
Abstract
Purpose:
To evaluate the clinical characteristics of newly diagnosed pseudoexfoliative glaucoma and compare them with those pertaining to newly diagnosed primary open-angle glaucoma as well as pseudoexfoliation syndrome.
Methods:
This case–control study involved 306 participants, including patients with newly diagnosed pseudoexfoliative glaucoma, age- and sex-matched normal controls, patients with newly diagnosed primary open-angle glaucoma, and subjects with pseudoexfoliation syndrome. The study was conducted at the Glaucoma Department of Clinic for Eye Diseases, Clinical Center of Serbia, as the referral center for glaucoma in Serbia.
Results:
The mean age in the pseudoexfoliative glaucoma, primary open-angle glaucoma, pseudoexfoliation syndrome, and normal control groups was 73.61 ± 8.46, 65.50 ± 8.97, 74.81 ± 6.80, and 73.58 ± 9.34 years, respectively (pseudoexfoliative glaucoma vs primary open-angle glaucoma, p < 0.001). Unilateral pseudoexfoliative glaucoma was diagnosed in 35 patients (42.2%). The intraocular pressure was higher in the eyes affected by pseudoexfoliative glaucoma (32.0 ± 9.5 mmHg) than that in the primary open-angle glaucoma eyes (28.8 ± 5.9 mmHg) (p < 0.001). In pseudoexfoliative glaucoma and primary open-angle glaucoma eyes, glaucoma severity was determined via the vertical cup-to-disk ratio (C/D) 0.65 (0.45–1.0) versus 0.60 (0.45–1.0), p = 0.048 and visual field mean deviation −5.68 (−1.58 to −30.9) versus −4.70 (−1.39 to −31.0), p = 0.045. Alzheimer’s was the only systemic disease associated with pseudoexfoliative glaucoma in the study sample, with an odds ratio of 0.021 (95% confidence interval = 0.00−21.52, p = 0.022).
Conclusion:
At the time of diagnosis, pseudoexfoliative glaucoma exhibits different clinical features compared with primary open-angle glaucoma. Higher intraocular pressure, narrow or occludable angle, increased trabecular pigmentation, phacodonesis, and poorer pupillary dilatation emerged as the factors associated with pseudoexfoliative glaucoma.
Keywords
Introduction
Pseudoexfoliation syndrome (XFS) is an age-related generalized disorder of the extracellular matrix, characterized by excessive production and progressive accumulation of fibrillar pseudoexfoliation material (XFM) deposits in the anterior segment of the eye.1–3 XFS is a genetically determined systemic condition4,5 and systemic associations have been reported with transient ischemic attacks, systemic hypertension, angina, myocardial infarction, stroke, abdominal aortic aneurysm, Alzheimer’s disease, and hearing loss.6–9 The most widely recognized disease manifestation is pseudoexfoliative glaucoma (XFG), which is a common cause of blindness worldwide. 10 The etiology of XFG is still unclear and is presently not known why glaucoma develops in only about 30% of XFS eyes in patients’ lifetime. 1 Unlike XFS, XFG is not genetically determined. The known risk alleles of the single-nucleotide polymorphisms of the lysyl oxidase–like protein 1 (LOXL1) are found in nearly 100% of the population at risk for XFS. However, conversion from XFS to XFG is believed to be induced by environmental factors that increase oxidative stress in the anterior chamber. 11 XFG is the most common form of secondary open-angle glaucoma worldwide. 6 In Caucasian population, a narrow or closed angle is a rather common finding in XFS.1–3 Its global ethnic and regional prevalence is, however, highly variable. In general, it presents most often in coastal European countries. 12 Thus, it is not surprising that a particularly high incidence of XFS ranging from 25% to 75% is reported for the Nordic region. Nonetheless, XFS is relatively common in Germany, Great Britain, Italy, Russia, Spain, Turkey, and Greece, while moderately high prevalence is recorded in Hungary.12,13 In Serbia, even though accurate incidence and prevalence data for XFS/XFG are presently lacking, clinical practice suggests a frequent occurrence of XFS/XFG in local population. XFG typically develops after 60 years of age, and in most cases significant optic nerve head and visual field (VF) damage in at least one eye is already present at the time of diagnosis.3,12 XFG clinical features are distinct from those characterizing primary open-angle glaucoma (POAG). 10 When patients diagnosed with XFG are compared with POAG patients, their intraocular pressure (IOP) is often higher and the diurnal IOP fluctuation is much more significant. 14 Consequently, in the involved eye(s), optic nerve head damage and visual filed deterioration are frequently severe in XFG patients. At the population level, this may partially be counterbalanced by the fact that, in certain countries, XFG is significantly less likely to remain undiagnosed relative to POAG. 15
The purpose of this study was to evaluate the clinical characteristics of newly diagnosed untreated XFG and compare them with those pertaining to newly diagnosed untreated POAG. The second goal was to conduct a comparative analysis of the clinical features of XFG and XFS.
Methods
Study population
This case–control study involved 306 consecutive patients that were seen between June 2016 and December 2017 at the Glaucoma Department of Clinic for Eye Diseases, Clinical Center of Serbia, as the referral center for glaucoma in Serbia. The sample comprised patients with newly diagnosed XFG and age- and sex-matched normal controls (NCs), along with patients with newly diagnosed POAG and subjects with XFS. Subjects were classified as having POAG if they presented the typical glaucomatous optic disk (neural rim thinning or notching, saucerization, thin nasal rim, or total cupping) and/or glaucoma VF changes, in the presence of an IOP ⩾ 22 mmHg without medication, and a gonioscopy finding of a wide and open anterior chamber angle. Subjects were classified as having XFG if they had typical glaucomatous optic disk and/or glaucoma VF changes in the presence of an IOP ⩾ 22 mmHg without medication, with the presence of pseudoexfoliation on the edge of pupil and/or the anterior lens capsule after mydriasis by biomicroscopic evaluation in either or both of the eyes. XFS diagnosis was established by visualization of XFM on the pupillary margin and/or on the anterior lens surface after pupillary dilation, having an IOP < 22 mmHg, in the absence of glaucomatous optic nerve damage and VF changes. The patient was classified as having XFS if XFM was present in either or both of the eyes. The classic pattern of XFM on the anterior lens surface consists of three distinct zones that become visible when the pupil is fully dilated, comprising a central disk, an intermediate clear zone created by the iris rubbing pseudo exfoliation material from the lens surface during its physiologic excursions, and a granular peripheral zone. 3 Presence of XFM on the cornea manifesting as scattered flakes of XFM on the endothelial surface of the cornea and pigment deposition usually causes a diffuse, non-specific pigmentation of the central endothelium of the cornea. Iris changes mean the clinically evident peripupillary atrophy and characteristic “moth-eaten” transillumination defects in the peripupillary region. NC patients had no evidence of XFS or glaucoma based on clinical examination.
Exclusion criteria were as follows: (1) use of anti-glaucoma medications; (2) use of topical/systemic steroids within the last 6 months; (3) previous intraocular surgery; and (4) history of ocular trauma, uveitis, corneal scars, lens-induced glaucoma, and any other ocular pathology that could have led to secondary glaucoma.
