
Abstract
Purpose:
Combined hamartoma of the retina and retinal pigment epithelium is a rare benign tumor characterized by a variable combination of glial, vascular, and pigmented components. The purpose of our study was to analyze the features of combined hamartoma of the retina and retinal pigment epithelium on optical coherence tomography angiography.
Methods:
Small case series of two cases of combined hamartoma of the retina and retinal pigment epithelium with macular and optic nerve involvement, evaluated with multimodal imaging including optical coherence tomography, fluorescein angiography, and optical coherence tomography angiography.
Results:
On optical coherence tomography, combined hamartoma of the retina and retinal pigment epithelium is characterized by disruption of the inner neurosensory retina and a variable degree of involvement of the external retina. Optical coherence tomography angiography showed diffuse alterations of the retinal vessels of the superficial and deeper layers, extended to the peripapillary area. Vessel abnormalities included increased tortuosity and caliber of vessels, vascular traction, and vessel stretching within the lesion.
Conclusion:
Optical coherence tomography angiography allows in-depth multilayer analysis of tumor vascular network, highlighting the fine abnormalities of retinal vasculature characteristic of combined hamartoma of the retina and retinal pigment epithelium.
Keywords
Introduction
Combined hamartoma of the retina and retinal pigment epithelium (CHRRPE) is a rare, generally unilateral, benign tumor first reported by Gass in 1973. 1 On histological examination, this condition is characterized by a variable combination of glial, vascular, and pigmented elements, resulting in peculiar thickening of the sensory retina, blood vessels proliferation, and preretinal gliosis. 2 Although the etiology of this retinal disorder is currently unclear, new insight into the intrinsic vitreoretinal modifications of CHRRPE is being given by recent advances of imaging techniques.2–7 Optical coherence tomography angiography (OCT-A) is a novel, non-invasive, dye-less imaging tool, providing in-depth multilayered visualization of the retinal and choroidal vasculature, allowing to obtain distinct and more detailed information compared to conventional fluorescein angiography.6–8 The purpose of our study was to investigate the modifications of retinal microvasculature on OCT-A in a small case series of patients with CHRRPE.
Methods
This was a retrospective case series of two consecutive patients with a diagnosis of CHRRPE. The study adhered to the tenets of the declaration of Helsinki. Patients were evaluated with swept-source optical coherence tomography (SS-OCT; DRI OCT Triton, Topcon Medical Systems, Oakland, NJ) or spectral-domain optical coherence tomography (SD-OCT; Spectralis, Heidelberg Engineering, Heidelberg, Germany), fluorescein angiography (Spectralis; Heidelberg Engineering), fundus photography (Topcon fundus camera; Topcon Medical Systems), and OCT-A (AngioVue, AngioDisc 3 mm × 3 mm and 6 mm × 6 mm; Optovue, Fremont, CA or Topcon OCT-A 6 mm × 6 mm; Topcon Medical Systems).
Case 1
A 35-year-old woman was referred to our clinic for a suspect diagnosis of retinal hamartoma in her right eye. The patient had a best corrected visual acuity of 20/20 in both eyes. Ophthalmoscopic examination revealed the presence of an ill-defined whitish-yellow retinal mass located on the optic nerve, extending to the peripapillary area (Figure 1). Radial internal limiting membrane striae were found on the temporal portion of the lesion. On SS-OCT, hypo-reflective intraretinal cavities were observed in the temporal parafovea, likely due to intraretinal schisis (Figure 2). Toward the optic disk, there was a remarkable disruption of the inner neurosensory retina, with scattered hyper-reflective areas casting an inferior cone of shadow and causing partial attenuation of the ellipsoid zone and retinal pigment epithelium (RPE) below the lesion. Partial loss of the interdigitation zone was noted beneath the lesion, whereas a thin hyper-reflective band was evident overlying the mass. No differences in terms of choroidal thickness were found between the two eyes. High-definition (HD) OCT-A (3 mm × 3 mm and 6 mm × 6 mm AngioVue; Optovue) of the macular area and corresponding optical coherence tomography (OCT) B-scan showed abnormal vessels in the superficial and deep plexus, with increased tortuosity and caliber of vessels and vascular traction within the lesion (Figure 3(a)–(f)). Stretching of the inner retinal perifoveal capillary area with alterations of the foveal avascular zone was also observed (Figure 3(e)). Similar angiographic features were found in correspondence of the nerve head and radial peripapillary capillaries plexus (6 mm × 6 mm AngioVue disc; Optovue; Figure 4(a)–(f)).

