power, 1.4 mm width.
First, laser treatment fragmented the lens in a 16-piece pie-cut pattern. We then performed an anterior 5.2-mm-diameter capsulotomy and created the two 1.4-mm corneal microincisions at the 10 o’clock and 2 o’clock positions. After the removal of the suction ring, the CCIs were checked by the surgeon using a smooth spatula and gentle movements along the incision in order to completely open the incision from the external cornea to the internal cornea.
Amvisc (Bausch & Lomb, Rochester, NY, USA) ocular viscoelastic device (OVD) was used to fill the anterior chamber so that the anterior capsule could be removed. Hydrodissection and hydrodelineation were carried out using a 26-gauge cannula with an injection of BSS under the anterior capsule edge paying attention to the presence of any air bubbles that could cause posterior capsular block with posterior capsule tear.
The bimanual phacoemulsification technique was used to aspirate the nucleus using a 20-gauge, 30-degree-angled, sleeveless probe and a 19-gauge irrigating chopper (Oertli Instruments AG). Then bimanual irrigation/aspiration of the residual cortex was performed using two 21-gauge probes (21-gauge smooth irrigation handpiece, 21-gauge rough aspiration handpiece; Bausch & Lomb, Rochester, NY, USA) and then posterior capsule polishing. BunnyLens AF IOL (Hanita Lenses, Hanita, Israel) was implanted in the capsular bag through a 1.4-mm microincision using the wound-assisted technique with the VISCOJECT™-BIO 1.5-mm injector. At the end of surgery, the OVD was removed and the incisions were hydro-sutured. In Figure 1, the main steps of the technique are shown.
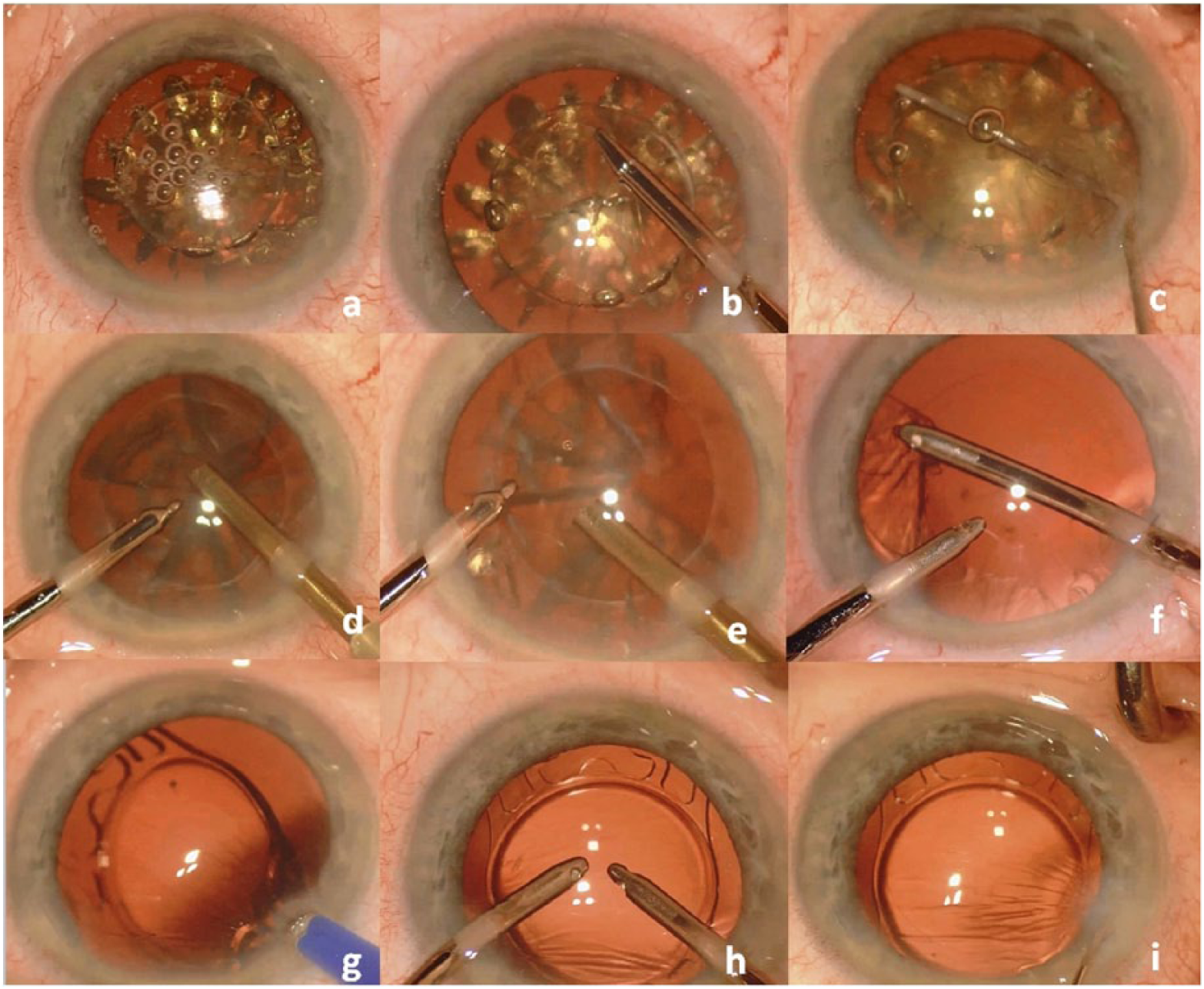
Bimanual FLACS – surgical technique: (a) creation of 1.4-mm microincisions, capsulotomies and nucleus fragmentation with femtosecond laser LDV Z8; (b), (c) removal of capsulotomy button with microforceps; (d), (e) microphacoemulsification; (f) bimanual irrigation/aspiration; (g) intraocular lens implantation without CCI enlargement; (h) removal of OVD and (i) hydrosuture of the microincisions.
Standard technique