All subjects that met the study inclusion criteria received a detailed explanation of the study purpose and the nature of their involvement, and those that agreed to take part in the investigation signed an informed consent form, in accordance with the principles embodied in the Declaration of Helsinki. The study was reviewed and approved by the Ethics Committee of the Faculty of Medicine, University of Belgrade.
Questionnaire
Participants’ demographic and comorbidity characteristics were obtained via interviews and by reviewing medical documentation. The ophthalmologist (V.D.M.) performed a face-to-face interview with each patient, using a structured questionnaire for the assessment of demographic data and medical history. The questionnaire employed in this study was developed by an epidemiologist (A.D.G.) with a particular interest in eye diseases, in collaboration with the ophthalmologist (V.D.M.). Demographic data included age and gender, educational attainment, marital status, and family history of glaucoma (FHG). Marital status was treated as a dichotomous variable and was coded as “single” (not married, divorced, widow/er) and “with partner” (married, in an extramarital relationship). Educational attainment was also a dichotomous variable, allowing those with secondary education and lower to be segregated from patients that completed tertiary education. Presence of systemic diseases, such as diabetes mellitus and diabetes treatment, hypertension, history of myocardial stroke, history of coronary artery bypass or vascular surgery, history of abdominal aortic aneurysm, arrhythmia, history of acute cerebrovascular disease, Alzheimer’s disease, and hearing loss, was identified through a review of medical records and during individual interviews.
Eye examinations
Ocular examination in all patients was performed by one ophthalmologist (V.D.M.) and included visual acuity (VA), slit-lamp biomicroscopy, gonioscopy (using Goldmann two-mirror indirect gonioscope), IOP measurement (using Goldmann applanation tonometry), and dilated fundus examination (using Volk Superfield +90 D lens). The mean IOP based on three readings in each eye was adopted as the pressure for that eye. A VF test was performed using the Threshold C 24-2 Swedish Interactive Testing Algorithm (SITA) standard program with Humphrey Visual Field Analyzer II (Carl Zeiss, Jena, Germany). Central corneal thickness (CCT) values were measured by trained ophthalmic technicians using an ultrasonic pachymeter (OcuScan® RxP Ophthalmic Ultrasound system; Alcon laboratories, Fort Worth, TX). The pachymetry value recorded for each eye was the average of three measurements taken per eye. Corneal curvature (CC) and refractive error were measured with an autokeratorefractometer (Topcon KR-7000, Topcon Medical Systems, Oakland, USA). CC measurements were expressed as keratometry values (K). Refractive error was calculated as spherical equivalent (SE) expressed in diopters, as the sum of the sphere and half the refractive astigmatism. VA was measured by Snellen chart at 6 m distance and recorded as the logarithm of the minimum angle of resolution (logMAR). If the patients were unable to read any letters displayed on the chart, their ability to count fingers was used as the VA. The next lower level of vision would be indicated by the ability to perceive light (denoted as “LP” or “light perception”). Complete blindness was diagnosed if no light perception (“NLP”) was determined by clinical examination.
If the anterior chamber angle was open, participants had their pupils dilated by administering dilation drops containing 5% phenylephrine and 1% tropicamide. Prior to pupil dilation, a detailed high-magnification slit-lamp assessment of the pupil margin was carried out. After pupil dilation, the anterior lens surface in each eye was scanned, looking specifically for signs of XFM. If the angle was potentially occludable, the lens and the fundus evaluations were performed without dilation, and the participants were referred for a laser peripheral iridotomy. In these cases, dilated lens and fundus examinations were performed upon iridotomy completion. An angle was defined as narrow using the Shaffer gonioscopic grading system. It was considered occludable if the pigmented trabecular meshwork was not visible across an angle > 180° in static gonioscopy. Chamber angle pigmentation was detected gonioscopically and the degree of pigmentation in the iridocorneal angle was defined using the Scheie grading system. The iris color was dichotomized into dark (brown/hazelnut, dark brown, dark green) and light (blue, green, tan-brown).
Indices of glaucoma severity were expressed numerically as the cup-to-disk ratio (C/D), allowing the vertical and mean C/D to be reported, along with the staging of visual filed defects using Hodapp classification, and separately VF mean deviation (MD) and pattern standard deviation (PSD). It should be noted that several patients could not partake in the VF test due to poor VA.
NCs and patients in the XFS group had bilaterally phakic eyes. In addition, cataract type was divided into nuclear, cortical, and posterior subcapsular opacities, and other cataracts (mature, non-mature).
Clinical characteristics for evaluating the inclusion criteria were IOP values, gonioscopy finding (width of the chamber angle and the degree of pigmentation in the iridocorneal angle), presence of pseudoexfoliation on the edge of pupil and/or the anterior lens capsule, MD, PSD and Hodapp classification, vertical cup-to-disk ratio (vC/D) and mean cup-to-disk ratio (mC/D), and cataract presence. Thus, the investigated clinical characteristics included the aforementioned inclusion criteria, along with VA, CCT values, refractive error calculated as SE, keratometry values, iris color, cataract stage, presence of XFM on cornea and iris, presence of phacodonesis, and presence of pterygium. It should be noted that subjects included in this study will be analyzed first, before considering the sample comprising the eyes. Then the eyes will be analyzed, independently considered.
Statistical analysis
Standard descriptive statistics were used (arithmetic mean with standard deviation (SD) for normally distributed numerical data, or median with range otherwise), while providing absolute and relative numbers for categorical data. Whether the data were distributed normally was established via mathematical (coefficient of variation, skewness and kurtosis, Kolmogorov–Smirnov and Shapiro–Wilk tests) and graphical (histogram, normal Q-Q diagram, detrended Q-Q diagram, and box-plot) methods. As at least two of the mathematical as well as graphical tests met the normal distribution criteria, we deemed this sufficient evidence for establishing that the data were normally distributed. The differences in numerical variables among the four groups were assessed via one-way analysis of variance (ANOVA) combined with Tukey’s post hoc test, or via the Kruskal–Wallis and Mann–Whitney U tests. For testing the difference in frequencies between the study groups, chi-square or Fisher’s exact test was performed. In order to identify the factors associated with XFG, multivariate logistic regression was performed. Models were constructed for the following inter-group comparisons: XFG versus POAG, XFG versus NC, and XFG versus XFS. The enter method of selecting variables for the model was used, and variance inflation factor (VIF) collinearity was examined (all variables with VIF > 5 were eliminated from the primary model). Correlation between parameters was tested by examining the Pearson correlation coefficients. Results yielded by all statistical methods were significant at p ⩽ 0.05. Statistical analysis was performed in IBM SPSS version 21.0 (IBM, Armonk, New York, USA).
