
Abstract
Tadeusz Krwawicz (1910–1988) pioneered the use of cryosurgery in, as ophthalmology. The idea arose in 1959 while experimenting because on lyophilization to store corneas and lenses for transplantation it was difficult to remove the lens without damage the capsule was usually torn. Subsequent experiments on rabbits revealed that touching the lens with a wire cooled to 203°K (–70°C) resulted in firm attachment of the lens capsule and subcapsular masses. A cryoextractor was developed and employed for clinical use in cataract extraction, likewise in intumescent cataracts and lens subluxation. Cataract surgery utilizing cryoextraction led to substantial progress to ophthalmology by reducing the number of complications, particularly capsule rupture, and resulted in achieving better outcome compared to other methods. This surgery soon and for almost 20 years became a routine method used all around the world in cataract removal. Simultaneously, Krwawicz developed techniques for corneal refractive surgery—partial lamellar removal of the corneal stroma and temporary interlaminar introduction of a plastic disk in order to change the corneal curvature. Krwawicz presented other ophthalmic interests—his research concerned immunology, histology, histochemistry, biochemistry of ocular tissue, and mainly corneal and experimental surgery with a particular focus on the pathology of the cornea.
Keywords
Biography
Krwawicz 1 (Figure 1) was born in Lvov on 15 January 1910. In 1938, he graduated from medical studies at the Faculty of Medicine of Jan Kazimierz University in Lvov. After receiving his diploma, thanks to persuasion by his colleagues (later famous professors Tadeusz Kielanowski and Wiktor Bross), he began scientific research on the cornea at the Department of Histology led by Bolesław Jałowy. Krwawicz dreamed of surgery; however, lack of employment opportunities in the Surgery Department with Professor T. Ostrowski made him accept the position of an assistant in the Ophthalmology Department led by Professor Adam Bednarski. Soon, he became fascinated by this discipline in terms of medical knowledge and devoted his entire career to it.
Tadeusz Krwawicz (1910–1988).
In 1939, he received a PhD based on his dissertation titled “On the colloid and peptic properties of corneal cells.” Krwawicz survived the extremely difficult for Lvov and its inhabitants Second World War period working in the Ophthalmology Department, helping many numbers of patients, including those who were wounded in the front fighting lines and during raids of the city. 2
He described this period as the following: There were rumors that there might be an opening in Professor Bednarski’s Ophthalmology Department. I was urged to take up this opportunity, but was still hesitant, hoping for a place in surgery. However, I applied and was accepted. After several months, I never wished to leave that clinic. With time, my admiration for Doc. J. Grzędzielski grew as he was a fine doctor, outstanding surgeon, and erudite, implementing novel developments. I am positive that had he not been executed, together with other academicians from Lvov in July, 1941, during the Nazi-German occupation, he would have reached the top in world ophthalmology.
1
In 1944, Tadeusz Krwawicz was enrolled in the military service in the Polish Second Army in Lublin and took over the Department of Ophthalmology of the II District Hospital.
After the end of the war, he was demobilized with the rank of a major and began working at the University of Lublin. Initially, he organized a Department of Pediatric Ophthalmology at the Child Jesus Hospital in Lublin. At the same time, Professor Ignacy Abramowicz came to Lublin where he tried to set up a University Clinic based on the Ophthalmology Department of the Municipal Hospital. Discouraged by difficulties, he moved to Gdańsk. His successor, Doc. Jasiński, also resigned from working in Lublin.
In 1948, the Council of the Medical Faculty of the Maria Curie-Skłodowska University entrusted Doctor Krwawicz with the duties of the head of the not-yet-existing Ophthalmology Department. For this purpose, with the energy characteristic of himself, he initiated adapting a house at Staszica Street and in very difficult conditions, he began his medical, scientific, and teaching activity.
In 1949, under the auspice of Professor Abramowicz, Krwawicz3,4 received his habilitation degree at the Medical University of Gdańsk on the basis of the dissertation entitled “Immunological properties of the eye.” In 1957, Krwawicz became a professor and in subsequent years, thanks to his initiative, a modern Ophthalmological Department was built in Lublin. In 1966, he founded the International Society of Cryo-ophthalmology and became its first President.