The surgeon performed two 1.4-mm biplanar trapezoidal incisions at the 10 o’clock and 2 o’clock positions with a precalibrated knife. Amvisc (Bausch & Lomb) OVD was used to fill the anterior chamber and a manual 5-mm continuous curvilinear capsulorhexis (CCC) with a cystotome and microforceps (E. Janach, Como, Italy) was performed. Hydrodissection was performed with a 26-gauge cannula; the bimanual phacoemulsification technique was used to aspirate the nucleus with a 20-gauge, 30-degree-angled, sleeveless probe and a 19-gauge irrigating chopper. Stop-and-chop technique was performed to obtain phaco-fracture. Irrigation/aspiration was performed with two 21-gauge probes with an oval-shaped section. BunnyLens AF IOL (Hanita Lenses) was implanted through a 1.4-mm microincision without the enlargement of the main incision and using the wound-assisted technique with the VISCOJECT-BIO 1.5-mm injector. At the end of the surgery, the OVD was removed and the incisions were hydrated.
Follow-up
All patients were prescribed tobramycin/dexamethasone eye drops four times a day for 15 days, followed by flurbiprofen eye drops three times a day for a further 15 days. Postoperative results were evaluated at 30 days and 3 months after surgery and included BCVA, corneal pachymetry, corneal astigmatism and endothelial microscopic examinations using the instruments described previously.
Statistical analysis
An Excel database (Microsoft Excel 2010, Microsoft Office Professional Plus 2010) was used to record prospectively all data for Group A and the data for Group B were collected retrospectively. Data analysis was performed using the Stata 13.1 software (StataCorp LP, College Station, TX, USA) with Student’s t-test and Wilcoxon rank-sum test. A p-value < 0.05 was considered statistically significant.
Results
Patients included in Group A and Group B were similar for all characteristics outlined in Table 1, including patient age, gender and LOCS value. BunnyLens AF IOLs were successfully implanted in all eyes in the capsular bag.
Comparison of demographic data at baseline for both groups.