Results
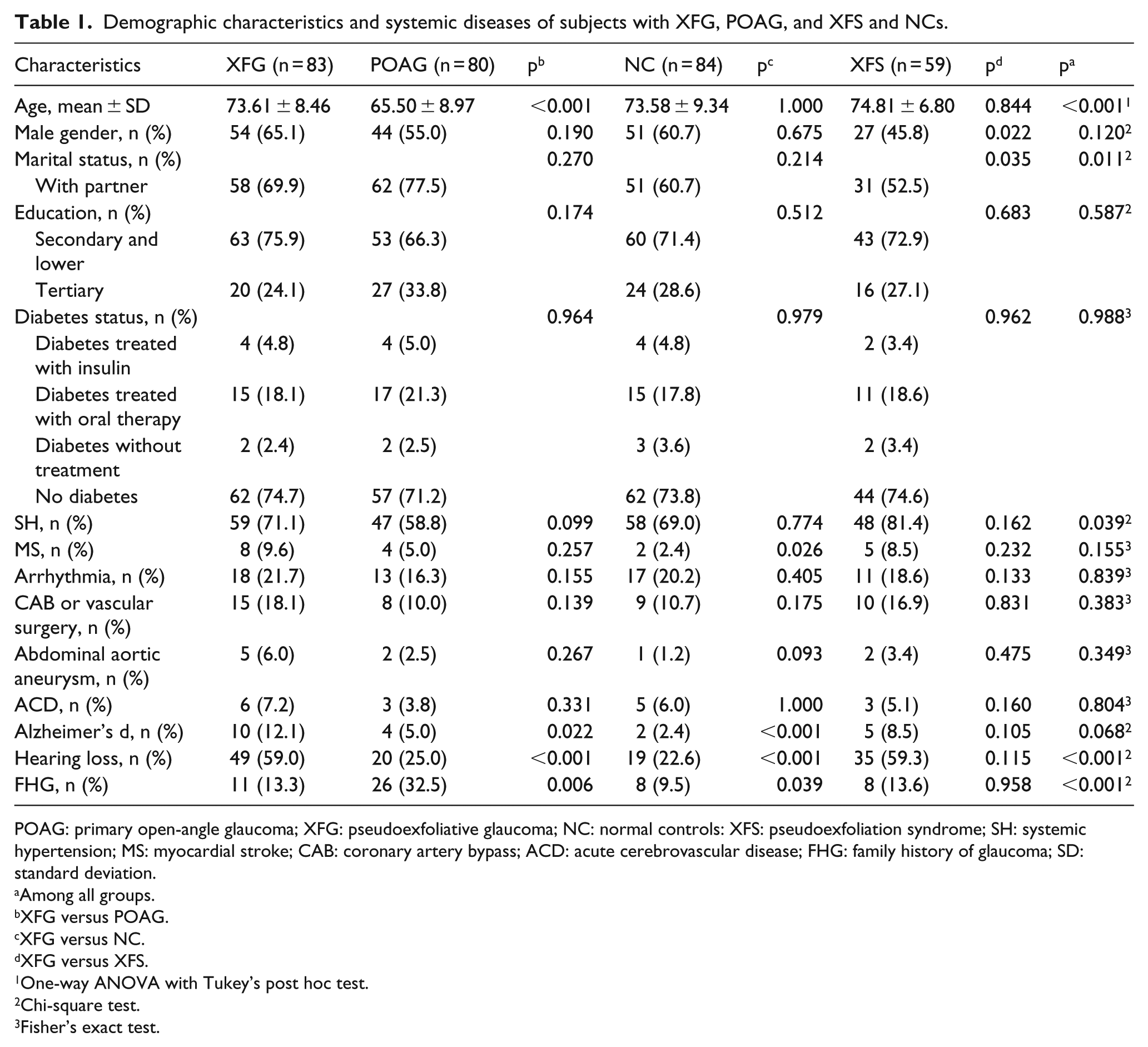
The study sample comprised 306 subjects, of which 83 and 80 were newly diagnosed as having XFG and POAG, respectively, while 59 patients had XFS and 84 individuals served as NCs. The patients’ demographic characteristics and the prevalence of systemic diseases in the sample are shown in Table 1. The mean age in the XFG, POAG, XFS, and NC groups was 73.61 ± 8.46, 65.50 ± 8.97, 74.81 ± 6.80, and 73.58 ± 9.34 years, respectively, whereby the age difference was statistically significant for XFG versus POAG (p < 0.001). In the XFG group, males were slightly younger than females (73.37 ± 9.3 vs 74.07 ± 6.64). With regard to systemic diseases, there were not statistically significant differences between the groups, except the history of myocardial stroke and Alzheimer’s disease. As shown in Table 1, a greater percentage of patients in the XFG group reported a history of myocardial stroke compared with the other groups, and this difference was statistically significant for XFG versus NC only (9.6% vs 2.4%, p = 0.026). Alzheimer’s disease was statistically significantly more frequent among XFG patients (12.1%) compared with those in the POAG (5.0%, p = 0.022) and the NC (2.4%, p < 0.001) groups, whereas the differences between the XFG and XFS (8.5%, p = 0.105) groups were not statistically significant. Similarly, a greater prevalence of hearing loss was noted between XFG and XFS patients relative to non-XFM individuals and the difference was statistically significant.
Demographic characteristics and systemic diseases of subjects with XFG, POAG, and XFS and NCs.
POAG: primary open-angle glaucoma; XFG: pseudoexfoliative glaucoma; NC: normal controls: XFS: pseudoexfoliation syndrome; SH: systemic hypertension; MS: myocardial stroke; CAB: coronary artery bypass; ACD: acute cerebrovascular disease; FHG: family history of glaucoma; SD: standard deviation.
Among all groups.
XFG versus POAG.
XFG versus NC.
XFG versus XFS.
One-way ANOVA with Tukey’s post hoc test.
Chi-square test.
Fisher’s exact test.
Moreover, compared with the POAG patients, a greater percentage of XFG patients reported a negative FHG compared with POAG patients (86.7% vs 67.5%, p = 0.006). However, they more frequently presented a positive FHG relative to the NC group (13.3% vs 9.5%, p = 0.039).