In the 1960s and 1970s, he gained membership into 17 foreign scientific societies, including the Societe Francaise d’Ophthalmologie, Oxford Ophthalmological Congress, Ophthalmological Society of the United Kingdom, and the International College of Surgeons. He also received honorary membership from numerous scientific societies, including the Barraquer Institute of America, Society of Eye Surgeons, and All-Russian and East-German Ophthalmological Societies.
For 25 years, he was the President of the Polish Ophthalmological Society. In recognition of his intense scientific and professional activity, numerous awards and honors were granted to him between the years 1964 and 1977 within the country and worldwide, including the Gold Medal Barraquer y Barraquer (Figure 2), the Teodor Axenfeld award, Nessim Habiff award, the award of the Scientific Institute of Oculistic Research in Venezuela, award of the International Biographical Centre in Cambridge, and the degree of honoris causa from the Medical University in Lublin and from the Soemmelweis University in Budapest. Krwawicz educated a large number of ophthalmologists, many of whom became heads of ophthalmological departments. Out of his students, 28 received the degree of Doctor of Medical Sciences including his only son, Lesław Krwawicz.

Krwawicz during the ceremony of awarding the Barraquer y Barraquer Gold Medal.
Raised in the Polish eastern borderlands, Tadeusz Krwawicz maintained respect for the historical and cultural past of Poland. Evidence of this was his passion for collecting paintings of Polish artists and subsequent creation of a wonderful collection.
He was fascinated by 17th-century paintings. In his gallery, he gathered the works of artists of Young Poland—Józef Chełmoński, Kazimierz Sichulski, and Jacek Malczewski. He was particularly fond of Peter Claesza’s still life series and the works of Józef Brandt and Henryk Siemiradzki. He paid particular attention to how the artists recreated the frailties and diseases of the human body. In his collection, the work of Fryderyk Pautsch is worth noting as it portrays an old man with sick eye, sitting in the spring sunshine “as if to confirm—as Krwawicz said—that both humans and nature strive for sunlight” 1 (Figure 3). He loved nature, and he spent his spare time hunting in the company of his friends and his favorite dogs. His other hobby was connected to his many travels, namely his car, which he loved to drive. He spent all of his free time resting, surrounded by nature in his house in Kazimierz Dolny; he always searched for contact with nature and appreciated its beauty.

The painting of Fryderyk Pautsch “Blind Man” (1909; Krwawicz’s favorite from his private collection).
Tadeusz Krwawicz died in Lublin on 17 August 1988 and is buried in the cemetery in Kazimierz Dolny.
Krwawicz’s successor as the head of the Ophthalmology Clinic in Lublin was Professor Zbigniew Zagórski, thanks to whom the Clinic bears the name of, Tadeusz Krwawicz. He also initiated granting the award of the “Gold Medal of Professor Tadeusz Krwawicz.” This award was given in 1993 to Professor Gottfried Naumann from the University of Erlangen Norynberg; in 1996 to Professor Franz Frankhauser from the University of Brno; in 1999 to Professor Peter Watson from Cambridge University; and in 2003 to Professor Stephen Drance from the University of British Columbia. In 2003, thanks to Professor Zagórski, the International Council of Ophthalmology took over the tradition of granting the medal. In 2005, the Gold Medal of Tadeusz Krwawicz was introduced into the Statute of the Council as an official award of the International Council of Ophthalmology awarded every 4 years during the World Ophthalmology Congress. (Tadeusz Krwawicz’s Gold Medal recognizes significant contributions to ophthalmology, especially in diseases of the anterior segment and/or introduction of new technologies, and the advancement of international relationships among ophthalmologists.) In 2008, the medal was awarded to Professor Douglas Anderson from Miami, in 2012 to Professor Alan Bird from London, and in 2016 to Professor Marie-José Tassignon from Antwerp.
Research conducted by Krwawicz concerned immunology, histology, histochemistry, biochemistry of ocular tissue, and corneal and experimental surgery with a particular focus on the pathology of the cornea.
The application of proteolytic enzymes in inflammatory corneal conditions
Understanding the biochemical phenomena taking place in the cornea made it possible to determine the mechanisms accompanying its healing after injuries and inflammatory conditions, as well as to develop a method of clearing corneal ulcers with proteolytic enzymes. 5 This method consisted of using trypsin solution locally in the form of eye drops or through direct application of a swab impregnated with its solution onto the diseased place for approximately 48 h, following an antibiotic treatment, mainly streptomycin and penicillin. By employing a trypsin solution (0.1–0.5 mg/mL) in viral diseases of the cornea, it was stated that both new and previously unsuccessfully treated cases healed faster and without leaving larger scars.