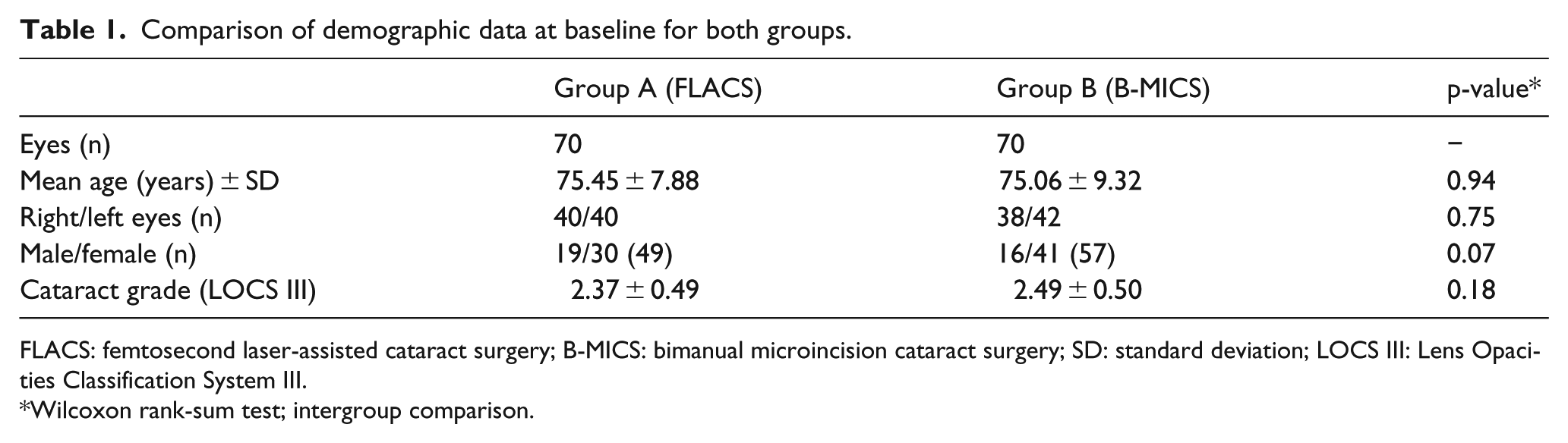
FLACS: femtosecond laser-assisted cataract surgery; B-MICS: bimanual microincision cataract surgery; SD: standard deviation; LOCS III: Lens Opacities Classification System III.
Wilcoxon rank-sum test; intergroup comparison.
Intraoperative parameters
Overall surgical time was longer for Group A compared to Group B (15.6 ± 3.4 vs 13.0 ± 2.7 min; p < 0.05). The mean EPT in Group A was shorter (3.8 ± 2.2 vs 4.5 ± 1.8 s; p = 0.041) and a reduced mean BSS was required (116.5 ± 9.0 vs 142.8 ± 26.8 mL; p < 0.05). All the results are outlined in Table 2.
Mean intraoperative parameters in the two groups.
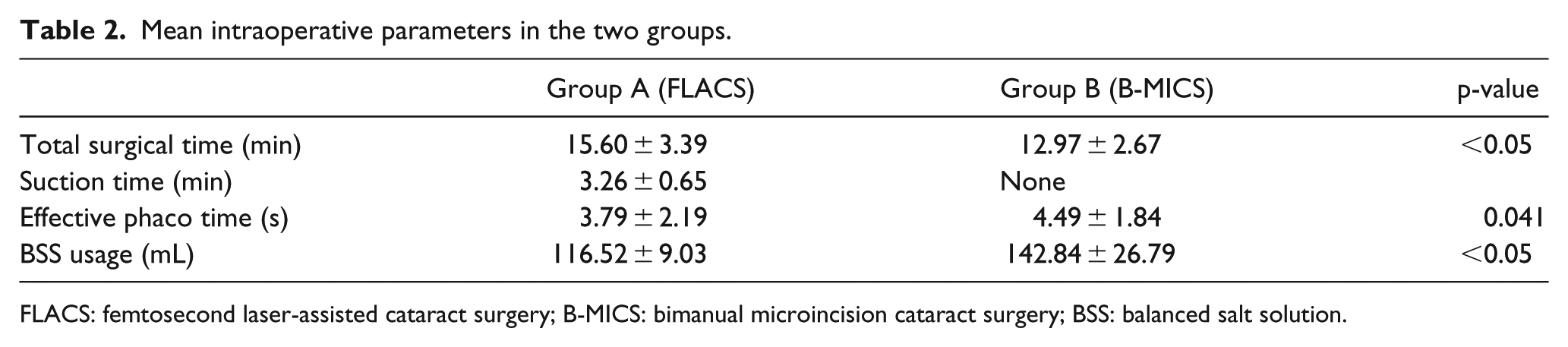
FLACS: femtosecond laser-assisted cataract surgery; B-MICS: bimanual microincision cataract surgery; BSS: balanced salt solution.