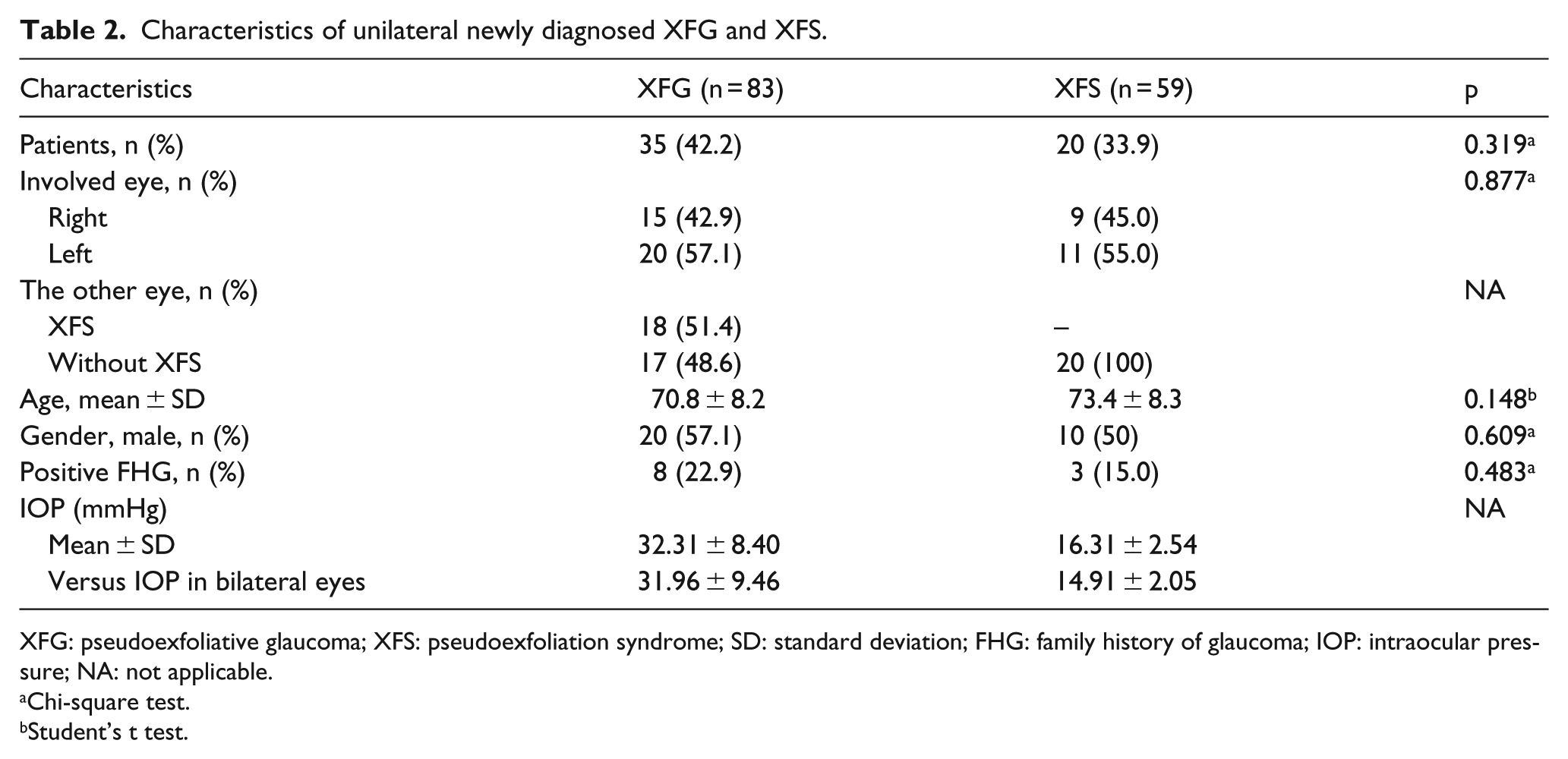
The XFG group included 35 patients (42.2%) with unilateral XFG, 15 (42.9%) of whom had XFG in the right eye and 20 (57.1%) in the left eye. In addition, 18 (21.7%) of the study sample had XFS on the unaffected eye and 17 (20.5%) were unaffected by XFS. Characteristics of unilateral XFG and XFS are shown in Table 2. Analyses of the demographic characteristics revealed that patients with unilateral XFG were younger than bilaterally affected patients (70.8 ± 8.2 vs 75.6 ± 8.1, p = 0.040). They were predominantly male (57.1%) and were more likely to report FHG, at 8 (22.9%) versus 3 (6.25%) (p = 0.028). In the XFS group, there were 20 (33.9%) subjects with unilateral XFS, 9 (45.0%) of whom were diagnosed with XFS in the right eye and 11 (55.0%) in the left eye. The subjects with unilateral XFS were also younger as compared to bilaterally affected subjects (73.4 ± 8.3 vs 75.5 ± 5.9). Three (15%) individuals in this group had a positive FHG (p = 0.817) and the gender distribution was equal. Among all the XFM eyes (irrespective of whether they were in the XFG or XFS group), XFM was diagnosed in 55 (38.7%) participants, while 24 (43.6%) individuals had XFM in the right eye and 31 (56.4%) in the left eye.
Characteristics of unilateral newly diagnosed XFG and XFS.
XFG: pseudoexfoliative glaucoma; XFS: pseudoexfoliation syndrome; SD: standard deviation; FHG: family history of glaucoma; IOP: intraocular pressure; NA: not applicable.
Chi-square test.
Student’s t test.
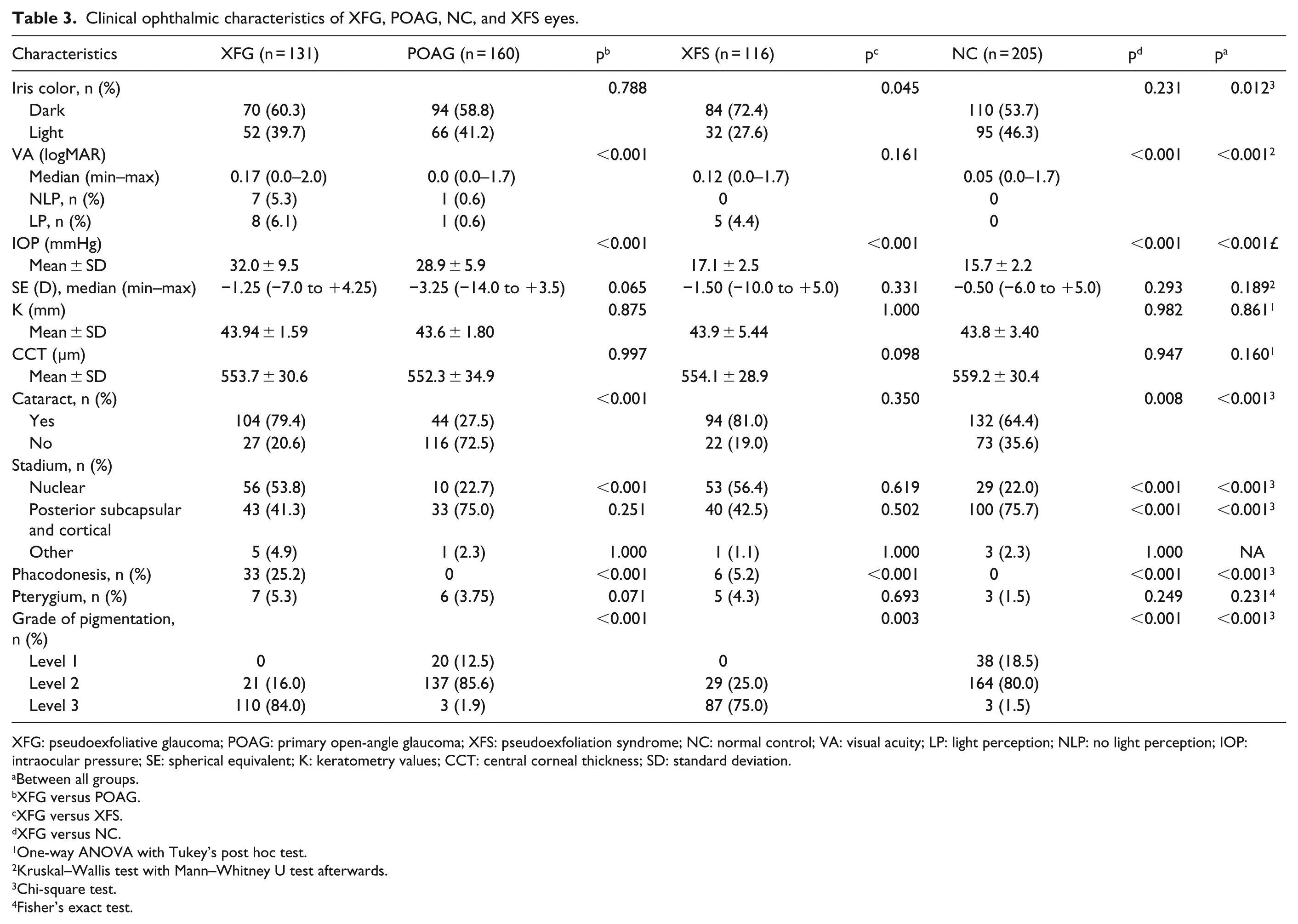
The clinical ophthalmic characteristics of the eyes of patients in whom XFG and POAG were newly diagnosed, as well as those of the NC and XFS groups, are shown in Table 3. The examination was performed on 612 eyes, whereby 131 (21.4%) eyes pertained to newly diagnosed XFG, 160 (26.1%) to newly diagnosed POAG, and 116 (19.0%) to XFS eyes, while in the remaining 205 (33.5%) eyes XFS or any type of glaucoma was absent, which thus served as NCs.
