
Abstract
Purpose:
To introduce a new surgical technique for the localization of corneal bulla to drain a massive corneal hydrops.
Methods:
Four consecutive cases with acute large protruded hydrops were selected. A limbal paracentesis was made via 15° blade. Afterward, trypan blue with a concentration of 0.1% was injected into the anterior chamber. Upon pooling trypan blue in the bulla, the surgeon immediately marked the primary site of stromal staining before further spreading of the dye. Anterior chamber irrigation was then carried out using balanced salt solution, and the excess of trypan blue was washed out. Subsequently, the surgeon made a beveled venting incision to decompress bulla via 15° blade resulting in a stream of dye egressed from the venting incision. At the end of the surgery, 20% diluted SF6 was injected into the anterior chamber.
Results:
Postoperatively, Descemet’s membrane was attached up to the second postoperative day. The corneal edema was resolved up to 3 weeks. Contact lens–corrected visual acuity was improved in all cases.
Conclusion:
Venting incision under the guide of injected trypan blue into the anterior chamber combined with intracameral SF6 injection could be effectively used for a large acute hydrops. This technique could prevent other interventions like passing full-thickness corneal suturing and subsequent complications.
Introduction
Acute hydrops is a complication of advanced keratoconus. It is characterized by a sudden significant decrease in visual acuity due to severe localized corneal edema. Previous investigations showed that limited rupture of Descemet’s membrane (DM) is the underlying mechanism expediting entrance of aqueous humor into the stroma that leads to the formation of bulla. 1
Prompt management of hydrops could be crucial in restituting vision and preventing extensive scar formation and neovascularization that could endanger the prognosis of later optical keratoplasty. Furthermore, irregularity of ocular surface and the epithelial defect caused by the confined area of corneal edema renders the patient susceptible to infectious keratitis. Also, ocular discomfort during blinking is another encountered problem that could mandate early treatment.2,3
However, there is difficulty regarding resolving and healing of a large hydrops, which may necessitate drainage of the trapped aqueous humor for rapid recovery. Vajpayee et al. 1 proposed the drainage using anterior segment optical coherence tomography (AS-OCT) pictures as a guide to reach more rapid recovery. In the present study, we aimed to introduce a new surgical technique for localization of corneal bulla, for targeted venting incision of a corneal hydrops to facilitate rapid recovery.
Methods
The study was performed in adherence to the tenets of the Declaration of Helsinki, and local ethics committee approved the methodology. Informed consent was obtained from all patients or legal guardians prior to enrolling them in the study.
Four consecutive cases of acute large hydrops were selected. Under topical or general anesthesia and sterile condition, a limbal paracentesis was made via 15° blade at a site according to surgeon’s preference. Afterward, trypan blue (TB) with a concentration of 0.1% was injected into the anterior chamber. Upon pooling TB in the bulla, the surgeon immediately marked the primary site of stromal staining before further spreading of the dye. Anterior chamber irrigation was then carried out using balanced salt solution, and the surplus of TB was flushed out. Subsequently, the surgeon made a beveled venting incision to decompress the bulla via 15° blade resulting in a stream of dye egressed from the venting incision. For re-attachment of DM, we used an intracameral injection of 20% diluted SF6 filling up to 50% of anterior chamber in a phakic eye (Supplemental Video 1) (Figure 1(a)–(c)). Finally, paracentesis site was sealed using 10-0 nylon suture to retain the intraocular gas. Upon discharge, patients were instructed to maintain a supine position. Postoperatively acetazolamide 250 mg, topical levofloxacin 0.5% eye drop, topical fluorometholone along with 5% NaCl ophthalmic solution every 6 h were given.