Ocular chalcosis
Krwawicz, together with Associate Professor Kazimierz Zagórski, was also involved in developing methods of preventing ocular chalcosis and conducted experiments on electrochemical removal of copper debris from the vitreous body. Studies conducted on animals were to hinder or eliminate the chemical activity of copper elements inherent within the vitreous body by covering it with a layer of copper sulfide. 6 This effect was based on the introduction of a small amount of hydrogen sulfide (0.5–1.0 mL) into the vitreous body, which did not exceed the amount of copper found in the normal vitreous body. Low level of copper ions in the vitreous body after the neutralization of the sliver inside the eyeball was to significantly prevent ocular chalcosis.
Corneal transplants
Krwawicz was one of the first in Poland to deal with corneal transplantation or keratoplasty and plastic surgery of the cornea in order to compensate for refractive errors. He utilized intracorneal lamellar keratoplasty, applying fresh and lyophilized grafts. 7 With the already existing method, lamellar keratoplasty was performed only on the surface of the cornea and the graft was fixed with sutures, whereby the operation conducted by the Professor differed in that the lamellar graft was implemented into the central part of the cornea under the scar into a specially formed pocket. The scar that formed the front wall of the pocket partially covered the graft and protected it until it became accreted to the bed. This method of placing the graft made it retain the desired position. After the graft was firmly attached to the bed, the anterior wall of the pocket (the scar proper) was removed, exposing it permanently. Owing to keratoplasty, it was possible to avoid suturing, significantly simplifying the operation and lowering the risk of failure.
Krwawicz also developed a method of economic lyophilization, thanks to which the sample from the donor’s cornea rapidly frozen in isopentane was not hampered by injury and was later subjected to slow drying at a low temperature. Such a preparation of the cornea allowed it to be kept for an indefinite period of time and this made it possible to open a cornea bank in Lublin.
Refractive surgery
In the 1950s and 1960s, there were several attempts to correct high refractive errors. The most successful were keratomileusis and epikeratophakia developed by Jose Barraquer.8–11 Modified keratomileusis—referred to as LASIK (laser-assisted in situ keratomileusis)—is now accomplished with an excimer laser, while a keratome or femtosecond laser is applied for flap creation. Krwawicz was also working on innovative methods of changing corneal curvature. He introduced the so-called lamellar stromectomy (stromectomia lamellaris)—partial lamellar removal of the corneal stroma—in order to correct myopia (Figure 4). 12 Some decades later, it was also considered a precursor of LASIK. The procedure was performed under topical anesthesia. The cornea was marked with a 5-mm trepane. On the margin of the operative area, a 3-mm incision was made with a keratome and the superficial cornea was delaminated with a small flat knife. The created flap was lifted with a silk suture. Another incision was made, at the bottom of the first one, but reaching deeper layers of the cornea. The stroma was again split longitudinally, but this time deeper and over a slightly smaller area, subsequently being removed with forceps. Postoperatively, atropine, antibiotics, and cortisone were applied. The surgery was performed in three patients with anisometropia and unilateral high myopic astigmatism. No complications were observed in a maximal 10-month observation period. Uncorrected distance visual acuity was equal to the preoperative best-corrected visual acuity, where two patients achieved 20/40 while one patient reached 20/50. 12 In a subsequent paper, seven further operations were reported and corneal resectors 2.1–2.6 mm wide were introduced. 13