Case 2. Ophthalmoscopic examination revealed the presence of an ill-defined whitish-yellow retinal mass on the optic nerve, extending to the peripapillary area. Radial retinal striae can be seen on the temporal portion of the lesion.
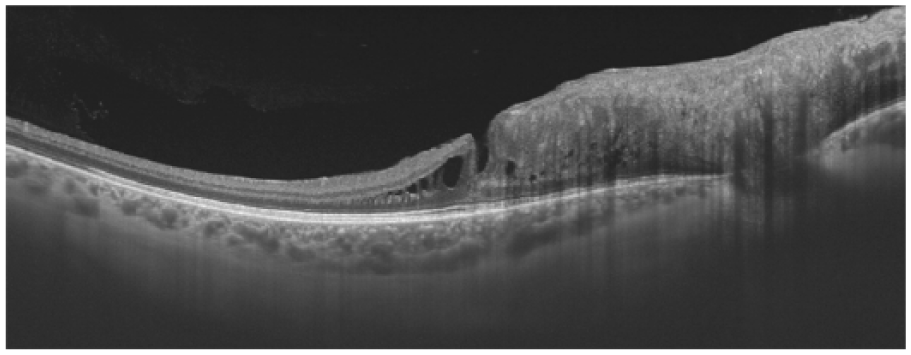
Case 1. Swept-source optical coherence tomography highlighted hypo-reflective intraretinal spaces in the temporal parafovea and a thin hyper-reflective band overlying the lesion. Notable disorganization of