Clinical ophthalmic characteristics of XFG, POAG, NC, and XFS eyes.
XFG: pseudoexfoliative glaucoma; POAG: primary open-angle glaucoma; XFS: pseudoexfoliation syndrome; NC: normal control; VA: visual acuity; LP: light perception; NLP: no light perception; IOP: intraocular pressure; SE: spherical equivalent; K: keratometry values; CCT: central corneal thickness; SD: standard deviation.
Between all groups.
XFG versus POAG.
XFG versus XFS.
XFG versus NC.
One-way ANOVA with Tukey’s post hoc test.
Kruskal–Wallis test with Mann–Whitney U test afterwards.
Chi-square test.
Fisher’s exact test.
The IOP in the eyes affected by XFG was higher than that in the POAG eyes. We found statistically significant differences in both peak IOP (74.0 vs 56.0 mmHg) and mean IOP (32.0 ± 9.5 vs 28.8 ± 5.9 mmHg) (p < 0.001). In 16.8% and 4.4% of the eyes affected by XFG and POAG, respectively, the IOP exceeded 40 mmHg. The mean IOP in unilaterally affected XFG patients was slightly higher than that in those in whom bilateral XFG was diagnosed (32.31 ± 8.40 mmHg vs 31.96 ± 9.46 mmHg, p = 0.145) as well as relative to the IOP in the XFS group (16.31 ± 2.54 vs 14.91 ± 2.05, p = 0.035), as shown in Table 2.
Patients in all the four groups were predominantly myopic, with only the difference between the XFG and POAG groups approaching borderline statistical significance.
Cataract was more frequent in the eyes affected by XFG relative to the POAG eyes (79.4% vs 27.5%, p < 0.001) and NC (64.4%, p = 0.008). On the other hand, the difference between XFG and XFS eyes was not statistically significant (81.0%, p = 0.350). Moreover, phacodonesis was more common in the XFG group than in the other three groups (p < 0.001).
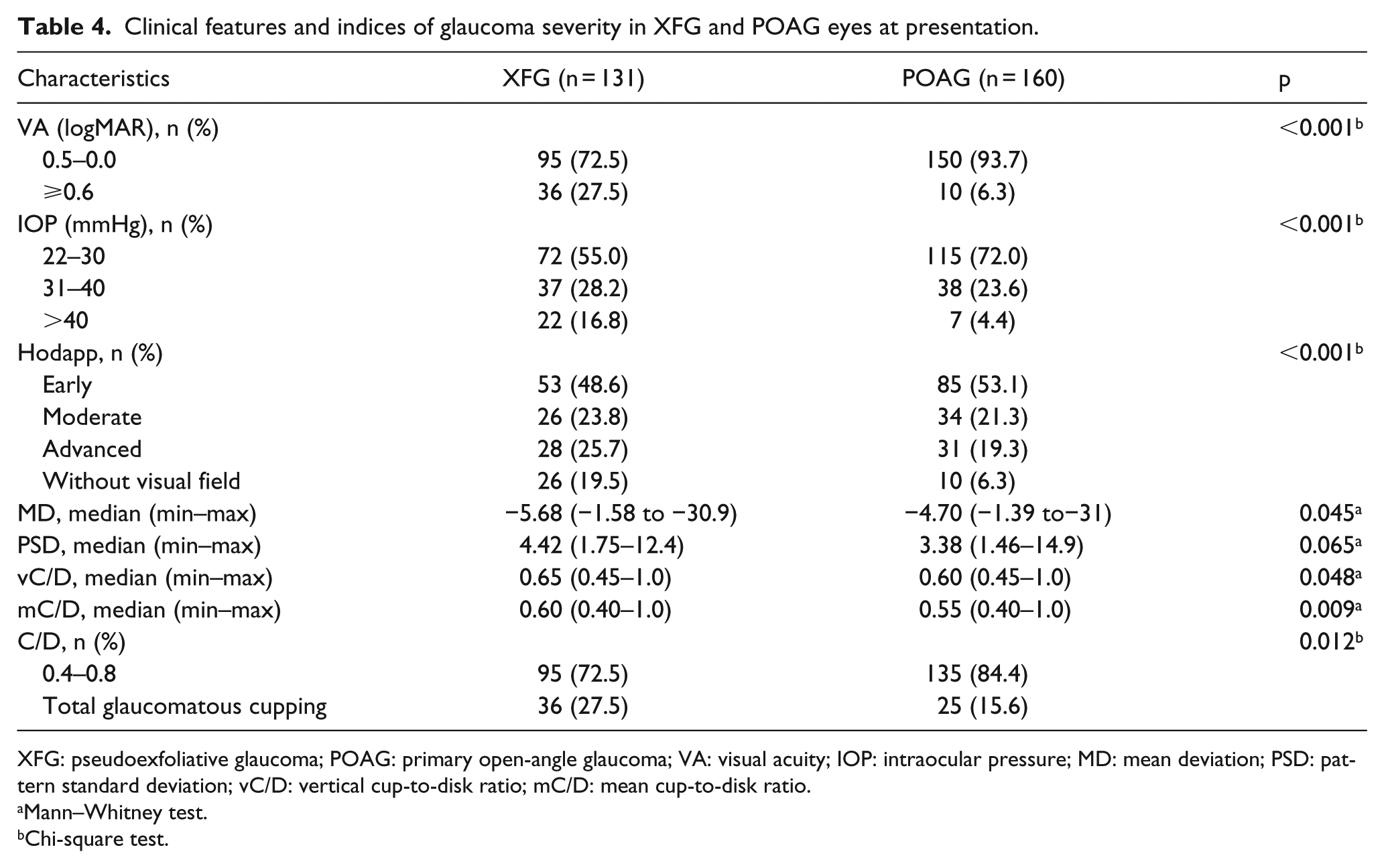
Indices of glaucoma severity pertaining to the newly diagnosed XFG and POAG eyes are shown in Table 4. A greater VF loss was noted in eyes affected by XFG relative to the POAG eyes (p < 0.001). In the XFG group, MD was greater in males compared to females (−5.93 (−1.60 to −30.9) vs −4.79 (−1.58 to −30.24)). A statistically significantly smaller vC/D and mC/D was recorded in the POAG group.
Clinical features and indices of glaucoma severity in XFG and POAG eyes at presentation.
XFG: pseudoexfoliative glaucoma; POAG: primary open-angle glaucoma; VA: visual acuity; IOP: intraocular pressure; MD: mean deviation; PSD: pattern standard deviation; vC/D: vertical cup-to-disk ratio; mC/D: mean cup-to-disk ratio.