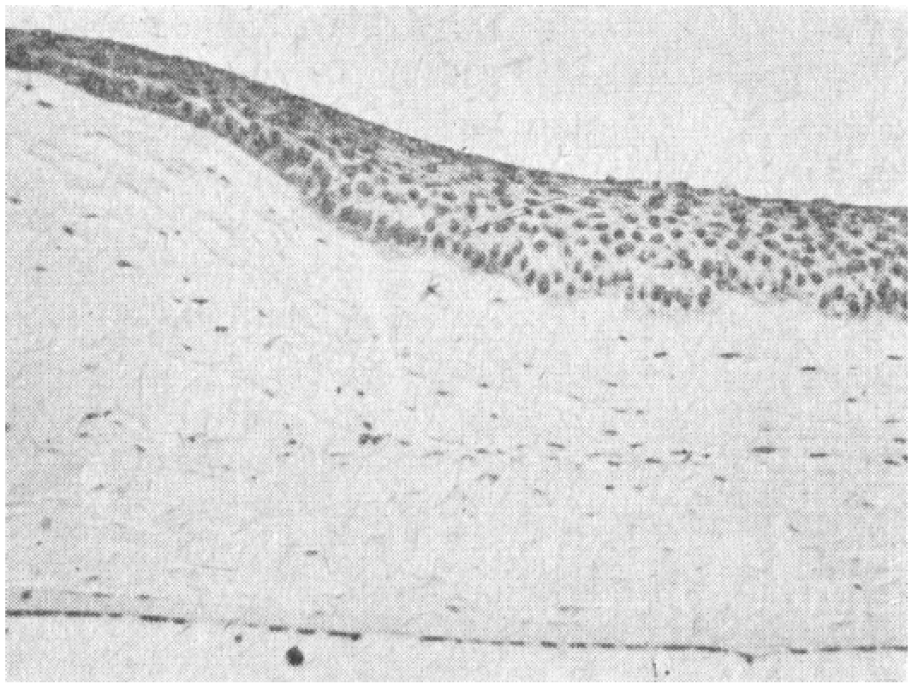
Section of a rabbit’s cornea 30 days after partial lamellar stromectomy—thinning of the cornea can be observed, as well as stromal cell multiplication and epithelial thickening. 51
Owing to the lack of operating microscope in that time, the procedure was challenging. Krwawicz was using Zeiss loupes that magnified the image twice. This operation required precision and mastership: “When I described it in Bogota”—Krwawicz recalled—“everyone asked me what kind of microscope did I use. I did not have a microscope, and I was ashamed to admit it so I equivocated until everybody gave me a break.” Krwawicz reported patients’ great interest in this procedure; however, in most cases, he discouraged such an intervention. He performed the surgery only with anisometropia greater than or equal to 3 D. 14 With the introduction of soft contact lenses, the aforementioned surgery was abandoned.
Krwawicz 15 is also the creator of another refractive surgery that seeks to change the corneal curvature and compensate for the refractive error of aphakia by temporary introduction of a plastic disk intrastromally. Krwawicz observed that after permanent intrastromal implantation of a 3.5- to 4-mm-wide polymethylacrylic lens in rabbits, the first delicate corneal opacities were observed after 50 days, while infiltrates and significant opacities developed after 100 days. If the lens was removed 7 days after the implantation, the cornea remained completely transparent and inclined in the central region. 16 Subsequently, the first clinical application was described in eight eyes. 15 Near the corneal margin, a vertical incision 4 mm long and deep enough to penetrate into the deeper layers of the stroma was made with a small keratome. The corneal stroma was split with a flat knife and a pocket was formed in the central part of the cornea, corresponding in shape and size to the lens to be implanted. With lifting of the incision edge with a spatula, a plastic lens was introduced with another thin spatula into the incision, pushed through the channel between the split layers of the cornea, and finally placed at the bottom of the pocket, that is, in the center of the cornea. Topical atropine, antibiotics, and later cortisone were administered postoperatively. After 8–10 days, the plastic lens was removed by pulling it out with forceps; however, in one case, it was removed after 48 h because of corneal infiltrates. In two eyes, cataract extraction preceded the plastic operation, while in six eyes, it was conducted 10–14 days after implant removal. Uncorrected visual acuity of 5/15 was achieved in four eyes, in one eye 5/20, and in three eyes 5/30. However, the extent of the benefits of the surgery was gradually decreased. Nowadays, intracorneal implants are made from newer biocompatible materials and can be implanted permanently to improve vision.
Cryosurgery
Krwawicz’s most important achievement was the introduction of low temperatures into eye surgery and eye therapy. In 1960, during the session of the XXVII Congress of the Polish Ophthalmic Society in Poznań, he proposed a new method of intracapsular cataract extraction, which he called cryoextraction. 17
Krwawicz’s team included Kazimierz Zagórski (1910–1989; the father of Zbigniew Zagórski, Professor of Ophthalmology and Krwawicz’s successor as Chair of Ophthalmology in Lublin) a pharmacist and chemist who, in the mid-1950s, introduced dry ice into the laboratory, a substance which had never been seen before by the staff. A mixture of dry ice and alcohol was later employed for freezing tissues during lyophilization and for cooling cryoextractors and cryoapplicators.