retinal architecture was seen adjacent to the optic disk, with major involvement of the inner retinal layers. Partial loss of the interdigitation zone was observed beneath the lesion.
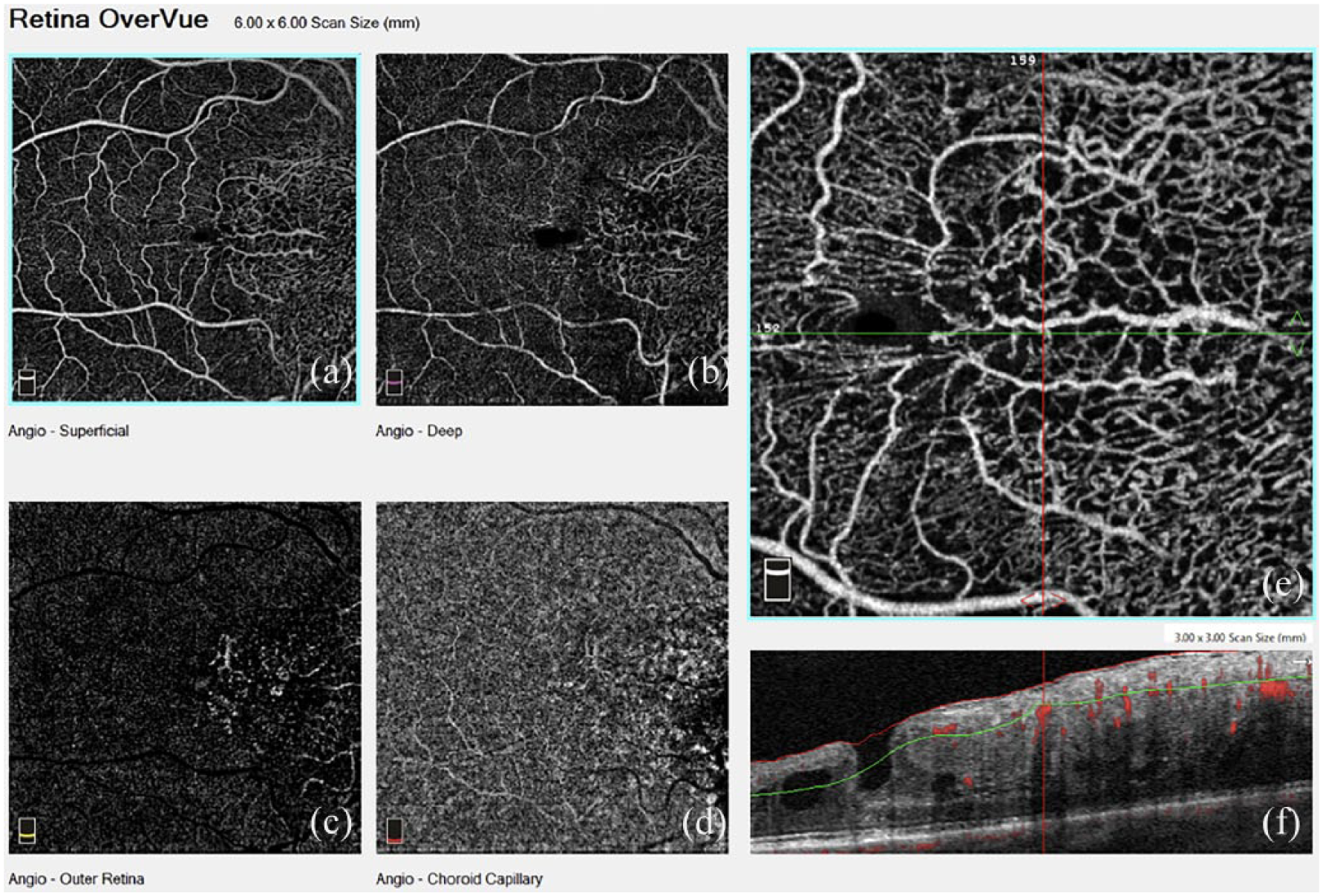
Case 1. High-definition optical coherence tomography angiography (6 mm × 6 mm AngioVue; Optovue) of the macular area showing abnormal vessels in the superficial and deep plexus within the lesion, with vascular traction (a–d). At higher magnification, increased