Mann–Whitney test.
Chi-square test.
In the XFG group, while patient’s age was negatively correlated with MD (r = −0.144, p < 0.064), no correlation with PSD (r = −0.116, p = 0.233) and C/D (r = −0.074, p = 0.406) was noted.
Clinical features between newly diagnosed XFG and XFS eyes are shown in Table 5. In all eyes affected by XFG and XFS, more pronounced pigmentary changes were observed relative to the POAG and NC groups (p < 0.001). The pigmentation angle also differed between the XFG and XFS groups, whereby XFG eyes were denser than the XFS eyes. In the unilateral cases of XFG, the involved eye was denser in 94.2% of the cases, while it was denser in 85% of the eyes affected by XFS.
Clinical features between newly diagnosed XFG and XFS eyes.
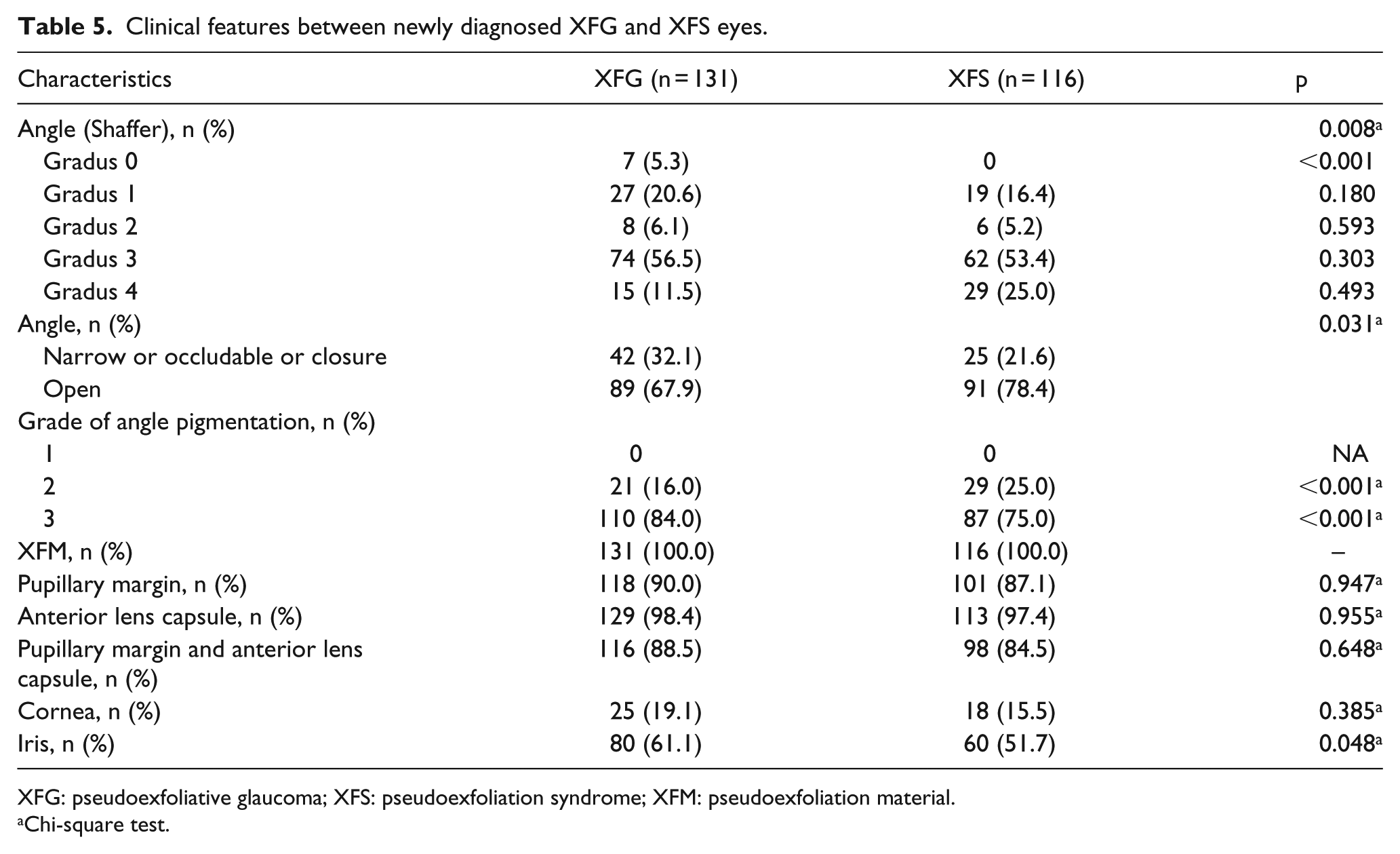
XFG: pseudoexfoliative glaucoma; XFS: pseudoexfoliation syndrome; XFM: pseudoexfoliation material.
Chi-square test.
Factors associated with XFG that distinguish it from POAG, NC, and XFS according to multivariate logistic regression analysis are shown in Table 6.
Factors associated with XFG versus POAG, NC, and XFS according to multivariate logistic regression analysis.
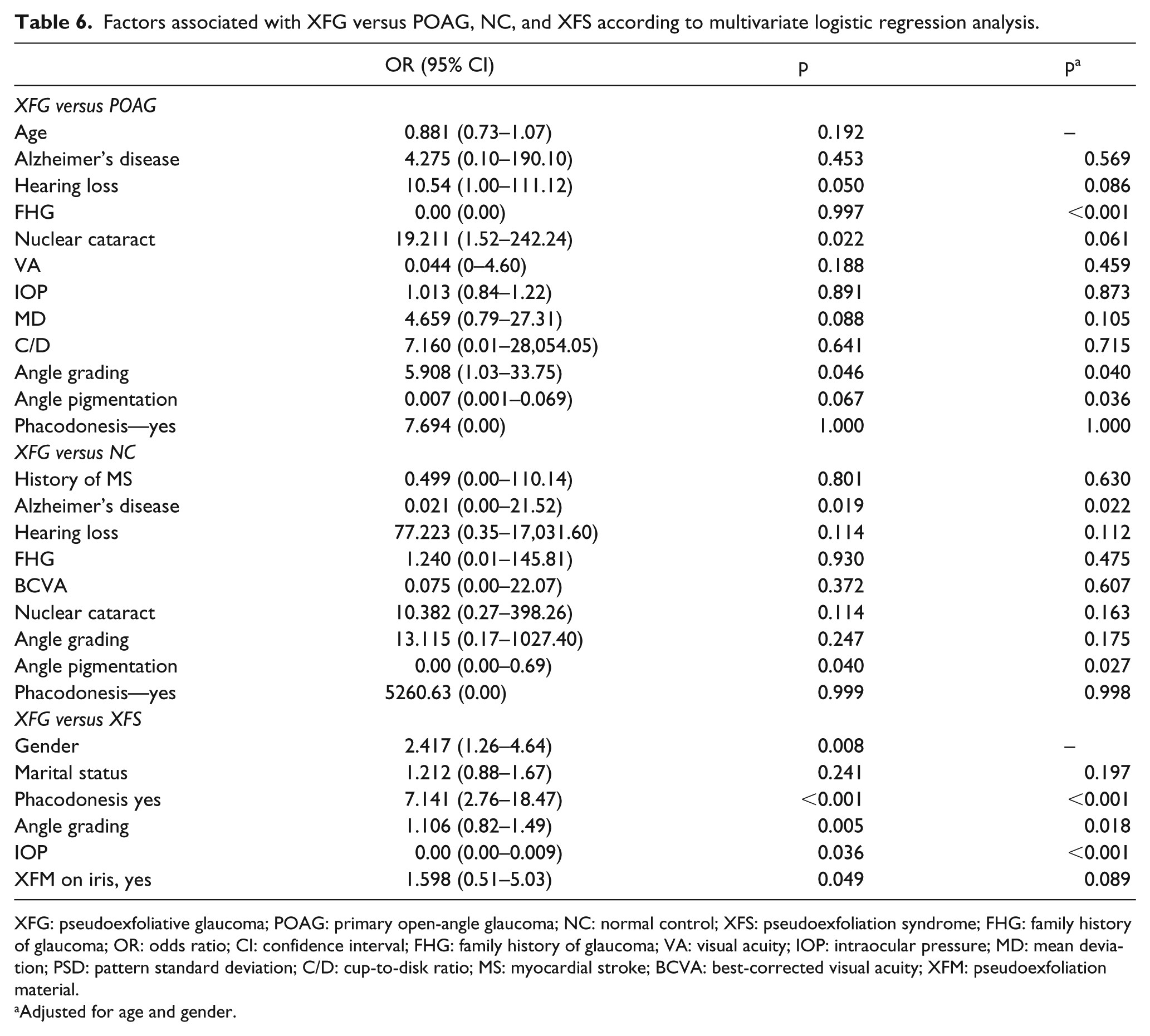
XFG: pseudoexfoliative glaucoma; POAG: primary open-angle glaucoma; NC: normal control; XFS: pseudoexfoliation syndrome; FHG: family history of glaucoma; OR: odds ratio; CI: confidence interval; FHG: family history of glaucoma; VA: visual acuity; IOP: intraocular pressure; MD: mean deviation; PSD: pattern standard deviation; C/D: cup-to-disk ratio; MS: myocardial stroke; BCVA: best-corrected visual acuity; XFM: pseudoexfoliation material.