Intraoperative complications
No major intraoperative complications were observed in either group. We recorded two cases of incomplete CCIs in Group A only. Of particular interest here were no incomplete capsulotomies or capsule buttons observed or any cases of intraoperative miosis.
Postoperative results
In both groups, a mean BCVA improvement was observed; Group A reported a mean BCVA improvement of 0.433 ± 0.321, which was a statistically significant improvement compared to the baseline values (p < 0.05) and the mean BCVA improvement in Group B was 0.420 ± 0.142, which was also a statistically significant improvement compared to the baseline values (p < 0.05). However, the difference in the improvement of BCVA between the two groups did not reach statistical significance.
No differences were observed concerning astigmatism and corneal pachymetry between the baseline and postoperative values for both groups, or in the comparison between the groups. Also the astigmatism axis remained stable over time with a modification of 5.72 ± 24.73 degrees in the FLACS group and 7.88 ± 27.57 degrees in the B-MICS group with no statistically significant difference between the two groups (p = 0.18).
The mean ECC loss of 194.35 ± 263.62 cells/mm2 in Group A (9.3%) and 334.75 ± 361.81 cells/mm2 in Group B (14.1%) was observed following surgery. This difference in reduction was statistically significant when the two groups were compared in favour of Group A (p = 0.009). All postoperative values are reported in Table 3.
Mean values of preoperative and postoperative parameters for Group A and Group B (BCVA is expressed in logMAR).
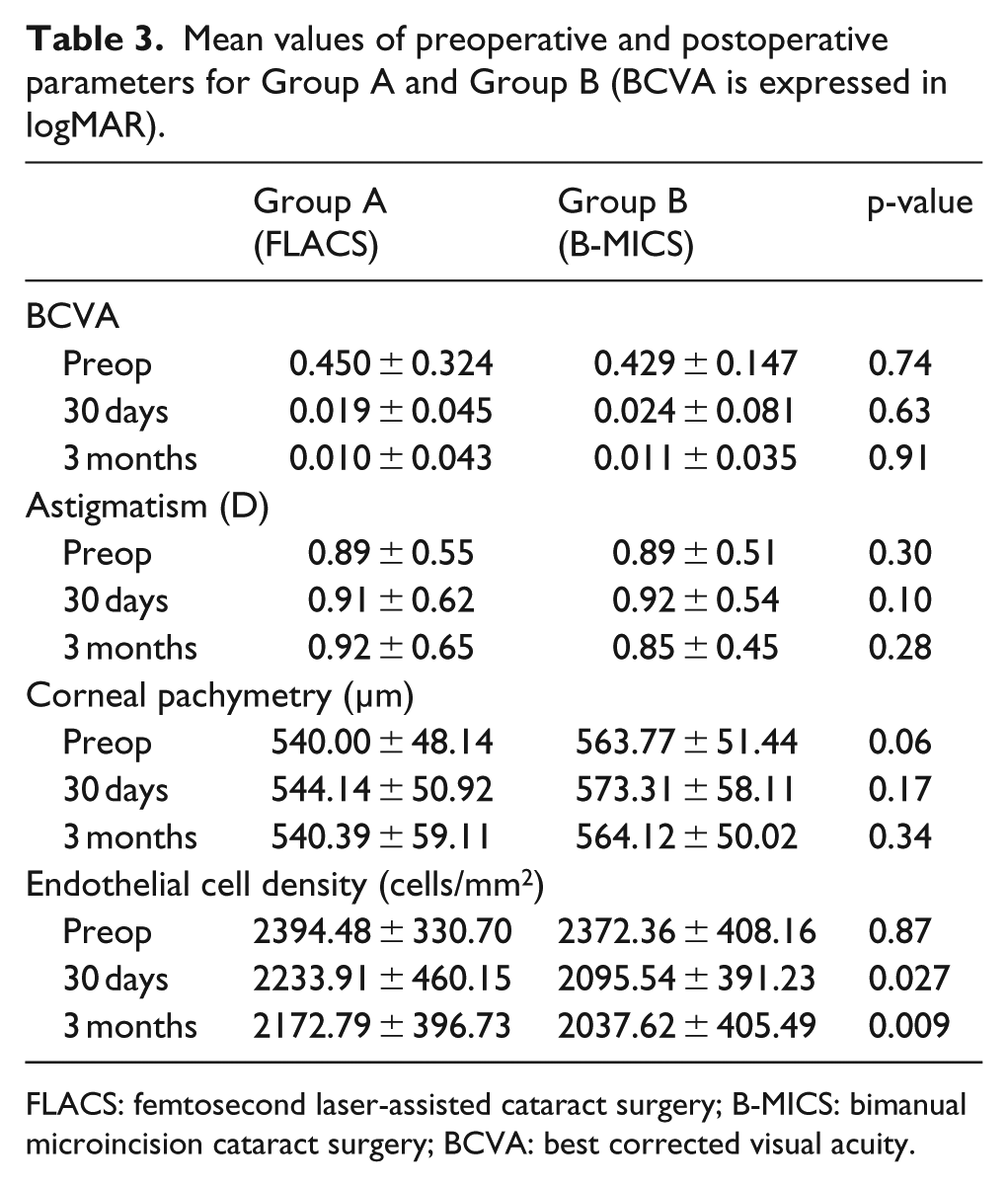
FLACS: femtosecond laser-assisted cataract surgery; B-MICS: bimanual microincision cataract surgery; BCVA: best corrected visual acuity.
There were no postoperative complications reported among all participants.
Discussion
The use of FLACS during cataract surgery offers many potential advantages over a B-MICS procedure and includes the execution of precisely centred corneal microincisions, perfectly circular anterior capsulotomies and effective lens fragmentation with reduced ultrasound power. Although the theoretical advantages of FLACS seem to facilitate and standardize some crucial surgical steps of cataract surgery, its effectiveness is still debated. Recently, three large meta-analyses were published suggesting that there are no statistically significant differences between FLACS and standard manual cataract surgery in terms of visual and refractive outcomes and general complications.1–3 Moreover, recent literature reporting on high-energy lasers shows that FLACS is associated with higher prostaglandin concentrations and higher rates of anterior capsule tears. 20