Zagórski suggested starting studies on lyophilization of tissues, especially the cornea, and developed special equipment to allow for very delicate freezing and drying. The tissue retained many of its original features and certain elements could even be revitalized. The method was applied clinically for lamellar keratoplasties, especially the intracorneal lamellar keratoplasty developed by Krwawicz.
The idea of using low temperatures to remove cataracts arose in 1959 while experimenting on lyophilization to store corneas and lenses for transplantation. A method was needed to remove the lens without damage, a difficult task as the capsule was usually torn. The idea was to freeze the lens in situ in order to remove it when hardened. The first trial was carried out very crudely, using a small soldering tool with a copper tip cooled in a mixture of dry ice and methanol, but it worked. Unexpectedly, part of the capsule and cortex adhered strongly to the wire used. Thus, the decision was made to investigate the possibilities of this experiment. An idea emerged to use the copper wire soldered to a metal flask that was cooled in a mixture of dry ice and methyl alcohol to approximately 203°K (–70°C); this is how the prototype of the cryoextractor came into being. 1 The original cryoextractor had the following dimensions: copper rod-length: 10 cm; diameter: 10 mm; and the ending had a 1-mm ball tip. In order to isolate it from low temperatures, it was placed in a plastic cover. The starting temperature of an already cooled cryoextractor was approximately −79°C (about 194°K). 18
The first attempts of lens extraction conducted by Krwawicz were performed on rabbits. Specifically he touched the bare and dried lens with a cooled wire. The result was that the lens capsule and the subcapsular lens masses became attached to the early cryoextractor. Initially, Krwawicz18,19 applied low temperatures in the intumescent cataract removal, senile cataract in various periods of its maturation,20,21 and lens subluxation. 22 This surgical technique consisted of applying the tip of the cryoextractor to the equator of the lens after a prior incision in the limbus, corneal flap deflection, and the retraction of the iris upward using the cryoextractor (or other equipment) with assistance, then freezing the lens and its removal through rotational movement. After removing the lens, the iris was placed in its proper position and the corneal flap was released (Figure 5). With time, Krwawicz 23 placed near the limbus—before performing the cut—a stitch which was to deflect the corneal flap. Krwawicz immediately got the idea of applying this method in cataract surgery, which proved very successful, dramatically decreasing the rate of capsular rupture. Krwawicz described his discovery as “serendipity,” but for more than two decades, cryoextraction was the most frequently used method in cataract surgery around the world. He employed primitive cryoextractors and cryoapplicators, which were cooled in the mixture of dry ice and methanol. Only several years later, he could make use of the modern devices developed by Amoils.