Adjusted for age and gender.
Discussion
Although the XFG characteristics have been extensively studied, to the best of our knowledge, there is a paucity of studies focusing specifically on the newly diagnosed or undiagnosed XFG.12,15–17 There are only few published reports pertaining to a direct comparison between newly diagnosed XFG and POAG.16–19
Konstas et al. 12 evaluated both the presentation and the progression characteristics of XFG in four relatively distinct population groups in Europe, namely, Greece, Spain, Russia, and Hungary. The IOP in XFG eyes obtained in this study is similar to that reported by Konstas et al. for the Greek (32.3 ± 7.7 mmHg) and Hungarian (31.8 ± 9.6 mmHg) samples at baseline and is higher than that measured in Spain (29.1 ± 7.3 mmHg) and Russia (26.7 ± 3.2 mmHg). Compared with the POAG group, higher mean and peak IOP were measured for patients with XFG that took part in this study. Similar findings were recently reported by Topouzis et al. 15 and Konstas et al.18,20 The IOP in the XFS group was higher than that in the NC group. Similar findings were reported by Astrom et al. 21 and Arnarsson et al. 22
The findings yielded in this study revealed a significantly greater severity of optic nerve damage in newly diagnosed XFG compared to newly diagnosed POAG, as indicated by both vC/D and mC/D. Our newly diagnosed XFG patients also had significantly more advanced VF changes than those newly diagnosed with POAG. This difference probably reflects the detrimental effects of the higher IOP on the optic nerve. Indeed, it has recently been shown that the lamina cribrosa becomes more vulnerable in XFG due to elastosis.11,23 The vulnerability of the lamina cribrosa exacerbates optic nerve head damage induced by the unfavorable IOP profile in eyes affected by XFG. In their study, Konstas et al. 18 examined the clinical features in 24 newly diagnosed XFG patients and compared them with those in 22 newly diagnosed POAG patients. These authors failed to establish statistically significant differences in optic disk parameters at presentation between the two groups. However, the mean defect in patients with XFG was significantly worse than that in their POAG counterparts. Similarly, Tarkkanen and Kivelä 17 compared the characteristics at the time of diagnosis between 176 patients with XFG and 329 patients with POAG, and there were differences in the C/D ratios pertaining to POAG and XFG eyes and the visual field (VF) profiles were similar.
The VA findings yielded by our study indicate a more severe visual loss in newly diagnosed XFG cases relative to that noted in the POAG group. This observation is in agreement with the results reported by Tarkkanen and Kivelä 17 who observed slightly lower best-corrected visual acuity (BCVA) in XFG eyes relative to POAG eyes at the time of diagnosis. Conversely, in the study conducted by Musch et al., 16 the mean VA at baseline, as well as the Humphrey 24–2 visual field test findings and vC/D, was not significantly different between newly diagnosed XFG and POAG eyes. These discrepancies in the reported results could be due to sample differences, as a significantly higher percentage of cataracts in the XFG relative to the POAG group (79.4% vs 27.5%) was noted in this study, which could have contributed to the greater incidence of poor VA. Still, it should be emphasized that, in this investigation, LP and NLP were noted in 11.4% eyes with XFG compared to only 1.2% in the eyes affected by POAG, which was probably the result of glaucoma damage rather than a cataract. In their recently published study, Topouzis et al. 19 reported that their XFG patients also had lower VA and more advanced VF changes, while no statistically significant differences were noted between the newly diagnosed XFG and POAG groups with respect to other clinical characteristics, including vC/D and Advanced Glaucoma Intervention Study VF score.
XFG differs from POAG by being asymmetric in a greater number of cases. A review of pertinent literature comparing the frequency of unilateral versus bilateral involvement suggests the lack of consensus regarding their relative prevalence in different populations. For example, European reviewers tend to report a more frequent unilateral involvement of XFS, with ratios almost as high as 3:1, 10 while American authors report a predominantly unilateral involvement. 3 In this study, 42.2% of the patients in the newly diagnosed XFG group had unilateral XFG, whereby the left eye was more frequently affected. In fact, unilateral pseudoexfoliation was recorded in 38.7% of all XFM cases (XFG and XFS patients). Nevertheless, clinically unilateral involvement is often the harbinger of potential development of XFS and XFG in the fellow eye and clinically “uninvolved” eye often demonstrates the morphological presence of XFM, which can be ultrastructurally detected in both eyes, as well as in other organ systems.3,10,12 Clinically unilateral involvement is often a precursor to bilateral involvement. In a prospective follow-up study conducted by Puska, 24 however, clinically unilateral XFS advanced to bilateral involvement in only 38% of patients over the course of 10 years. When glaucoma develops in patients with bilateral XFS, there is a tendency for it to occur in both eyes simultaneously, or within a limited period of time.3,25 However, in clinically unilateral cases, trabecular pigment is almost always more dense in the involved eye, 3 as confirmed by our findings.
