
Abstract
Background:
Evaluate subclinical myocardial injury associated with intravitreal anti-vascular endothelial growth factor therapy by measuring serum high-sensitivity cardiac troponin T.
Methods:
This is a prospective pilot comparative study conducted at American University of Beirut Medical Center, Beirut, Lebanon. In total, 40 consecutive patients were randomized to receive either intravitreal bevacizumab or ranibizumab. Patients received three consecutive monthly injections of the assigned drug, then continued treatment as needed. Systemic concentrations of high-sensitivity cardiac troponin T and vascular endothelial growth factor were obtained at baseline, week 9, and week 24. Primary endpoint measure was change in high-sensitivity cardiac troponin T levels compared to baseline. Secondary endpoint measure was change in systemic vascular endothelial growth factor levels.
Results:
There was no significant difference in high-sensitivity cardiac troponin T levels over time (p = 0.227) within each treatment group and no significant difference between treatments at any time point (p = 0.276). There was a significant decrease in plasma vascular endothelial growth factor levels at week 9 (p = 0.001) and week 24 (p < 0.001) compared to baseline. In the ranibizumab group, vascular endothelial growth factor levels were not significantly different at weeks 9 and 24 compared to baseline (p = 0.708 and p = 0.117, respectively). There was a significant association between the number of bevacizumab injections from weeks 8 to 24 and the decrease in vascular endothelial growth factor levels at week 24 (R = −0.67, p = 0.032). This correlation was not observed in the ranibizumab group (R = −0.341, p = 0.141).
Conclusion:
Repeated intravitreal bevacizumab or ranibizumab did not influence serum high-sensitivity cardiac troponin levels. Intravitreal bevacizumab but not ranibizumab lowered free-systemic vascular endothelial growth factor levels, which was observed in this study to be inversely related to the number of bevacizumab injections.
Introduction
Neovascular age-related macular degeneration (AMD), diabetic macular edema (DME), and retinal vein occlusion (RVO) are major causes of irreversible vision loss.1–3 Vascular endothelial growth factor (VEGF) plays an important role in the pathogenesis of these three entities, 4 and intravitreal anti-VEGF therapy is now the standard-of-care treatment.5–7 Bevacizumab, ranibizumab, and aflibercept are the anti-VEGF agents currently used for intravitreal administration.
VEGF is involved in a wide variety of physiologic processes, and VEGF inhibition might have serious systemic consequences. 8 Intravenous bevacizumab in patients with cancer was associated with arteriothrombotic events, venous thrombotic events, gastrointestinal perforation and hemorrhage, wound-healing complications, and hypertension.9,10 All three anti-VEGF agents used for intravitreal treatment can enter the systemic circulation after intravitreal administration, and even these low systemic levels appear sufficient to suppress circulating systemic VEGF.11–14 However, it is not clear if this can cause systemic adverse events.5,14
The current literature does not confirm a direct relationship between intravitreal anti-VEGF therapy and cardiac ischemic events.15,16 Usually, these events are detected when there are overt clinical manifestations. However, subclinical myocardial injury may be a concern in the context of systemic VEGF suppression with intravitreal anti-VEGF therapy. In this study, we tried to detect potential subclinical cardiac myocyte injury from repeated intravitreal injections of bevacizumab or ranibizumab by measuring systemic high-sensitivity cardiac troponin T (hs-cTnT), a highly sensitive and objective marker for myocardial damage.15–19 We correlated hs-cTnT levels with changes in free-systemic VEGF levels.
Materials and methods
Subjects
This prospective randomized pilot study was conducted at the American University of Beirut Medical Center in accordance with the Declaration of Helsinki and after obtaining approval of the institutional review board. In total, 40 patients were randomized in a 1:1 ratio to receive 1.25 mg of intravitreal bevacizumab (Avastin; Roche Diagnostics, Basel, Switzerland) or 0.50 mg of ranibizumab (Lucentis; Novartis Pharma AG, Basel, Switzerland). All patients provided informed consent after randomization.