The current findings describe the results of FLACS performed by an experienced surgeon using the bimanual technique with IOL implantation through a 1.4-mm incision compared to B-MICS standard technique, in terms of intraoperative and postoperative complications, as well as the visual outcomes, over a 3-month follow-up period.
Recently, Aliò et al.15,16 reported on bimanual versus coaxial MICS techniques with IOL implantation through enlarged 2.2-mm incisions, both assisted by the femtosecond laser. The authors showed that the bimanual technique offers excellent results in terms of safety and efficacy and that it is surgically and statistically more efficient than the coaxial intervention. Femtosecond laser incisions in both techniques were proven to be safe and well positioned and did not induce high-order aberrations.
EPT was significantly reduced in the FLACS group compared to the B-MICS group in this study. This is in line with the recent literature which showed that FLACS is accompanied by a significantly decreased EPT21,22 in comparison to conventional phacoemulsification and that mean EPT is better in bimanual FLACS than in coaxial FLACS. 15 In addition, low-pulse laser energy has been shown to minimize cell loss and reduce peripheral damage, along with capsulotomy.23,24 The strength of the capsulotomies also depends on the laser pulse energy and increases with decreasing energy. 25
A significantly higher total surgical time in the FLACS group was registered compared to B-MICS. The longer total surgical time is mostly due to the docking/suction with the femtosecond laser, which represents a new phase in cataract surgery. Further analysis was performed to obtain surgical time without the docking/suction time to measure the effective time of surgery inside the eye. This parameter was found to be marginally lower in the FLACS group than in the standard B-MICS procedure (12.43 s in FLACS vs 12.98 s in standard B-MICS): the laser treatment facilitates the surgical manoeuvres, thus reducing the presence of instrumental manoeuvers inside the eye.