In this study, patients with XFG were younger than the Hungarian and Spanish cohorts that took part in the study conducted by Konstas et al., 12 but were older than the patients from Greece and Russia. Compared with the POAG patients, they were statistically significantly older, as the mean age of subjects with XFG was 8.11 years greater than that of the POAG patients, but they were of similar age to the XFS participants. It is noteworthy that 66% of patients with POAG developed glaucoma before the age of 70, while glaucoma was diagnosed in 72% of patients with XFG after the age of 70. Patients in Tarkkanen and Kivelä’s 17 study were of similar age (74 ± 8.6 years) to those in the XFG group of this study, but were older than those newly diagnosed with POAG (68 ± 11.4 years). However, in the study conducted by Musch et al., 16 newly diagnosed XFG subjects were younger than our sample (65.1 years) and were 7 years older on average than those with POAG (58.0 years).
Both the XFG and POAG groups had a greater percentage of men, at 65.1% and 55.0%, respectively. Conversely, patients assigned to the XFS group were predominantly female (54.2%), which is in line with most of the published reports, indicating that women tend to develop XFS without glaucoma more often than men do. 26 Nonetheless, a greater prevalence in men was reported in some cases. 27 According to the multivariate model developed as a part of this study, male gender is associated with XFG compared to the XFS group. On the other hand, if XFS is more common in women, having an equal number of men and women affected by glaucoma could signify a greater predilection for men to develop glaucoma.
Although XFG is considered the most common form of secondary open-angle glaucoma worldwide, 5 in this study, 32.1% of eyes in the XFG group had a narrow, occludable or closure angle, with open angle detected in the remaining 67.9% of eyes. In the XFS group, there was a statistically significantly smaller percentage (21.6%) of eyes with narrow or occludable angle than in the XFG group. In the multivariate age- and gender-adjusted analyses, narrow or occludable angle was more frequently detected in XFG eyes relative to those affected by XFS. When the sample was stratified by iris color, the findings revealed a greater prevalence of darker-colored irises in the XFM group than in non-XFM eyes. Conversely, in the XFG group, lighter-colored irises were statistically significantly more frequent than in the XFS but iris color did not emerge as a risk factor. Kang et al. 28 reached the same conclusion, based on the absence of the association between iris color and XFG/XFS incidence. It should be noted, however, that no consensus presently exists in the pertinent literature regarding this relationship. For example, Arnarsson et al. 22 found that having more pigmented irises was associated with an increased prevalence of XFS.
As already mentioned, in this study, cataract was more prevalent in the XFG group relative to POAG and NC, but the difference between with the XFG and XFS groups was not statistically significant. Nuclear cataract was the most common stage in XFG and XFS cases. A statistically significant difference in the frequency of cataract between XFG and POAG eyes was observed (79.4% vs 27.5%). However, it should be noted that XFG patients were older than the POAG patients. According to the multivariate model, XFG was associated with a higher frequency of nuclear cataract compared to the POAG group. In comparison with age- and sex-matched NCs, the XFG patients were more likely to develop cataract (79.4% vs 64.4%), in particular nuclear cataract (53.8 vs 22.0). Our finding pertaining to the higher prevalence of nuclear cataract in the XFM population is in accordance with the results yielded by previous studies. 29 The reason could be higher levels of oxidative stress markers. Moreover, a decrease in the quantity of antioxidant protection molecules has been shown in the anterior segment of eyes affected by XFS or XFG.5,11 Phacodonesis due to weakness of the zonules holding the lens is common in eyes with XFM, with varying reported incidence. 3 In this study, phacodonesis was statistically significantly most prevalent in the XFG group, while it was not present in POAG and NC eyes. Moreover, phacodonesis was statistically significantly more frequent in XFG than in XFS eyes (25.2% vs 5.2%). In the multivariate model, phacodonesis was associated with XFG eyes more strongly than with XFS.
A variable degree of pigment accumulation is detectable gonioscopically in almost all eyes affected by pseudoexfoliation. In this study, it was more pronounced in the XFG and XFS patients relative to those unaffected by XFM. On the other hand, eyes with XFG had greater pigmentation than eyes with XFS. Unaffected eyes of patients with unilateral newly diagnosed XFG and XFS contained less pigmentation. It may suggest that the larger quantities of both chamber angle pigmentation and visible XFM may be a more important risk factor for XFG. Similar conclusion was reached by Astrom et al. 21
The association between XFS and glaucoma is well recognized.4,19 Glaucoma may develop simultaneously with the appearance of clinical signs of pseudoexfoliation, as well as shortly after, or after a considerable length of time. It may even precede clinically detectable XFS.10,25 In this study, the presence of XFM on the anterior lens capsule, pupillary margin, and cornea was similar in the XFG and XFS groups, while iris changes were statistically more frequent in the eyes affected by XFG (61.1% vs 51.7%, p = 0.048). Iris changes are an early and well-recognized clinical feature of XFS and, in most cases, they are associated with poor or absent pupillary dilation as a result of atrophic and/or fibrotic changes in the iris sphincter muscle. In the multivariate analyses, iris changes were associated with XFG versus XFS. XFM deposits on the iris sphincter and pupillary margin can be found in 32%–94% of patients. 3 Narrow, occludable, or closure angle was more frequent in the XFG than in the XFS group in this study.
XFS is a systemic disorder and XFM material has been found not only in the eye, but also in several other tissues and organs. 3 The association of XFS/XFG with cardiovascular or cerebrovascular diseases has been extensively investigated, albeit with inconclusive results. While some authors reported associations between XFS/XFG and vascular diseases,5,7 others failed to link XFS/XFG with systemic hypertension, cardiovascular disease, or diabetes mellitus. 30 In this study, only Alzheimer’s disease was related to newly diagnosed XFG. Specifically, Alzheimer’s disease was statistically significantly more frequent in XFG patients compared with the POAG and NC groups, but no statistically significant differences between the XFG and XFS groups were noted. Many authors found a significant increase in the prevalence of XFS among Alzheimer’s patients. 8 However, Ekström and Kilander 31 recently reported that XFM is not a predictor of Alzheimer’s disease.
In our study, hearing loss was statistically significantly more frequent among XFG and XFS patients than in non-XFM individuals. This is in line with available evidence, indicating that XFS/XFG patients tend to experience a greater hearing loss. 9
When interpreting the results yielded by our investigation, it is important to note some study limitations. Specifically, as the study aim was to determine the time of the XFG and POAG occurrence, we did not select POAG patients that were age and sex matched to the XFG cohort. The existence of systemic diseases and hearing loss was established through interviews that were guided by the questionnaire, as well as via an overview of medical documentation. Thus, it needs to be emphasized that neither systemic diseases nor hearing loss were clinically determined in our study sample. It is also noteworthy that we might have failed to detect some subclinical cases of XFS, which would be diagnosable by histological methods only.
In conclusion, XFG exhibits clinical features that distinguish it from POAG at the time of diagnosis. In most cases, significant optic nerve head and VF damage is already present at the time of XFG diagnosis. On the other hand, glaucomatous damage is more severe in patients with newly diagnosed untreated XFG than in those with newly diagnosed untreated POAG. The time of manifestation and/or the discovery of XFG was on average 8 years later in XFG than in POAG eyes. According to our study findings, besides the presence of XFM on the anterior lens surface and/or pupillary margin, higher IOP, narrow or occludable angle, increased trabecular pigmentation, phacodonesis, and poorer pupillary dilatation were the factors associated with XFG. However, no association between newly diagnosed XFG and any of the examined systemic diseases, except Alzheimer’s disease, was established.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.