Eligibility criteria included the following: (1) age more than 50 years; (2) previously untreated or did not receive intravitreal anti-VEGF agents for at least 6 months prior to enrollment; (3) active neovascular AMD, DME, or RVO in at least one eye with best-corrected visual acuity (BCVA) between 20/25 and 20/320; (4) presence of sub-retinal or intraretinal fluid on optical coherence tomography (OCT); (5) central retinal thickness (CRT) greater than 250 µm on OCT; and (6) ability to understand and sign a consent form. Patients were excluded if there was history of a thromboembolic event, myocardial infarction, or stroke within a period of 12 months prior to enrollment. Patients with stable coronary disease or prior revascularization without a myocardial infarction event were not excluded.
Baseline evaluation
Baseline evaluation included BCVA, slit-lamp examination of the anterior segment, dilated fundus examination, and OCT. Visual acuity testing was done according to the Early Treatment Diabetic Retinopathy Study (ETDRS) refraction protocol using ETDRS charts at 4 m with an illuminated cabinet (Precision Vision, La Salle, IL, USA); 1-mm CRT was determined by spectral-domain OCT (Cirrus; Carl Zeiss Meditec, Dublin, CA, USA) using a macular cube (512 × 128 lines). Fluid in the macula was defined as intraretinal cysts or sub-retinal fluid. A fluid-free macula was considered if there was absence of intraretinal or sub-retinal fluid on OCT. Fluorescein angiography was done at the discretion of the treating physician.
Intravitreal injection and follow-up
All patients received three mandatory consecutive monthly injections of the drug they were assigned. All injection procedures followed a standard injection protocol.20,21 Follow-up was carried out every 4 weeks. At each follow-up, BCVA, slit-lamp examination, dilated fundus examination, and OCT were performed. Retreatment after the third injection was based on the following criteria: (1) recurrence or presence of any fluid in the macula on OCT in a previously dry macula; (2) an increase in OCT CRT of at least 50 µm from the lowest recorded value, especially for eyes with persistent macular fluid; (3) visual acuity loss of at least five letters with OCT evidence of fluid in the macula; or (4) new macular hemorrhage in AMD cases.
Blood sample collection and analysis
Based on the work by Avery et al., 22 we assumed that elevation in hs-cTnT would manifest when free-systemic VEGF would be at the lowest level between days 1 and 7 after the third injection. Therefore, blood samples to test for hs-cTnT and free-systemic VEGF levels were obtained before the initial intravitreal injection and 1 week after the third injection (i.e. at 9 weeks). A third sample was obtained at week 24 to see how a sustained yet reduced treatment frequency would influence hs-cTnT and systemic VEGF levels.
Blood samples for free-systemic VEGF analysis were collected in ethylenediaminetetraacetic acid (EDTA) disodium tubes and for hs-cTnT in serum separator tubes. About 4 mL of blood was collected in each tube. Blood samples for hs-cTnT were allowed to coagulate in the tube for 30 min, then centrifuged at 4000 r/min for 5 min at room temperature. Hs-cTnT was assayed immediately using electrochemiluminescence immunoassay (Roche Diagnostics). Blood samples for VEGF were centrifuged at 1800 r/min for 30 min, and isolated plasma was labeled and stored at −80°C. Once enough samples were collected, plasma-free VEGF level was determined using Quantikine VEGF enzyme-linked immunosorbent assay (ELISA) kit (R&D Systems, Minneapolis, MN, USA). The kit was used as described by the manufacturer, and the procedure was performed in duplicates. Optical density was taken at 450 nm in ELISA reader (Bio-Rad, Hercules, CA, USA). VEGF analysis was done after all the samples were collected; hence, the treating physicians were unaware of the results until the conclusion of the study. The staff performing the analysis on the blood samples were all blinded to study information including the assigned drug to each patient and serum VEGF levels.
Sample size calculation
The primary objective of the study was to assess the effect of intravitreal anti-VEGF therapy on serum hs-cTnT levels. The standard deviation of normal hs-cTnT levels has been reported to be around 0.05 ng/mL. A clinically significant change in hs-cTnT levels would be between 0.04 and 0.05 ng/mL. Thus, we needed to recruit 20 patients in each group to have 80% power to detect a 0.045 difference in the troponin levels with an alpha level set at 0.05.