tortuosity and caliber of vessels, stretching and distortion of the inner retinal perifoveal capillary area, and alterations of the foveal avascular zone can be noted (3 mm × 3 mm AngioVue; Optovue; e–f).
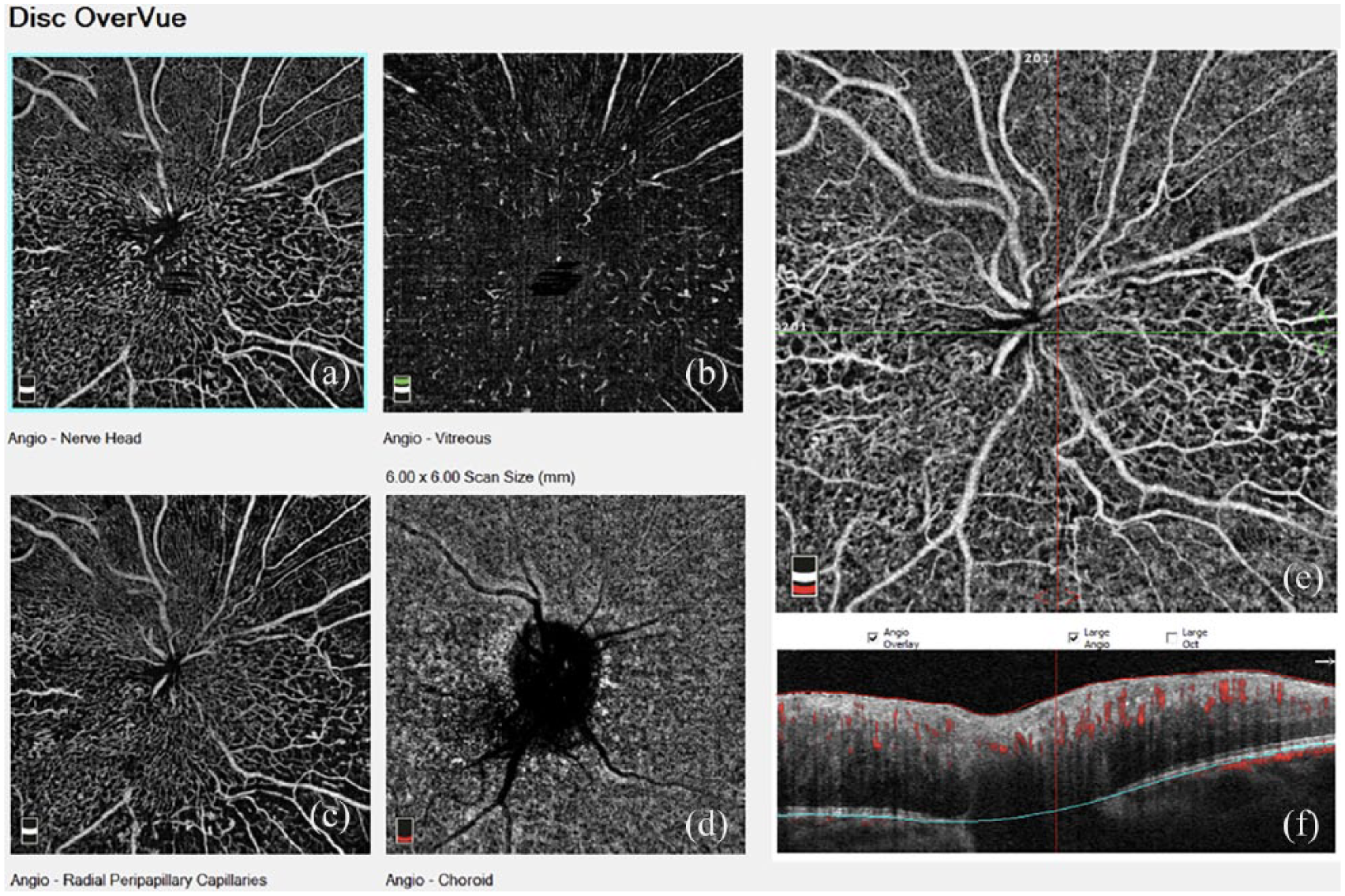
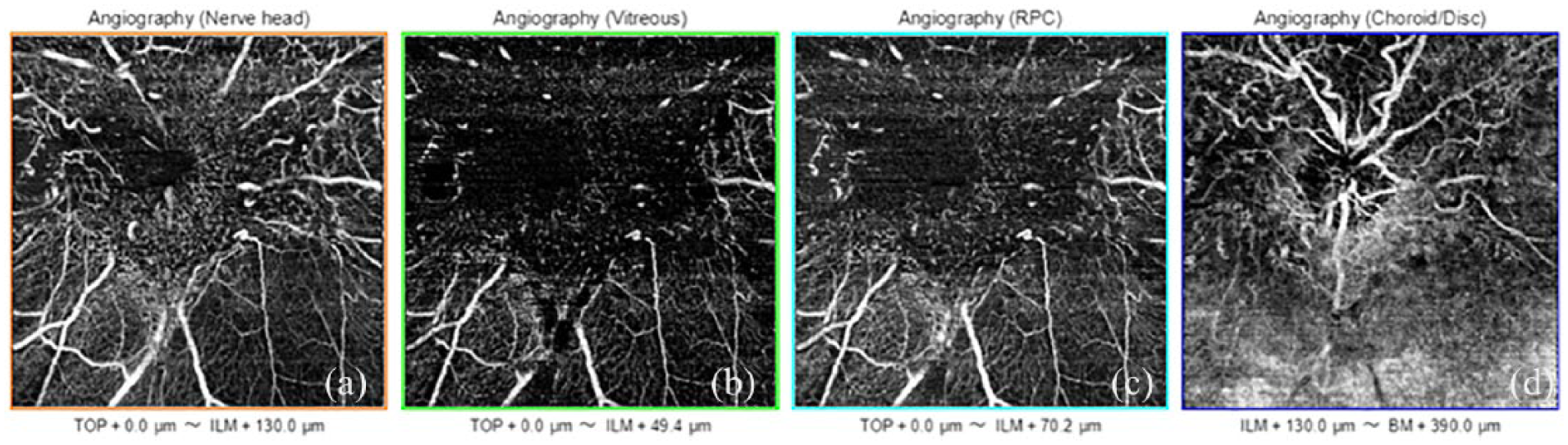
Case 1. High-definition optical coherence tomography angiography (6 mm × 6 mm AngioVue; Optovue) of the papillary area revealed similar vascular abnormalities in the superficial and deep layers (a–f).