However, the Z8 femtosecond laser system, due to its reduced dimensions, enables all surgical steps to be performed in the same theatre saving time and reducing infective risk for the patient if compared to other femtosecond laser systems. 26
We also found a statistically significantly reduced BSS usage in the FLACS group. This finding indicates that the microincisions made with the femtosecond laser result in a better fit with the surgical instruments, with a reduced BSS loss during surgery. Moreover, this finding can have a cost-effective benefit for surgery.
Recently, Pajic et al. 11 described a low complication incidence using the LDV Z8 but they did not compare results with a control group. Chen et al. 26 found a statistically significant decrease in intraoperative complication (1.8%) when compared to traditional phacoemulsification technique (5.8%), suggesting that it can be safely incorporated into routine practice. Nagy et al. 27 showed that the majority of complications in FLACS occur principally during the first 100 cases. However, they did not find any cases of capsule blockage, posterior capsule tear or any complication that would require vitrectomy. Finally, Aliò et al. 16 found some cases of incomplete capsulorhexis (4%), anterior capsule rupture without posterior capsule tear (4%) and posterior capsule rupture (4%).
In our case series, the bimanual FLACS intervention was found to be safe with an optimal ease of fragmentation when performed by an experienced surgeon compared to the standard B-MICS technique, as has been reported in other studies.1–3 We did not observe any major complications, such as capsule tears or dropped nuclei.
In our study, we recorded two cases of incomplete creation of CCI. We did not find any other complications in the two groups. In particular, we did not record any intraoperative miosis: the low-energy laser system is designed to induce less inflammation with lower level of prostaglandins, lower suction and a lower rise of anterior chamber temperature.9,11
Of note, in our cohort the liquid interface did not induce any marked corneal fold and produced precise and complete capsulotomies. We did not observe incomplete capsulotomy and capsule buttons were always free-floating. Recent studies have proved that FLACS capsulotomies are more predictable, regular and well centred than the manual ones, leading to safer surgery. 28 Sometimes, during lens fragmentation, the surgeon noted the formation of some microbubbles created by photodisruption of tissue; for this reason, the surgeon performed a more accurate and slow hydrodissection that could have contributed to the higher mean surgical time in the FLACS group.
Regarding postoperative results, we ascertained a significant improvement in mean BCVA in both groups. There was no significant difference in surgically induced astigmatism (SIA) and astigmatism axis or CCT between the pre- and postoperative values for both groups, as has been found previously.29–31 Moreover, our findings regarding ECC demonstrate the endothelial sparring effect of the femtosecond laser, likely due to the reduction in overall phaco energy which has been shown to harm the endothelium. The positive impact of FLACS on the endothelium has been widely reported in the literature and appears to be consistently present regardless of what device is used.30,31 Endothelial cell loss is a critical clinical concern in patients whose endothelium is already compromised due to corneal diseases or trauma. In these patients, FLACS may provide a clinical benefit. No postoperative complications in either group were recorded, including IOL decentrations during the 3-month follow-up.
This study has inherent limitations associated with the comparison of a retrospectively evaluated control group. Furthermore, this study included selected patients with uncomplicated cataracts and did not include patients with corneal endothelial diseases or weak zonules. The included patients were treated by a single, expert surgeon and hence the results should be interpreted accordingly.
In conclusion, the results of this comparative study of uncomplicated cataracts treated by an expert surgeon suggest that bimanual FLACS with a low-energy femtosecond laser is safe and effective when compared to the standard B-MICS technique in terms of complications and visual acuity, astigmatism, pachymetry and endothelial cell loss. Furthermore, in this small cohort study, FLACS was associated with significantly reduced EPT and endothelial cell loss. Further research should be needed in the future to compare FLACS to standard B-MICS in complicated cataract scenarios as Fuchs endothelial dystrophy or traumatic cataracts where minimally invasive interventions with reduced overall energy and less mechanical manipulation of the capsule could be most beneficial.
Footnotes
Acknowledgements
This work was presented in part at the XXXV Congress of the European Society of Cataract and Refractive Surgery (ESCRS), 7–11 October 2017, in Lisbon (Portugal). The authors would like to thank Johanna Chester for her critical revision of the content and editorial assistance.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.