Statistical analyses
Patient demographics and clinical baseline characteristics were summarized using median ± interquartile range for continuous variables and frequency distribution for categorical data. Differences between the bevacizumab and ranibizumab groups were analyzed using the Mann–Whitney U test for continuous variables. The chi-square test or Fisher’s exact test (if expected cell counts fell below 5) was used for categorical variables. Baseline levels of hs-cTnT and VEGF were compared between the study groups using the Mann–Whitney U test. Repeated-measures analysis of variance (ANOVA) was used to compare hs-cTnT and VEGF levels over time (baseline, 9 weeks, and 24 weeks) within each group and between groups.
The number of injections from weeks 8 to 24 was compared between the two study arms using the Mann–Whitney U test. Spearman’s correlations were computed to assess the relation between the number of injections and hs-cTnT or VEGF levels. IBM-SPSS software (version 22.0, IBM, Armonk, NY, USA) was used for all analyses. The p value of 0.05 or less was considered significant.
Results
Patient characteristics
In total, 40 patients were enrolled in this study (20 in each treatment group). Median age of patients who received intravitreal bevacizumab was 76.5 ± 9.8 years (range = 56–88) compared to 71.0 ± 11.8 years (range = 57–86) in the ranibizumab group (p = 0.06). Seven women were enrolled into the ranibizumab group versus nine in the bevacizumab group (p = 0.75). Thirteen patients in the bevacizumab group and 18 in the ranibizumab group had prior history of diabetes mellitus, arterial hypertension, cardiac diseases, or hyperlipidemia (p = 0.13); this is illustrated in more detail in Table 1. Those patients with history of cardiac disease included coronary artery revascularization, stable coronary artery disease, and arrhythmias. None had cardiac failure or valvular disease. In the bevacizumab group, the most common reason for treatment was neovascular AMD (14 patients), then RVO (5 patients) and DME (1 patient). In the ranibizumab group, 10 patients needed treatment for neovascular AMD, 5 for DME, and 5 for RVO. This distribution was similar between both groups (p = 0.30).
Risk factor distribution among patients receiving intravitreal bevacizumab or ranibizumab.

Hs-cTnT levels
All individual hs-cTnT concentrations were in the normal range for all patients at baseline, 9 weeks, and 24 weeks. The median hs-cTnT level at baseline was 0.0100 ± 0.0102 ng/mL in the bevacizumab group versus 0.0125 ± 0.0145 ng/mL in the ranibizumab group (p = 0.429). In the bevacizumab group, the median hs-cTnT level at week 9 (i.e. 1 week after the third injection) was 0.0095 ± 0.0085 ng/mL and at week 24 was 0.0100 ± 0.0107 ng/mL. Median hs-cTnT level in the ranibizumab group was 0.0140 ± 0.0132 and 0.0155 ± 0.0165 ng/mL at weeks 9 and 24, respectively. Repeated-measures ANOVA showed similar trend over time in hs-cTnT levels among the two treatment groups (p = 0.191) with no significant time effect (p = 0.227) within each treatment group and no significant treatment differences at any time point (p = 0.276) (Figure 1).