Case 2
A 31-year-old man presented to our clinic with decreased vision to counting fingers in his right eye. On fundus examination, an ill-defined partially pigmented polygonal grayish lesion, located in the epi- and circumpapillary area, was observed in the right eye, with extensive gliosis over the lesion (Figure 5(a)). SD-OCT showed prominent thickening and disruption of the neurosensory retina, increased hyper-reflectivity of the inner retina, and epiretinal membrane overlying the lesion (Figure 5(c)). The fovea was not clearly discernible due to the disorganization of retinal architecture, causing diffuse loss of detail. The RPE appeared visible, though partially attenuated due to shadow effect from the overlying inner retinal hyper-reflective areas, whereas the ellipsoid zone and external limiting membrane appeared increasingly obscured adjacent to the optic nerve head (Figure 5(c)). En face OCT-A image of the optic nerve head (Topcon) showed marked bending and tortuosity of the major retinal vessels located in the vascular superficial layers, with diffuse vascular irregularities of the radial peripapillary network and deep vascular layers (Figure 6(a)–(d)). Fluorescein angiography of the same lesion revealed central hypo-fluorescence and typical pattern of punctate hyper-fluorescence due to early leakage from abnormal blood vessels in the pigmented lesion (Figure 5(b)). When compared to fluorescein angiogram, the corresponding OCT-A image allowed a more detailed visualization of vascular alterations.
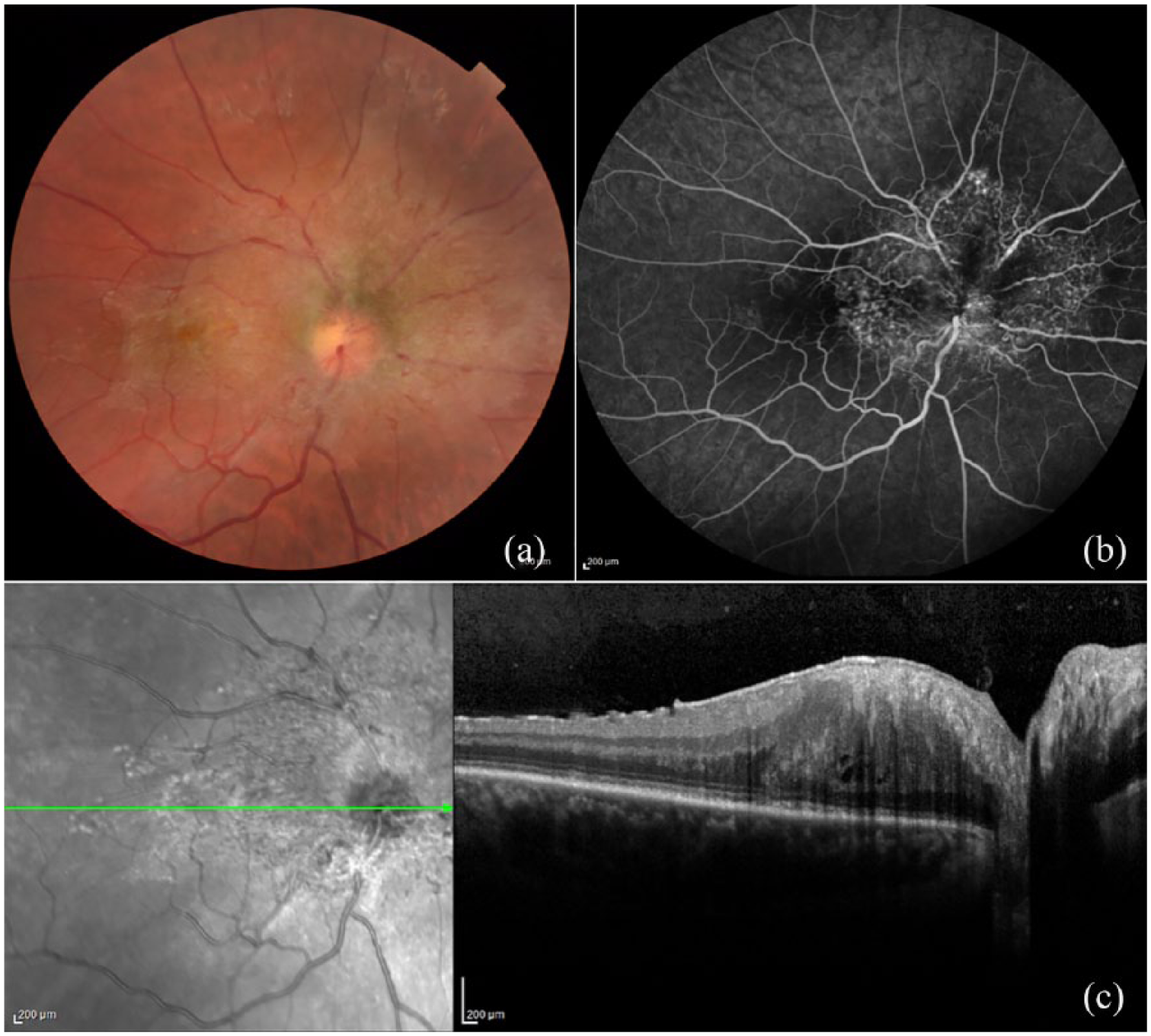
Case 2. (a) Fundus examination of the right eye showed an ill-defined partially pigmented grayish lesion, located in the epi- and circumpapillary area, with broad gliosis over the lesion encompassing the foveal area. (b) Fluorescein angiography of the hamartoma revealed central hypo-fluorescence and typical pattern of punctate hyper-fluorescence due to early leakage from abnormal tumor blood vessels. (c) Spectral-domain optical coherence tomography revealed diffuse abnormalities of the inner neurosensory retina, with prominent thickening, disruption, and increased hyper-reflectivity. An epiretinal membrane was observed overlying the lesion. The retinal pigment epithelium, ellipsoid zone, and external limiting membrane appeared partially attenuated due to shadow effect from overlying inner retinal hyper-reflective zones.