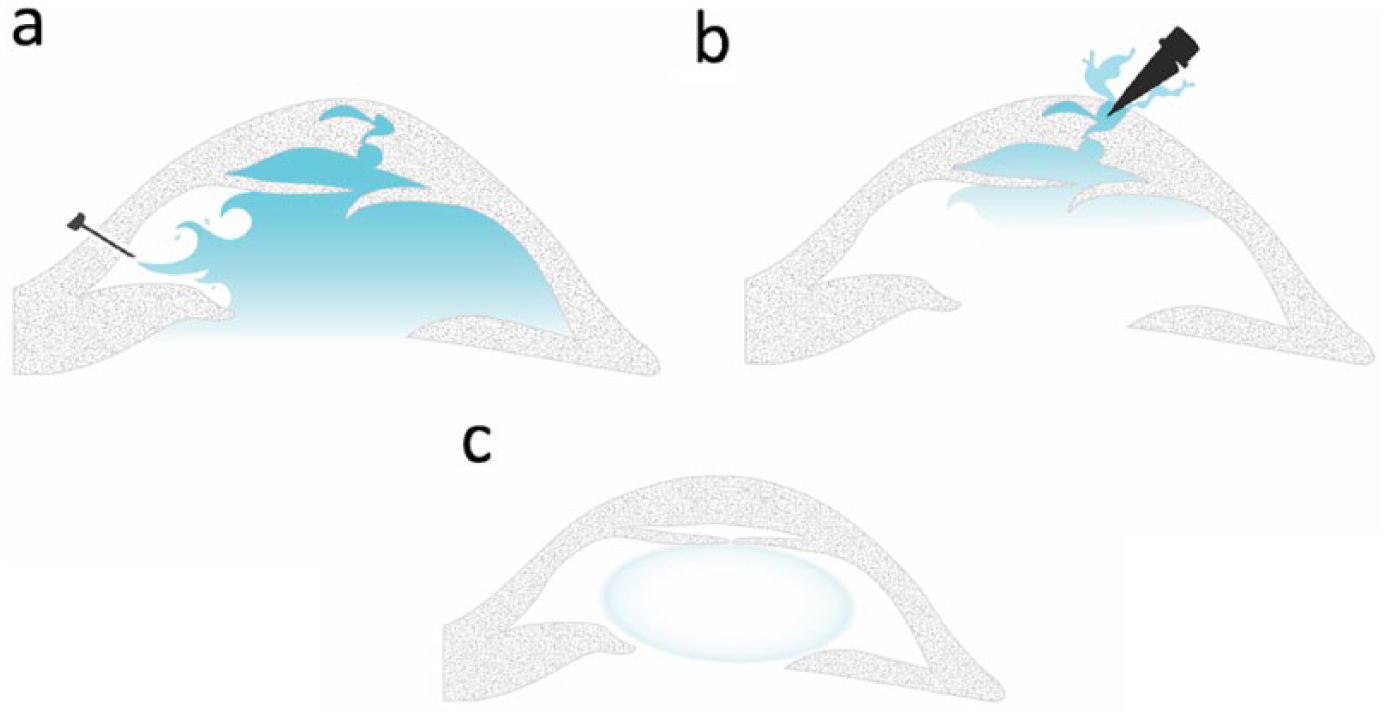
Trypan blue (TB) was injected into the anterior chamber (a). Upon pooling TB in the bulla, the surgeon immediately marked the primary site of stromal staining before further spreading of the dye. Subsequently, the surgeon made a beveled venting incision to decompress the bulla via 15° blade resulting in a stream of dye egressed from the venting incision (b). Finally, 20% diluted SF6 was injected into the eye (c).
Results
Four eyes with severe massive hydrops were included; preoperative visual acuity was hand motion in all eyes, because of large hydrops. All surgeries were done under topical anesthesia except one eye (a 12-year-old down patient). All procedures were done by the same experienced surgeon (M.S.). Postoperatively, DM was attached up to the second postoperative day captured by AS-OCT (CASIA2; TOMEY, Japan) (Figure 2(a) and (b)). This procedure resulted in the rapid decrease in corneal edema. The corneal edema was resolved up to 3 weeks (Figure 2(c) and (d)) (Table 1). Contact lens–corrected visual acuity (CCVA) was significantly improved in all cases.