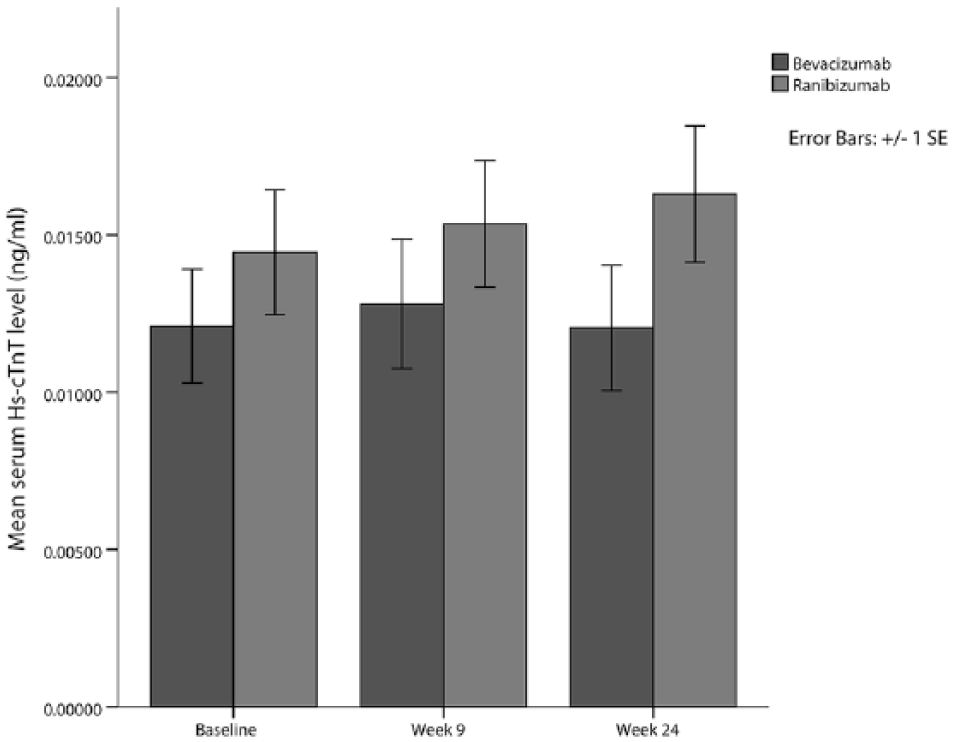
Mean change in serum high-sensitivity cardiac troponin T (hs-cTnT) levels for patients treated with intravitreal bevacizumab (n = 20) or ranibizumab (n = 20). Hs-cTnT levels were measured at baseline prior to any treatment and at week 9 after three consecutive monthly injections of either bevacizumab or ranibizumab. Patients were treated based on an as-needed regimen after the third mandatory injection, and hs-cTnT levels were measured at week 24. There was no significant difference between baseline and various time points within each treatment group and between groups.
Systemic VEGF levels
In the bevacizumab group, the median plasma VEGF level was 91.92 ± 421.50 pg/mL at baseline, 23.47 ± 24.50 pg/mL at week 9, and 48.55 ± 82.35 pg/mL at week 24. Patients who received ranibizumab had a median plasma VEGF level of 103.58 ± 168.82 pg/mL at baseline, 72.21 ± 77.83 pg/mL at week 9, and 44.11 ± 41.84 pg/mL at week 24. There was no significant difference in the baseline plasma VEGF levels between the two study groups (p = 0.529). Repeated-measures ANOVA showed a similar time trend in the plasma VEGF levels between the two groups (p = 0.074). The time trend reached significance for the bevacizumab group with pairwise comparisons showing a significant decrease in VEGF levels at week 9 (p = 0.001) and week 24 (p < 0.001) compared to baseline. However, in the ranibizumab group, VEGF levels were not significantly different at weeks 9 and 24 compared to baseline (p = 0.708 and p = 0.117, respectively) (Figure 2).
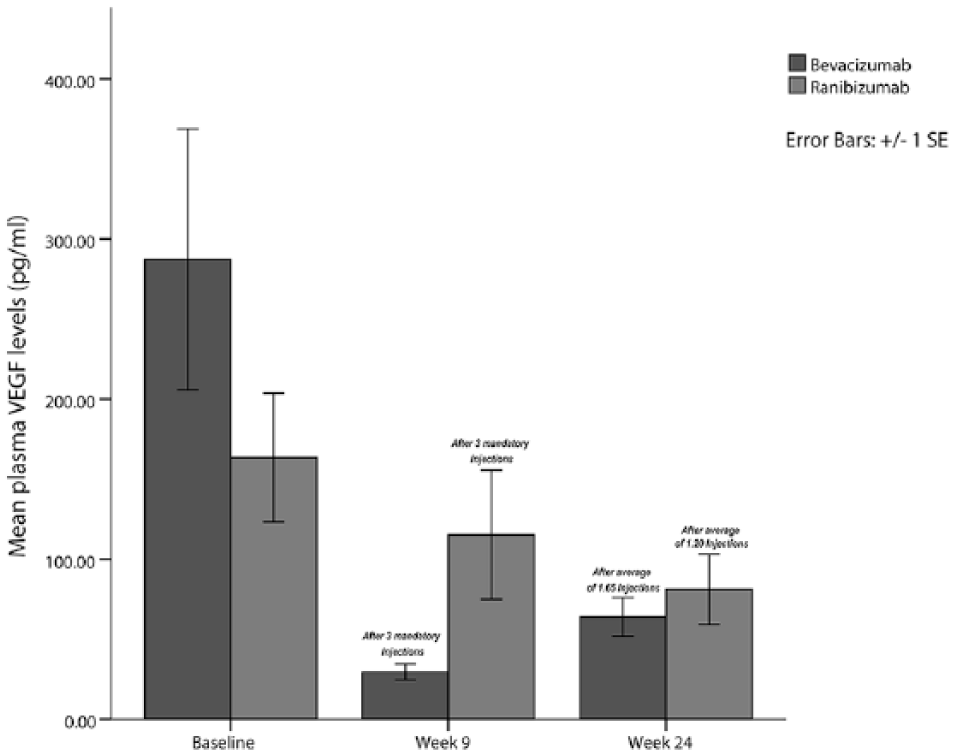
Mean change in plasma vascular endothelial growth factor (VEGF) levels for patients treated with intravitreal bevacizumab (n = 20) or ranibizumab (n = 20). VEGF levels were measured at baseline prior to any treatment and at week 9 after mandatory three consecutive monthly injections of either bevacizumab or ranibizumab. Patients were treated based on an as-needed regimen after the third mandatory injection, and VEGF levels were measured at week 24. There was a significant decrease in mean VEGF levels in bevacizumab-treated patients at weeks 9 and 24 compared to baseline. This was not observed with ranibizumab.
Patients in both groups received three consecutive monthly injections by week 8. Between weeks 8 and 24, patients in the bevacizumab received a median of 2.0 ± 3.0 injection versus 1.0 ± 2.8 injection in ranibizumab group (p = 0.314). Spearman’s correlation showed a significant association between the number of bevacizumab injections from weeks 8 to 24 and the decrease in VEGF levels at week 24 (R = −0.67, p = 0.032). This correlation was not observed in patients receiving ranibizumab (R = −0.341, p = 0.141).