Case 2. En face optical coherence tomography angiography of the optic nerve head (Topcon) showed abnormal vascularization of the lesion, with dense tortuous retinal vessels of irregular caliber in the vascular superficial layers, and diffuse vascular irregularities of the radial peripapillary network and deep vascular layers (a–d).
Discussion
Combined hamartoma of the retina and RPE is a rare benign ocular tumor, usually diagnosed in young patients, characterized by hamartomatous proliferation of glial and vascular elements, in combination with pigmented cells.1–3 CHRRPE has been described as a tumor primarily arising from all retinal layers, extending from the vitreoretinal interface to the external retinal layers, including the RPE. 2 However, while evidence of vitreoretinal traction is still considered a prominent feature of CHRRPE, the involvement of RPE has been questioned based on recent evidence from studies focusing on the OCT features of the lesion. 2 In agreement with current concepts concerning the retinal layers altered by the tumor, no actual abnormality of the RPE was detected in our two cases on OCT scans. Nonetheless, we would not consider CHRRPE to be just limited to the inner retinal layers, since a certain degree of involvement of the external retina was found in patient 2, displaying loss of the interdigitation zone beneath the lesion. To our knowledge, this is the first case series of two patients with CHRRPE with simultaneous macular and optic nerve involvement, evaluated with OCT-A. In both cases, OCT-A was able to identify the fine macular and papillary microvascular alterations related to the presence of CHRRPE. In particular, OCT-A allowed to singularly evaluate the modification of caliber and course of retinal and papillary vessels located in the superficial and deep layers, confirming the high degree of vascularization of this benign tumor. In consideration of the high imaging resolution and non-invasive nature of this tool, routine OCT-A evaluation of CHRRPE could help gaining more information on the vascular alterations associated with these lesions. Further studies are warranted to verify if the reported vascular modifications are a distinctive feature of CHRRPE and if they remain stable or change during follow-up.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.