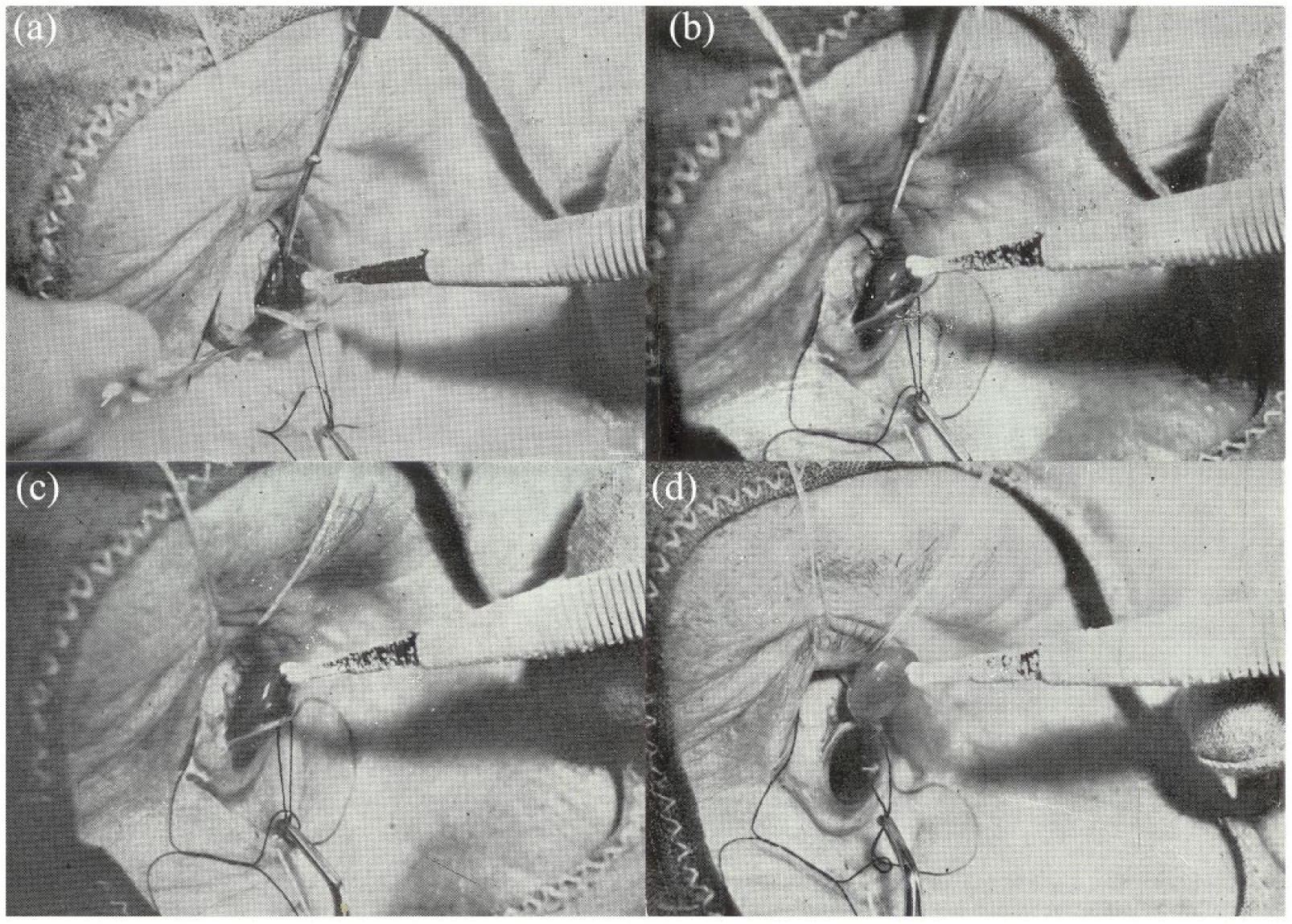
Cataract surgery with the cryoextractor: (a) the tip of the cryoextractor covered with a thin layer of ice applied to the lens at approximately 12.00 o’clock near the equator, (b) frenulum is torn off with a rotary movement, (c) the lens held by frenula is pulled toward the precinct of the surgery wound, and (d) the removed lens adheres closely to the cryoextractor.
This surgery soon and for almost 20 years became a routine method utilized all around the world in cataract removal. Professor Hollwitch, the president of the World Academy of Ophthalmology, stated that the last hundred years witnessed great progress in the treatment of glaucoma and the closure of the retinal detachment using the Gonina method. I am inclined to recognize Professor Krwawicz’s cryoextraction as the third achievement equally important as the two afore mentioned.
1
Of immense importance to the success of intracapsular cataract extraction was frenula release. Mechanical frenula release was not free from technical complications and the possibility of complications, such as iritis, cyclitis, discharge of the vitreous humor, or retinal detachment resulting from extensive pulling or applying pressure. Thus, in cases where intraoperative significant ciliary zonule resistance was stated, Krwawicz applied enzymatic zonulolysis. 23
Cryoextraction of the cataract became popular worldwide in removal of all types of senile cataract, including types with complications.24–38
Cataract surgery with cryoextraction advanced ophthalmology by reducing the number of complications, resulting in achieving better results compared to other methods. Apart from many ophthalmologists fascinated by this method, there were also many skeptics. After the announcement of his results in England in 1961, Professor Krwawicz 1 hosted in Lublin Professor Riddell, who, after his return from Poland, stated: “I was there for a long time, I looked and saw a lot, I came to believe that he [Krwawicz] is either a madman or a genius. It is better we wait.” In this way, England introduced cryosurgery with an approximately 5-year delay.
Physicians working under difficult conditions and with poor treatment results, such as those in Third World countries, adopted this new method immediately, having considerable success during cataract operations.
Upon the publication of the first works of Krwawicz in the West on using low temperatures in eye surgery and with his visit to the United States where he arrived with a series of lectures, the mass production of cryoextractors began. Of note is that this invention was not protected by international patent rights.