Discussion
In this study, we used serum hs-cTnT as a marker for possible subclinical cardiac myocyte injury during intravitreal anti-VEGF therapy. Serial intravitreal injections of bevacizumab or ranibizumab did not lead to elevation in hs-cTnT. In both treatment groups, mean systemic hs-cTnT levels were practically unchanged compared to baseline after three consecutive monthly injections. Similarly, hs-cTnT levels were relatively stable between weeks 9 and 24 when fewer intravitreal injections were administered. Hs-cTnT is a highly sensitive marker of cardiac myocyte injury, more so than any myocardial imaging. Levels rise with any myocyte injury, whether it is macrovascular, microvascular, or from direct cytotoxic insult. As such, hs-cTnT is an established sensitive and objective marker for the diagnosis of acute myocardial infarction and myocardial damage in general.15,17–19 Even subclinical elevation in hs-cTnT concentration portends a higher likelihood of cardiovascular events in the future.23,24 Several studies have used cardiac troponin to demonstrate subclinical cardiac myocyte damage related to various interventions or treatments such as chemotherapy or radiation to the chest.25–28 More importantly, systemic bevacizumab treatment was associated with a transient rise in hs-cTnT. 29 Even with a relatively small sample size, these studies demonstrated subclinical cardiac myocyte damage when it occurred. Although highly sensitive, hs-cTnT can become elevated in other circumstances such as renal failure, pneumonia, pulmonary embolism, chronic obstructive pulmonary disease, and stroke. 19 Therefore, similar studies in the future should take this into account. Another point to consider for future studies is the timing of blood sample collection. We assumed that the lowest levels of systemic VEGF would be 1 to 7 days after the third injection, and any cardiac ischemic event will most likely coincide with this drop in VEGF. It is conceivable that an elevation in hs-cTnT may have occurred before or after the test was performed at weeks 9 and 24. Since systemic levels of hs-cTnT remain elevated 10 to 14 days after myocyte injury, it is unlikely that a significant cardiac injury would be missed if it had occurred within 2 weeks prior to the assay. Future studies can account for this by measuring hs-cTnT more frequently.