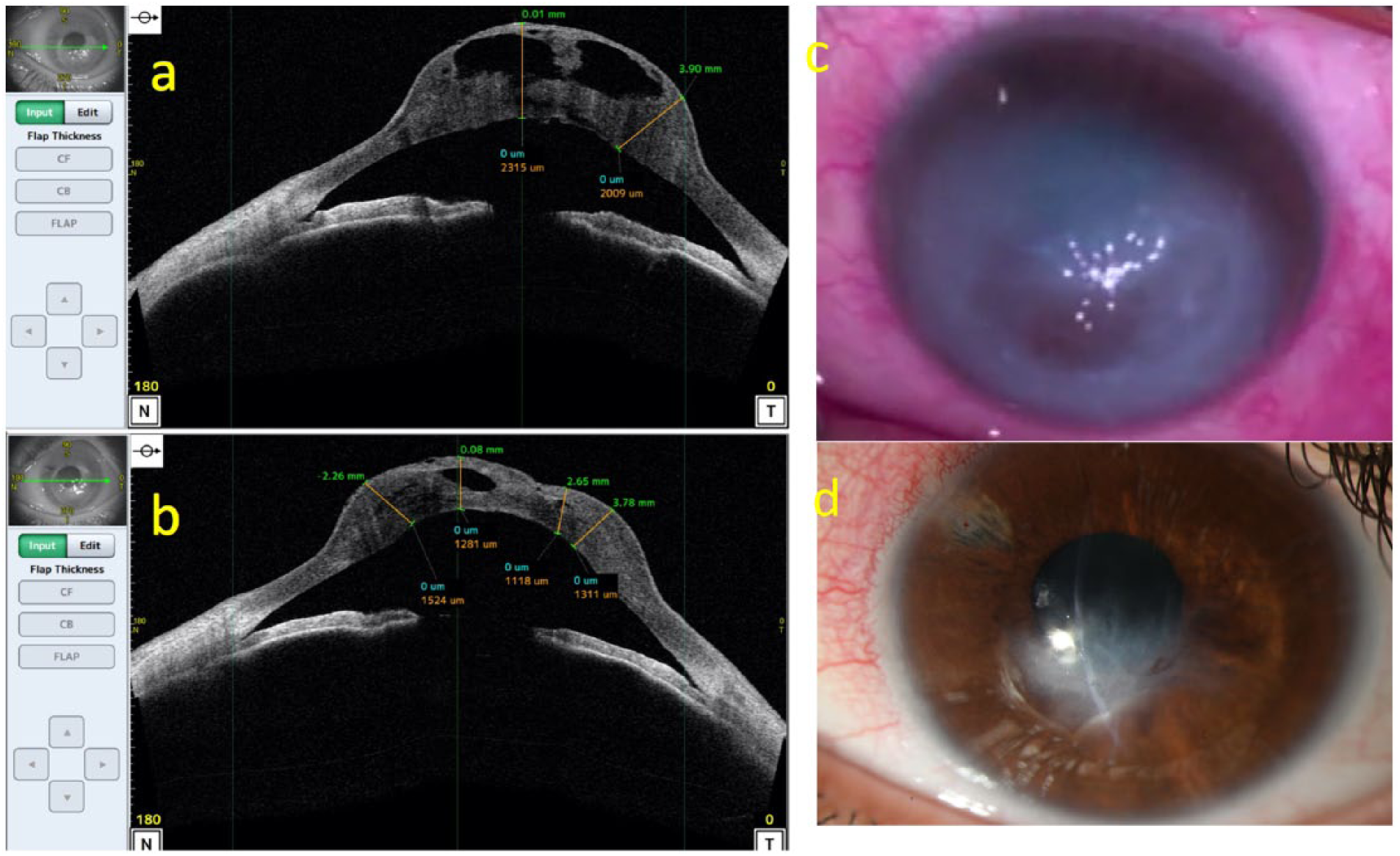
Preoperative anterior segment optical coherence tomography (AS-OCT) (a) shows Descemet’s tear and severe edema. Postoperative (first day after surgery) AS-OCT (b) shows decrease in the corneal edema and attached Descemet’s membrane. (c) Preoperative localized bulla and (d) 3-week state after the resolution of corneal hydrops.
The detailed data of patients underwent venting incision and intracameral SF6 injection.
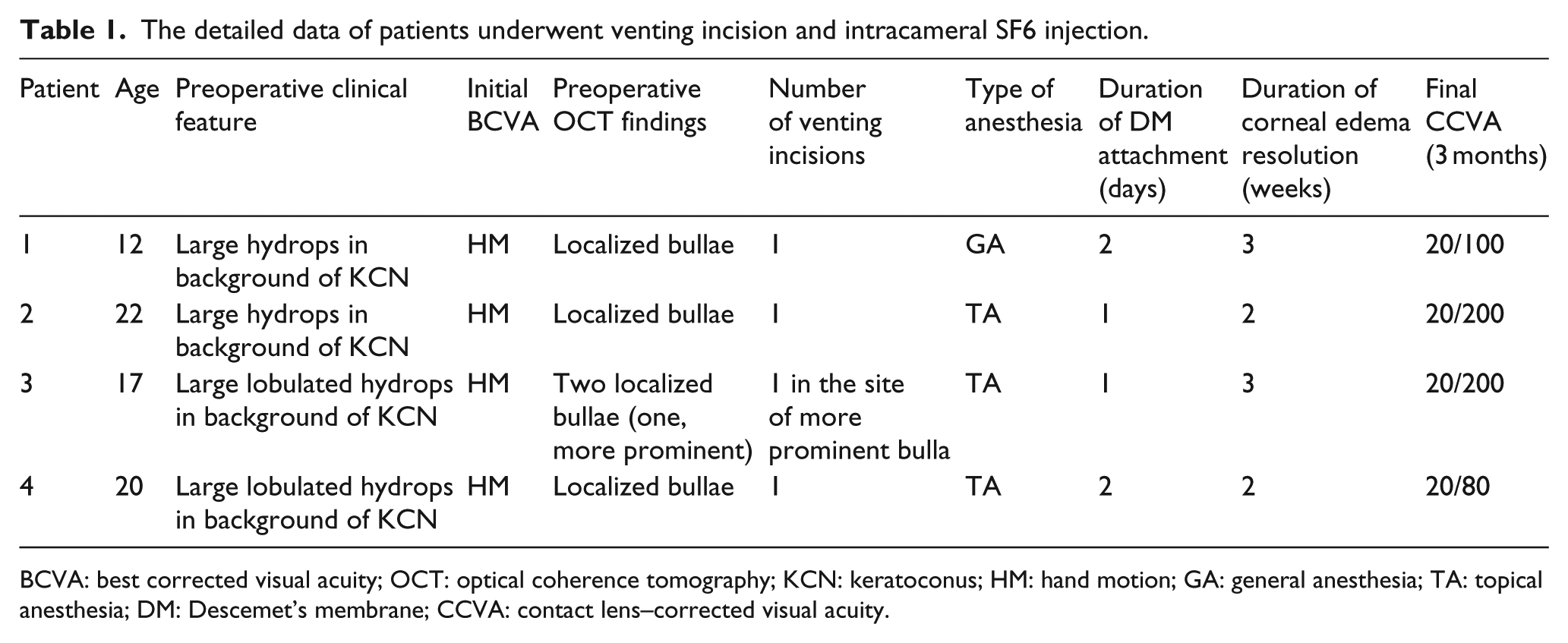
BCVA: best corrected visual acuity; OCT: optical coherence tomography; KCN: keratoconus; HM: hand motion; GA: general anesthesia; TA: topical anesthesia; DM: Descemet’s membrane; CCVA: contact lens–corrected visual acuity.
Discussion
Several modalities have been proposed for the management of acute hydrops. In case of the small and relatively flat bulla, mere medical therapy, including lubricants, topical corticosteroids, hypertonic saline, and aqueous suppressants, suffices. 4 However, many experts prefer to perform surgery for a large hydrops.
The goal of surgical management is the restoration of DM integrity at the site of the presumed defect. Different approaches are employed to fulfill this goal. Passing a full-thickness corneal suture encompassing the torn DM surrounding the defect is a recommended technique.3–5 Moreover, DM could be reattached using an intracameral injection of gas especially SF6 and C3F8 which have more extended durability.2,3 Passing a full-thickness suture could lead to postoperative endophthalmitis and needs specific considerations for suture removal. However, our technique could prevent these additional concerns.
This study proposed a new technique for intra-operative localization corneal bulla in the setting of large acute hydrops. We implemented this method in four patients and achieved a rate of 100% in the successful drainage of the intrastromal bulla and DM re-attachment.