The introduction of cryosurgery of cataracts encouraged the seeking of other opportunities to use low temperatures. During cataract removal, Krwawicz noticed that fortuitous short-term freezing of the cornea does not have any adverse effects. This gave him the idea to employ low temperatures in the treatment of viral corneal ulcers,39,40 a condition that does not respond to any current treatment. Treatment with this method became very effective, and the success encouraged him and his colleagues to conduct numerous studies seeking to explain the effect of low temperatures on eye tissues. This mechanism proved to be omnidirectional and soon cryotherapy was applied to wounds, scars, and corneal degeneration. 41 Once again, the interest and development of the proposal of Bietti 42 and Deutschmann 43 in using low temperatures during surgery of retinal detachments and other forms of glaucoma had begun. Soon, cryopexy supplanted surgical diathermy.
The most important advantage of cryopexy was that without damaging the sclera it decreased the possibility of complications from the uveal layer and facilitated eventual reoperation. Taking into consideration other advantages of this method, it is essential to mention there is a lower tendency of hemorrhage appearance, lack of sub-retinal effusion, minimal of no damage to the vitreous body and vessels, and the possibility of performing it on a wet surface. Cryopexy, in combination with other treatments, aimed to induce chorioretinal adhesions in retinal detachment, significantly improving the outcome. 44 Krwawicz used cryopexy together with the scleral buckling according to Arruga, achieving a 88.2% reattachment rate in a large group of 460 patients. The destructive and inflammatory properties of low temperatures have also been leveraged in peripheral retinal degeneration and in blocking the openings in its flat lamellar, 45 in the treatment of inoperable hemorrhage into the anterior chamber 46 and to the vitreous body. 47
In 1967, taking advantage of the properties of cold, Krwawicz 48 introduced cryotherapy together with casual treatment of subacute and chronic inflammation of the iris, ciliary body, and uveitis, including uveitis with hypertension. Krwawicz put forth utilizing cyclocryotherapy in cases where surgical methods used in the treatment of primary glaucoma proved futile, when surgery of secondary glaucoma was impossible, and in cases of aphakic eyes. Soon, low temperatures proved to be beneficial in the treatment of retinopathy of prematurity, diabetic retinopathy, and many other illnesses.
The first applications of low temperatures in ophthalmology took place in the 1930s for retinal detachment42,43 and in 1948 for glaucoma. 49 Their use, however, was very limited. After the introduction of cataract cryoextraction, further cryogenic techniques were developed quickly. Krwawicz used it successfully for the treatment of herpetic keratitis, which posed a serious problem owing to widespread use of corticosteroids and lack of antiviral drugs. He also applied low temperatures in the treatment of certain forms of uveitis, intravitreal hemorrhages, corneal scars, and corneal degenerations. For many years, cryotherapy was the leading method for inducing chorioretinal adhesions in retinal detachment surgery, as advocated by Lincoff and McLean 50 in 1965. Cyclocryotherapy in glaucoma is frequently practiced and cryosurgery has become critical in oncology.
Conclusion
Tadeusz Krwawicz’s contribution via the introduction of cryosurgery to cataract treatment is well known. It is worth underscoring, however, that cryotherapy found application in other fields of ophthalmology, such as the treatment of corneal inflammation, retinal detachment, and glaucoma. Cryotherapy and cryoretinopexy became effective treatment methods used till recent times. With this, Krwawicz was a pioneer not only in cataract cryoextraction but also in keratoplasty (intracorneal lamellar keratoplasty with a lyophilized graft) and certain refractive procedures, like stromectomia lamellaris in myopia (a precursor of LASIK) and by changing the corneal curvature through allogeneic intracorneal implants.
Sir Stewart Duke-Elder, in his System of Ophthal-mology, wrote: “He will be always remembered for introduction of cryosurgical techniques in 1959, especially cataract cryoextraction and cryotherapy of such diseases as viral infections of the cornea. These achievements made him well-known all over the world.”
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially funded by the Foundation for Ophthalmology Development, Poznan, Poland. A.G. reports grants, personal fees and non-financial support from Bayer, non-financial support from Novartis, non-financial support from Alcon, non-financial support from Thea, personal fees and non-financial support from Valeant, and non-financial support from Santen, outside the submitted work. P.K. reports non-financial support from Visim.