Many large randomized clinical trials did not find a definite risk of thromboembolic events with intravitreal anti-VEGF use.30–32 However, some systematic reviews detected a possible systemic safety signal related to higher dose and more frequent administration.33,34 Although systemic exposure with intravitreal bevacizumab seems higher than ranibizumab, 22 the rate of cardiovascular events with both agents seems to be similar.8,35–37 The Comparison of AMD Treatments Trials (CATT) study showed no difference in thromboembolic events between ranibizumab and bevacizumab. 5 On the other hand, the Inhibit VEGF in Age-related choroidal Neovascularisation (IVAN) study observed an increased risk of thromboembolic events and heart failure in the ranibizumab group. 14 Overall, the results in the literature are not conclusive due to the low frequency of these adverse events. In addition, the patient population that is most likely to require this treatment is already at risk for cardiovascular events and stroke, which makes it difficult to determine whether the adverse event is related to natural history or the intravitreal treatment. 37 One method to monitor for possible cardiac adverse events would be through serial examinations of serum cardiac troponin. This would give a more objective indicator of possible cardiac ischemic events.
Intravitreal ranibizumab had almost no effect on free-systemic VEGF concentrations, whereas bevacizumab significantly reduced free VEGF. These findings are consistent with previous reports where bevacizumab, but not ranibizumab, was associated with significantly reduced free VEGF concentrations after intravitreal injections in patients with neovascular AMD.13,14,22 We found that the decrease in free-systemic VEGF levels seemed to be related to the number of bevacizumab injections where the most precipitous drop occurred after the first three consecutive monthly injections. Moreover, systemic VEGF levels between weeks 9 and 24 were inversely related to the number of bevacizumab injections. This relationship was not observed with ranibizumab. We should not disregard changes in free-systemic VEGF levels associated with intravitreal bevacizumab since VEGF has a broad physiological role.38,39 Patients who need intravitreal anti-VEGF therapy, as those in this study, are a high-risk group for possible systemic thromboembolic events.37,40 This becomes a greater concern when there is chronic systemic inhibition from intravitreal anti-VEGF agents, especially bevacizumab. Of note is that the baseline VEGF values that we measured in both groups were higher than those obtained by Avery et al. 22 It may be due to the fact that we used EDTA tubes to collect the blood samples. This could have allowed more platelet activation or rupture compared to the citrate, theophylline, adenosine, and dipyridamole (CTAD) tubes used by Avery et al.
In conclusion, our measure of hs-cTnT did not indicate subclinical cardiac myocyte injury during intravitreal bevacizumab and ranibizumab therapy. However, we observed a negative effect on free-systemic VEGF levels after repeated intravitreal bevacizumab injections. One must keep in mind that this study was not powered to analyze changes in systemic VEGF levels. It will be interesting for future studies to examine the relationship between systemic VEGF levels and the frequency of intravitreal anti-VEGF injections. Although this was a prospective randomized study, the sample size was relatively small and the follow-up period was short. In addition, it would be more helpful to take blood samples 1 week after every injection since this would track changes in VEGF and hs-cTnT more accurately over time. Perhaps future studies can take this into consideration and measure other biomarkers for vascular injury such as C-reactive protein. Another possible limitation is the heterogeneity of patients enrolled with varying levels of vasculopathy and risk factors for cardiovascular events. Therefore, a larger study with longer follow-up and more homogeneous sample is necessary to determine the effect of chronic intravitreal anti-VEGF therapy on serum hs-cTnT levels.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported partly by Novartis Pharma AG (Basel, Switzerland) for the cost of the blood tests, namely, high-sensitivity cardiac troponin T (hs-cTnT) and vascular endothelial growth factor (VEGF). The authors indicate no financial interest in any product discussed in this study. ZFB has participated on advisory boards for Novartis Pharma AG and Bayer (Leverkusen, Germany). ZFB has received honoraria from Bayer and Novartis Pharma AG as invited speaker. ZFB has received research grants from Novartis Pharma AG and Allergan (Center Valley, PA, USA). The remainder of the authors have no financial disclosures.