There are multiple studies in the literature that investigated the role of ultrasound biomicroscopy (UBM) in the evaluation of corneal hydrops. UBM can efficiently visualize stromal edema and cyst along with the exact site of defective cleft as a discontinuity in hyper-reflective decrement’s membrane. 4 Nevertheless, the additional ocular discomfort imposed on the patient is one of the drawbacks of this procedure. AS-OCT is also a well-known modality for the assessment of the cornea. It is shown that AS-OCT is prosperous in the detailed examination of anterior segment despite significant stromal edema. In corneal hydrops, flat or rolled ends of split DM are readily seen via OCT.5,6 However, this technique needs a complying patient with the ability to maintain fixation for a period and many of advance keratoconus cases are patients with Down syndrome suffering from mental retardation. Vajpayee et al. 1 proposed the drainage of trapped aqueous humor using AS-OCT as a guide to reach a more rapid recovery. They used venting incision under the AS-OCT picture guide as previously documented in Descemet’s stripping endothelial keratoplasty (DSEK). They found a rate of 100% DM attachment after a maximum of 3 days. The difference between our work and their work was real-time drainage using a dye to determine the exact site of trapped aqueous in our setting. Drainage using AS-OCT printouts could be challenging to find the exact site and may need multiple incisions despite one incision in our technique.
A significant limitation of corneal venting is the risk of the perforation especially in the presence of a very thin cornea. Nonetheless, the sterile condition in the operating room brings this complication under control. Also, a compressing suture could be applied with a dual purpose of primary repair and facilitating closure of DM gap. In eyes with diffuse bullous changes and generalized corneal edema (albeit less severe protrusion), the site of maximum corneal edema and bullae formation may not always correspond to the site of initial pulling by vital dye, so this technique may not always work in these cases.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.